Health care transitions for persons living with dementia and their caregivers
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ashbourne et al. BMC Geriatrics (2021) 21:285
https://doi.org/10.1186/s12877-021-02235-5
RESEARCH Open Access
Health care transitions for persons living
with dementia and their caregivers
Jessica Ashbourne1, Veronique Boscart1,2, Samantha Meyer1, Catherine E. Tong1 and Paul Stolee1*
Abstract
Background: Persons with dementia are likely to require care from various health care providers in multiple care
settings, necessitating navigation through an often-fragmented care system. This study aimed to create a better
understanding of care transition experiences from the perspectives of persons living with dementia and their
caregivers in Ontario, Canada, through the development of a theoretical framework.
Methods: Constructivist grounded theory guided the study. Seventeen individual caregiver interviews, and 12 dyad
interviews including persons with dementia and their caregivers, were recorded and transcribed verbatim. The data
were coded using NVivo 10 software; analysis occurred iteratively until saturation was reached.
Results: A theoretical framework outlining the context, processes, and influencing factors of care transitions was
developed and refined. Gaining an in-depth understanding of the complex care transitions of individuals with
dementia and their caregivers is an important step in improving the quality of care and life for this population.
Conclusion: The framework developed in this study provides a focal point for efforts to improve the health care
transitions of persons living with dementia.
Keywords: Dementia, Health care system navigation, Health care transitions, Care coordination, Constructivist
grounded theory
Background accompanied by increases in economic consequences,
The term ‘dementia’ refers to a number of disorders system constraints related to demand for long-term care
resulting in a progressive decline in cognition [1]. Symp- beds and community services, and an increase in unpaid
toms of memory loss and communication difficulty often informal caregiving hours from 231 million to 756 mil-
precipitate dependence in activities of daily living lion hours per year [1]. There is thus an urgent need for
(ADLs) with consequences for quality of life [1–5]. De- effective coordination of health care and community
mentia is often complicated by comorbid conditions and support services for individuals living with dementia and
polypharmacy, necessitating care by multiple providers their informal caregivers [8].
in multiple care settings [6]. Older adults with dementia The nature of dementia frequently requires individuals
use health care services more frequently than older and their caregivers to contact multiple health care sec-
adults without cognitive impairment [7]. tors, and to experience transitional periods in which they
Approximately 1.5% of the Canadian population has a need to navigate through an often-fragmented system [6,
diagnosis of dementia, and this proportion will nearly 7, 9–11]. A health care transition can be defined as “the
double over the next 30 years [1]. This growth will be movement patients make between health care practi-
tioners and settings as their condition and care needs
* Correspondence: stolee@uwaterloo.ca change during the course of a chronic or acute illness”
1
School of Public Health and Health Systems, University of Waterloo, 200
University Avenue West, Waterloo, ON N2L 3G1, Canada [12]. The care transition process is one of increased vul-
Full list of author information is available at the end of the article nerability and risk, due to the potential for inadequate
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.Ashbourne et al. BMC Geriatrics (2021) 21:285 Page 2 of 13
transfers of information, medication errors, and other Health care system improvements for persons living
adverse events impacting patient safety, care quality, and with dementia could be facilitated by a theoretical
outcomes [5, 13–15]. The dementia experience exists framework based on an in-depth understanding of how
amid current system- and organizational-level inadequa- persons living with dementia and their caregivers experi-
cies in care coordination and continuity; overlaps and ence transitions across the care continuum. The object-
gaps in health care services further complicate transi- ive of this study was to explore the care transition
tions [11, 16–18]. Transitional care is a concept that has experiences of individuals living with dementia and their
been previously described as “a set of actions designed caregivers and to use these perspectives to develop a
to ensure the coordination and continuity of health care theoretical framework outlining the factors affecting
as patients transfer between different locations or differ- health care transitions.
ent levels of care within the same location” [19].
Although system navigation and transitional care for Methods
persons with dementia have been recognized as prior- Study design
ities for policy [1], research [20], and performance im- Constructivist grounded theory methods [32] were used
provement [21], there remains a lack of understanding to fulfill the study objectives. In line with social con-
of how these challenges might best be addressed. Most structivism, multiple realities and individual values were
research on care transitions has overlooked older adults acknowledged and respected, and knowledge was co-
living with dementia [22]. In fact, a review of studies of constructed by researchers and participants. Memos and
transitional care programs [23] found that some studies journaling helped maintain reflexivity [32, 33].
purposefully excluded persons with dementia. Literature
on transitions has largely focused on specific transitions Study participants
(e.g., hospital-to-home) [18, 24, 25]. This trend is echoed Recognizing the present and growing importance of in-
in recent studies exploring transitions for persons with formal caregivers for persons living with dementia [34,
dementia [26–29]. For example, Gilmore-Bykovskyi and 35] both persons living with dementia and their care-
colleagues [26] obtained nurses’ perspectives on transi- givers were included in the study. Caregivers were also
tions for persons living with dementia from hospitals to able to provide information about the transitions of
skilled-nursing facilities. Therefore, additional research those with dementia who could no longer communicate
on care transitions from a cross-system perspective is effectively. Eligible participants were individuals who: a)
warranted. had a self-reported diagnosis of dementia or a were a
By focusing on cross-system transitions, this study re- caregiver for someone with a diagnosis, and b) had
spects the inherent complexity of the health care system. undergone a health care system transition since time of
Understanding how health care in Ontario is organized diagnosis. There were no explicit exclusion criteria based
can provide some insight into the system through which on dementia diagnosis or stage, so as not to risk the
participants navigated. Health care in Ontario is gov- omission of important voices, as has been the case previ-
erned by the Ministry of Health and Long-Term Care ously [23, 36, 37]. Care transitions were also defined
(MOHLTC). The MOHLTC divides health care spend- broadly; participants must have moved between more
ing into different sectors of operating expenses. Physi- than one health care provider or health care setting.
cians are funded through the Ontario Health Insurance
Program (OHIP), which consists of a portion of Recruitment and study setting
MOHLTC funding. As of 2017, most individuals (90.8%) Eight Alzheimer Society of Ontario chapters and one
in the province had access to a family doctor or other Family Health Team were approached via e-mail to help
primary care provider [30]. The role of the family phys- identify persons with dementia and their caregivers will-
ician is to provide comprehensive medical care to indi- ing to participate. This yielded a participant pool of pri-
viduals at all stages of life or disease in various health marily community-dwelling persons with dementia and
care settings. They are seen as a central hub for an indi- their caregivers. All interviews were conducted in the
vidual’s care, acting as a gatekeeper for access to and co- community setting; however, some of the individual in-
ordination of additional health services, including terviews with caregivers represented persons with de-
referral to specialists [31]. In Ontario, regionalized mentia who had transitioned into institutionalized
health organizations provide further infrastructure to settings, such as long-term care.
support planning and coordination of health services.1
Data collection
1 Preferences for individual or dyad interviews (including
At the time of data collection for this study, these were the Local
Health Integration Networks (LHINs); LHINS are currently evolving a person with dementia and an informal caregiver) were
to a new organizational structure and identity. respected [38, 39]. All persons with dementia who wereAshbourne et al. BMC Geriatrics (2021) 21:285 Page 3 of 13
recruited preferred to be interviewed in the presence of With consent of the participants, interviews were audio-
an informal caregiver; some caregivers were also inter- recorded. The interviews lasted approximately 1 h each.
viewed individually. Preferences for interview location Interviews were conducted by the lead author, a Mas-
were also respected. All participants chose to be inter- ter’s-level trainee with prior qualitative research training,
viewed in their own homes. Each participant was given over a seven-month period; verbatim transcriptions
an information letter, which was reviewed verbally. completed shortly after each interview allowed for simul-
Transitions were described to participants as periods of taneous data collection and analysis.
time during which they moved from one health care set-
ting to another or from one provider to another within Data analysis
the health care system. The researchers determined Following the analytic steps outlined by both Glaser [40]
whether persons with dementia were able to provide and Charmaz [41], we engaged in two stages of coding,
consent by ascertaining whether the participants under- after an initial read-through of the transcripts: first, open
stood the nature of the research, appreciated the conse- coding, and second, focused coding. Per Charmaz [32],
quences of participation and understood alternative theoretical coding was integrated throughout. The cod-
choices. Each person interviewed was able to provide his ing was completed by two data coders and the results
or her own consent. All participants who began the were reviewed with a third analyst. In open coding, data
study continued until the end. were closely examined using line-by-line and incident-
A background information form was completed using by-incident coding. Short, action-focused codes, or ger-
verbal information from participants; this provided data unds, were assigned to each small piece of data (for ex-
for sample description. Open-ended questions were used ample: ‘maintaining a social life’, ‘seeing the future in
to obtain stories about care transition experiences. All others’ experiences’, ‘learning caregiver strategies’, ‘being
questions were directed to persons with dementia first. prepared’, ‘having multiple providers in the room’). A
If they did not answer, their caregivers were given the constant comparative method, during which segments
opportunity to provide details. Participants were first within and between interviews were compared through-
asked to identify the services, support and care that they out the data collection and analysis processes, was
had received since the dementia diagnosis. They were employed [32]. Guided by Charmaz [32], data were com-
subsequently asked to describe a time during which they pared to other data throughout the entire coding process
moved from one person or setting in the health care sys- to elucidate similarities and differences. Observations
tem to another person or setting. Further sample inter- and ideas that arose from the data were noted in memos
view questions are summarized in Table 1 and the full [42]. For example, one memo noted how participants de-
interview guide is included in Supplementary File 1. scribed their transition experiences in relation to others’
experiences. Comparative methods were used to identify
and compare incidents in the data wherein participants
Table 1 Sample interview guide questions and prompts spoke about others’ experiences. In focused coding, the
Sample Interview Guide Questions & Prompts most frequent or significant codes from the initial cod-
Can you tell me about time during which you moved from one ing were synthesized from the data into a more coherent
person or setting in the health care system to another person or story [32]. The initial codes were grouped into categories
setting? *Give examples if necessary*
a. In what setting did you begin your experience?
and subcategories based on their similarities and differ-
b. What care setting did you transition to? ences, and relationships were suggested using memos
Optional Prompts: and diagrams. The categories were refined and devel-
Can you walk me through what happened? What aspects of your oped using theoretical sampling, a process by which pre-
transition from X to X went well/could have been improved? liminary categories are further developed by directing
Do you think that your diagnosis of dementia influenced this experience (if
yes, in what way?) subsequent interviews. Charmaz states, “theoretical sam-
pling can entail studying documents, conducting obser-
Was any organization or service helpful during or after your
transition? What did X help you with? How has it been helpful? vations, or participating in new social worlds as well as
Can you tell me about any instructions that you received, if any,
interviewing or reinterviewing with a focus on your the-
from the care providers about how you could manage your oretical categories.” Given that it was difficult to choose
condition(s) on your own? new participants based on the emerging categories,
Follow-up: Were these instructions important to your experience
moving between providers/settings? Why/why not?
probing questions were used to delve into specific as-
pects of experiences and further refine categories [32,
Can you tell me anything about the communication that you
observed or were aware of between the care providers that were 33]. For example, when people described their transi-
involved in your care? tions, they often spoke about the events leading up to
Follow-up: Was this communication important to your the transition. To further refine this category, partici-
experience moving between providers/settings? Why/why not?
pants were probed to describe how each transitionAshbourne et al. BMC Geriatrics (2021) 21:285 Page 4 of 13
experience began. This led to the refinement of the sub- Table 2 Participant characteristics
category of influencing factors titled ‘catalysts’ in the Participant Characteristics (N = 41, in 12 dyad and 17 individual
results. interviews; n = 29 for persons with dementia who were
represented in the interviews*)
Data were collected and analysed until the authors be-
lieved theoretical saturation was reached; in practice, Mean (min, max)
theoretical saturation was determined by noting a point Age
in the coding process at which no new codes were re- Persons with dementia 78 (min: 58, max: 94)
quired to explain the meanings behind participants’ stor- Caregivers 69 (min: 56, max: 80)
ies [43]. After no new codes were required, an additional N (%)
five interviews were conducted to confirm saturation.
Participant Type
The researchers conducted member checks with partici-
Persons with dementia 12 (29.3)
pants by telephone; thirteen participants provided
feedback. Caregivers 29 (70.7)
Gender
Persons with dementia- Women 6 (20.7)
Theoretical framework development
When theoretical saturation was reached and confirmed, Persons with dementia- Men 23 (79.3)
a framework was developed and refined to describe care Caregivers- Women 25 (86.2)
transitions from the perspectives of persons with demen- Caregivers- Men 4 (13.8)
tia and their caregivers and to fulfill the study’s primary Relationship of Caregivers to Person with Dementia
objective. Since the study has been situated within a
Son 1 (3.4)
constructivist framework, the resulting theory is inter-
Husband 3 (10.4)
pretive [32]. Diagramming was used throughout the data
collection and analysis process to visually represent Daughter 4 (13.8)
emerging categories and relationships; additional infor- Wife 21 (72.4)
mation about the diagramming and analysis can be Types of Dementia Diagnosed
found in [blinded for review]. Lewy Bodies 1 (3.4)
Parkinson’s 1 (3.4)
Sample description Fronto-temporal 2 (6.9)
Twenty-nine interviews were conducted in 15 cities Mild Cognitive Impairment 2 (6.9)
or towns and three health regions (then organized as
Mixed 3 (10.4)
Local Health Integration Networks) within Ontario,
Vascular 4 (13.8)
Canada; this included twelve dyad interviews and
seventeen caregiver-only interviews. Participants char- Alzheimer’s 8 (27.6)
acteristics are summarized in Table 2. Participants Non-specified 8 (27.6)
presented with a range of self-reported dementia diag- Number of chronic conditions of persons with dementia
noses; in order of frequency these were: Alzheimer’s 0–1 15 (51.7)
Disease, Vascular Dementia, Mixed Dementia, Mild
2–3 5 (17.2)
Cognitive Impairment, Fronto-temporal Dementia,
4–5 5 (17.2)
Parkinson’s Dementia, and Dementia with Lewy Bod-
ies. Over one quarter of participants reported a non- 6+ 4 (13.8)
specified or unclear diagnosis. Individuals received *While only 12 persons with dementia were directly interviewed, n = 29 refers
to the persons with dementia who were either interviewed directly in a dyad
their dementia diagnoses from a variety of providers interview AND who were spoken of/for in the caregiver interviews
including geriatricians, primary care physicians, physi-
cians at memory clinics, neurologists, and one doctor Results
in a care home. Per the eligibility criteria, all partici- Theoretical framework
pants had experienced a transition with the health The final representation of the emergent framework of
care system after a diagnosis of dementia. Transitions dementia-specific transitions is depicted in Fig. 1. Key
experienced by participants included those between themes that emerged from the data were organized into
primary care providers, specialists, memory clinics, three categories: transition context, transition processes,
hospital, respite care, long-term care home, and home and influencing factors. Identifying important contextual
care providers. elements respected the fact that transitions did not
This study received ethics clearance through the occur within a vacuum; they were situated within com-
[blinded for review] Office of Research Ethics. munities and influenced by the perceptions and aims ofAshbourne et al. BMC Geriatrics (2021) 21:285 Page 5 of 13
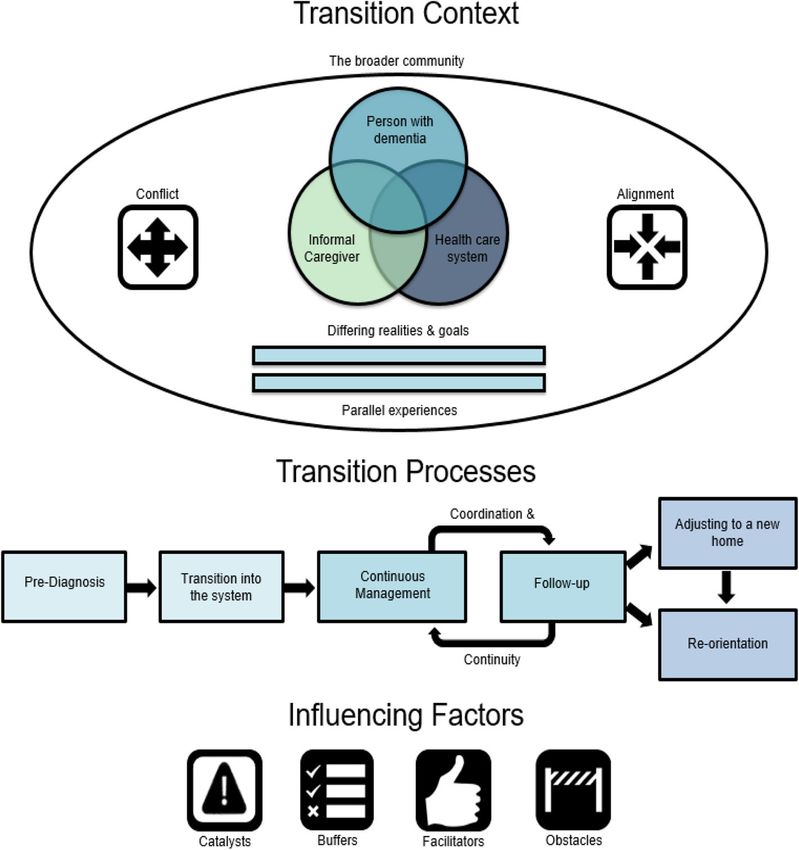
Fig. 1 A three-part theoretical framework outlining the context, processes and influencing factors of care transitions from the perspectives of
individuals with dementia and their caregivers
participating parties. Subcategories of transition context her husband’s view of reality did not align with hers in
reflected differing realities and goals among those in- saying: “…his opinion of what he is capable of and reality
volved in the transitions, the parallel experiences of is not always the same.” She continued on to express her
other individuals undergoing similar transitions, and the concerns for safety related to such disparities in percep-
broader community. Rather than discrete instances of tion, indicating that her husband’s descriptions of his
movement from setting to setting, transitions were expe- own abilities made him seem in need of less support
rienced as continuous and linked to phases of the de- than she deemed necessary. A similar concern was pre-
mentia journey. Subcategories of transition processes sented by a daughter, 56, in caring for her father, 87. She
described by participants included the transition into de- stated: “…at one point he was on 20 to 22 prescription
mentia care, a continuous process of management and drugs per day, but you’d ask him, and he’d say, ‘No I
follow-up, and adjustment to a new home and reorienta- don’t take pills.’” These caregivers expressed worry that
tion. Four subcategories of influencing factors were identi- the health care system was not getting the information re-
fied within these processes: catalysts, buffers, facilitators, quired to properly assess the transition needs of the per-
and obstacles. son with dementia. Thus, conflicting realities may impact
the appropriateness of recommendations (e.g., long term
Transition context care placement) and referrals (e.g., to specialists).
Differing realities and goals: in conflict and alignment Similarly, conflicting goals were indicated to have
Conflicting realities often led to communication difficul- caused problems during transitions when participants
ties during transitions. One caregiver, 57, explained how felt that their views were not respected in the health careAshbourne et al. BMC Geriatrics (2021) 21:285 Page 6 of 13
team. Sometimes, system goals directly opposed and Parallel experiences
“outranked” the goals of persons with dementia and The final aspect of transition context was labeled paral-
their caregivers. One wife and caregiver, 68, described lel experiences, which are shaped by others’ anecdotes.
her conflict with system-level goals in a story about try- Rather than having a direct influence on care, parallel
ing to access home care support: experiences provide context because they affect percep-
tions of care experiences. Hearing about others’ experi-
Trying to book these events…[the coordinator’s] goals ences further along in the dementia journey allowed
were different than mine. Mine were to make [my participants to better understand what might happen to
husband] happy with the people that came, to try them: “The caregivers that we have, there’s different
and make it as few new faces as possible… Her goal stages. So you kind of get an understanding of what
was to have you be specific about the exact times might be down the road. Which is very nice to get feed-
that you would want those PSWs (personal support back from them” (wife/caregiver, 67). People used their
workers, a.k.a. nursing aides), and to have it a regu- interactions with others to learn about potential future
lar weekly booking. experiences, which may colour perceptions of impending
transitions.
In this scenario, system constraints were prioritized Individuals understood their own experiences in rela-
over her wishes, but this was not always the case: “They tion to anecdotes heard from others. When speaking of
didn’t have rules. They had ways of, rather than a rule, others’ negative experiences, participants reported feel-
they had a way of giving me support. They found a way” ing comparatively fortunate or lucky. For example, one
[wife (caregiver), 78]. When the system did accommo- caregiver noted: “We have been very lucky…‘cause I’ve
date the person living with dementia and their caregiver, heard some horror stories.” One daughter and caregiver,
they had more positive experiences. 61, expressed a similar sentiment: “I was surprised when
I do meet people and they seem to have all these chal-
lenges. We were just very fortunate… I’ve heard horror
The broader community stories. But never from my point of view.” Less negative
Many transitions occurred while persons with dementia experiences than those reported in others’ stories were
were living at home, and thus their communities were viewed in a more positive light in contrast. These paral-
considered an important part of their context. lel experiences are an important finding, as they indicate
Knowledgeable and supportive communities helped indi- how peer supports can help individuals prepare for and
viduals live well at home by supporting caregivers and cope with potentially difficult transitions.
sharing responsibility: “It made my life easier. I didn’t
have to be the…Helicopter mother…Or wife…When he Transition processes
was out walking I knew I had eyes on the street” (wife/ Pre-diagnosis and transition into the system
caregiver, 65). Participants relayed stories about several transition
Community support was greatly appreciated by both points during their care, starting with diagnosis and
caregivers and persons with dementia; it is thus import- transition into the care system. System entry was de-
ant that providers are aware of a family’s supports when scribed as either gradual or sudden, each presenting dif-
assessing them. One caregiver, 77, described how a pro- ferent issues. For some, a slow progression eased the
vider inquired about her community support during her transition into the system; they knew it was coming, so
husband’s transition out of hospital: “She noticed how he they had been mentally preparing for years. For others,
was and she said to me, ‘what help do you have at this gradual transition represented a failure of the health
home?’ And I said, ‘I don’t have any.’ And she said, ‘you care system to address their needs in a timely fashion. A
just take him right upstairs and say you’re not going wife and caregiver, 64, noted: “…it took… a long time to
home until you get help.’” Despite taking the initiative to convince [the family doctor] that [my husband] had
ask about support, the onus was placed on the caregiver memory issues.”
to find help, indicating that more could potentially be Some participants described feeling like they had been
done by the provider. By understanding the available waiting for a crisis to occur. When crises did occur,
community and family support systems, providers can people were “…propelled into the care that [they]
better understand the context of transitions and help fa- needed” (wife and caregiver, 57), suggesting a sudden
cilitate strong community support systems. These sup- entry into the system. Crises were often said to follow a
port systems may influence the need for transitions; for period of waiting for a diagnosis; however, in a few cases
example, caregivers who have more community support the diagnosis was also sudden and a surprise. For one
may delay a transition to a formal care environment, wife and caregiver, 72, “…it came as a shock when [my
such as long-term care. husband] was diagnosed.” Participants’ stories alsoAshbourne et al. BMC Geriatrics (2021) 21:285 Page 7 of 13
suggested that the perceptions of initiation of care are area: “Well, a lot of them up there… they’re all, on their
influenced by how they receive a diagnosis. This initial own… each one… so they got their own controls. I think
transition sets the stage for the rest of the journey it’s the biggest thing here.” Further, a lack of information
through the health care system, as a diagnosis can pro- transfer contributed to deficits in provider collaboration.
vide an entry to support services and treatment. For ex- A wife and caregiver, 78, noted: “We made sure our-
ample, one wife and caregiver, 64, stated: years. “[My selves. We didn’t just trust them, and it didn’t all just fall
husband] was diagnosed on a Friday. I called them on into place… They didn’t do it the way they said they
Monday, and by Thursday there was a…coordinator at would.”
our house…she has been by our side every step for the Regarding the goal of care continuity [44], one wife
last six years.” and caregiver, 80, explained, concerning her husband’s
care: “Having a doctor see [my husband] every six
Continuous management and follow-up aided by months… I know that someone has his journey on paper.”
coordination and continuity efforts Relatedly, participants indicated that maintaining
When responding to questions about the types to transi- consistency in providers was preferable: “You need a lit-
tions they had experienced, participants described transi- tle bit of continuity here with these poor people who don’t
tions in care after the initial diagnosis as a process of even know who they are themselves” [wife(caregiver), 68].
continuous management and follow-up. One wife and Another wife and caregiver, 68, described how
caregiver, 74, noted: consistency made the assessment process easier: “If you
have somebody who’s been here three times before, she’s
I mean our transitions have…from one thing it seems familiar with your file and she… didn’t have to start
to be…on-going…I don’t think that’s ever going to be down here all over again.”
at a standstill. Because of age and because of …some
of the medical diagnoses…it’s always going to be a Adjusting to a new home and reorientation
continuous transition. Although most care transitions were viewed as con-
tinuous, many participants indicated that moving to
Regarding his mother’s care experiences, one son (care- long-term care represented a distinct, difficult transi-
giver), 56, suggested that “it all flows together.” An indi- tion. One daughter and caregiver, 56, called it a “big
vidual with dementia remarked that his care consisted of step”, while a wife and caregiver, 77, noted that “it’s
“just visits to the doctor’s office, or the hospital, whatever no easy route.” Caregiver feelings of loss of control
comes first.” Another caregiver, 74, felt that her hus- contributed to its emotional significance: “It’s also
band’s transitions were so intimately linked that she was overwhelming to be in a position where you have to
“almost barely aware of the transitions.” Many care tran- face the fact that you cannot do it, and you have to
sitions may occur during the course of a journey with turn his care over to somebody else” [wife (caregiver),
dementia; however, these are often not considered 77]. When the father of a daughter and caregiver, 56,
discrete instances of movement from provider to pro- moved into long-term care, the environmental shift
vider. They are perceived as individuals’ reactions to was a major stressor for him as well:
changes in the dementia symptoms, in their needs, and
in their lives. He took a dive bomb as far as… understanding
During continuous transitions and adaptations, partici- things, being able to… he had no idea he was in
pants desired regular follow-up by those involved in [city]. Like, ‘when are we going back home’… like he
their care: “I think that they need to be the ones that are just dive bombed horribly and stayed that way for
following up, and checking maybe every six months to see many, many days.
where things are at” [wife(caregiver), 70]. Persons with
dementia and their caregivers often required ongoing Familiarization with the long-term care environment
care from several providers; therefore, efforts to ensure prior to the transition was suggested to ease the transi-
coordination and continuity of care helped connect the tion. One wife and caregiver, 72, suggested, “there might
transition processes. be some advantage to having him in [respite care] there
Important aspects of coordination included clear refer- because as the thing progresses, he will be stabilized in a
rals to appropriate services, professional collaboration, place that’s familiar.” When transitions to long-term
and information transfer. There was a perceived need care went smoothly, persons with dementia began to ad-
for providers to be aware of and refer to each other. Be- just and consider the facility their new home. One hus-
yond that, participants believed that providers should band and caregiver, 73, noted that positive experiences
work together to meet their needs. One caregiver, 67, allowed his wife’s long-term care facility to “become her
described a lack of collaboration among providers in her home.”Ashbourne et al. BMC Geriatrics (2021) 21:285 Page 8 of 13
A progression of dementia symptoms and the move to If you’re able to step back and take steps like getting
long-term care marked the need for reorientation or the powers of attorney, adjusting the household ar-
finding a new normal. One wife and caregiver, 65, indi- rangements…you become much more resilient, and
cated that she had trouble knowing what to do when she that resilience cushions you against… the next part
no longer had the full-time job of taking care of her hus- of that transition.
band: “What am I supposed to do with this time?” An-
other wife and caregiver, 72, said she had trouble Participants reported having to advocate for their own
transitioning from doing things together to doing them care while moving throughout the system. One person
alone: “We always discuss this together. I’ve got to make with dementia, 73, stated, “You have to be aggressive,
a decision all by myself… I’ve heard that other people say and if you’re not an aggressive type person then you’ll
that all of a sudden, ‘I’m just alone.’” One husband, 64, miss out on those things. You’ll just go by.” A wife and
described his transition into a new role and learning to caregiver, 84, illustrated the connection between self-
move on without his wife: “So now my transition is… the advocacy and the need for individuals to be educated
challenge for me transitioning as an individual, is how and prepared for health care encounters: “We’ve defin-
do I re-orient my life?” itely got to be our own advocates when we go to the doc-
tor’s. You’ve got to know a little bit about some stuff.”
People desired information about stages of dementia, fu-
Influencing factors ture transitions, and system processes.
Catalysts One wife and caregiver, 58, suggested that her know-
Participants described factors that led to their transi- ledge provided an advantage: “Knowing what the process
tions. Precipitating crises included falls, overdoses, heart is, and how lengthy it is, and knowing some of the little
attacks, surgeries, and major behavioural problems. One techniques to put yourself in a better advantage.” By
caregiver, 71, revealed that her husband had a heart at- gaining a better understanding of dementia and the
tack that worsened his dementia symptoms, thus, neces- health care system, participants were able to prepare for
sitating care outside of the home for a period of time: future transitions:
“When he had his heart attack, that spiked his dementia,
and he was really confused and didn’t know where he I knew I didn’t need anything at the time, but I just
was and what day it was and I could not bring him wanted to make sure that I had all of my research
home in that condition.” Events and crises in the lives of and homework done... When I do need assistance...
caregivers also precipitated transitions. One wife and I’m already in the system. (wife and caregiver, 64)
caregiver, 77, noted: “So then it came to the point where
I got a knee problem… So then I was booked for surgery. Facilitators
So then we decided that we’ll book him for the nursing Facilitators are factors that subjectively contributed to
home.” the success of transitions. Participants appreciated pro-
Not all transitions were preceded by major events or viders who were understanding and compassionate while
crises. Participants’ ability to manage at home changed also professional and skilled. Comments about provider
over time, leading to different care requirements. One attitudes often involved statements about providers’ pro-
wife and caregiver, 57, noted a change in coping, which fessionalism and expertise. One wife and caregiver, 80,
led her to have her husband assessed for home support: noted that her husband’s physician in the memory clinic
“we were getting to the point that we weren’t coping very was “a very gentle man and he always has time for you,”
well, which is why I made the call.” Similarly, another but also that “he’s the one who calls the shots,” suggest-
wife and caregiver, 72, began to have an increasingly dif- ing she valued both his attitude and his expertise.
ficult time with her husband’s eating problems, leading Participants recognized that the development of a
her to reach a tipping point: “I thought, well, I’ll take working relationship with a provider required effective
him home, and tomorrow I’m going to call her and tell engagement. One participant with dementia, 92, de-
her I can’t do this anymore, I just, I’ve reached the end.” scribed how his providers included him, along with his
caregiver in decision-making: “very cooperative in dis-
cussing things with us. Not saying you must do this.” A
Buffers wife and caregiver, 71, suggested that people with de-
Pre-transition proactivity and preparation can provide mentia should be given the right to participate in deci-
an emotional and physical buffer for care transitions. A sions: “So for the few that really are able to choose, I
husband and caregiver, 64, found that taking necessary think that they should let them.”
steps and preparing for the future allowed him to be- Caregivers suggested that it was important that the
come resilient to the transitions to come: health care system viewed persons with dementia in theAshbourne et al. BMC Geriatrics (2021) 21:285 Page 9 of 13
same way they are viewed by their loved ones: as people heterogeneity of transition experiences discussed by par-
with individual needs: “They’re still people” (wife and ticipants, it became clear that transitional care cannot be
caregiver, 68); “It’s important to see the person as the fully described by a series of actions taken to ensure that
person instead of as the disease” (wife and caregiver, 70). an individual moves seamlessly from one setting in the
Furthermore, one wife and caregiver, 74, believed that health care system to another, as it has been classically
the system should accommodate individual needs: “I defined [19]. Participants typically did not view transi-
think that they should be able to look at that and…make tions as discrete events that could be studied, assessed
it work for individual people.” Another caregiver, 56, re- and/or improved without an understanding of both their
vealed that her father’s transition into long-term care personal journey and the broader health care system.
was eased by the person-centered care he received: The theoretical framework presented in the results sec-
“They make it their business to know what that person tion aims to distil a multifaceted topic while respecting
did in their life and what’s important to them.” its complexity.
Many of the features of existing transitional care
Obstacles models and interventions are consistent with the results
Finally, transition obstacles are system, provider, or of this study. Coleman et al’s [45] Care Transitions
individual-level factors that hinder transitions. Transi- Intervention (CTI) is tailored to individual goals, indicat-
tions may be impeded by the complexity of the health ing consideration of the multiplicity of goals in health
care system and resulting confusion. Furthermore, the care practice. Both the CTI and Naylor and Van Cleave’s
health care system is also constrained by factors such as [46] Transitional Care Model consider factors such as
time, money, and strict regulations. follow-up, professional collaboration, provider
There was a perceived need for increased knowledge consistency, patient education, engagement, and person-
and education of providers: “I think that as time goes on centered care; all of which were also identified as im-
it is an area where more training is going to be needed portant in the theoretical framework. That said, these in-
with all staff. Because more and more of this is coming” terventions focus on specific transitions, typically a
(wife and caregiver, 65). Knowledge about rarer demen- hospital discharge or acute event [45–47]. The broad
tias was described as requiring improvement: “I feel that perspective adopted for this study facilitated the devel-
they do have some training… but more so it seems to me opment of a framework that elucidates aspects of several
that it’s more of an Alzheimer’s training” (daughter and types of transitions while respecting the continuous na-
caregiver, 68). ture of transition experiences. The theoretical frame-
Participants felt that their ability to successfully navi- work presents a novel contribution to the literature, as it
gate the health care system was hindered by information aims to avoid an over-simplification and does not as-
or communication deficits. One wife and caregiver, 72, sume a one-size-fits-all transitional care model.
felt her providers were withholding information from Effective transitional care has the potential to reduce
her: issues associated with fragmentation; however, reduc-
tionist thinking can be a significant barrier to the
So that’s what I mean by not always lying but just provision of care across the continuum. Complex sys-
holding information in. And I got that feeling all the tems theory has a natural application to the concept of
time that it was all private information and I had transitions. Cilliers [48] noted: “A complex system is not
the bloody nerve thinking I should be entitled to constituted merely by the sum of its components, but
stuff. also by the relationship between these components. In
‘cutting up’ a system, the analytical method destroys
When participants’ providers did not provide them with what it seeks to understand.” (p. 2). This study indicates
enough useful information, they felt they had to go look- that the complex nature of transitions must be
ing for it themselves, which contributed to their stress: respected; rather than reducing transitions to their indi-
“You have to go searching and that’s just one more thing vidual components, transitions are viewed by both per-
in the day” (wife and caregiver, 67). Participants emphat- sons with dementia and their caregivers as continuous
ically noted that engagement of persons with dementia, and are situated within a broader context. Despite being
and their caregivers, must begin with appropriate and asked to describe specific instances of transition, partici-
clear communication. pants tended toward describing their journey through
the health care system more broadly. Although some
Discussion specific transitions (i.e., the transition to long-term care)
It is clear from the diversity of information that arose stood out as distinct and important to participants, sep-
from the interviews that care transitions in the context arating the transition experience into discrete instances
of dementia are complex. Given the significant of movement in the health care system does notAshbourne et al. BMC Geriatrics (2021) 21:285 Page 10 of 13 adequately explain their experiences. Rather than con- buffers (e.g., proactive caregivers), facilitators (e.g., posi- stricting individuals to view transitions through the lens tive relationships with health care providers), and obsta- of previous studies and health care system norms, this cles (e.g., lack of awareness and training). In order to framework respects the reality presented by the appropriately intervene, and support persons on this participants. journey and through numerous complex transitions, Distinct from previous work on transitions for older practitioners must be aware of the unique blend of cata- persons [e.g., 45], our framework here urges both practi- lysts, buffers, facilitators and obstacles that each person tioners and researchers to think of health care transi- living with dementia faces. This observation, and the tions for persons with dementia not as events, but rather foundation of our model, is closely aligned with the another aspect of their dementia journey [49]. The de- principles of person-centered [52] and collaborative care mentia journey is a complex one, often with multiple [53]. transitions, and which the caregiver and person with de- Collaborative patient-centred practice, which “is de- mentia may experience differently. Both Coleman’s [e.g., signed to promote the active participation of each dis- 45] and Hirschman’s [50] programs include family care- cipline in patient care” [53], can play an important role givers, but in these articles, patients and family care- in addressing transition complexity. Encouraging collab- givers are generally referred to together, without oration across the care continuum rather than between differentiation. Our framework also emphasizes the par- discrete sets of providers can help to ensure that the allel experiences and differing realities and goals that provision of health care aligns with the way care is expe- occur within the context of dementia care. Misaligned rienced. Persons with dementia and their caregivers have priorities within dementia care have also been docu- individual goals, needs, and perspectives that must be mented in Gilmore-Bykovskyi et al.’s [26] study. During considered during care transitions. A commitment to re- transitions from hospital to skilled-nursing facilities, specting realities of individuals with dementia and nursing staff commented on the impact that misalign- adopting person-centered transitional care approaches ment in system-level pressures and goals between these can help ensure that system constraints do not over- settings had on the transition process for persons with shadow individual needs. This could ultimately enhance dementia [26]. Similarly, Richardson et al. [51], in a sys- quality of care for persons with dementia and limit the tematic review aiming to understand transition experi- occurrence of adverse events [22]. Consistent with For- ences of individuals with dementia from the perspectives tinsky & Downs [49], we agree that future work on care of key stakeholders, found that the perspectives of indi- transitions for persons with dementia must focus on im- viduals with dementia, their family members, and care proving the quality and experiences of care transitions, providers did not always match. Hospital pressures led and not simply focus our efforts on delaying or avoiding to rushed discharge practices and worse transition expe- transitions. Even with prevention and diagnostic efforts riences. Involvement of families and adequate communi- in place, persons living with dementia will experience cation between stakeholder groups facilitated successful transitions, and those charged with improving dementia transitions [51]. By including the perspectives of care- care must plan accordingly [49]. Individual and family givers and persons with dementia, our study further ex- engagement in care can also help providers gain an un- plored the idea of alignment in dementia care contexts. derstanding of the context of transitions, including the Varying realities and goals between caregivers and per- community and social support available to those navigat- sons with dementia led to difficulties during transitions. ing the system. Similar to Gilmore-Bykovsky and colleagues’ study [26], in this study wider health care system-level pressures Limitations and strengths and constraints at times conflicted with the care needs Limitations of this study included an overrepresentation of persons with dementia and their caregivers. We of well-supported female caregivers and of males with hypothesize that differing priorities and realities may dementia. Recruiting through Alzheimer Society Chap- also be true with older adults who are not living with de- ters and a Family Health Team may have yielded a sam- mentia, and this would be an important avenue of future ple more connected to community supports than an transitions research. In other work of our group, we in- average Canadian with dementia. Furthermore, during vestigated care transitions of older individuals with hip interviews, caregivers spoke more than their family fracture [18]; the resulting framework also differentiated members with dementia. Despite addressing individuals family caregivers as a specific area of focus, while recog- with dementia directly, persons with dementia often re- nizing overlap with other domains. ferred to their caregivers. Finally, approximately one Our framework also highlights that a dementia jour- quarter of participants reported an unclear diagnosis, ney, and transitions embedded within, is significantly though all identified with the umbrella term of dementia. impacted by a range of catalysts (often acute events), Whether it is related to a lack of clarity in terminology
Ashbourne et al. BMC Geriatrics (2021) 21:285 Page 11 of 13
used by providers or poor understanding on the part of Conclusion
the persons with dementia or caregivers, this hazy ex- This study extends current knowledge to include an in-
perience with diagnosis reflects participant realities, depth account of care transitions from the perspectives
which are considered paramount within a constructivist of individuals with dementia and their caregivers, who
paradigm. In practice, specific dementia diagnoses are have often been excluded from related research. Obtain-
based on constellations of symptoms and cognitive test- ing the perspectives of individuals with dementia is not
ing; therefore, the diagnostic uncertainty within the um- always easy, and their views do not always match those
brella of dementia observed in this study reflects the of their caregivers or their health care providers [56].
reality of many practitioners as well [54, 55]. Rather than We chose to adopt a constructivist outlook that
limiting the generalizability of the study, the broad inclu- respected these differing realities and perspectives, an
sion of persons who identify with a diagnosis of demen- idea that was central to transition context.
tia supports the generalizability of the results to a larger It is important to incorporate the perspectives of per-
population. sons with dementia and their caregivers into our know-
We did not conduct theoretical sampling for transi- ledge of the dementia journey. Understanding the
tion type because we found that participants often de- experiences of persons with dementia interacting with
scribed multiple transitions, and their transition the health care system can help facilitate a more holistic
experiences were not always distinct. Based on these understanding of care transitions, however, this study
initial observations, we used probing questions to fur- did not compare the care transitions of persons living
ther explain the elements of transitions that arose with dementia to those of persons without dementia.
during initial interviews rather than explicitly asking Due to the intimate link between participant stories and
about or sampling for specific transitions. We felt the dementia experience, the voices of persons with de-
that this approach respected the realities of the cross- mentia cannot be generalized to the voices of all other
system transitions experienced by those that were older adults. Care transitions were often associated with
interviewed. The heterogeneity of types of transitions stages of their dementia journey; the diagnosis, for ex-
described by participants made it difficult to provide ample, signified a transition into the system. Transitions
specific guidance on improving any one given transi- were interrelated and continuous when participants were
tion (e.g., hospital to home or home to long-term living at home; a transition into long-term care may be
care). However, this study does provide important in- required when the dementia had progressed significantly
formation about how individuals perceive their health [57].
system navigation more generally. The results respect The conceptualization of transitions developed in this
the realities of participants, who feel that their transi- study may be used to generate recommendations to im-
tions are less distinct and more fluid than tradition- prove dementia care across the continuum, in particular
ally perceived and defined in health care systems as local and national dementia strategies are presently
research. being developed and implemented [58, 59]. Given the
Criteria for evaluating grounded theory research significance of transitions for safety and caregiver stress,
outlined by Charmaz [32] were considered throughout improving care transitions may in turn improve the
the study design. Credibility was maintained through quality of care and quality of life for individuals living
gathering rich data, transcribing interviews verbatim, with dementia.
and ensuring that initial codes remained close to par-
ticipant wording. The study has met the criterion of Abbreviation
originality, as it addresses a gap in the literature. Res- ADLs: Activities of Daily living
onance with participants was ensured through mem-
ber checks, wherein researchers presented results to
Supplementary Information
participants for feedback. Nearly half of the partici- The online version contains supplementary material available at https://doi.
pants (n = 13) engaged in member checks, and every org/10.1186/s12877-021-02235-5.
individual agreed that the framework accurately and
comprehensively reflected their health care transition Additional file 1. Interview Guide.
experiences. As for the usefulness of the study, it has
added a new perspective of cross-system care transi-
Acknowledgements
tions from the perspectives of those with dementia We are grateful to Kathleen Pauloff and Veronica Sacco who helped with
and their caregivers. It is situated within the Ontario editing earlier drafts of this manuscript. We thank the Alzheimer Society
health care system; however, many of the elements Chapters and the Family Health Team that aided in recruitment of study
participants. Most of all, we are grateful to the older adults living with
deemed important by participants are likely more dementia, and their family members, who gave of their time to speak about
broadly generalizable. their health care experiences.Ashbourne et al. BMC Geriatrics (2021) 21:285 Page 12 of 13
Authors’ contributions 8. Bunn F, Burn AM, Goodman C, Rait G, Norton S, Robinson L, et al.
JA, PS, VB, and SM were involved in conceptualization and design of the Comorbidity and dementia: a scoping review of the literature. BMC Med.
study. JA was involved in data collection. JA, PS, and CT were involved in 2014;12(1):192. https://doi.org/10.1186/s12916-014-0192-4.
data analysis. JA, CT, PS drafted the article. VB and SM reviewed and revised 9. Aaltonen M, Raitanen J, Forma L, Pulkki J, Rissanen P, Jylhä M. Burdensome
the manuscript. All authors have read and approved the submitted version transitions at the end of life among long-term care residents with
of the manuscript. dementia. J Am Med Dir Assoc. 2014;15(9):643–8. https://doi.org/10.1016/j.ja
mda.2014.04.018.
Funding 10. Coleman EA. Falling through the cracks: challenges and opportunities for
Jessica Ashbourne was supported by an Ontario Graduate Scholarship and a improving transitional care for persons with continuous complex care
University of Waterloo President’s Scholarship. This project is funded in part needs. J Am Geriatr Soc. 2003;51(4):549–55. https://doi.org/10.1046/j.1532-
by St. Joseph’s Healthcare London. This research was completed 5415.2003.51185.x.
independently from the funding agencies; they had no role in determining 11. Manderson B, McMurray J, Piraino E, Stolee P. Navigation roles support
the study design, analysis, results or discussion. chronically ill older adults through healthcare transitions: a systematic
review of the literature. Health Soc Care Community. 2012;20(2):113–27.
https://doi.org/10.1111/j.1365-2524.2011.01032.x.
Availability of data and materials
12. National Association of Clinical Nurse Specialists: Definitions of translational
The datasets used and/or analysed during the current study are available
care. https://nacns.org/professional-resources/toolkits-and-reports/tra
from the corresponding author on reasonable request.
nsitions-of-care/definitions-of-transitional-care/#:~:text=The%20term%20%
E2%80%9Ccare%20transitions%E2%80%9D%20refers,a%20chronic%20or%2
Declarations 0acute%20illness (2020). Accessed 1 December 2020.
13. Callahan CM, Arling G, Tu W, Rosenman MB, Counsell SR, Stump TE, et al.
Ethics approval and consent to participate Transitions in care for older adults with and without dementia. J Am Geriatr
This study was performed according to the Helsinki Declaration and received Soc. 2012;60(5):813–20. https://doi.org/10.1111/j.1532-5415.2012.03905.x.
ethics clearance through the University of Waterloo Office of Research Ethics, 14. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and
ORE #20050. Written informed consent was obtained from all participants. severity of adverse events affecting patients after discharge from the
hospital. Ann Intern Med. 2003;138(3):161–7. https://doi.org/10.7326/0003-4
Consent for publication 819-138-3-200302040-00007.
Not applicable. 15. McMurray J, Hicks E, Johnson H, Elliott J, Byrne K, Stolee P. “Trying to find
information is like hating yourself every day”: the collision of electronic
Competing interests information systems in transition with patients in transition. Health Inform J.
The authors declare that they have no competing interests. 2013;19(3):218–32. https://doi.org/10.1177/1460458212467547.
16. Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW.
Author details Deficits in communication and information transfer between hospital-based
1 and primary care physicians: implications for patient safety and continuity
School of Public Health and Health Systems, University of Waterloo, 200
University Avenue West, Waterloo, ON N2L 3G1, Canada. 2School of Health of care. J Am Med Assoc. 2007;297(8):831–41. https://doi.org/10.1001/jama.2
and Life Sciences, Conestoga College Institute of Technology and Advanced 97.8.831.
Learning, Kitchener, Ontario N2G 4M4, Canada. 17. Clarfield AM, Bergman H, Kane R. Fragmentation of care for frail older
people—an international problem. Experience from three countries: Israel,
Received: 22 December 2020 Accepted: 15 April 2021 Canada, and the United States. J Am Ger Soc. 2001;49(12):1714–21. https://
doi.org/10.1046/j.1532-5415.2001.49285.x.
18. Stolee P, Elliott J, Byrne K, Sims-Gould J, Tong C, Chesworth B, et al. A
References framework for supporting post-acute care transitions of older patients with
1. Alzheimer Society of Canada. Rising tide: The impact of dementia on hip fracture. J Am Med Dir Assoc. 2019;20(4):414–9. https://doi.org/10.1016/j.
Canadian society Toronto (ON): Alzheimer Society. 2010. https://archive.a jamda.2019.01.147.
lzheimer.ca/sites/default/files/files/national/advocacy/asc_rising_tide_full_ 19. Coleman EA, Boult C. Improving the quality of transitional care for persons
report_e.pdf?_ga=2.245233477.1392387294.1606936718-1421201037.160693 with complex care needs. J Am Geriatr Soc. 2003;51(4):556–7. https://doi.
6718. Accessed 1 December 2020. org/10.1046/j.1532-5415.2003.51186.x.
2. Cipher DJ, Clifford PA. Dementia, pain, depression, behavioral disturbances, 20. Stolee P, Hillier LM, Cook S, Rockwood K. Cause, care, cure: research
and ADLs: toward a comprehensive conceptualization of quality of life in priorities for Alzheimer’s disease and related dementias. Can J Aging. 2011;
long-term care. Int J Geriatr Psychiatry. 2004;19(8):741–8. https://doi.org/10.1 30(04):657–67. https://doi.org/10.1017/S0714980811000523.
002/gps.1155. 21. Institute of Medicine. Performance measurement: accelerating
3. Andersen CK, Wittrup-Jensen KU, Lolk A, Andersen K, Kragh-Sørensen P. improvement. Washington (DC): The National Academies Press; 2006.
Ability to perform activities of daily living is the main factor affecting quality 22. Hirschman KB, Hodgson NA. Evidence-based interventions for transitions in
of life in patients with dementia. Health and Qual Life Outcomes. 2004;2(1): care for individuals living with dementia. Gerontologist. 2018;58(suppl_1):
52. https://doi.org/10.1186/1477-7525-2-52. S129–40.
4. Covinsky KE, Newcomer R, Fox P, Wood J, Sands L, Dane K, et al. Patient 23. Piraino E, Heckman G, Glenny C, Stolee P. Transitional care programs: who is
and caregiver characteristics associated with depression in caregivers of left behind? A systematic review. Int J Integr Care. 2012;12:132.
patients with dementia. J Gen Intern Med. 2003;18(12):1006–14. https://doi. 24. Coleman EA, Smith JD, Frank JC, Eilertsen TB, Thiare JN, Kramer AM.
org/10.1111/j.1525-1497.2003.30103.x. Development and testing of a measure designed to assess the quality of
5. Change Foundation. Health system navigators: band-aid or cure? 2013. care transitions. Int J Integr Care. 2002;2:1–9.
https://changefoundation.ca/wp-content/uploads/2016/05/TCF_Panorama_ 25. Jeffs L, Saragosa M, Law MP, Kuluski K, Espin S, Merkley J. The role of
Navigator_final.pdf. Accessed 1 December 2020. caregivers in interfacility care transitions: a qualitative study. Patient Prefer
6. Naylor MD, Hirschman KB, Bowles KH, Bixby MB, Konick-McMahan J, Adherence. 2017;11:1443–50. https://doi.org/10.2147/PPA.S136058.
Stephens C. Care coordination for cognitively impaired older adults and 26. Gilmore-Bykovskyi AL, Roberts TJ, King BJ, Kennelty KA, Kind AJ. Transitions
their caregivers. Home Health Care Serv Q. 2007;26(4):57–78. https://doi. from hospitals to skilled nursing facilities for persons with dementia: a
org/10.1300/J027v26n04_05. challenging convergence of patient and system-level needs. Gerontologist.
7. Gill SS, Camacho X, Poss JW. Community dwelling older adults with 2017;57(5):867–79.
dementia. In: Bronskill SE, Camacho S, Gruneir A, Ho MM, editors. Health 27. Zmora R, Statz TL, Birkeland RW, McCarron HR, Finlay JM, Rosebush CE, et al.
system use by frail Ontario seniors: an in-depth examination of four Transitioning to long-term care: family caregiver experiences of dementia,
vulnerable cohorts. Toronto, ON: Institute for Clinical Evaluative Sciences; communities, and counseling. J Aging Health. 2021;33(1–2):133–46. https://
2011. p. 47–69. doi.org/10.1177/0898264320963588.You can also read