HERPETISCHE UVEITIS FEBO-KURS - PROF. DR. MATTHIAS BECKER - SAOO KONGRESS 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Herpetische Uveitis
FEBO-Kurs
Prof. Dr. Matthias Becker
Seite 1 SAoO-Kongress 28.2.2018
Which one of the following concerning necrotizing herpetic retinitis (acute retinal necrosis) is false? 1. Anterior segment inflammation is variable. 2. Posterior segment inflammation is generally heavy. 3. The periphery of the retina is affected earlier and more severely than the posterior pole. 4. Retinal detachment occurs in up to three-quarters of cases. 5. Like other viral retinitides, affected patients are usually immunosuppressed. Seite 2 SAoO-Kongress 28.2.2018
Each of the following statements is true about valacyclovir except: 1. Valacyclovir acts as a “prodrug” because it is converted into acyclovir in the small intestine and liver. 2. Oral valacyclovir is substantially more bioavailable than oral acyclovir. 3. Valacyclovir may reduce the incidence of postherpetic neuralgia, if given within 72 hours of onset of symptoms. 4. Although a typical regimen for herpes zoster may be less expensive than acyclovir, the standard dosing of valacyclovir is more frequent than that for acyclovir. 5. Concurrent use of cimetidine can increase plasma concentrations of the active drug. Seite 3 SAoO-Kongress 28.2.2018
Cytomegalovirus (CMV) retinitis is the most common ocular manifestation of human immunodeficiency virus (HIV) infection. 1. TRUE 2. FALSE Seite 4 SAoO-Kongress 28.2.2018
In Übergängen denken… Seite 5 SAoO-Kongress 28.2.2018
Herpesviridae • Large family of DNA viruses (>130 herpesviruses) • Large double-stranded, linear DNA genomes • At least five species of Herpesviridae are extremely widespread among humans • More than 90% of adults have been infected with at least one of these • Latent form of the virus remains in most people Seite 6 SAoO-Kongress 28.2.2018

Herpesvirus types
Herpesvirus types known to infect humans:
1. Herpes simplex virus 1 (HSV-1)
2. Herpes simplex virus 2 (HSV-2)
3. Varicella-zoster virus (VZV)
4. Epstein–Barr virus (EBV)
5. Cytomegalovirus (CMV)
6. Human herpesvirus 6A (HHV-6A)
7. Human herpesvirus 6B (HHV-6B)
8. Human herpesvirus 7 (HHV-7)
9. Kaposi's sarcoma-associated herpesvirus (KSHV)
Seite 7 SAoO-Kongress 28.2.2018
Herpetic anterior Uveitis Seite 8
Zoster ophthalmicus
• Vesicles on the tip or
the side of the nose
• Hutchinson sign
• Precedes the
development of
uveitis
• Nasociliary branch of
N. V. innervates
both: cornea, lateral
dorsum of the nose
Courtesy of D. Goldstein,
BCSC
Seite 9 SAoO-Kongress 28.2.2018
Clinical signs (VZV, HSV) • VZV-uveitis: history of ipsilateral zoster ophthalmicus • Varicella-zoster sine herpete: anterior uveitis without prior cutaneous component • Variable corneal involvemet (keratouveitis) • Decreased corneal sensation (diffuse or localized) • Anterior, posterior synechiae • Hypopyon (hemorrhagic) Seite 10 SAoO-Kongress 28.2.2018
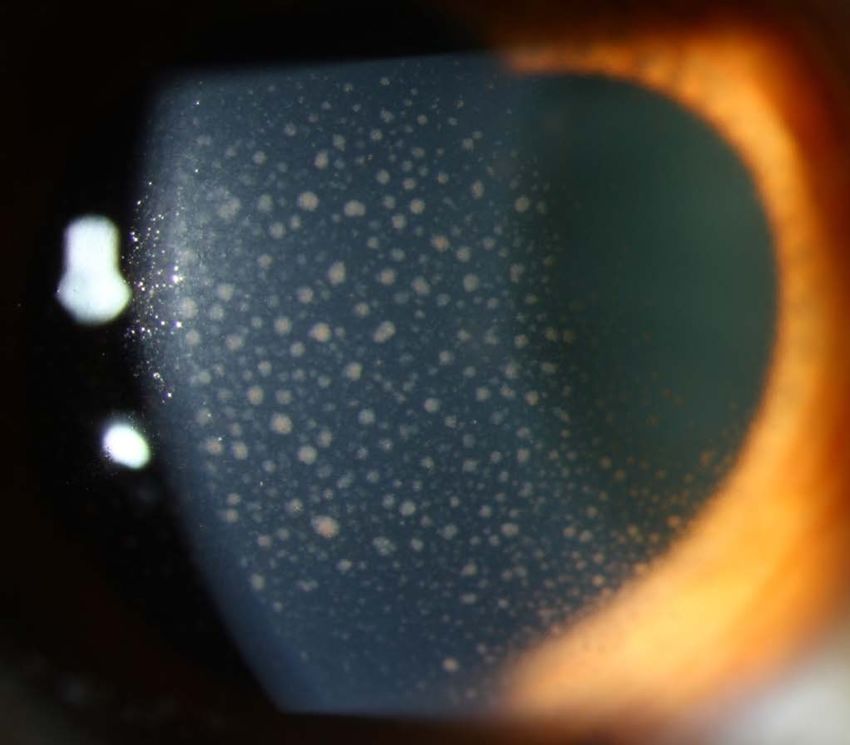
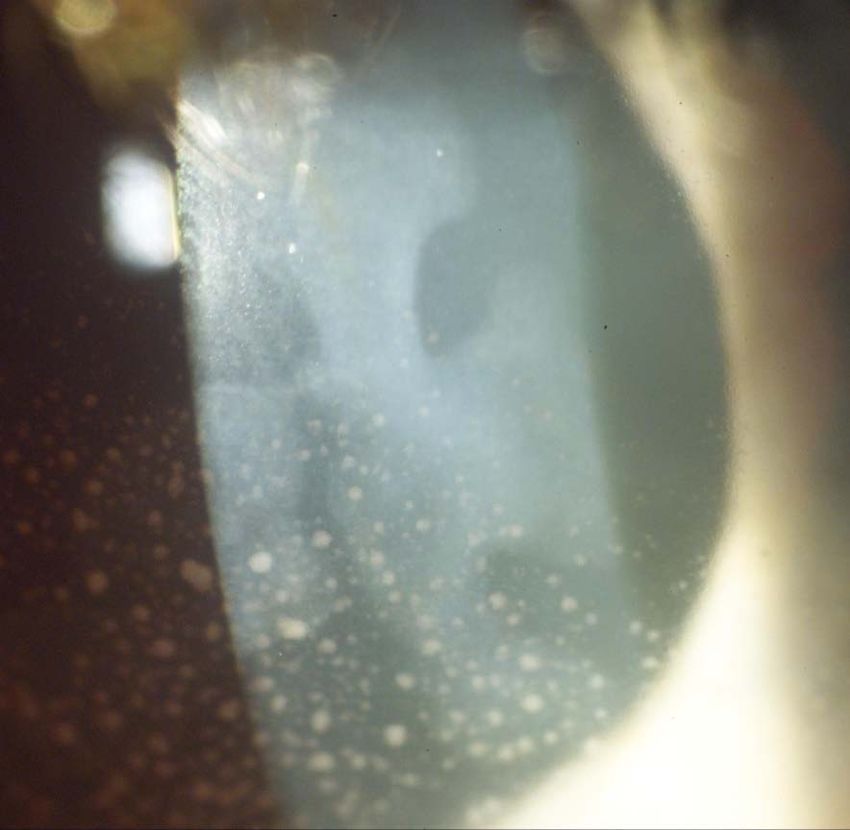
Übersicht Endothel-Präzipitate
Granulomatös („speckig“)
• Sarkoidose, Tuberkulose, MS (beidseitig)
• Herpetische Uveitis (einseitig)
Nicht-granulomatös
• Fein
• Ankylosierende Spondylitis, HLA-B27+ AAU
• Sternförmig-diffus
• Fuchs Uveitis Syndrom
SAoO-Kongress 28.2.2018DD: Präzipitate - granulomatös SAoO-Kongress 28.2.2018
DD: Nicht-granulomatös / fein SAoO-Kongress 28.2.2018
DD: Nicht-granulomatös/ sternförmig SAoO-Kongress 28.2.2018
Keratic precipitates
• Large, central greasy
• Fine stellate, diffusely
distributed
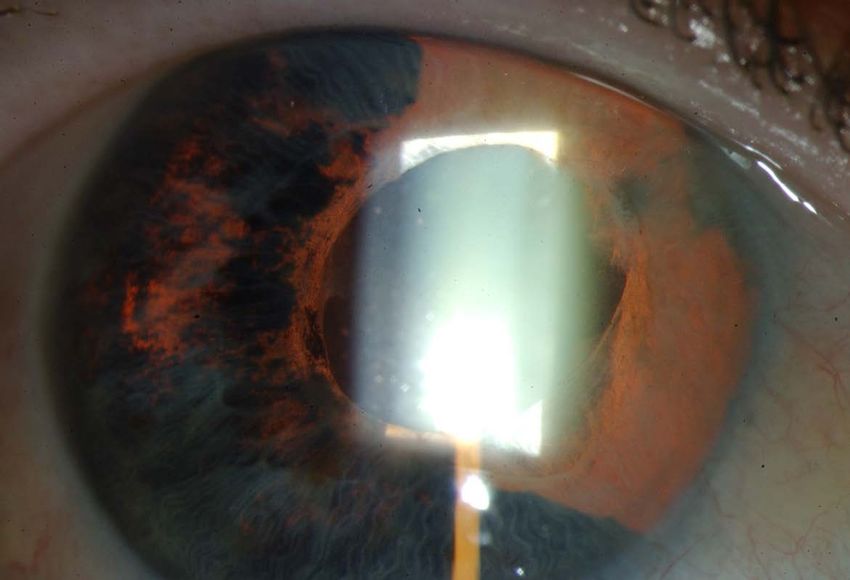
Seite 15 SAoO-Kongress 28.2.2018Iris atrophy
• Patchy or sectoral
• Pupil dilated
Atrophy of iris
pigment epithelium
not just anterior
stroma
Seite 16 SAoO-Kongress 28.2.2018Ocular hypertension • Trabeculitis • Frequent complication (DD: toxoplasmosis) • Other uveitides: decreased IOP (ciliary body hyposecretion) Seite 17 SAoO-Kongress 28.2.2018
Clinical signs (CMV) • Immunocompetent adults • Chronic or recurrent, unilateral, anterior uveitis, mild AC activity • Ocular hypertension • Corneal edema • Variable degrees of sectoral iris atrophy • No corneal scars, no posterior synechiae, no flare or fibrin and no posterior segment involvement Seite 18 SAoO-Kongress 28.2.2018
CMV • Fails to respond to corticosteroids and high doses of acyclovir • Can present as acute relapsing hypertensive anterior uveitis, also known as Posner-Schlossman syndrome (PSS); half of all presumed cases of PSS are CMV- positive Seite 19 SAoO-Kongress 28.2.2018
Epstein-Barr Virus • Associated with infectious mononucleosis (IM), Burkitt lymphoma, nasopharyngeal carcinoma, Hodgkin disease, and Sjögren syndrome • Primary infection in the context of IM: mild, self-limiting follicular conjunctivitis • Most ocular disease is self-limiting and does not require treatment • Topical corticosteroids and cycloplegia Seite 20 SAoO-Kongress 28.2.2018
Diagnostic options • Aqueous tap • Real-time PCR analysis • Goldmann-Witmer coeffizient Seite 21 SAoO-Kongress 28.2.2018
Therapeutic management: Topical • Corticosteroids • Cycloplegics • Antiviral drugs (Zovirax) for keratouveitis (to prevent dendritic keratitis as a complication of topical corticosteroid therapy) • Prolonged topical antiviral therapy is associated with the development of keratopathy Seite 22 SAoO-Kongress 28.2.2018
Therapeutic management: Systemic HSV or VZV (higher doses) : • Acyclovir (Zovirax, 400– 800 mg, 5 times/day) • Valacyclovir (Valtrex, 500 mg to 1 g, 2 times/day) • Famciclovir (Famvir, 250–500 mg, 3 times/day) Seite 23 SAoO-Kongress 28.2.2018
Prophylactic therapy HSV: • Acyclovir, 400 mg 2 times/day • Valacyclovir, 500 mg/day VZV • Acyclovir, 800 mg 2 times/day • Valacyclovir, 1 g/day Immunization • VZV (Zostavax) Seite 24 SAoO-Kongress 28.2.2018
Take home message
• Diagnosis often made clinically
• Viable therapeutic options available
• Role of corticosteroids
• Sometimes long-term therapy necessary
Seite 25 SAoO-Kongress 28.2.2018Herpetic posterior Uveitis
Clinical manifestations
• Viral retinitis
• Spectrum of necrotizing herpetic retinopathies
• Vasculitis
• Anterior segment ischemia
• Retinal artery occlusion
• Scleritis
• Vasculitis in the orbit: cranial nerve palsies
Seite 27 SAoO-Kongress 28.2.2018Necrotizing herpetic retinopathies
• Spectrum
• Rapidly progressing
• Clinical picture depends upon host’s immune status:
• Immunocompetent:
• Peripheral necrotizing retinitis accompanied by vasculitis, iridocyclitis,
and vitritis (ARN)
• Immunocompromised:
• Necrotizing retinitis, may rapidly involve the macula + peripheral retina
• without significant intraocular inflammation or vasculopathy (PORN)
Seite 28 SAoO-Kongress 28.2.2018Acute Retinal Necrosis (ARN)
• Immunocompetent patients
• Most common cause of ARN syndrome is VZV, followed
by HSV-1, HSV-2, and rarely CMV
• Patients with ARN due to HSV-1 and VZV tend to be
older, while those with HSV-2 tend to be younger
Van Gelder RN, Willig JL, Holland GN, et al.
Ophthalmology. 2001;108:869
Seite 29 SAoO-Kongress 28.2.2018Diagnostic criteria (ARN)
American Uveitis Society (AUS) criteria
• Single or multiple areas of retinal necrosis with distinct borders
• Necrotic foci usually located in peripheral retina
• Rapid disease progression if antiherpetic treatment not instituted
• Extension of foci of retinal necrosis in a circumferential fashion
• Presence of occlusive vasculopathy with arteriolar involvement
• Prominent anterior chamber and vitreous inflammation
• Characteristics that support but are not required for diagnosis: Optic
neuropathy or atrophy, scleritis, pain
Holland GN Am J Ophthalmol. 1994;117:663
Seite 30 SAoO-Kongress 28.2.2018http://eyewiki.aao.org/Acute_retinal_necrosis Seite 31 SAoO-Kongress 28.2.2018
Seite 32 SAoO-Kongress 28.2.2018
DD ARN FAST SLOW • Progressive outer retinal • Syphilis necrosis (PORN) • Intraocular lymphoma or • CMV retinitis leukemia • Atypical toxoplasmosis • Sarcoidosis • Acute multifocal hemorrhagic • Sympathetic ophthalmia retinal vasculitis • Vogt-Koyanagi-Harada • Bacterial/Fungal retinitis or syndrome endophthalmitis • Collagen-vascular disease • Autoimmune retinal vasculitis • Retinoblastoma • Behçet‘s disease • Ocular ischemic syndrome • Commotio retinae • Central or branch retinal artery occlusion Seite 33 SAoO-Kongress 28.2.2018
Progressive outer retinal necrosis (PORN) • Morphologic variant of acute necrotizing herpetic retinitis, profoundly immunosuppressed • Most often in advanced AIDS (CD4+ T lymphocytes ≤50 cells/μL) • VZV infection most common cause • Posterior pole may be involved early in the course of the disease, vitreous inflammatory cells are typically absent, and the retinal vasculature is minimally involved, at least initially • PORN in HIV: history of cutaneous zoster (67%) and eventually incur bilateral involvement (71%) Seite 34 SAoO-Kongress 28.2.2018
PORN • Similarly high rate (70%) of retinal detachment as in ARN • 2/3 final visual acuity of no light perception • Often resistant to treatment with intravenous acyclovir alone, successful with combination systemic and intraocular therapy using foscarnet and ganciclovir Seite 35 SAoO-Kongress 28.2.2018
Cytomegalo-Virus (CMV) Retinitis • Human immunodeficiency virus (HIV) retinopathy is the most common ocular manifestation of patients with acquired immunodeficiency syndrome (AIDS), and occurs in 50% of cases. • Most common viral manifestation of both congenital CMV infection and of CMV as an opportunistic coinfection in HIV/AIDS • Combination antiretroviral regimens (HAART) resulted not only in a significant decline in HIV/AIDS–associated mortality, but also in an 80% decline in new cases per year of CMV retinitis and its complications • 3 distinct variants: Seite 36 SAoO-Kongress 28.2.2018
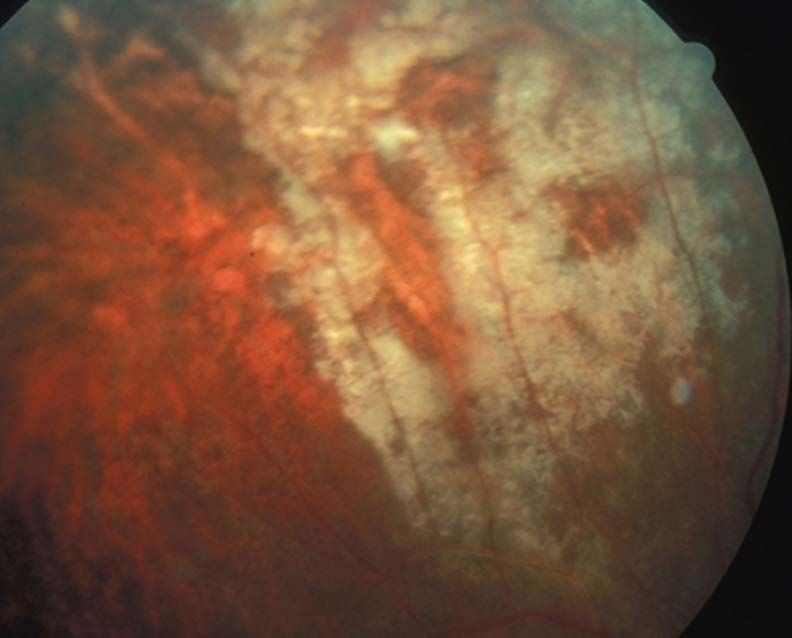
CMV Type 1: Classic or Fulminant • Large areas of retinal hemorrhage against a background of whitened, edematous, or necrotic retina • Typically appears in the posterior pole, from the disc to the vascular arcades, in the distribution of the nerve fiber layer, and associated with blood vessels Seite 37 SAoO-Kongress 28.2.2018
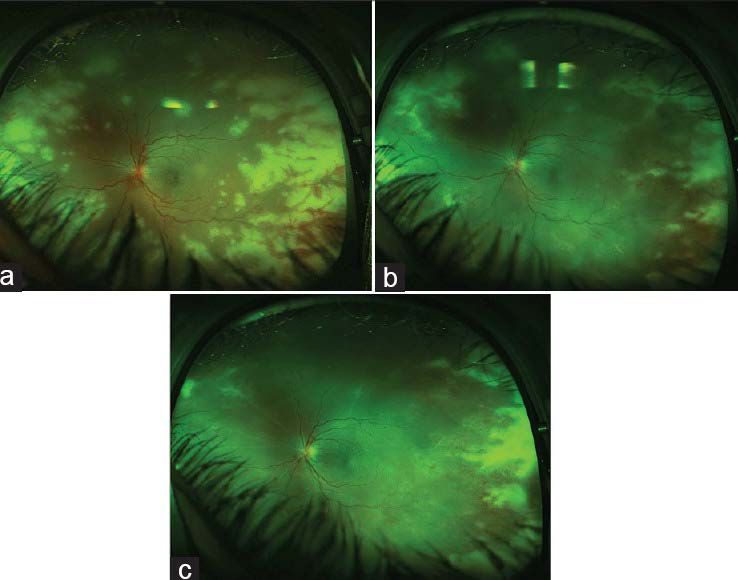
CMV Type 2: Granular or Indolent
• Retinal periphery
• Little or no retinal edema, hemorrhage, or vascular
sheathing
• With active retinitis progressing from the borders of the
lesion
Courtesy of C. Lowder
BCSC
Seite 38 SAoO-Kongress 28.2.2018CMV Type 3: Perivascular
• Variant of “frosted-branch” angiitis
Courtesy of A Vitale
BCSC
Seite 39 SAoO-Kongress 28.2.2018CMV ARN • Immunocompromised • Immunocompetent • Posterior pole along • Initially peripheral, later vessels posterior pole • Hemorrhage (pizza pie) • Hemorrhage less severe • No vitritis • Severe vitritis • Periphlebitis • Occlusive arteriolitis • Valganciclovir, ganciclovir • Valaciclovir, aciclovir Seite 40 SAoO-Kongress 28.2.2018
EBV-induced posterior uveitis
• Isolated optic disc edema and optic neuritis
• Macular edema
• Retinal hemorrhages
• Retinitis
• Punctate outer retinitis
• Choroiditis
• Multifocal choroiditis and panuveitis (MCP)
• Pars planitis and vitritis
• Progressive subretinal fibrosis
• Secondary choroidal neovascularization (CNV)
Seite 41 SAoO-Kongress 28.2.2018Intraocular fluid / tissue analysis • Aqueous tap • Diagnostic vitrectomy • Retinal biopsy Seite 42 SAoO-Kongress 28.2.2018
Polymerase chain reaction (PCR)
• May detect minute quantities of herpetic DNA
• Most sensitive, specific, and rapid diagnostic method
• Vitreous an aqueous samples
• Has largely supplanted viral culture, intraocular antibody
titers, and serology
• Quantitative PCR-based tests may provide additional
information
• viral load
• disease activity
• response to therapy
Seite 43 SAoO-Kongress 28.2.2018Goldmann-Witmer (GW) coefficient • Ratio > 3 is diagnostic of local antibody production to a specific microbial pathogen • Adjunct to the diagnosis of HSV and VZV uveitis • Little value for CMV retinitis • Combining GW coefficient with PCR analysis Seite 44 SAoO-Kongress 28.2.2018
Medical Management
The goals of treatment of ARN
1. Stop the retinal necrosis in order to avoid the late
consequences of the disease (retinal detachment and
optic atrophy)
2. Minimize the collateral damage caused by severe
inflammation and vascular occlusions
3. Protect the fellow eye (second eye involvement 3-35%,
usually within 6 weeks of disease onset, BARN)
Antiviral therapy should begin immediately after the
clinical diagnosis is made, rather than waiting for
results of laboratory testing!
Seite 45 SAoO-Kongress 28.2.2018General therapeutic considerations • Initiation of oral antiviral therapy at the onset of uveitis • Prolonged corticosteroid therapy with very gradual tapering • Topical corticosteroids: very long-term, albeit extremely low doses (1 drop per week) • Prednisone (0.5-2.0 mg/kg/day orally for up to 6-8 weeks) initiated 24-48 hours after the start of antiviral therapy or once regression of retinal necrosis been demonstrated • Long-term, suppressive, low-dose antiviral therapy may be indicated • Aspirin may minimize vascular thrombosis and propagation of further retinal ischemia and necrosis Seite 46 SAoO-Kongress 28.2.2018
HSV and VZV 1. Intravenous acyclovir, 10 mg/kg every 8 hours for 10– 14 days (check serum creatinine and liver enzymes) 2. After 24–48 hours systemic corticosteroids (prednisone, 1 mg/kg/day) are introduced to treat active inflammation and are subsequently tapered over several weeks 3. Acyclovir at 800 mg orally 5 times daily, Valacyclovir at 1 g orally 2-3 times daily, or famciclovir at 500 mg orally 3 times daily should be continued for 3 months (HSV oral dose is one-half of that for VZV) 4. Extended antiviral therapy may reduce the incidence of contralateral disease or bilateral ARN by 80% over 1 year. Seite 47 SAoO-Kongress 28.2.2018
Medical management: CMV
• Intravenous
• Ganciclovir (Cymevene®, 5 mg/kg twice daily)
• Foscarnet (Foscavir®, 90 mg/kg twice daily) for 2
weeks
• Low-dose daily maintenance therapy or oral
valganciclovir (900 mg twice daily) for 3 weeks
• Maintenance therapy (900 mg/day)
Seite 48 SAoO-Kongress 28.2.2018Antiviral agents intravitreally Especially if retinitis (HSV, VZV, CMV) is threatening the macula or optic disc: • Ganciclovir (Cymevene®, 200 - 2000 µg per 0.1 ml) • Foscarnet (Foscavir®, 1.2 - 2.4 mg per 0.1 ml) Seite 49 SAoO-Kongress 28.2.2018
Therapy EBV • Systemic corticosteroids • Efficacy of systemic antiviral therapy for EBV infection has not been established Seite 50 SAoO-Kongress 28.2.2018
Surgical Management
• Large retinal breaks frequently develop in areas of retinal
necrosis
• Tractional–rhegmatogenous retinal detachment in 50-
75% of patients with ARN
• Exudative retinal detachment may arise with severe
inflammation
• Prophylactic laser photocoagulation
• posterior to the area of retinitis
• 360°-barrier retinal photocoagulation delay laser until retinal
detachment necessitates surgery
• Prophylactic vitrectomy, esp. when PVD occurs
• Vitrectomy, endolaser, silicon oil
Seite 51 SAoO-Kongress 28.2.2018Complications
Many cases finally have less than 20/200 due to
• Vitreous hemorrhage
• Retinal holes and tears
• Retinal detachment
• Macular pucker
• Proliferative vitreoretinopathy (PVR)
• Optic neuropathy
• Encephalitis, dementia
Untreated, ca. 2/3 final V/A of 20/200 or worse
Treated, ca. ½ final V/A of 20/40 or better; 92% better than
20/400
Seite 52 SAoO-Kongress 28.2.2018Take Home Message • Outcomes of posterior entities may be devastating • Prognosis for patients with severe immune dysfunction remains guarded • Early diagnosis and treatment remains the key to successful management Seite 53 SAoO-Kongress 28.2.2018
Which one of the following concerning necrotizing herpetic retinitis (acute retinal necrosis) is false? 1. Anterior segment inflammation is variable. 2. Posterior segment inflammation is generally heavy. 3. The periphery of the retina is affected earlier and more severely than the posterior pole. 4. Retinal detachment occurs in up to three-quarters of cases. 5. Like other viral retinitides, affected patients are usually immunosuppressed. Seite 54 SAoO-Kongress 28.2.2018
Each of the following statements is true about valacyclovir except: 1. Valacyclovir acts as a “prodrug” because it is converted into acyclovir in the small intestine and liver. 2. Oral valacyclovir is substantially more bioavailable than oral acyclovir. 3. Valacyclovir may reduce the incidence of postherpetic neuralgia, if given within 72 hours of onset of symptoms. 4. Although a typical regimen for herpes zoster may be less expensive than acyclovir, the standard dosing of valacyclovir is more frequent than that for acyclovir. 5. Concurrent use of cimetidine can increase plasma concentrations of the active drug. Seite 55 SAoO-Kongress 28.2.2018
Cytomegalovirus (CMV) retinitis is the most common ocular manifestation of human immunodeficiency virus (HIV) infection. 1. TRUE 2. FALSE Seite 56 SAoO-Kongress 28.2.2018
Thank you! SAoO-Kongress 28.2.2018
You can also read