Identification and Prevention Pressure Ulcers in the ED - Evidence Based Practice Project UC Davis Medical Center's Nurse Residency Program Janine ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Identification and
Prevention
Pressure Ulcers in the ED
Evidence Based Practice Project
UC Davis Medical Center’s Nurse Residency Program
Janine Taylor R.N., B.S.N.
Peg Freitag R.N., B.S.N.Hospital Acquired Pressure
Ulcers (HAPUs)
• Patient safety, quality of care, and the
patient’s (and family’s) perception of both
have become a major driver for the
establishment of best practices.
• CMS no longer reimburses for “never”
events, events they have designated as
entirely preventable (Centers for Medicare
and Medicaid Services, 2008).Prevalence • Approximately 2.5 million patients are treated for pressure ulcers in acute care facilities in the United States annually, and approximately 60,000 patients die each year of complications related to pressure ulcers (PU). (Tschannen,et al., 2012).
What does this have to do with the
Emergency Department (ED)?
• The ED is the single greatest point of entry into
the hospital (Denby & Rowlands, 2010).
• Wait times in EDs are increasing as patient
demographics increasingly shift from life-
threatening conditions to acute and critical
illnesses
– Pressure ulcers can develop in only a few hours
– The equipment and supplies used in the ED are often
not designed with reduction of HAPUs in mind
(Naccarato & Kelechi, 2011).So What Can We Do? First step is understanding the risk factors and utilizing the nursing process to assess each patient as to what their individual risk is.
Risk Factors • Alderden, et al. (2011), in their retrospective analysis of HAPUs compiled the following risk factors (see Table 1): – Braden Score 65 – Diabetes – Prior recent hospital stay – Emergent admission to the ICU – BMI 35
Risk Factors, cont. • Other risk factors include (Tschannen, et al., (2012) – Recent Cardiac Arrest – SHOCK/Sepsis – Hx of pressure ulcers – Current redness in area – Going to the OR? Multiple procedures > 6 hrs – Quad/Para/Hemiplegic – Stroke/Paralysis
Best Practice Intervention • Most HAPUs are located in just three areas: heels, sacrum, and coccyx (Denby & Rowlands, 2010). • The Institute for Clinical Systems Improvement has identified several key interventions to promote PU prevention, including minimizing/eliminating friction and shear, minimizing pressure, providing support surfaces, managing moisture, and ensuring the patient maintains adequate nutrition/hydration (2012).
Additional Interventions • UC Davis Medical Center O.R. unit already uses Mepilex borders prophylactically on pts to help prevent the development of HAPUs. • Case studies indicate this is a cost-effective intervention with significant real-world results.
Case Studies • In Connecticut, an ICU that began to use Mepilex (the brand of silicon foam dressing UC Davis utilizes) in their ICU saw sacral HAPU incidence decrease from 12.5% to 7% in one year (Walsh et al., 2012). • A Chicago ICU saw an even more significant reduction going from 13.6% to 1.8% during a 6-month prospective study utilizing Mepilex (Chaiken, 2012).
What’s the Goal? • The purpose of this project is to prevent further damage to existing pressure ulcers and to prevent the development of pressure ulcers in those patients found to be at risk. • The recommendations for the use of preventative measures are part of an evidence-based care plan.
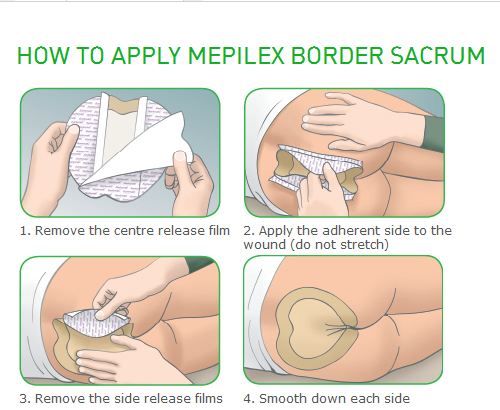
What should We Do? • While routine use of a silicone border foam dressing should not be the only intervention employed to reduce HAPU in the ED, it should become standard practice for any patient who meets the criteria for being at risk for potentially developing a pressure ulcer to have a Mepilex foam dressing applied to the sacrum, pelvic area, occiput or heels • This is an economically sound measure to prevent the development of a HAPU, and to prevent further damage to an existing PU.
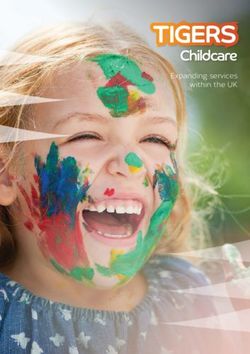
Let’s Make it Easy • ‘Best Practice’ means nothing if not used • “quick card” reference guide to identify the at risk patient population as part of the assessment • Apply the Mepilex Borders when appropriate. • The “quick card” should serve to raise awareness of the importance of the application of the dressing and the patients with which the dressing is appropriate.
Quick Card
FRONT BACK
Apply Mepilex to all patients with:
• Recent Cardiac Arrest
• Vasopressor Rx > 48 hrs
• SHOCK and/or Sepsis
• Hx of pressure ulcers
• Current redness in area
• Emergent OR or ICU dispositions
• Quad/Para/Hemiplegic
• Stroke/Paralysis
And to pts with 3 or more of the below criteria :
• Ages 65 -70 or above
• Fecal or urinary incontinence
• Prolonged bed rest = or > 4 hrs AND unable to shift
weight, independently
• Diabetes Remember to:
• BMI above 35 or less than 25 Date, time, and initial with a marker on
• Liver failure
• Renal failure
Mepilex Border prior to application And
• Braden Score below 18 Note application of Mepilex Border in EMR
• Weeping edema or anasarca
• Malnutrition (albumin at or below 2.5)References:
Alderden, J., Whitney, J. D., Taylor, S. M., & Zaratkiewicz, S. (2011). Risk profile characteristics associated with
outcomes of Hospital-Acquired Pressure Ulcers: A retrospective review. Critical Care Nurse, 31(4), 30-43.
doi:10.4037/ccn2011806
Centers for Medicare and Medicaid Services. Medicare and Medicaid move aggressively to encourage greater
patient safety in hospitals and reduce never events [press release]. July 31, 2008.
https://www.cms.gov/apps/media/press/release.asp?Counter=3219&intNumPerPage=10&checkDate=&c
heckKey=&srchType=1&numDays=0&srchOpt=0&srchData=&keywordtype=All&chkNewsType=1%2C+2%2
C+3%2C+4%2C+5&intPage=&showAll=1&pYear=1&year=2008&desc=false&cboOrder=date.
Chaiken, N. (2012). Reduction of sacral pressure ulcers in the Intensive Care Unit using a silicone border foam
dressing. Journal of Wound, Ostomy and Continence Nursing, 39(2), 143–145.
doi:10.1097/WON.0b013e318246400c
Denby, A., & Rowlands, A. (2010). Stop them at the door: should a pressure ulcer prevention protocol be
implemented in the emergency department?. Journal of Wound, Ostomy & Continence Nursing, 37(1), 35-
38. doi:10.1097/WON.0b013e3181c68b4b
Institute for Clinical Systems Improvement. (2012). Pressure ulcer prevention and treatment: Health care
protocol. Institute for Clinical Systems Improvement (ICSI).
Naccarato, M., & Kelechi, T. (2011). Pressure ulcer prevention in the Emergency Department. Advanced
Emergency Nursing Journal, 33(2), 155-162. doi:10.1097/TME.0b013e3182157743
Tschannen, D., Bates, O., Talsma, A., & Ying, G. (2012). Patient-specific and surgical characteristics in the
development of pressure ulcers. American Journal Of Critical Care, 21(2), 116-125.
doi:10.4037/ajcc2012716
Walsh, N., Blanck, A., Smith, L., Cross, M., Andersson, L., & Polito, C. (2012). Use of a sacral silicone border
foam dressing as one component of a pressure ulcer prevention program in an intensive care unit setting.
Journal Of Wound, Ostomy & Continence Nursing, 39(2), 146-149. doi:10.1097/won.0b013e3182435579You can also read