IMPLEMENTING THE 2017-2021 FRAMEWORK FOR VOLUNTARY MEDICAL MALE CIRCUMCISION - MALE CIRCUMCISION FOR HIV PREVENTION
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MALE CIRCUMCISION FOR HIV PREVENTION
MEETING REPORT
IMPLEMENTING THE
2017–2021 FRAMEWORK
FOR VOLUNTARY MEDICAL
MALE CIRCUMCISION
27 FEBRUARY–1 MARCH 2017
MALE CIRCUMCISION FOR HIV PREVENTION — IMPLEMENTING THE 2017–2021 FRAMEWORK FOR VOLUNTARY
MEDICAL MALE CIRCUMCISION 27 FEBRUARY–1 MARCH 2017, MEETING REPORT
ISBN : 978-929023405-0
© WHO Regional Office for Africa 2017
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike
3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes,
provided the work is appropriately cited, as indicated below. In any use of this work, there should be no
suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not
permitted. If you adapt the work, then you must license your work under the same or equivalent Creative
Commons licence. If you create a translation of this work, you should add the following disclaimer along with the
suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not
responsible for the content or accuracy of this translation. The original English edition shall be the binding and
authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation
rules of the World Intellectual Property Organization.
Suggested citation. Male Circumcision for HIV Prevention — Implementing the 2017–2021 Framework for
Voluntary Medical Male Circumcision 27 February–1 March 2017, Meeting Report. Brazzaville: World Health
Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit
requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as
tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and
to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-
owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not
imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted
and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed
or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and
omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication.
However, the published material is being distributed without warranty of any kind, either expressed or implied.
The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be
liable for damages arising from its use.
Printed in the WHO Regional Office for Africa, Brazzaville, Republic of Congo
i
CONTENTS
Acknowledgementsii
List of acronyms ii
List of acronyms of organizations 1
Introduction2
Background3
Meeting objectives 3
Presentations, summaries and priority actions 4
Day 1 4
Day 2 13
Day 3 27
Meeting conclusions 38
Annex 1. – Youth advocacy brief 39
Annex 2. – List of participants 41
LIST OF FIGURES
Figure 1: Key milestones in VMMC for HIV prevention 4
Figure 2: Overview of VMMC implementation progress in 14 countries in eastern and southern Africa 5
Figure 3. N
umber of VMMCs conducted through 2015 in 14 priority African countries, with estimated target number
required to reach 80% male circumcision 5
Figure 4: Decrease in VMMC uptake by age in Tanzania 7
Figure 5: Malawi national policy documents 8
Figure 6: Global HIV targets 9
Figure 7: Relative impact of scaling up VMMC – based on modelling 10
Figure 8: UNAIDS Fast-Track MC targets 10
Figure 9: Years of life lost among men in eastern and southern Africa, according to age group and cause (2013) 11
Figure 10: Influences and stages of the journey to VMMC 13
Figure 11: Overview of implementation science studies in Tanzania, Kenya and South Africa 14
Figure 12: HIV testing results for VMMC clients at male clinic in Scott Hospital, Lesotho 15
Figure 13: Defining and locating the world of work 16
Figure 14: VMMC among men aged 20–29 years in 2015 and 2016, by priority country in Africa 17
Figure 15: Results of policy scans by Sonke Gender Justice 18
Figure 16: Current activities in the ASRH–VMMC Linkages pilot project, Zimbabwe 20
Figure 17: Successes of the Youth Psychosocial Support Programme in South Africa 23
Figure 18: Scale and sustainability of using soccer to increase uptake of VMMC 24
Figure 19: Community entry model and elements of Lihawu Camps 25
Figure 20: Key actors for sustainability of VMMC programmes 29
Figure 21: Conclusions on condoms and VMMC 30
Figure 22: Decision-making around the introduction of the human papilloma virus vaccination 31
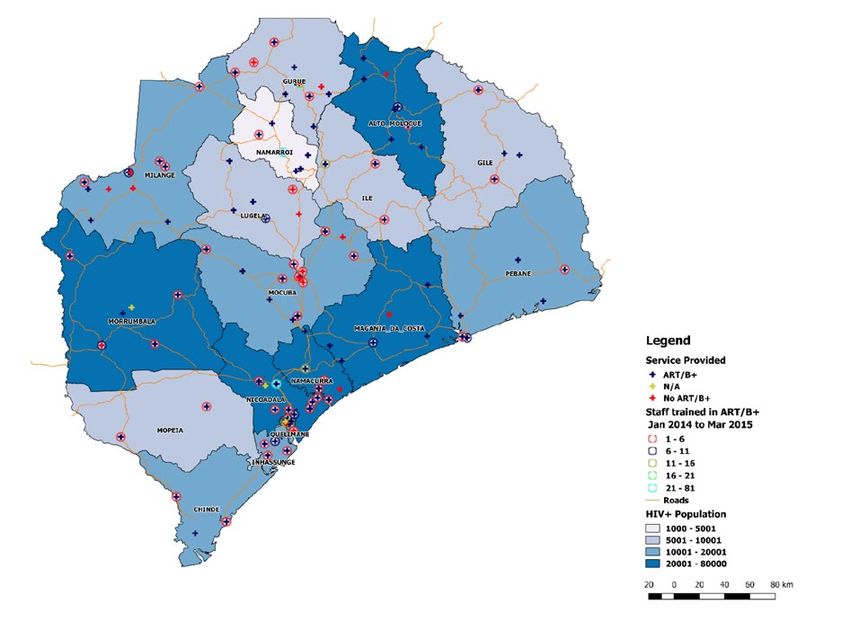
Figure 23: Availability and accessibility of VMMC services based on data from human resource information systems in Mozambique 32
Figure 24: Lessons learnt from VMMC implementation and possible mitigating measures 34
Figure 25: Sample data analysis outputs on resource needs and availability by strategic pillar, Zimbabwe 35
LIST OF TABLES
Table 1: Framework for exploring minimum service package in Kenya 21
ii
ACKNOWLEDGEMENTS
WHO would like to thank the participants and presenters of this
regional meeting on implementing the 2017–2021 framework for
voluntary medical male circumcision. The valuable contribution of
young people is especially recognized.
WHO would also like to thank Raymond Yekeye who served as
principal reporter.
This report was prepared by Raymond Yekeye, Buhle Ncube,
HIV Prevention Focal Point, WHO AFRO, and Julia Samuelson,
Department of HIV and Global Hepatitis Programme, WHO, Geneva.
LIST OF ACRONYMS
AA-HA! Global Accelerated Action for the Health of Adolescents
AIDS acquired immunodeficiency syndrome
ART antiretroviral therapy
ASRH adolescent sexual and reproductive health
DMPPT Decision-Makers’ Program Planning Tool
HIV human immunodeficiency virus
HPV human papilloma virus
MC male circumcision
MoH ministry of health
NGO nongovernmental organization
NSP national strategic plan
SDGs Sustainable Development Goals
SRH sexual and reproductive health
STI sexually transmitted infection
VMMC voluntary medical male circumcision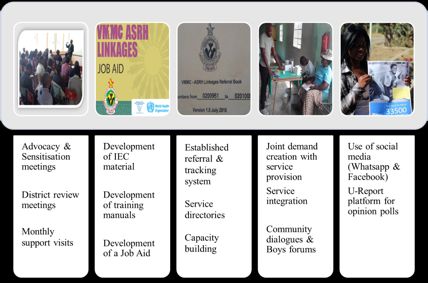
1
LIST OF ACRONYMS OF ORGANIZATIONS
AFRIYAN African Youth and Adolescent Network on Population and Development
AFRO WHO Regional Office for Africa
BMGF Bill and Melinda Gates Foundation
CAPRISA Centre for the AIDS Programme of Research in South Africa
CDC Centers for Disease Control and Prevention
CHAPS Centre for HIV and AIDS Prevention Studies
COSECSA College of Surgeons of East, Central and Southern Africa
ICAN Infection Control Africa Network
ICAZ Infection Control Association of Zimbabwe
ILO International Labour Organization
JHCCP Johns Hopkins Center for Communication Programs
Jhpiego [This is no longer a formal acronym. Jhpiego is an international non-profit
health organization affiliated with Johns Hopkins University.]
OGAC Office of the US Global Aids Coordinator
PEPFAR United States President’s Emergency Plan for AIDS Relief
PSI Population Services International
SafAIDS Southern Africa HIV and AIDS Information Dissemination Service
UNAIDS Joint United Nations Programme on HIV/AIDS
UNESCO United Nations Educational, Scientific and Cultural Organization
UNFPA United Nations Population Fund
UNICEF United Nations Children’s Fund
USAID United States Agency for International Development
WHO World Health Organization
2
INTRODUCTION
This report provides an overview of proceedings of a meeting held 27 February–
1 March 2017 in Durban, South Africa attended by 135 participants from different
levels of various organizations, including from 14 voluntary medical male circumcision
(VMMC) priority countries in eastern and southern Africa1. The meeting sought to share
information on progress, successes, impact and lessons learnt in scaling up national
VMMC programmes. It also provided a platform for updates on strategy and technical
aspects of VMMC interventions, including the 2017–2021 framework, new guidance
and key initiatives for adolescent boys’ and men’s health. The meeting sought to
identify strategic actions, gaps, challenges and possible solutions for continued VMMC
programme scale-up and sustainability. A further key objective was to agree on priority
directions and key country-specific actions for national leadership of programmes.
Participants included government officials, communication experts, implementation
researchers, adolescent and young men, women, traditional leaders, and
representatives from nongovernmental organizations (NGOs), community-based
organizations, implementing agencies and development partners (see Annex 3
for a full list of participants).
1 Botswana, Ethiopia, Kenya, Lesotho, Malawi, Mozambique, Namibia, South Africa,
South Sudan, Swaziland, Tanzania, Uganda, Zambia, Zimbabwe.3
BACKGROUND
By end 2016 over 14 million2 men had been With this intention two meetings were held 27 February–
circumcised for HIV prevention in eastern 3 March 2017 in Durban, South Africa. The first meeting
and southern Africa. (27 February–1 March 2017) was attended by all
participants (see Annex 3) and the proceedings and
It is estimated that these male circumcisions (MCs) main outcomes are summarized in this report. The second
will avert around 500 000 HIV infections through 2030. meeting (2–3 March 2017) was attended by 33 participants
Efforts to scale up national VMMC programmes have (out of the 135 who took part in the first meeting),
been enabled through the development of national including VMMC focal points from the ministries of health
policies on MC, investments in service delivery, in the 14 priority countries and from the WHO country
widespread communication and demand generation offices, as well as representatives from WHO headquarters,
along with the engagement of many partners and the WHO Regional Office for Africa and the Intercountry
communities. Experience from VMMC programmes in 14 Support Team for Eastern and Southern Africa. This second
priority countries in eastern and southern Africa has shown meeting was held to provide a forum for further discussion
high uptake among adolescent boys in particular. The men of key issues emerging from the first three-day meeting,
and boys reached through VMMC programmes have also including technical support needs and the way forwards
been provided with a minimum level of safer sex education, in scaling up VMMC.
offered condoms and HIV testing, and been assisted with
the management of sexually transmitted infections.
As a follow-on to the Joint Strategic Action Framework
to Accelerate the Scale-Up of Voluntary Medical Meeting objectives
Male Circumcision for HIV Prevention in Eastern The objectives of the 27 February–
and Southern Africa 2012–2016 UNAIDS and WHO put 1 March 2017 meeting were to:
forward new strategic directions with a focus on adolescent
boys and young men in the Framework for Voluntary i. Share progress, successes, impact and lessons
Medical Male Circumcision: Effective HIV Prevention learnt in scaling up VMMC.
and a Gateway to Improved Adolescent Boys’ and ii. Provide updates on strategy and technical
Men’s Health in Eastern and Southern Africa by 2021, aspects of VMMC, including the framework,
the targets of which are aligned with the UNAIDS new guidance and key initiatives for adolescent
Fast-Track goals, namely: males and other men.
i) 90% of males aged 10–29 years will have been iii. Identify strategic actions, gaps, challenges and
circumcised in priority settings in sub-Saharan Africa possible solutions for continued scale-up and
as part of integrated sexual and reproductive health sustainability of VMMC.
services for males;
iv. Agree on priority directions and country-specific
ii) 90% of males aged 10–29 years will have accessed key actions for national programme leadership.
age-specific health services tailored to their needs.
Modelling done in 2014–15 showed that an intensified
focus on younger men aged 15–29 years was required
for VMMC programme efficiency and to achieve the most
immediate impact on the HIV epidemic. Efforts have been
underway to expand the evidence on how to operationalize
VMMC services for adolescents while simultaneously
accelerating scale and reach to higher-risk and young
men. Thus, the need was expressed by many stakeholders
to reflect on progress, challenges, lessons learnt and
opportunities to inform future VMMC programmes.
2 The finalized figure for 2016 is a total of 14.5 million VMMCs performed,
of which 2.8 million in 2016.4
PRESENTATIONS, SUMMARIES
AND PRIORITY ACTIONS
DAY 1 The official opening ceremony was presided over by
the WHO Country Representative for South Africa, Dr R.
OPENING SESSION Chatora, along with Mr C. Bonnecwe and Dr R. Ndaba from
the South African Department of Health, who work at the
national and provincial levels respectively.
The speakers highlighted the main successes achieved to
date by the VMMC programme in South Africa, which not
only provides men with access to MC services but also links
them to other relevant health services. The programme
has leveraged existing partnerships, particularly with the
private sector and other health programmes, to facilitate
the achievement of results. Challenges around data
collection and data quality, low VMMC uptake by older
men and the quality of services provided by traditional
circumcision providers need to be further addressed.
Share progress, successes, impact and lessons learnt in scaling up VMMC
Setting the scene (B. Ncube, WHO)
WHO presented the context for the meeting and made reference to some of the key VMMC milestones that have been
achieved to date (see Fig. 1).
Figure 1 Key milestones in VMMC for HIV prevention
HIV prevention research: Implementation in 14
– Observational data priority countries of
– Durban IAS2000 East & Southern Africa
– global consensus to conduct RCTs
1989 2000 2005 – 2007 2007 2007 – today
Kenya, Uganda,
South Africa trials
UNAIDS and WHO Global Recommendations5
Almost 12 million VMMC procedures were performed 452 000 HIV infections by 2030, and the median cost per
in eastern and southern Africa by end 2015. This figure HIV infection averted of US$ 3800 demonstrates the cost-
increased to more than 14 million3 in 2016, which is almost effectiveness of VMMC. Figure 2 provides an overview
two thirds of the target of 20.8 million MCs set within the of the number of VMMCs performed in the 14 priority
initial VMMC framework in 2011. The more than 12 million countries in eastern and southern African in the period
MCs performed by end 2015 will avert an estimated 2008–2015.
Figure 2 Overview of VMMC implementation progress in 14 countries in
eastern and southern Africa
Cumulative total: 11 685 591 through 2015
3 000
Botswana Rwanda
Ethiopia South Africa
2 500
Number of circumcisions (000)
Kenya Zwaziland
Lesotho Uganda
2 000 Malawi United Rep Tanzania
Mozambique Zambia
Namibia Zimbabwe
1 500
1 000
500
0
2008 2009 2010 2011 2012 2013 2014 2015
Year
Most countries did not meet the 80% VMMC coverage Africa 2012–2016. South Africa, Kenya, Uganda and
target set within the Joint Strategic Action Framework Tanzania contributed the highest number of MC procedures
to Accelerate the Scale-Up of Voluntary Medical Male in 2015 (see Fig. 3).
Circumcision for HIV Prevention in Eastern and Southern
Figure 3 Number of VMMCs conducted through 2015 in 14 priority African countries,
with estimated target number required to reach 80% male circumcision
5.0
VMMCs through 2015
4.5
Target
4.0
Millionsof VMMCs
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
a
in ,
ya
o
wi
e
ia
da
a
d
nia
da
a
e
ov ia
bw
qu
bi
an
r ic
th
an
ib
n
ala
P r io p
an
an
za
m
ce
so
Ke
m
Af
t sw
bi
zil
ba
Za
Rw
Ug
n
M
Na
lla Eth
m
Le
a
h
Ta
Zim
Sw
Bo
a
ut
oz
So
M
be
m
Ga
3 The finalized number for 2016 is a total of 14.5 million VMMCs performed, of which 2.8 million in 2016.6
In the 14 priority African countries, through 2015, 32% Perspectives and experiences of young
of VMMCs were performed in the 10–14-year age group.
These circumcisions alone will contribute to a 16%
people (L. Mosooane, AVAC; J. Kayombo,
reduction in the number of new HIV infections which AFRIYAN)
would have occurred through 2030. This session provided the floor for young people – who
are key for the success of VMMC programmes – to share
34% of VMMCs through 2015 were performed among
their perspectives. AVAC and AFRIYAN highlighted the
adolescents aged 15-19 years; these will avert an
importance of ensuring young people are fully involved in
estimated 35% of new HIV infections through 2030.
consultations as well as in programming/implementation so
that VMMC programmes are relevant. In addition, reference
Lessons learned
was made to the critical role played by women and girls in
Lessons learnt from implementing the Joint Strategic decision-making around VMMC for adolescent boys/young
Action Framework to Accelerate the Scale-Up of Voluntary men. Moreover, during the design and implementation of
Medical Male Circumcision for HIV Prevention in Eastern programmes careful consideration needs to be given to
and Southern Africa 2012–2016 include the importance of social norms and structures. Experience has shown that
working within country-specific contexts and investing in adolescent boys and young men have been left out of
innovation to increase the scope of success. The centrality programmes on sexual and reproductive health (SRH) or
of sustained national leadership for programme success gender-based violence and gender equality, despite the
was also recognized. Key lessons further illustrated fact that they exert a tremendous influence over girls.
that different demographic groups are influenced in Interaction between boys and girls is a fundamental
varying ways, requiring age-specific communication requirement if there is to be better understanding of
tools and messaging. Strategic information was critical in gender equality and sexual violence at the societal level.
supporting programme implementation and scale-up; thus, Therefore, it is essential to involve boys and young men
strong monitoring and evaluation (including collecting in programmes on gender equality and gender-based
and analysing disaggregated data) was important for violence. SRH interventions also need to be designed for
facilitating informed decision-making. Another lesson and targeted at both adolescent boys and girls, bearing in
was that programme success is dependent on strong mind their similarities and differences. Furthermore, efforts
multi-stakeholder efforts and coordination, including should be made to provide timely and correct information
partnerships with civil society organizations and at all about SRH to young people. Finally, it was highlighted that
levels of the national health system. programme design and implementation approaches should
be built on the understanding that VMMC is a gateway to
Challenges other services, for example HIV testing services.
Key challenges faced in implementing the 2012–2016
joint strategic action framework were primarily around
generating demand for VMMC services among men
aged 24 years and above. Insufficient research has been
conducted on the barriers to service uptake among this
population. In addition, leadership at the subnational level
has been limited – or when available was unsustainable
– which has affected progress, especially as leadership at
all levels is fundamental for programme success. Further,
human resource shortages affected progress, especially
where programmes were predominantly physician-led,
compared to those settings where task-sharing efforts
resulted in the inclusion of other cadres.7
KEY PROGRESS, SUCCESSES AND LESSONS
LEARNT TOWARDS THE 2016 TARGETS
Country presentations (K. Serrem, Kenya Ministry of Health (MoH); Zambia MoH; G. Lija,
Tanzania MoH; Malawi MoH)
This session provided perspectives from the VMMC programmes in Kenya, Tanzania, Malawi and Zambia. One common
observation was that uptake of VMMC decreases with age, as evidenced in Tanzania (see Fig. 4), Malawi and Zambia.
Figure 4 Decrease in VMMC uptake by age in Tanzania
250000
200000
VMMC/Age group
150000
100000
50000
0
10-14 Yrs 15-19 Yrs 20-24 Yrs 25-29 Yrs 30-34 Yrs 35-49 Yrs 50+ Yrs
FY 2014 234699 135887 59581 24360 15581 13747 2834
FY 2015 205410 131983 61871 27648 18049 15926 3402
FY 2016 177207 99054 45395 20655 12429 10839 2026
FY 2017 4954 3534 1640 737 448 358 72
In all four countries: discrepancies were experienced innovative demand creation. Data issues – discrepancies
between partner data and data from district-level health between partner data and data from district-level health
information systems; there are plans for the introduction information systems – have not yet been resolved; and the
of tetanus mitigation measures; and consideration is being community VMMC coverage survey planned for 2016 is
given to providing early infant male circumcision services. still to be undertaken.
In summary, the following country-specific progress has • Zambia: 75% VMMC coverage has been achieved.
been made: Success is attributable to good partner coordination and
resource leveraging through regular technical working
• Kenya: although a phased approach to implementation group meetings and planning; task shifting; robust
of the national VMMC programme has been adopted, community demand generation; involvement of traditional
there has already been an impact on HIV incidence and community leaders and women; harmonization
as reported in Kenya’s VMMC impact evaluation. This between partner reporting and data from the national
success has been attributed to: political engagement and health information system. However, there have been
MoH leadership (technical working groups) at all levels; challenges with competing health priorities, the lack of
stakeholder engagement, especially cultural and traditional data disaggregated by age group or data on adverse
leaders in non-circumcising communities; the availability events, and inadequate infrastructure.
of a national strategy with subnational targets; and8
• Tanzania: Successes are attributable to: task shifting, • Malawi: Successes were attributed to the availability of a
which has permitted nurses to perform VMMC; large-scale national policy on VMMC, an operational plan, guidelines
public awareness campaigns; MoH ownership – with an and standard operating procedures (see Fig. 5). Challenges
operational plan through 2017; and partner support for included an inadequate number of trained providers to
implementation. Challenges have included: inadequate routinely offer VMMC services, few implementing partners
capacity for waste management, especially disposable to cover all priority districts, seasonality of demand as well
instruments; implementation in 2015 was only in the as inadequate infrastructure (limited spaces in facilities
PEPFAR-supported Scale-Up Districts, which resulted in and some geographical areas being hard to reach)
lower numbers of MCs performed; discrepancies between and data management (limited submission of data by
data issued by the national health information system partners to MoH).
and that used by implementing partners.
Figure 5 Malawi national policy documents
Partners panel (C. Toledo, PEPFAR; creation. Experience has shown that VMMC is a fast-
moving programme, hence there is a need for flexibility
M. Sundaram, BMGF; A. Kaggwa, AVAC; to put in place learning and sharing mechanisms that
C. Laube, Jhpiego) facilitate rapid scale-up of approaches that are effective.
This session provided opportunities for reflection by Appropriate target setting, sustained resource mobilization
partners on progress made in the implementation of VMMC and a consistent commitment to implementation are key
programmes in the 14 priority countries and discussion on factors for success. The panel recommended ambitious
the implications of current results on future programming. VMMC targets be tied to funding, which is necessary to
The presenters stressed that even though the 80% provide motivation for intervention success. Challenges
target set out in the Joint Strategic Action Framework around financial and technical sustainability were flagged,
to Accelerate the Scale-Up of Voluntary Medical Male highlighting the need to further strengthen the capacities
Circumcision for HIV Prevention in Eastern and Southern of national VMMC programmes. Sustainability is more
Africa 2012–2016 had not been reached in most countries, probable if there is a diversification of the resource base;
major milestones had still been achieved in mainly difficult thus, there is a need to strengthen linkages between
operating environments with competing health priorities. VMMC programmes and other services and sectors as well
A key theme that has emerged is that demand creation as geographic coordination between implementing partners
is fundamental to programme success. Formative work to avoid competition.
and strong partnerships are needed for improved demand9
New strategies and technical updates
GLOBAL AND REGIONAL LANDSCAPE
UNAIDS targets and strategies in the context Three Frees: Start Free, Stay Free, AIDS Free
of the Sustainable Development Goals (SDGs) (P. Nary, UNICEF)
and engaging adolescents and men (P. It is important that the different United Nations HIV
Somse, UNAIDS) prevention frameworks work together to avoid duplication
and to collectively advance towards the goal of zero HIV
VMMC is included in the fourth pillar (Reduce inequality
infections and an AIDS-free generation. The Three Frees is
in access to services and commodities) of the UNAIDS
a collaborative agenda between UNAIDS and PEPFAR. It is
2016–2021 Strategy (On the Fast-Track to End AIDS), where
a fast-track policy and delivery framework for ending AIDS
it is recognized as a game changer. The pillar and related
among children, adolescents and young women by 2020.
target (90% of women and men, especially young people
VMMC is part of the Stay Free component. The key next
and those in high prevalence settings, have access to HIV
steps are to encourage ministers of health and stakeholders
combination prevention and SRH services) provide the basis
to adopt this framework, align existing resources and
for pursuing sustainability. Technical aspects of programme
develop implementation plans.
implementation need to be distinguished from nontechnical
components. There is no such thing as a single issue
struggle because we do not live single issue lives. HIV and AIDS: Framework for Action in
the WHO African Region 2016–2020
(F. Lule, WHO/AFRO)
This framework for action includes five strategic
directions: i) country ownership, ii) effective partnerships,
iii) universal health coverage, iv) integration of HIV and AIDS
in national health systems and strategies, v) a public health
and people-centred approach. It further includes guidance
on prioritization – especially high-impact prevention
interventions, eliminating HIV in infants, expanding
ational HIV testing services, accelerating the scale-up
of antiretroviral medicines for treatment and prevention,
and early detection and treatment of coinfections.
Figure 6 Global HIV targets – Towards the global HIV targets for 2020 and 2030
Reaching the 2020 targets requires accelerating the integrated public health approach that enabled the achievements of
the past 15 years. The proposed WHO Global Health Sector Strategy on HIV 2016-2021 charts such a response.
2.0 million 1.2 million 15.8 million
(2014) (2014) (mid-2015)
< 500 000
< 500 000 (2020)
(2020) � 30 million
< 400 000 (2020)
< 200 000 (2030)
(2030) � 37 million
(2030)
Annual number of people newly Annual number of people dying from Annual number of people
infected with HIV HIV-related causes receiving ART10
EVIDENCE FOR FOCUSED STRATEGIC ACTION
Age, risk and geography modelling to inform costs. In 2016 WHO and UNAIDS held a meeting to
consolidate the findings from the diverse models.
VMMC strategy and targets (T. Farley, The models consistently showed that VMMC programmes
consultant for WHO) that reach males aged 15–29 years and males at higher
Models used earlier to estimate the impact and cost of sexual risk of HIV infection (such as those with multiple
VMMC programmes have been updated and new models partners) will have the most immediate impact on
developed. These models use more precise age groups, the AIDS epidemic, followed by boys aged 10–14 years.
updated HIV incidence estimates and lower HIV treatment
Figure 7 Relative impact of scaling up VMMC – based on modelling
1
Reduction in HIV incidence
by age group, 2014–2050.
Each line represents HIV incidence
0.9
ratio under scenario in which
only indicated 5-year age group
a circumcised. Marker a represents
HIV incindence ratio
0.8
5-yr period from 2014. Marker
b represents a 15-yr period
b Age group from 2014.
0.7
10–14
15–19
0.6 20–24
25–29
30–34
0.5 35–39
2013 2018 2023 2028 2033 2038 2043 2048
Year
VMMC coverage, modelling and translation Figure 8 UNAIDS Fast-Track MC targets
of results to inform national strategies (P. Estimated number of circumcisions required by country to
Stegman, Avenir Health) achieve 80% or 90% coverage in 10-29 yr age group by 2020
The Decision-Makers’ Program Planning Tool (DMPPT), Country % in 2015 Target 80% Target 90%
developed in 2009 for advocacy purposes, was used to Botswana 31% 240,000 280,000
generate initial estimates on HIV infections averted by MC
Ethiopia (Gambela) 75% 10,000 19,000
at diverse coverage levels. A second version of the DMPPT,
Kenya (Nyanza) 72% 290,000 505,000
developed in 2011, was used for strategic planning in nine
African countries with national VMMC programmes and by Lesotho 69% 55,000 100,000
the Government of the United States of America (PEPFAR) Malawi 26% 2.5 million 3.0 million
in the formulation of country operational plans and for Mozambique 57% 2.2 million 2.9 million
monitoring purposes. Achieving the Fast-Track 90–90–90 Namibia 27% 310,000 370,000
HIV prevention goals requires 90% VMMC coverage among
Rwanda 35% 1.3 million 1.6 million
males aged 10–29 years (see Fig. 8) and health services
South Africa 56% 2.7 million 3.9 million
that are tailored to the needs of specific age brackets.
South Sudan 26% 1.8 million 2.1 million
Swaziland 32% 150,000 180,000
Uganda 53% 3.6 million 4.6 million
Tanzania 84% 1.1 million 2.4 million
Zambia 37% 2.0 million 2.4 million
Zimbabwe 22% 2.2 million 2.6 million
Total 20.4 million 26.8 million
Source: UNAIDS11
Framework on VMMC: effective HIV of 90% circumcision coverage among males aged 10–29
years and broadening the range of age-specific health
prevention and a gateway to improving services offered to this same age group. How to integrate
adolescent boys’ and men’s health VMMC services into broader health and development
(J. Samuelson, WHO) aspirations and systems needs to be determined to ensure
sustainability. The Framework is based on three principles:
WHO presented on the new landscape in which VMMC
a people-centred approach, gender-based perspective
implementation is situated and how the new Framework
and enhancing partnerships.
on VMMC is aligned with the SDGs and other global
health strategies. It builds on the two Fast-Track targets
Figure 9 Years of life lost among men in eastern and southern Africa,
according to age group and cause (2013)
eastern Africa southern Africa
100
Other non communicable diseases
90
Other infectious diseases
80
70 Alcohol & drug use disorders
Percentage
60
Interpersonal violence
50
40 Self-harm
30 Unintentional injuries
20
HIV/AIDS
10
0 Tuberculosis
10-14 15-19 20-24 25-29 15-49 10-14 15-19 20-24 25-29 15-49
YEARS YEARS
Six causes (HIV, tuberculosis, violence, self-harm, injuries and alcohol or drug misuse) contribute more than 80% of
years of life lost among men aged 15-49 years in southern Africa, and more than 60% in eastern Africa.
Source: Prepared by the authors, based on the Global Burden of Disease Study 2013 (3).
The Framework has four strategic directions: 3. I nnovations for accelerations and the future.
Health policies need to be established that better
1. F ocused action for scale-up. Using strategic address the needs of men and boys, including
information to determine among which population supportive policies from other sectors such as
groups and geographic areas to focus and tailor VMMC sports and gender. Investing in new coalitions and
interventions is essential for impact, as noted in the partnerships is essential for programme success.
modelling results. Age groups should be prioritized, Research on implementation and operations can inform
especially the age bracket 10–29 years. Priority improvements in service delivery. Creating a culture
should also be given to males at higher sexual risk of health care seeking behaviour will require learning
of HIV infection. about and changing demand generation approaches,
2. P
olicies and services for greatest impact. including the effective use of relevant media.
Male-friendly health service delivery approaches 4. Accountability for quality and results. Results must
must be enhanced along with relevant age- and risk- be evaluated across programmes and sectors, including
specific packages of services. the effectiveness of partnerships. Countries need to
put strong national monitoring and quality assurance
systems in place within the next five years and expand
their financial resource portfolios.12
BRIEF TECHNICAL UPDATES
(PARALLEL SESSIONS)
Manual for male circumcision under containing vaccine (two doses sufficiently timed for
protection) should be administered before the elastic
local anaesthesia, second edition collar compression method (PrePex) is used. WHO also
(M. Mahomed, Jhpiego) recommends vaccination programmes add tetanus-toxoid-
Jhpiego provided a brief overview of the revisions that containing vaccines (boosters) for adolescent boys 4.
will be made in the second edition of the Manual for male The WHO schedule for provision of both tetanus-toxoid-
circumcision under local anaesthesia. These revisions are containing vaccines for adolescent boys and girls and
based on the last 10 years of experience with over 14 human papilloma virus vaccinations for girls is now aligned
million MCs performed in eastern and southern Africa. to during the ages 9–15 years. Also, awareness should be
It includes revised and rearranged chapters geared towards raised among individuals and communities about clean
improving quality and safety. WHO recommendations have wound care so that substances such as dung, which may
been incorporated from guidance on infection prevention contain spores, are not used. VMMC in general remains
and control, including hand hygiene and safe injection a safe procedure with a low rate of adverse events.
practices, as well as new surgical recommendations.
Youth advocacy workshop
VMMC methods, tetanus risk and mitigation Fourteen youth advocates, selected through a nomination
through tetanus-toxoid-containing process carried out by AFRIYAN, attended the meeting as
vaccination (J. Samuelson, WHO) part of their country teams. Their role was to contribute
the perspectives of adolescent boys and young men
WHO has monitored the safety of MC methods, including and advocate for responsive VMMC programming.
new device-based methods. The PrePex (elastic collar In collaboration with AVAC and AFRIYAN, the youth
compression) and the Shang Ring (collar clamp) have been advocates developed key advocacy messages to encourage
prequalified by WHO for use among males aged 13 years policy-makers and programme implementers to give further
and over. Less than 4% of the more than 14 million VMMCs attention to adolescent boys and young men in the HIV
performed to date were done using devices; the majority response and make full use of the opportunity that VMMC
were performed with conventional surgical methods. provides to address their broader health needs. The young
Between 2012 and mid-year 2016, 16 cases of tetanus participants used these messages for advocacy throughout
were reported. A difference in risk was noted by the three-day meeting. The messages were further
circumcision method. For example, there was a 30-fold developed into an advocacy note for youth organizations
increased risk of tetanus with the use of the elastic to use at the country and international levels. (See Annex 1
collar compression method. Mitigation of this tetanus for a full report on the youth advocacy workshop.)
risk is possible. The WHO position, issued after two
advisory group consultations, is that a tetanus-toxoid-
4 WHO Weekly Epidemiological Record,10 February 2017, vol. 92, 6 (pp.53–76).13
DAY 2
Evidence, lessons and promising practices to actions
FOCUSED ACTION FOR MALES 20–29 YEARS
AND MOST AT RISK MEN
Demand creation (L. Van Lith, JHCCP; C. encouraging implementing partners to focus on age pivots
(ages of highest priority for HIV incidence reduction)
Laube, Jhpiego; D. Taljaard, CHAPS; C. through differential reimbursements. Typically, there
Toledo, CDC; A. Machinda, PSI Zambia) are multiple steps in a person’s progression to changed
This session provided an overview of demand creation behaviour, thus numerous interactions with a client may be
strategies, including specific strategies for older men. required to advance him from baseline to action. At each
step, internal (cognitive and emotional) and environmental
Two key approaches to accelerating VMMC uptake among (cultural and ethical factors, or issues around service
men were outlined: interpersonal communication and delivery) factors can influence an individual’s immediate
community mobilization. The presentation focused on VMMC needs and wants, which will govern his subsequent
strategies used for VMMC uptake among males aged 20– actions (see Fig. 10). Therefore, different strategies,
29 years in South Africa. These strategies have included: messages and sets of tactics might be employed at
focusing on high schools, providing group-based support, each interaction.
Figure 10 Influences and stages of the journey to VMMC
Structural
factors
Cultural and
society norms
Personal
relationships
Individual
User-Centric Behavioral Framework
Unaware Unaware, Opposition/Apathy Pre-intention Intention Action Relief
Knowledge Cognitive/Emotional/ CEC + structural CEC + structural
barriers Cultural (CEC) barrier barriers and barriers and
and facilitators facilitators facilitators14
The session also focused on the need to invest in most immediate impact on HIV incidence. The CDC-
implementation science research. CDC shared information supported studies addressed demand and service delivery
from studies conducted in Tanzania, Kenya and South (setting). They showed the need to vary demand creation
Africa (see Fig. 11). One key issue that has emerged is that approaches, including messaging, according to the context,
males aged 20 years and over are not accessing VMMC maturity of the VMMC programme and/or target group.
services as much as younger males. Older men are more Some approaches showed modest increases in VMMC
likely to take part in riskier sexual behaviours, therefore, uptake among adults.
circumcising men aged 20–34 years would provide the
Figure 11 Overview of implementation science studies in Tanzania,
Kenya and South Africa
TANZANIA KENYA SOUTH AFRICA
Research Question
Does VMMC uptake increase among Does VMMC uptake increase among Does VMMC uptake increase among men
men aged 20-34 years when exposed men 25-39 years when exposed to aged 25-49 years when an ‘Exclusive
to communications and service delivery interventions addressing barriers? Intervention Package’ is offered to older
tailored to older men? men?
Objectives
• Increase the total number of VMMC clients • Increase the proportion of men • Develop tailored VMMC messages
and the proportion of men aged 20-34 years aged 25-39 years who accept addressing barriers for men aged 25-49
• Assess relationship between client age and VMMC compared to men randomized years.
reported rick of HIV acquisitions to routine service delivery and demand • Evaluate the effectiveness of an ‘Exclusive
creation activities (including enhanced Intervention Package’ to men aged 25-49
interpersonal communication and dedicated years.
service outlets).
Market research combined with behavioural economics
was shared by PSI as a method used in Zambia to increase
VMMC uptake. The method includes journey path mapping
of a man from awareness of VMMC to uptake of the service
and quantitative market segmentation. This approach
allows target client archetypes to be developed.15
Accessing services (C. Toledo, CDC; V. Kikaya, Jhpiego; K. Hatzold, PSI Zimbabwe;
S. Mabhele, ILO; T. Teka Amero, PEPFAR Ethiopia)
This session offered examples of channels through which showing that in general Basotho men [men from Lesotho]
adult men may be reached with HIV prevention services, have suboptimal health seeking behaviours. Within the
including VMMC. clinic there is evidence that VMMC is serving as a gateway
to other health services (offered at the clinic), including
Jhpiego presented on the VMMC/male clinic in the Scott HIV testing, counselling and testing/treatment of other
Hospital in Lesotho, which is a stand-alone facility located sexually transmitted infections. All VMMC clients at the
away from the main hospital. It is the only male clinic in clinic were tested for HIV between July 2016 and January
South Africa to be part of a public hospital. The clinic was 2017 (see Fig. 12).
set up based on demographic and health survey evidence
Figure 12 HIV testing results for VMMC clients at male clinic
in Scott Hospital, Lesotho
All Clients tested for HIV in the male clinic, July 2016 to Jan 2017
Positive, 150, 14%
Negative, 926, 86%
The ILO presentation on reaching adult men with VMMC treatment services and other health services. The example
services through occupational settings highlighted that provided was that of the South African Clothing and Textile
workplace responses to HIV have an impact on the AIDS Workers’ Union: Worker Health Programme, which provides
epidemic and can, therefore, contribute to national AIDS quality HIV- and tuberculosis-related services to blue collar
responses. The commitment of workplace senior managers workers and engages with representatives of employers
and workers’ leaders are driving forces. Engaging worker and workers through tripartite consultation forums (labour
representatives (trade unions) facilitates the mobilization advisory councils). It was noted that the public sector often
of workers (particularly men) to access HIV prevention/ employs a larger number of men than the private sector.16
Figure 13 Defining and locating the world of work
Formal/Informal/Self Employment
People looking for Employment Interns, Volunteers, Apprentices
Public Sector Private Sector Civil Society
Organized Employers and Workers
Government Ministries of Private Companies and Non-Governmental Organizations
Public Service or Departments Business (different sectors and and their Coalition
/Agencies/Offices industries of the economy (Associations and Networks)
People who have exited employment Ex-Mineworkers and other workers
PEPFAR/Ethiopian Department of Defence gave a HIV testing is not mandatory for men who undergo VMMC.
presentation on reaching adult males with VMMC The PSI/Zimbabwe presentation on HIV self-testing showed
services through the military in Ethiopia, where VMMC is that fear of HIV testing, in particular getting a HIV-
being offered to new recruits during their training period. positive result, is a barrier to the uptake of VMMC among
Approximately 10–15% of new recruits are uncircumcised, sexually active men. Since HIV self-testing was introduced
of which around 90–95% accept circumcision. Some in Zimbabwe, there has been high uptake among men,
active soldiers also accept circumcision. Because of the young people and key populations. Among these groups,
integration of the VMMC programme in the training centres 20–30% are first-time testers. Evidence shows that HIV
for new recruits, the Ethiopian National Defence Force is self-testing may help address fears of taking up provider-
able to achieve its annual VMMC target and there is also delivered HIV testing services. HIV self-testing will help to
an opportunity to address the stigma that some men who link HIV-negative people to appropriate prevention services
are uncircumcised sometimes face. The Ethiopian National and identify people living with HIV by providing testing to
Defence Force has shared its experience of integrating populations that would otherwise not test due to access
VMMC services with the militaries in other African or privacy barriers.
countries, some of which are now working towards
this model. The CDC presentation highlighted that in the period
2015–2016 males aged 20–29 years constituted less than
30% of all VMMC clients in the 14 priority countries (see
Fig. 14). VMMC is one of few preventative health services
that caters specifically to males and also provides health
screening opportunities, including for noncommunicable
diseases. Evidence from Namibia showed that some men
were newly diagnosed with hypertension as a result of
the screening they received as part of their VMMC service.17
Figure 14 VMMC among men aged 20–29 years in 2015 and 2016, by priority country in Africa
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
2015 20-29 2015 Total Population 2016 20-29 2016 Total Population
Policies that affect men’s health and •M
en’s health requires urgent attention – for
everybody’s sake.
address masculinity (D. Peacock, Sonke
Gender Justice) • Improving men’s and boys’ health should enhance –
not detract from – women’s health and Health for All.
The results of policy scans by Sonke Gender Justice (see
Fig. 15) show that although most national strategic plans • Women too often blame men for their [men’s] ill health
acknowledge the importance of gender mainstreaming and absolve themselves of responsibility.
in HIV-related interventions, very few refer to the need • The low use of health services among men reflects
to engage men; almost all the national strategic plans prevailing gender norms, structural drivers, poor access
reviewed have a very limited conceptualization of gender to health services, lack of policies and weak political will.
– seeing it as referring to women only. National strategic
• A growing number of policies and programmes are
plans are more likely to mention men in relation to efforts
improving men’s health – in the few countries where
to prevent mother-to-child transmission of HIV and medical
they exist.
MC. They rarely mention men in terms of policies to affect
their attitudes towards condom use, involving them in • It is necessary to develop and implement policies and
home-based care or targeting them to increase their uptake programmes that shift gender norms, improve men’s
of HIV testing and treatment services. Sonke Gender Justice access to services and address structural drivers of
emphasized the following points: men’s ill health.18
Figure 15 Results of policy scans by Sonke Gender Justice
3. HIV HIV and Attempts Engaging Men’s Male Condoms Men’s use Marginalized Treatment Home
Gender to challenge men for support of circumcision of VCT men & boys Based Care
NSP Gaps or transform prevention PMTCT
gender of GBV
norms
Burundi
Cote D’Ivoire
2006-2010
Ethiopia
2009 – 2010/11
Kenya
2009/10 – 2012/13
Mozambique
Namibia
2011 – 2016
Rwanda
2009 – 2012
Sierra Leone
South Africa
2007 – 2011
Tanzania
2008 – 2012
Uganda
2007/8 – 20011/12
Zambia
2011 – 2015
Zimbabwe
2011 – 2014
Key Adequate Room for improvement Inadequate
BREAKOUT GROUP WORK SESSION
Implementation considerations for young in order to encourage uptake of VMMC services among
this population group. There is a need to: include VMMC
men and high-risk men within labour policies; create incentives for employers;
These group work sessions aimed to provide an opportunity strengthen private–public funding partnerships; coordinate
for countries to share their experiences and further explore scheduling of VMMC services with/between workplaces.
the requirements for VMMC reprogramming and key
• Peers, champions and traditional/community influencers
implementation considerations. The main feedback from
have been successful in generating demand for VMMC
the working groups was as follows:
services. This approach should be strengthened, while
ensuring links to VMMC services, especially in rural areas,
Young men in order to minimize the time between mobilization
• Since young men are an economically viable group, and the provision of VMMC. In addition, it is necessary
concerted efforts are needed to engage employers, trade to ensure that sites where VMMC services are offered
unions and medical health insurance companies and are ready for increased uptake (staffing, infrastructure
facilitate their understanding of the benefits of VMMC and supplies).19
• More use should be made of up-to-date channels of • Increasing VMMC coverage among men most at risk
communication, including mass media, interpersonal will have both programmatic and policy implications
communication, mid-media and social media. and will, therefore, require further significant political
Additionally, messages should be targeted also at and resource commitments.
women as key influencers over men’s health.
• Innovation is required to generate demand and improve
• More engagement with tertiary institutions is necessary access to VMMC services among most at risk populations.
to further leverage opportunities for demand creation. Suggestions included: providing incentives, flexible
services outside of working hours, venue-based outreach,
• In order to better understand what works for young men,
couples services and workplace-based strategies. For men
both in terms of service delivery and demand creation,
on the move, suggested reprogramming considerations
a review of the data collected over the last five years
included: health passports, cross-border health service
is needed to compare VMMC programme experiences
access and referrals as well as shared financial and
in different countries, including the outcomes of pilot
political responsibilities between countries.
initiatives and end-user participation rates.
• Countries will need to make concerted efforts to obtain
• VMMC should be used as a gateway to address other
strategic information on most at risk men since data on
aspects of young men’s health (the same is true for all
this group is often not routinely captured or disaggregated
age groups). Providing VMMC services through men’s
in health information systems and it is important for
health clinics, which offer screening for and treatment
planning and monitoring of VMMC and other services.
of noncommunicable diseases, including mental health
and substance misuse, might be less stigmatizing and
improve VMMC uptake.
High-risk men
• It is important for countries to define which men are
‘at high risk’ or ‘most at risk’ and to understand that
while men in this population will have some common
characteristics there will also be some differences,
which has implications for programming. Some countries
considered the term ‘most at risk’ to apply to: men
in serodiscordant relationships, those with sexually
transmitted infections, clients of sex workers, migrants,
miners, long distance truckers and prisoners.
• Prevention messaging alone is insufficient to increase
VMMC uptake among men who are most at risk given
that other concerns and issues drive their risk behaviour.
Therefore, it is important for VMMC services to provide
an entry point not only to other HIV prevention services
but also to additional priority health services, especially
for men who have limited access to these services.
The VMMC service package could be broadened to
include access to pre-exposure prophylaxis for HIV
prevention, information on family planning, guidance
on addressing attributes of masculinity that affect health
seeking behaviours, and screening for conditions such
as hypertension or substance misuse.20
FOCUSED ACTION FOR ADOLESCENTS
AA-HA! Adolescent implementation Spotlight presentations (S. Mabaya,
framework – synergies with VMMC2021 WHO Zimbabwe; E. Njeuhmeli, USAID;
(T. Desta, WHO) P. Devos, JHCCP)
WHO presented the AA-HA! guidance, which aims to WHO Zimbabwe, on behalf of the Zimbabwe MoH,
provide technical advice to countries to enable them to presented the Adolescent Sexual and Reproductive Health
decide what to do and how to do it as they respond to (ASRH) and VMMC Linkages pilot project, which is being
the health needs of adolescents. Primary target audiences implemented to assess the feasibility of creating and
for the guidance include national-level adolescent health sustaining linkages between ASRH and VMMC services in
policy-makers and programme managers in all relevant Zimbabwe, including related capacity needs. The results of
sectors. Secondary-level audiences include subnational the pilot will contribute to guidance on how to effectively
adolescent health policy-makers and programme deliver the two programmes in order to provide sustainable
managers, international advisors, funders and others. adolescent services and maintain high VMMC coverage
while offering or linking clients to other needed health
In the same way as the Framework for Voluntary Medical services. The pilot started in 2014 and has three phases.
Male Circumcision: Effective HIV Prevention and a Gateway The first phase (2014) focused on preparatory assessments
to Improved Adolescent Boys’ and Men’s Health in Eastern and stakeholder inputs. The second phase (2014–2015)
and Southern Africa by 2021, AA-HA! identifies VMMC as focused on implementation by identifying linkages, feasible
one of a number of priority interventions for countries with approaches and lessons for scale-up. The third phase
generalized HIV epidemics. The AA-HA! implementation (2015–2016) is focused on ongoing implementation (see
guidance also provides advice to Member States on Fig. 16) with monitoring embedded in the two programmes
financing adolescent health interventions through existing and research conducted to assess effectiveness and costs
opportunities such as the Global Fund and the Global in order to inform scale-up by optimizing strategic actions
Financing Facility investment case. In addition, the AA- and the delivery of interventions.
HA! guidance can be used to guide countries in prioritizing
high-impact national interventions and developing
coherent national plans for adolescent health in the
period 2017–2030.
Figure 16 Current activities in the ASRH–VMMC Linkages pilot project, Zimbabwe
Advocacy & Development of Established Joint demand Use of social
Sensitisation IEC material referral & tracking creation with media (Whatsapp
meetings system service provision & Facebook)
Development of
District review training materials Service directories Service U-Report platform
meetings integration for opinion polls
Development of a Capacity building
Monthly support Job Aid Community
visits dialogues & Boys
forumsYou can also read