Headache Pathway Case for Change - November 2017 - TVSCN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Headache Pathway Case for Change November 2017
Table of Contents
1 Executive summary ...................................................... 3
2 Background................................................................... 4
3 Introduction................................................................... 5
4 Epidemiology of headache .......................................... 5
5 National strategic context and drivers for change .... 6
6 Local Strategic Context ............................................... 7
7 The vision for Headache management ..................... 12
7.1 Improvement in primary care recognition of primary
headaches including migraine and medication overuse
headache ................................................................................ 12
7.2 Specialist triage of referrals .................................................. 13
7.3 Development of a community headache clinic .................... 16
7.4 Cost savings ........................................................................... 16
7.5 Cost of the new service in your area .................................... 18
8 Summary ..................................................................... 19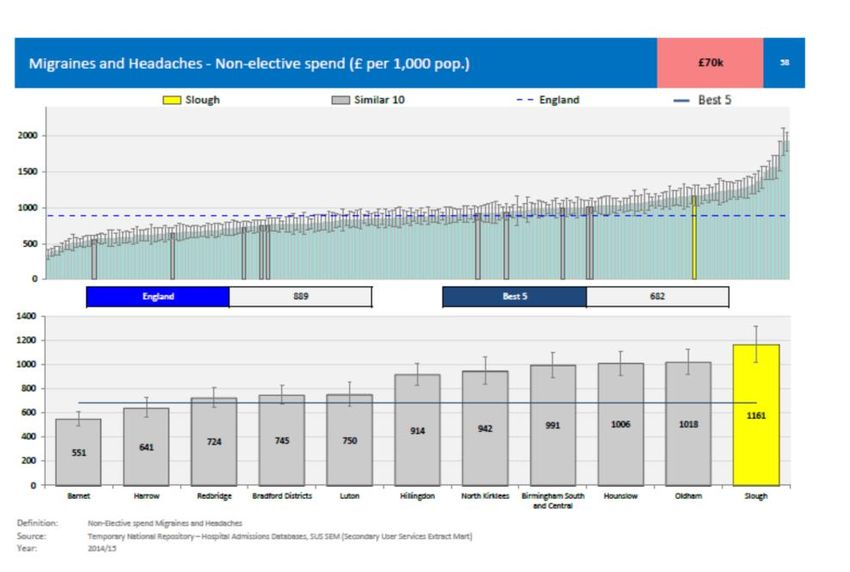
1 Executive summary
There are significant opportunities for the patient, the NHS, and the economy through
the improvement of the management of headache. England has one of the lowest
ratios of neurologists per population and case numbers are rising so it is imperative
that their time is used for the maximum value to the patient.
This Case for Change alongside a short summary document and a presentation
forms part of a pack for commissioners which provides detailed information to help
consideration of the development of a community headache pathway. This Case for
Change has been developed by assessing the current situation in Oxfordshire but the
methodology for consideration can be replicated in any area and the document
includes links to specific CCG data sets which are useful when a CCG develops their
own case. Oxfordshire CCG have undertaken a pilot and subsequent audit of the
proposed pathway and have plans to move to the new service in early 2018.
Current management of primary headache disorders and the challenges that are
being faced are described along with future projections and detail of the local and
national drivers for change.
This document outlines a number of opportunities for improvement in the way that
headaches can be managed in order to deliver the benefits listed below:
Improved patient experiences and health outcomes
Care provided more appropriately
Reduced health system costs and pressures on the acute sector
Care closer to home improving patient experience and reducing inequality
Improved access times to health services
Better, more efficient use of the limited resources of the NHS
Reduced costs to the NHS through inappropriate or delayed care
Reduced burden of disability and social care costs
Reduced variation
3 of 17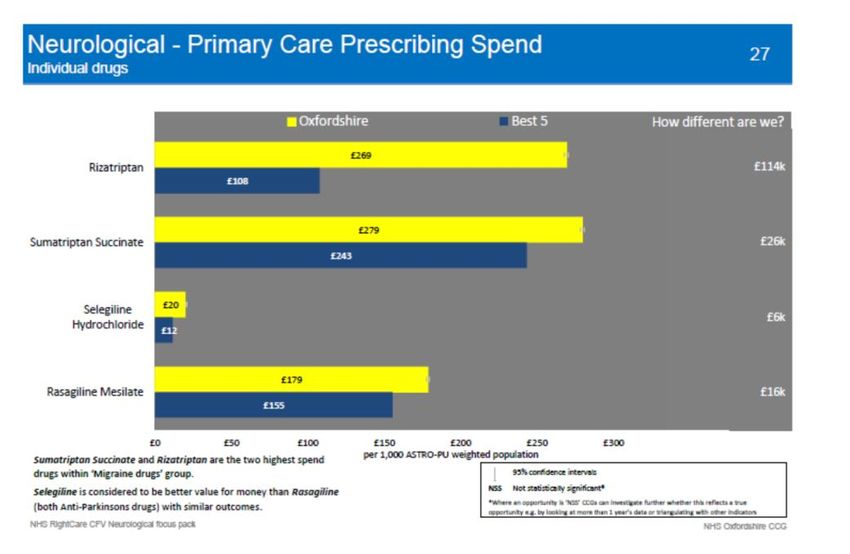
2 Background
The following key points highlight why focus on the headache pathway is important.
Headache accounts for 33% of all new referrals to neurology although the
majority of cases can be treated in primary care. It is the most common
neurological reason for A&E attendance, and A&E admissions for headache
have continued to increase steadily.i
In the year 2013/14 there were 17.4m A and E attendances in England for
headache, resulting in 17105 emergency admissions, 14123 were for migraine
It is estimated that 4% of primary care consultations are related to headaches
Improved community care for neurological conditions can improve care co-
ordination for the individual, optimise self-management and focus specific
resources on those with the greatest need
Data on hospital activity related to headache shows a steady increase in
activity between 2012 – 2016
The system is overstretched and the increase in neurology referrals is causing
pressure on outpatient clinics and patient delays.
Numbers of neurologists are at critical levels in many parts of England leading
to delays in provision of care so use of other skilled clinicians such as GPs
with special interest or nurse specialists is key
Most of the health and social burden of headaches is caused by primary
headache disorders and medication overuse headache.
The traditional model is process driven and not patient-centred
Local analysis in Oxfordshire shows 66% of primary headache and medication
overuse headaches referred to neurology outpatients could be successfully
managed in the community
Across England the total hospital admissions and costs for headache have
increased over the past four years.
The shift in services from the acute to the community/primary sector is
expected to be a key enabler in delivering around £4.3bn of a total £22bn
efficiency savings by 2020
National direction offers an opportunity and a requirement to reform and
considerably improve community care of long-term neurological conditions
4 of 20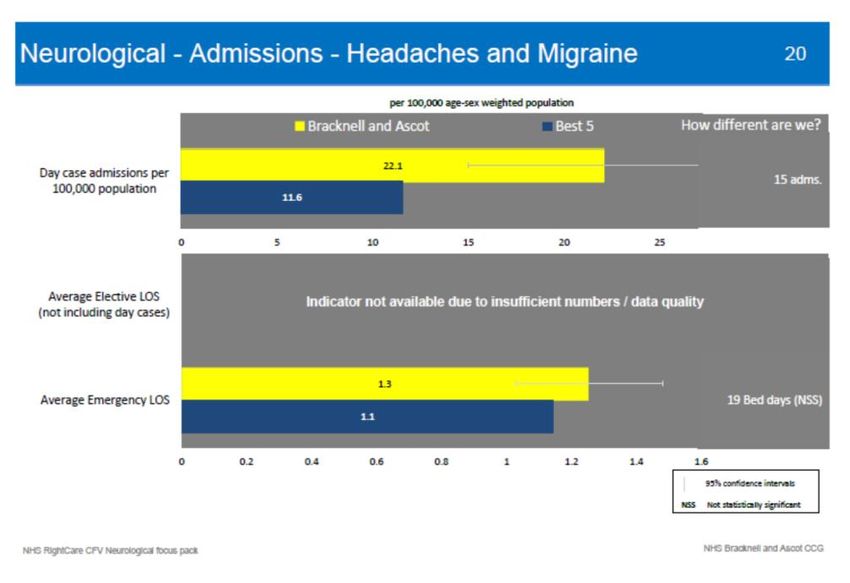
3 Introduction
Through review of current healthcare usage in Oxfordshire, this case for change
highlights that a significant part of the activity and financial pressure on the
neurology pathway is caused by primary headache and medication overuse
headache. It shows a clear argument for treating these types of headache in the
community where clinically appropriate.
This aligns with the national policy direction around developing more integrated
approaches to care delivery, improving quality and efficiency of services and moving
care closer to people’s homes from acute hospitals to community services.
The Transforming Community Neurology project report produced by the SCN in June
2016 aimed to encourage the adoption of community-based care models in order to
improve person-centred coordinated care and improve the quality of life for people
with long-term neurological conditions. This case for change focuses on a
community-based proposed solution for the specific management of
headache.
4 Epidemiology of headache
Headaches are one of the most common neurological problems presented to GPs
and neurologists. They can be painful and debilitating, an important cause of
absence from work or school, and a substantial burden on society.
Headache is a painful and disabling feature of the primary headache disorders
including migraine, tension-type, and cluster headache. Headache may be a
presenting symptom for many disease processes and is then termed as
secondary headache.
Headache affects 90% of the population at some time. They are among the
most common disorders of the nervous system and can be the cause of
significant and long-term disability. 4% of adults consult a GP each year for
headache or migraine.ii(Latinovic et al. 2006)
Whilst tension-type headache is the most common primary headache disorder
(experienced by 70% of the population), the most frequent headache seen in
general practice is migraine.
Migraine is classed by the World Health Organisation as one of the top 20
leading causes of disability amongst adults. 80% of migraine sufferers have
disabling attacks that interfere with life at work, home, and socialisation.iii
There are approximately 6,720,000 people living with migraine in England.
5 of 20
Migraine is more prevalent than diabetes, epilepsy and asthma combined.iv
(The Migraine Trust)
Patients with frequent headaches may overuse acute treatments such as
codeine, paracetamol, ibuprofen or triptans. With medication overuse, the
headaches can become chronic and intractable increasing the disability
arising from the headache.
There are many serious conditions that will present with headaches. Many
patients may visit their GP or A&E because they are worried about an
underlying sinister cause for their headaches. However most patients with
headaches will have a primary headache disorder.
97% of headache is managed in primary care (Latinovic et al: 2005) and it is
therefore essential to ensure that the correct management is initiated by GPs
to avoid ongoing disability, medication overuse, and inappropriate emergency
attendance and repeat GP attendance.
The majority of patients who are referred to secondary care for headaches are
seen once by a general neurology consultant; in many cases, this referral is to
exclude secondary causes such as tumours.
The direct cost to the NHS for headache is estimated at £1 billion per year
(Ridsdale 2007), with GP consults and medications of £468 per patient per
year. Costs may be substantially higher than estimated as headache patients
have frequent co-morbidities. For example, depression is three times more
common in patients with migraine than healthy people. The cost of headache
to the economy in terms of lost productivity was estimated at £5 billion.
Across Thames Valley the total hospital admissions and costs for headache
have increased over the past four years. In 2012/13 total costs for those with a
primary diagnosis of headache across the SCN area were £2,016,691 and for
those with a secondary diagnosis were £5,008.805. The total cost burden to
the Thames Valley SCN area was just over £7 million.
5 National strategic context and drivers for change
This project supports the vision set out in NHS England’s The Five Year Forward
View (2014) to explore the potential of new models of care to deliver locally-provided,
integrated care, organised around the patient. It offers an opportunity and a
requirement to reform and considerably improve community care of long-term
neurological conditions. Alongside improved patient experience and outcomes, it has
the ambition to achieve 2% net efficiency gains each year for the rest of the decade.
Arlene Wilkie, chief executive of the Neurological Alliance, said: “Good community
care services are crucial to people living with neurological conditions. They can
6 of 20
support improved wellbeing and better health outcomes for patients, help people to
self-manage their conditions more effectively and maintain good mental health. There
is great potential for better community care to reduce pressure on hospitals by
helping people maintain their good health and independence for longer.”
The All Party Parliamentary Headache in England report noted in 2014 that
‘The biggest opportunities to address the burden of headache exist within primary
care, since this is where the majority of cases present to. Despite the NICE
headache guideline and quality standards, the provision of good quality headache
care and patient satisfaction within primary care is poor. Strengthening resources to
improve the provision of care at primary care level will therefore yield good value for
money for commissioners. Initiatives to provide support to headache patients outside
of clinical settings will reduce the demand on busy GP surgeries. Approaches to
support properly diagnosed migraine and tension-type headache patients through
ongoing ‘remote’ support from primary care specialists have the potential to save
CCGs money by reducing clinical appointments. Partnerships with third sector
organisations to deliver this care can ensure that patient outcomes are achieved’
6 Local Strategic Context
New
Care closer
models of
Care to home
STP Increased
priorities activity
RightCare Cost
Approach pressures
6.1 Sustainability and Transformation Partnership priorities
Many of the Sustainability and Transformation Partnerships (STP) across the country
are focussing on moving care out of the acute sector and into the community closer
to home. There is also a focus on initiatives which provide easier to access high
7 of 20
quality care whilst delivering savings through reduction of admissions and use of
secondary care.
6.2 Care closer to home
Currently many patients across the country have to travel beyond their CCG area to
receive care. The development of community clinics will improve patient experience
as care will be provided closer to home. Data in the Right Care Neurology focus pack
shows that for 2013-14 shows that in England only 49.8% of neurology outpatient
appointments (consultant) are seen in their home CCG.
6.3 Demographic pressures
The population across England is predicted to rise by 16.5% in the period 2014 –
2039Error! Bookmark not defined.. A sustainable solution needs to be developed
to deal with the additional capacity needed for headache management.
%
AREA 2014 2018 2022 2026 2030 2034 2038 2039 increase
England (All Ages) 54,317 56,062 57,634 59,135 60,524 61,800 62,992 63,282 16.50%
Specific CCG data on demographics can be sourced at the following link:
https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationpr
ojections/datasets/clinicalcommissioninggroupsinenglandz2
8 of 20
6.4 Increase in activity
The increase in neurology activity is marked and provides a clear case for the review of current management. The below data was
published in August 2017 and individual CCG data is available at the following link: *Neurology services: hospital activity data -
GOV.UK
The data below shows that in England there is a 12.2% increase in ordinary (inpatient admissions) and 53% increase in day case
admissions for Headache and migraines between 2012-2016 which highlights the importance of managing referrals early in the
community.
Hospital admissions with a mention of a neurological condition, England, age 20+
2012/13 hospital admissions 2013/14 hospital admissions 2014/15 hospital admissions 2015/16 hospital admissions
with mention of neurological with mention of neurological with mention of neurological with mention of neurological
condition condition condition condition % increase 2012 - 2016
Primary diagnosis ordinary ordinary ordinary ordinary ordinary
on admission (inpatient) day case (inpatient) day case (inpatient) day case (inpatient) day case (inpatient) day case
episode admissions admissions Total admissions admissions Total admissions admissions Total admissions admissions Total admissions admissions Total
Headaches and
migraine 65,252 8,223 73,475 69,136 10,561 79,697 70,664 12,163 82,827 73,189 12,612 85,801 12.16% 53.37% 16.78%
6.5 Increase in Emergency Admissions
Between 2012 – 2016 in England there was a 10% increase in emergency hospital admissions with a mention of a neurological
condition and 13% increase in emergency hospital admissions where the primary diagnosis on admission is identified as
Headaches and Migraine.
Emergency hospital admissions with a mention of a neurological condition, England CCGs total, age 20+ (2012-2016)
(By neurological condition group)
% increase 2012
Primary diagnosis on admission episode 2012/13 2013/14 2014/15 2015/16 - 2016
Headaches and migraine 62,824 66,616 68,320 70,966 12.96%
Neurological condition total 186,429 192,410 198,448 205,214 10.08%
*Neurology services: hospital activity data - GOV.UK(accessed 23 August 2017)
9 of 17
6.6 CCG specific data
Specific Hospital Episode statistics data (HES) related to headache and migraine by individual CCG can help with development of
the case for change.
The following codes are relevant:
Headache ICD 10 codes : G44- Other headache syndromes, G440- Cluster headache syndrome, G441- Vascular headache, not
elsewhere classified, G442- Tension-type headache, G443- Chronic post-traumatic headache, G444- Drug-induced headache, not
elsewhere classified, G448- Other specified headache syndromes
Migraine ICD codes: G43- Migraine, G430- Migraine without aura [common migraine], G431- Migraine with aura [classical
migraine], G432- Status migrainosus, G433- Complicated migraine, G438- Other migraine, G439- Migraine, unspecified.
6.7 CCG/STP performance against comparators
Analysis of Right Care data in the Neurological focus pack published in 2016 enables CCGs and STPs to understand how they are
performing against Right Care Comparator CCGs and the average performance across England. It highlights opportunities for
savings and for improving outcomes. This data can highlight where prescribing or non-elective spend is more than comparator
CCGs or where there are more admissions and longer length of stay compared to comparator CCGs.
Neurology is highlighted as an area where outcomes can be improved and savings made in many STP areas as illustrated by the
following information from the Frimley STP and Buckinghamshire, Oxfordshire, Berkshire West STP.
10 of 2011 of 20
7 The vision for Headache management
‘To develop a headache pathway that allows patients with headache who need to be
seen in secondary care to do so quickly, while keeping in the community those
patients with headache who can be better managed there, through supporting GPs
in their independent practice and providing community headache services that are
cost-efficient, easier to access and care is delivered closer to home. Not only would
this improve patient care but also release capacity in over-stretched neurology
outpatient clinics’. Dr Richard Wood, Oxfordshire CCG
There are three key elements in the development of the optimal community headache
pathway.
1. Improvement in primary care recognition of primary headaches including
migraine and medication overuse headache
2. Triage process to reduce outpatient clinic appointments
3. Development of community headache clinic
7.1 Improvement in primary care recognition of primary headaches
including migraine and medication overuse headache
The following section outlines potential ways to support improved diagnosis of primary
headaches in primary care. This can be supported as follows:
Education and Support for GP management of headache
Clear guidelines and proformas for diagnosis
It is important that guidelines are provided to the GPs to show clearly what steps can be
tried prior to referral and to describe those cases when referral is important. The NICE
guidelinev for Headache provides the framework but the specialist neurologist experience
and learning can help interpret and enhance these.
Urgent referrals that include symptoms of brain tumours should be treated outside
the proposed headache pathway and have their own dedicated cancer pathway.
They are not included in the proposal.
Learning opportunities
Opportunities should be found to educate qualified and GPs in training on what to look out
for. When it is felt a referral can be handled by the GP it should be returned with
comprehensive advice from the specialist for continued management.
Structured Education and Support for Patients to self-care
When people self care and are supported to do this, they are more likely to:
experience better health and well-being
12 of 17reduce the perceived severity of their symptoms, including pain
improve medicines compliance
prevent the need for emergency health and social services
prevent unnecessary hospital admissions
have better planned and co-ordinated care
remain in their own home
have greater confidence and a sense of control
have better mental health and less depression
Patients need targeted education on headaches and when to seek medical advice and
particular education around medication overuse headache. In some areas, clinics have
been set up for those who have received a positive diagnosis of migraine, to provide
education and effective treatment in a group environment which aims to reduce the
patient’s migraine related disability and improve their ability to manage their migraine
independently, reducing reliance on medical services for management of migraine over
the longer term.
Support for Pharmacists
Pharmacists play a key role in dispensing over the counter or prescribed medication to
patients with headache and need to be supported in delivering targeted patient education
especially around medication overuse headache.
7.2 Specialist triage of referrals
In order to ensure that the optimum pathway is considered for each patient referred by a
GP or from another consultant in the hospital it is important that a triage process is
undertaken. The consultant can also be contacted for advice around patients attending
Accident and Emergency with headache.
The triage needs to be undertaken by a neurology consultant who will also provide advice
to referrers, interpret imaging reports and provide clinical oversight and support to the
community clinicians. There should be a robust mechanism (ideally electronic portal) for
communication between the consultant undertaking the triage, the GP referrer, the
community clinic and the hospital.
After reviewing the referral the neurology consultant could manage the referral in the
following ways:
– Provide advice back to referrer for continued management
• Where clearly a primary headache (such as migraine)
– Offer appointment at Community Based Headache clinic
• Where patient needs more support than GP can provide (mainly
migraine, tension-type headache, and cluster headache but also
medication overuse headache and chronic post-concussion
headache)
• Where investigations are not required
13 of 20– Arrange Imaging without outpatient appointment
• If it is felt imaging is needed (typically structural MRI head without
contrast) this could be arranged without a face to face clinic
appointment
• If the scan is normal the patient can then be managed in the
community clinic of by the GP or have an appointment at outpatients if
further investigation needed
– Offer General neurology outpatient clinic appointment
• If patients have headaches with neurological signs or red flag
symptoms that require an underlying pathology to be ruled out so
further investigations are needed
– Offer Specialist headache clinic appointment
• Rarely the consultant may feel the patient should receive specialist
consultant neurology assessment and management directly rather
than through presentation at a general clinic
– Refer to Physiotherapist
Rarely it may be appropriate to refer directly to physio (eg for those
with clear cervicogenic headache)
An audit of a cohort of 135 patients in Oxfordshire by 3 consultant neurologists suggested
that the likely split between the above options is as follows:
14 of 20Urgent referrals that
include symptoms of brain
tumours have their own
Headache pathway dedicated 2 week cancer
pathway.
Neurology
Community
outpatient
Patient education Headache Clinic
and advice from
clinic
Pharmacy
Referral
Headache
GP consultant
GP management Advice triage Specialist
Headache clinic
A and E MRI without
outpatient
appointment
15 of 177.3 Development of a community headache clinic
A community headache clinic could be run by headache specialist nurse or GP
with a special interest in headache with the training and support of the consultant
where needed. It would manage primary headache disorders such as migraine,
tension-type headache, cluster headache, chronic post-concussion headache and
can provide long term consistent care close to home if appropriate.
It is important to select the locality of the clinic carefully with reference to the local
population and likely number of referrals. Patient engagement and involvement of
patient participation groups in the planning at an early stage is vital.
The clinic will need a robust information sharing mechanism with the hospital and
the GP practices to make referrals management and appointment booking effective
and efficient. Ideally this will be through an electronic portal. Administration support
to process bookings and arrange follow ups and maintain communication with the
patient’s GP is also important.
There is also evidence of a link between anxiety/depression and headache.
Although not fully understood a study in the Journal of Neurology, Neurosurgery, &
Psychiatryvi of 107 patients with Chronic Cluster Headaches, 75 percent were
diagnosed with an anxiety disorder and 43 percent with depression. The inclusion of
psychological support within the pathway merits consideration.
7.4 Cost savings
The savings from this community model come from the difference in the charges for
appointments in the general neurology outpatient clinic and in the community
headache clinic. The cost savings will obviously depend on local numbers and
situations but the below Oxfordshire chart identifies how savings may be made if
referrals are managed according to the expected triage as shown on page 13.
The Oxfordshire pilot shows that the tariff for a first appointment in a community
health clinic (which is set to cover costs of the clinic and triage and training) is likely
to be 43% of the cost of a hospital first outpatient appointment
The below table shows savings for those patients who are currently seen in
outpatient clinic but could be seen elsewhere. It is based on a cohort of 1100
patients of which 6% could have imaging without appointment, 10% could be
referred back to GP and 50% (550) could go to Community health clinic.
The clinic costs are based on managing the cohort of 550 patients plus their
anticipated follow-ups. They are based on 3 clinics for 42 weeks a year with 6 x 30
min appointment in each clinic (18 appointments x 42 weeks = total of 756 x 30 min
appointments). Calculation of anticipated follow up rate is complex and will differ
according to clinician involved but the chart below is worked on an estimate and an
assumption that a follow-up appointment would take 15 minutes.
16 of 20Savings for the 66% of patients who are currently seen in
outpatient clinic but could be seen elsewhere
Savings come from:
- Reduced tariff of CHC
(for which 50%
referrals now seen)
- Sending 6% of
referrals to MRI
without appointment
- Advising GP without
seeing patient in 10%
of cases
Includes cost of time for
referral triage, ordering and
interpreting MRIs, advice to
Community clinic GP, supporting community
tariff for 30min clinic, and pathway
appointment is oversight
£110
17 of 207.5 Cost of the new service in your area
Each CCG will be paying different amounts for their outpatient first and follow up
appointments and will incur different local set up costs but the principles of where
savings can be made remain the same.
Apart from the savings made through referrals which are:
1) returned to the referrer
2) have imaging and are then returned to the referrer
3) take place in the community rather than the outpatient clinic
there may be additional savings from seeing follow ups, of the referrals which were
initially seen in the hospital, within the community clinic
It is important to highlight that If the released appointments in the neurology clinic are
used for seeing patients rather than decommissioned this will obviously impact on
any potential savings. However, the clear benefit of having hundreds of additional
appointments available to see more appropriate referrals in the acute hospital clinic
to support the 18 week pathway cannot be underestimated.
The following areas need to be considered when setting up a new pathway:
– Cost of Consultant Neurologist time to triage referrals
– Training costs for Neurology consultant to train community clinic specialist
(GP with special interest or specialist nurse
– Numbers of patients likely to be seen in community clinic (1st appointments
and follow ups)
– Costs of running weekly clinic (30 min first appointment slot for each patient
plus follow ups)
– Cost of Clinician time in clinic plus admin time
– Cost of Management time
– Patient/PPG involvement and engagement in the design of the service
– Secretarial time (20 mins per patient for report)
– Receptionist/admin time for booking and attendance at clinic
– Service charge (rent clinic space, utilities etc)
– Governance and Indemnity premium (may be negotiated with acute Trust)
– Education programme costs
– Psychological support
– Information technology to ensure joined up service
– Key performance indicators/metrics
18 of 208 Summary
The evidence from the Oxfordshire CCG community headache pilot has evidenced
that cost savings can be made, patient experience and outcomes improved and
pressure on hospital clinics reduced through the set up of community provision for
headache.
It is hoped that CCGs across the country will review their case for change and use
some of the learning from the Oxfordshire experience in order to enhance the care
and experience of local patients.
In summary, it is anticipated that the following benefits will be realised:
Provision of a more efficient local service Appropriate care closer to home
Improved patient experience as faster Improved knowledge and skills in primary
access to the right support care
Improved use of finances to ensure cost Transfer of care from the acute to the
effective and appropriate expenditure community
Improved patient outcomes as patients Closer links with third sector support in
who need to see a specialist have the community
quicker access
Increased capacity in outpatient clinics Improved patient education and self
reducing waiting times management
Increased communication between Reduction in number of referrals to
primary and secondary care supporting secondary care which can be managed
learning in primary care
Increased consistency of care Reduction in A and E admissions and
attendances due to easier access to
support
The community pathway is due to be set up in Oxfordshire in early 2018. For further
information please contact:
Dr Zam Cader, Consultant in Neurology zameel.cader@ndcn.ox.ac.uk
Dr Richard Wood, GP Richard.Wood@oxfordshireccg.nhs.uk
19 of 20References
i
Headache Services in England - A Report of the All-Party Parliamentary Group on
Primary Headache Disorders 2014
https://www.migrainetrust.org/wp-content/uploads/2015/12/APPGPHD-Report-on-
Headache-Services-in-England-–-Full-Report.pdf
ii
Latinovic R, Gulliford M, Ridsdale L (2006) Headache and migraine in primary
care: consultation, prescription, and referral rates in a large population. J Neurol
Neurosurg Psychiatry 77:385–387
iii
WORLD Health Organisation factsheets
http://www.who.int/mediacentre/factsheets/fs277/en/
iv
Migraine Trust facts and figures on Migraine
https://www.migrainetrust.org/about-migraine/migraine-what-is-it/facts-figures/
v
NICE guidance on management of headache
https://www.nice.org.uk/guidance/cg150
vi
Donnet A, Lanteri-Minet M, Guegan-Massardier E, Mick G, Fabre N et al. Chronic
cluster headache: A French clinical descriptive study.J Neurol Neurosurg Psychiatry
2007;78:1354–1358.
20 of 20You can also read