Intentions to use maternity waiting homes and associated factors in Northwest Ethiopia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281
https://doi.org/10.1186/s12884-020-02982-0
RESEARCH ARTICLE Open Access
Intentions to use maternity waiting homes
and associated factors in Northwest
Ethiopia
Mekonen Endayehu1, Mezgebu Yitayal2* and Ayal Debie2
Abstract
Background: Maternity Waiting Homes (MWHs) are residential facilities located within hospitals or health centers to
accommodate women in their final weeks of pregnancy to bridge the geographical gap in obstetric care. Little is
known, however, about women’s intentions to use MWHs. Thus, this study aimed to assess pregnant women’s
intentions to use MWHs and associated factors in East Bellesa district, northwest Ethiopia.
Methods: A community-based cross-sectional study was conducted among 525 pregnant women in East Bellesa
district from March to May 2018. Study participants were selected using systematic random sampling. Binary logistic
regression was used for analysis. Adjusted Odds Ratio (aOR) with 95% Confidence Interval (CI), and p-value < 0.05
were used to identify factors associated with intentions to use MWHs.
Results: In the study area, 326/499 (65.3%) pregnant women had the intention to use MWHs. Pregnant women
who had good knowledge about maternal healthcare and obstetric complications (aOR 6.40; 95% CI 3.6–11.5),
positive subjective norms related to women’s perceptions of social pressure (aOR 5.14; 95% CI 2.9–9.2), positive
perceived behavioral control of women on the extent to which women feel confident (aOR 4.74; 95% CI 2.7–8.4),
rich wealth status (aOR 4.21; 95% CI 2.1–8.4), women who decided by themselves to use maternal services (aOR
2.74; 95% CI 1.2–6.2), attended antenatal care (aOR 2.24; 95% CI 1.2–4.1) and favorable attitudes towards women’s
overall evaluation of MWHs (aOR 1.86; 95% CI 1.0–3.4) had higher odds of intentions to use MWHs.
Conclusion: Two thirds (65.3%) of pregnant women had intentions to use MWHs. Factors such as women’s
knowledge, subjective norms related to women’s perceptions of social pressure, perceived behavioral control of
women on the extent to which women feel confident to utilize, and wealth status, decision-making power,
attending antenatal care and attitude towards women’s overall evaluation of MWHs were significantly associated
with the intention to use MWHs. Therefore, improving women’s awareness by providing continuous health
education during antenatal care visits, devising strategies to improve women’s wealth status, and strengthening
decision-making power may enhance their intention to use MWHs.
Keywords: Maternity waiting home, Northwest Ethiopia
* Correspondence: mezgebuy@gmail.com
2
Department of Health Systems and Policy, Institute of Public Health, College
of Medicine and Health Sciences, University of Gondar, P. O. Box, 196
Gondar, Ethiopia
Full list of author information is available at the end of the article
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 2 of 10 Background A comparative study in Attat and Butajira hospitals Maternity Waiting Homes (MWHs) are residential fa- showed that pregnancy outcomes among those using cilities located within hospitals or health centers to MWHs were better than outcomes among non-users [12]. accommodate women in their final weeks of preg- The Ethiopian Ministry of Health (MOH) has made nancy and a strategy to “bridge the geographical gap” MWHs available in all health facilities throughout the in obstetric care between rural areas with poor access country since 2015. Even though MWHs help to improve to functioning facilities, and urban areas where mater- maternal health care, costs, distance, and time-related bar- nity services are available. MWHs offer a low-cost riers are some of the challenges in using MWHs [4, 13]. way to bring women closer to obstetric care as one In many health facilities, costs for MWHs have been cov- component of a comprehensive package of essential ered with the support of the community, contributing obstetric services [1]. MWHs have been endorsed by food, and money for women staying in MWHs [13]. Poor the World Health Organization (WHO) as one com- accessibility, financial unaffordability, lack of transport ponent of a comprehensive package to reduce mater- and women’s inability to decide on their own to use nal morbidity and mortality [2]. Maternal deaths MWHs are factors affecting institutional births rates in around the world dropped from about 532,000 in low-resource countries [14]. 1990 to an estimated 303,000 at the end of the Mil- Few studies, however, have been conducted in Ethiopia lennium Development Goals (MDGs) [3]. Between to assess women’s intentions towards MWH’s utilization 1990 and 2015 the Maternal Mortality Ratio (MMR) during their last weeks of pregnancy, and findings of has been reduced from 385 to 216 per 100,000 live these few showed that only 55.1–57.3% of women have births globally and from 987 to 546 in sub-Saharan intentions to use MWHs [15, 16]. Therefore, this study Africa (SSA) [4]. The 2016 Ethiopian Demographic aimed to assess intentions to use MWHs and associated Health Survey (EDHS) reported a MMR of 412 per factors among pregnant women in East Belessa district, 100,000 live births [5]. In low-and middle-income northwest Ethiopia. countries, particularly SSA countries, MMRs are nearly 20 times higher than those in high-income Methods countries [4]. Study design and settings Pregnancy-related maternal mortality is usually af- A community-based cross-sectional study was con- fected by the “Three phases of Delay”: first phase delay ducted among pregnant women in East Bellesa dis- to decide to seek care in the community, second phase trict, northwest Ethiopia from March to May 2018. delay to reach appropriate facilities, and third phase The district is in the North Gondar administrative delay in the provision of adequate care or receiving ad- zone which is 720 km far from Addis Ababa (the cap- equate care after reaching facilities [6]. Though MWHs ital city of Ethiopia). Total population of the district have existed in Ethiopia for more than three decades, it was 154,937 with 140,209 rural and 14,728 urban in- has been limited mainly to some hospitals making these habitants [17]. In the district, 35,889 women of re- inaccessible for most pregnant women [7, 8]. The recent productive age are estimated to live. The district has expansion of MWHs to health centers is a break- one public primary hospital, five health centers, through to bridge the geographic barriers to skilled twenty-three health posts, three private primary care. MWHs are built to reduce second phase delays clinics, and one drug store. Point of service where in reaching health facilities in time and it is an insti- women got educated about MWHs were home visits tution within easy reach of emergency obstetric and by Health Extention Workers (HEWs), ANC visits newborn care facilities, where women with high-risk (84%), home visits by Health Development Armies pregnancies await the onset of labor during the final (HDAs), women’s conferences and other community weeks of pregnancy [8, 9]. events [13]. All health centers and the hospital in the Cost, distance, and time needed to access care are district have MWHs and provide free maternal health major barriers to the effective utilization of maternal care including bed and food services. Many MWHs and child health care in poor and marginalized areas were built with community support, that usually con- [10]. Available data from a rapid assessment in Eritrea tributed food items and money for women staying in from September 2006 to August 2007 show that a these MWHs, a workforce to build MWHs, and wood case fatality rate of 1.9% among women who gave and grass for construction. As a result, most MWHs birth before the introduction of MWH, but no mater- had no budget allocated from government funds [13]. nal mortality was recorded after its introduction from May 2008 to April 2009 [11]. Institutional birth rates Population and sampling procedures also increased with 56% in Eritrea after introducing All pregnant women in East Belesa district were the MWHs [11]. source population, while those who resided in the
Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 3 of 10
selected kebeles (the lowest administrative units in the your gestational age for your current pregnancy? 5) Do
country) were the study population. Participants who you know giving birth at home has a risk for women and
were critically ill during data collection were excluded. newborns? 6) Do you know that using an MWH is im-
Men were not the study participants, and not portant for pregnant women who need immediate ob-
interviewed. stetric care? 7) Do you know about birth preparedness
The sample size was calculated using a single population and complication readiness? 8) Are there MWHs in your
proportion formula with an assumption of a 5% margin of area? Each question contains 0 = no and 1 = yes. The
error, 95% CI, 1.5 design effect, 5% non-response rate, and total score ranged from 0 to 8 and a score of ≥60% was
57.3% proportion (P) of pregnant women intended to use considered as knowledgeable.
MWHs in Jimma district, Southwest Ethiopia [15]. The Women’s attitudes towards MWHs were measured using
sample was 592; however, the estimated number of preg- four questions: 1) For me using MWH is good; 2) For me
nant women in the study area was below 10,000 i.e. only using MWH is valuable; 3) For me using MWH is pleasant;
4639. As a result, we used finite population correction for- 4) For me using MWH is beneficial. Each question contains
mula and our final sample size was 525. Two urban and five points Likert scales (1 = strongly disagree, 2 = disagree,
six rural kebeles among 22 kebeles in the district were se- 3 = neutral, 4 = agree, 5 = strongly agree). The total score
lected using the lottery method. The sample size was allo- was 4–20 and women who had scored ≥60% were consid-
cated proportionally to the expected number of pregnant ered as having favorable attitudes.
women in different kebeles. Furthermore, subjective norms (SN) towards MWH
Finally, study participants were selected using a sys- utilization, related to women’s perceptions of social pres-
tematic sampling technique. Sampling interval was de- sure to utilize MWHs, were measured by using five
termined by dividing the total expected number of questions: 1) Most people who are important for me,
pregnant women by the sample size and the interval was think that I should use MWH; 2) Whether I use MWH
three. The first study participant was selected through or not is up to me; 3) Most women in my village/neigh-
the lottery method, and then every third household was borhood use MWHs; 4) It is expected from me to use
included. Furthermore, the next household was consid- MWH; 5) Most people whose opinions I value, would
ered when there were no pregnant women in the se- approve of my using MWH. Each question contains five
lected household. points Likert scales (1 = strongly disagree, 2 = disagree,
Pregnancy was ascertained by maternal self-report and 3 = neutral, 4 = agree, 5 = strongly agree). The total score
presumptive signs and symptoms of pregnancy such as was 5–25 and women who had scored ≥60% were con-
amenorrhea and/or increased uterine-size. Moreover, sidered as having positive SNs.
the Expected Date of Delivery (EDD) and Gestational Perceived behavioral control (PBC) towards MWHs
Age (GA) were calculated by using the first day of the is an indicator of the extent to which women feel
Last Normal Menstrual Period (LNMP) for women who confident to utilize MWHs. PBC was measured by
remembered that and measuring the fundal height to es- using three questions: 1) For me to use MWH is very
timate GA for women who did not remember their easy in our community; 2) If I want, I am confident
dates. Based on GA, decisions were made whether that I can use MWH in the last 2–4 weeks of my
the pregnancy was term (> 37 weeks) or not. pregnancy; 3) Using MWHs is possible in our set up.
Each question contains five points Likert scales (1 =
Measurements and variables strongly disagree, 2 = disagree, 3 = neutral, 4 = agree,
Intention to use MWHs was measured using three ques- 5 = strongly agree). The total score ranged from 3 to
tions: 1) I plan to use MWH for the last remaining 2–4 15 and women who had scored ≥60% were considered
weeks of my current pregnancy; 2) I will make my effort as having positive PBC.
to use MWH for my current pregnancy; 3) I intend to use Mode of transport to health facilities was assessed
MWH for my current pregnancy. Each question contains through asking mode of transport during obstetric
five points Likert scales (1 = strongly disagree, 2 = disagree, emergencies and women’s responses were categorized
3 = neutral, 4 = agree, 5 = strongly agree). As a result, the as on foot/carried by others, private bus or ambu-
total score was 3–15, and women who scored ≥60% were lance. Distance to reach health facilities was measured
considered as women who intended to use MWHs. by asking how long it would take to reach the nearest
Knowledge of women about maternal healthcare and health center or hospital from their house on foot in
obstetric complications in our study was measured by minutes and categorized as less than 60 min and 60
using eight questions: 1) Have you ever heard about ma- min or more.
ternity waiting homes in health facilities? 2) Do you Obstetric history was assessed by asking previous ob-
know about the danger signs of pregnancy? 3) Do you stetric characteristics and utilization of antenatal care,
know your expected date of delivery? 4) Do you know place of birth, postnatal care, stillbirth history, and facilityEndayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 4 of 10
type. A residence was considered to be urban if women < 0.05 were used to identify factors associated with
for the last 6 months stayed in areas identified by the mu- intentions to use MWHs.
nicipality as a town.
Wealth status was measured by assessing any property Results
of households using principal component analysis. Socio-demographic characteristics
Wealth status was categorized as low (poor), medium, A total of 499 (95%) pregnant women participated in
and high (rich). The source of information about MWHs the study. Almost half (233/499; 47.9%) of the partici-
has been assessed by using their most frequent source of pants were in the age range of 25–34 years, the ma-
information. jority was unable to read and write (410/499; 82.2%),
Intention to use MWHs was the dependent variable housewives (460/499; 92.2%), married (455/499;
whereas factors such as socio-demographic and eco- 91.2%), Orthodox Christians (481/499; 96.4%), rural
nomic factors, maternal knowledge, attitude, subject- residents (383/499; 76.8%) and (166/499; 33.3%) had
ive norm, perceived behavioral control, transportation, the poorest wealth status (Table 1). The study also
distance, and obstetric history were independent vari- revealed that 363/499 (72.7%) husbands were unable
ables of the study. to read and write, and 442/499 (88.6%) were farmers.
Twenty-one percent (105/499) of pregnant women
made maternal health care decisions by themselves,
Data collection tools and procedures 214/499 (42.9%) of them had good knowledge about
Data were collected using interviewer-administered maternal health care and pregnancy-related complica-
structured questionnaires adapted from previous stud- tions, 167/499 (33.5%) took more than an hour to
ies [15, 16, 18]. The questionnaire was first prepared reach the nearest health facility, and coming on foot
in English and translated to Amharic, and finally back or carried by others was means of transport for 232/
to English to ensure consistency. Six diploma gradu- 499 (46.5%) of participants during emergencies.
ated midwives were recruited as data collectors and Health workers were the source of information about
two Bachelor of Science (BSc) graduated midwives as maternal health care for 347/499 (69.5%) women
supervisors. Two days of training was given for data (Table 1).
collectors and supervisors on basic techniques of data
collection. A pre-test was done among 26 women in
Obstetric characteristics
west Bellesa district who had similar setups as the
Among participants, 436/499 (87.4%) women had at
study area and some modifications such as language
least one previous birth (multigravida), 76/499 (15.2%)
editing for ambiguous questions were made. Supervi-
had five or more pregnancies, 363/499 (72.7%) had
sors followed up the process of data collection daily,
started ANC, and 219/436 (50.2%) had PNC for their
checked data for completeness and consistency, and
previous births. Besides, 24/436 (5.5%) women had a
communicated with the principal investigator to be
previous history of MWH utilization and 19 of these
able to take immediate measures.
women were referred by Health Extension Workers to
MWHs, out of whom seven stayed more than 2 weeks in
a MWH (Table 2).
Data management and analysis
Data were analyzed using EPI -INFO version 7.1soft-
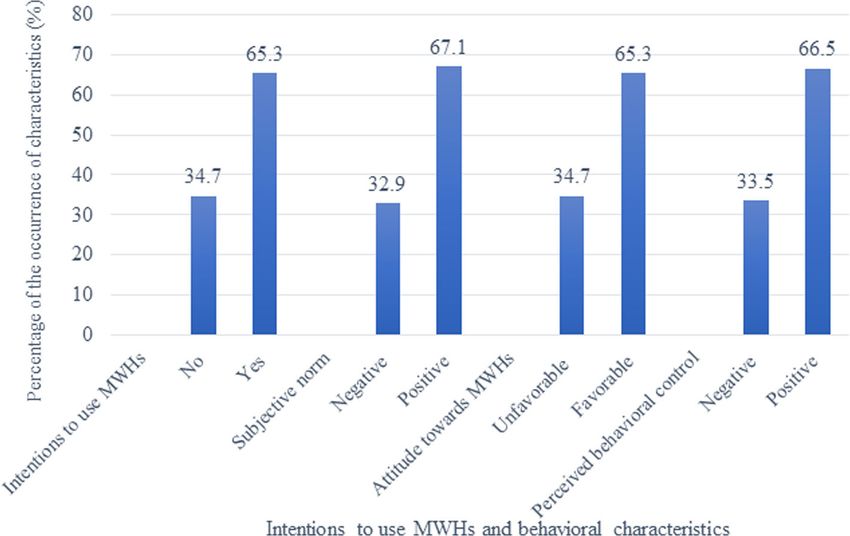
ware and exported to SPSS version 20. To reduce Intentions to use MWHs and behavioral characteristics
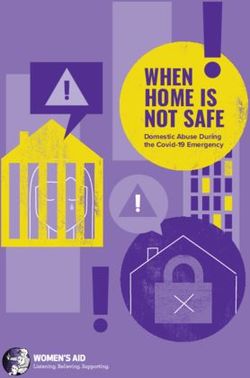
missing data, we used double data entry methods. If The study revealed that 326/499 (65.3%) women
we faced missing data, data were re-entered through intended to use MWHs. Moreover, pregnant women
retrieving data from hard copies. Data cleaning and had positive subjective norms (335/499; 67.1%),
close supervision were also conducted daily. Ques- perceived behavioral control (332/499; 66.5%), and fa-
tionnaires, however, with incomplete and unretrieva- vorable attitudes (326/499; 65.3%) towards MWHs
ble data were considered as non-response. (Fig. 1).
Completeness of the data was checked by running
frequencies and cross-tabulation. Recoding, valuing, Factors associated with intentions to use MWHs
transforming, computing, and categorizing variables Women had higher odds of intending to use MWHs if
were done before analysis. Binary logistic regression they had attended ANC compared to those who did not
was performed and those variables having p-values < (aOR 2.24; 95% CI 1.2–4.1). Women who made health
0.2 were fitted into multivariable logistic regression care decisions by themselves (aOR 2.74; 95% CI 1.2–6.2)
analysis. In multivariable logistic regression analysis, and were categorized as having medium (aOR 2.38; 95%
adjusted Odds Ratio (aOR) with 95% CI and p-value CI 1.3, 4.5) and rich wealth status (aOR 4.21; 95% CI 2.1–Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 5 of 10
Table 1 Socio-demographic characteristics of pregnant women Table 1 Socio-demographic characteristics of pregnant women
in East Bellesa district northwest Ethiopia, 2018 in East Bellesa district northwest Ethiopia, 2018 (Continued)
Variables Category Frequency Percent Variables Category Frequency Percent
(%) (%)
Age of women in years < 25 245 49.1 Mass media 95 19.0
25–34 233 46.7 Knowledge of mothers Not knowledgeable 285 57.1
≥ 35 21 4.2 Knowledgeable 214 42.9
Residence Rural 383 76.8
Urban 116 23.2
Maternal education Unable to read and 410 82.2 8.4) were more likely to use MWHs compared to poor
write
women (Table 3).
Primary school 65 13.0
Women who had good knowledge about maternal
Secondary and 24 4.8 health care and obstetric complications (aOR 6.40; 95%
above
CI 3.6–11.5), positive SNs (aOR 5.14; 95% CI 2.9–9.2),
Maternal occupation Housewives 460 92.2 positive PBC (aOR 4.74; 95% CI 2.7–8.4), and favorable
Merchants 26 5.2 attitudes (aOR 1.86; 95% CI 1.0–3.4) were more likely to
Government 13 2.6 use MWHs compared to those without those risk factors
employees (Table 3).
Current marrital status Unmarried 44 8.8
Married 455 91.2 Discussion
Religion Orthodox 481 96.4 Our study revealed that 65.3% of 499 women had inten-
tions to use MWHs. This percentage is lower than in
Muslim 18 3.6
Wolaita Sodo town, Ethiopia (75.5%), and Nyanza Prov-
Husband’s education Unable to read 363 72.7
and write
ince, Kenya (76.9%) [19]. It is higher, however, than in
Jimma district, Ethiopia (57.3%) [15], four districts of
Primary school 93 18.6
Eastern Gurage Zone, Southern Ethiopia (55.1%) [16],
Secondary and 43 8.6 and rural Kenya (45%) [20]. Possible explanations may
above
be differences in study participants, areas, period, and
Husband’s occupation Farmer 442 88.6
design. In some areas, the study was only conducted in
Merchants 37 7.4 health facilities among ANC attendants or urban
Government 20 4.0 dwellers who may have a better understanding of mater-
employee nal health issues. On the other hand, some studies were
Family size < 3 183 36.7 done at the community level, particularly in rural set-
3–4 172 34.5 tings. These women may have lower levels of awareness
≥5 144 28.9 due to a lack of information about maternal health care,
Wealth status Poor 166 33.3
including MWHs.
Women who attended ANC had higher odds of in-
Medium 175 35.1
tentions to use MWHs than participants who did not.
Rich 158 31.7 This finding is supported by studies in Tsegedie,
Decision maker Partner 139 27.9 North Gondar, Bahir Dar town, and Tigray region,
Together 255 51.1 Ethiopia, [21–24]. The possible explanation may be
Woman 105 21.0 fear of complications during childbirth as a result of
Time to reach nearest Less than 60 min 332 66.5
education by midwives to use MWHs during ANC
health facility visits. Even women who attended ANC in health fa-
60 or more minutes 167 33.5
cilities without MWHs were advised to go and wait
Transport during On foot/carried by 232 46.5 for birth in district hospitals or health centers with
emergency others
MWHs. Women attending ANC have the chance to
Private bus 56 11.2
familiarize themselves with the health facilities’ envi-
Ambulance 211 42.5 ronments. This may reduce unnecessary fear and
Source of information Health care 347 69.5 stress related to institutional birth. Moreover, women
providers may also be better informed about danger signs and
Health 57 11.4 obstetric complications that may occur during preg-
development army
nancy and childbirth [25].Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 6 of 10
Table 2 Obstetric histories in East Bellesa district northwest Ethiopia, 2018
Variables Category Frequency Percent (%)
Gravidity < 5 423 84.8
≥5 76 15.2
ANC visit No 136 27.3
Yes 363 72.7
Number of ANC visits (n = 363) 1 71 19.6
2 129 35.5
3 119 32.8
≥4 44 12.1
Type of HF for ANC (n = 363) Health post 33 9.1
Health center 273 75.2
Hospital 57 15.7
Gave childbirth previously No 63 12.6
Yes 436 87.4
Place of last birth (n = 436) Health facility 156 35.8
Home 280 64.2
Stillbirth No 457 91.6
Yes 42 8.4
Abortion No 452 90.6
Yes 47 9.4
Number of children 0 65 13.0
1–4 413 82.8
≥5 21 4.2
Postnatal care (n = 436) No 217 49.8
Yes 219 50.2
Use MWH previously (n = 436) No 412 94.5
Yes 24 5.5
Referred by (n = 24) Self 5 20.8
HEWs 19 79.2
Length of stay at MWH (in weeks) (n = 24) ≤2 17 70.8
>2 7 29.2
Family attendant at MWH (n = 24) No one 3 12.5
Husband and his families 11 45.8
Women’ families 10 41.7
Financial supporter in MWH (n = 24) Self 6 25.0
Husband / partner 2 8.3
Health facility 16 66.7
Odds of intentions to use MWHs among respon- husbands want their wives to stay at home until the
dents who decided by themselves were higher than in expected date of delivery because of heavy workload
the case decisions made by their husbands. This is and family care. Refusal of admission by husbands
supported by studies in rural health centers in Am- may be because of a lack of other adult caretakers at
hara, Oromia, Southern Nations Nationalities and home. This could be the reason why women in re-
People (SNNP), and Tigray regions Ethiopia and mote areas are not motivated to come to MWHs be-
Kenya [13, 20]. A possible explanation might be that cause the whole household is dependent on womenEndayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 7 of 10 Fig. 1 Intentions to use and behavioural characterstics towards MWHs among pregnant women in East Belessa district northwest Ethiopia, 2018 for all household support [13]. On the contrary, stud- women who are well aware of maternal healthcare ies in Attat hospital, Ethiopia [26], rural southern services and obstetric complications may fear bad Egypt (Upper Egypt) [27], rural Zambia [28] and Si- outcomes of birth at home. Similarly, women’s favor- erra Leone [29] reported that husbands played im- able attitudes towards MWHs were in agreement portant roles to encourage their wives to use MWHs. with studies in Jimma district, Ethiopia, rural They possibly have positive attitudes towards MWHs Zimbabwe, and Zambia [15, 28, 38, 39]. This might and perceived benefits from using MWHs, including be due to the wrong perceptions of community mitigating long distances and improving access to members that women admitted to MWHs are lazy facility-based delivery care. or careless to abandon their families [13]. Respon- Women with a medium and rich wealth status had dents’ subjective norms were also consistent with higher odds of intentions to use MWHs compared findings in Wolaita Sodo town and Jimma district, to women with poor wealth. This is in line with Ethiopia [15, 18]. Women with positive perceptions studies in rural Timor Leste, Mayan women in of social pressure may possibly have more inclination Guatemala, remote areas of Nepal, and Southern Lao to utilize maternal healthcare services. Moreover, PDR [30–34]. Possible explanations might be the women’s perceived behavioral control in our study costs of public transport and other costs associated was in line with studies in Jimma district, Ethiopia, with the use of MWHs. Availability of free ambu- and Kalomo, Zambia [15, 40]. Women who have lance services, lessening of costs associated with positive perceived behavioral control may feel more using MWHs, and subsequent institutional birth are confident to utilize MWHs. important strategies for enhancing MWH utilization. Maternal knowledge, subjective norms, and wealth Women with knowledge about maternal services status had the highest odds for intentions to use and obstetric complications, with favorable attitudes MWHs. The more favorable attitudes and subjective towards the overall evaluation of MWHs, positive norms, the greater perceived control resulted in subjective norms related to women’s perceptions on stronger women’s intentions to use MWHs with fewer social pressure and perceived behavioral control on worries about food shortages and the costs of trans- the extent to which they feel confident to utilize port [15, 38]. MWHs had higher odds of using MWHs compared with their counterparts. The effect of woman’s knowledge on MWHs is in line with studies in Limitation of the study Timor Leste, Bangladesh, and Northern Sierra Leone One limitation of our study was that it could not show [29, 35–37]. Possible justification might be that any cause-effect relationship. Beliefs of the women
Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 8 of 10
Table 3 Factors associated with women’s intentions to use MWHs in East Bellesa district northwest Ethiopia, 2018
Variables Category Intention to use MWH cOR (95%CI) aOR (95% CI)
Yes No
Age of women in years Less than 30 283 147 1 1
30 or more 43 26 0.86 (0.5,1.5) 0.97 (0.6,2.9)
Current marital status Unmarried 29 15 1 1
Married 297 158 0.97 (0.5,1.9) 0.60 (0.2,1.6)
Maternal education Unable to read & write 260 150 1 1
Primary school 48 17 1.63 (0.9,2.9) 1.78 (0.8,4.0)
Secondary & above 48 6 1.73 (0.7,4.5) 1.56 (0.4,6.1)
Gravidity < 5 269 154 1 1
≥5 57 19 1.72 (1.0,3.0) 1.61 (0.6,4.2)
Family size < 3 120 63 1 1
3–4 114 58 1.03 (0.7,1.6) 1.02 (0.5,2.0)
≥5 92 52 0.93 (0.6,1.5) 0.85 (0.5,1.8)
ANC visit No 77 59 1 1
Yes 249 114 1.67 (1.1,2.5) 2.24 (1.2,4.1) *
Decision-maker Husband 74 65 1 1
Together (both) 171 84 1.79 (0.8,3.4) 1.52 (0.4,2.6)
Herself 81 24 2.96 (1.9,6.5) 2.74 (1.2,6.2) *
Transport during emergency Foot / carried by others 135 95 1 1
Private transport 36 20 1.25 (0.7,2.3) 1.22 (0.5,3.0)
Ambulance 153 58 1.83 (1.2,2.7) 1.37 (0.8,2.4)
Time to nearest health facility Less than 60 min 215 117 1 1
60 or more minutes 111 56 1.08 (0.7,1.6) 1.04 (0.5,1.4)
Subjective norm Negative 52 112 1 1
Positive 274 61 9.68 (6.3,14.9) 5.14 (2.9,9.2) *
Attitudes towards MWH Unfavorable 56 68 1 1
Favorable 270 105 3.12 (2.1,4.8) 1.86 (1.0,3.4) *
Perceived behavioural control Negative 59 108 1 1
Positive 267 65 7.52 (5.0,11.4) 4.74 (2.7,8.4) *
Wealth status Poor 91 75 1 1
Medium 116 59 1.62 (1.1,2.5) 2.38 (1.3,4.5) *
Rich 119 39 2.51 (1.6,4.0) 4.21 (2.1,8.4) *
Knowledge of women Not knowledgeable 140 145 1 1
Knowledgeable 186 28 6.88 (4.3,10.9) 6.40 (3.6,11.5) *
*significant at p-value < 0.05
towards intentions to use MWHs may not be fully ad- utilization were significantly associated with intentions
dressed since the study lacked a qualitative approach. to use MWHs. Improving women’s attitudes and behav-
We also did not address the needs and beliefs of the ioral perceptions through awareness creation by con-
women’s partners, indicating gender inequality bias. tinuous health education during ANC visits, devising
strategies to improve wealth status, and strengthening
Conclusion women’s decision-making power in the household may
Two third of the women in this study had the intention enhance women’s intentions to use MWHs.
to use MWHs. Factors such as women’s attitudes, sub-
Abbreviations
jective norms, perceived behavioral control, decision- ANC: Ante-natal care; BP: Birth place; EDHS: Ethiopian demographic health
making power, knowledge, wealth status, and ANC survey; HC: Health center; HF: Health facility; HP: Health post; MNH: MaternalEndayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 9 of 10
and newborn health; MMR: Maternal mortality ratio; MWH: Maternity waiting 3. World Health Organization. Maternal deaths fell 44% since 1990–UN: Report
home; PBC: Perceived behavioural control; PNC: Post natal care; from WHO, UNICEF: UNFPA, World Bank Group, and the United Nations
RHB: Regional health bureau; SN: Subjective norm; SDA: Skilled delivery Population Division. Geneva: WHO; 2015.
attendance; WB: World bank; WHO: World health organization 4. World Health Organization and UNICEF. Trends in maternal Mortality: 1990-
2015: Estimates from WHO, UNICEF, UNFPA, World Bank Group and the
Acknowledgements United Nations Population Division. Geneva; WHO; 2015.
Authors would like to thank the Institute of Public Health, College of 5. Central Stastical Agency (CSA). Ethiopia Demographic and Health Survey.
Medicine and Health Sciences, the University of Gondar for allowing us Addis Ababa: CSA; 2016.
to conduct this study. Our gratitude goes to East Belessa District Health 6. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci
Office staff members for their co-operation by providing the necessary Med. 1994;38:1091–110.
information. Finally, we would like to thank the study participants and 7. Kelly J, Kohls E, Poovan P, Schiffer R, Redito A, Winter H, MacArthur C. The
data collectors. role of a maternity waiting area (MWA) in reducing maternal mortality and
stillbirths in high-risk women in rural Ethiopia. BJOG. 2010;117:1377–83.
Ethics approval and consent to participants 8. Gaym A, Pearson L, Soe K. Maternity waiting homes in Ethiopia--three
Ethical clearance was obtained from the Ethical Review Committee of the decades experience. Ethiop Med J. 2012;50:209–19.
Institute of Public Health, University of Gondar. Before communicating study 9. World Health Organization: Making pregnancy safer: the critical role of the
participants, an official permission letter of cooperation was obtained from skilled attendant. a joint statement by WHO, ICM and FIGO,2004.
Amhara National Regional State Health Bureau, North Gondar Zonal Health 10. World Health Organization: Health in 2015: from MDGs, millennium
Department, East Belessa District Health Office, and respective kebeles. development goals to SDGs, sustainable development goals. 2015.
Written informed consent was taken from each participant. Each eligible 11. Andemichael G, Haile B, Kosia A, Mufunda J. Maternity waiting homes: a
participant was informed about the purpose and importance of the study. panacea for maternal/neonatal conundrums in Eritrea. JEMA. 2009;4:18–21.
Participants were also assured that their name was not written on the 12. Braat F, Vermeiden T, Getnet G, Schiffer R, van den Akker T, Stekelenburg J.
questionnaire and confidentiality of the data kept at all levels. Comparison of pregnancy outcomes between maternity waiting home
users and non-users at hospitals with and without a maternity waiting
Authors’ contributions home: retrospective cohort study. Int Health. 2018;10:47–53.
ME designed the study, developed data collection tools, performed the 13. Tiruneh GT, Taye BW, Karim AM, Betemariam WA, Zemichael NF, Wereta TG,
analysis and interpretation of data, and drafted the paper. MY and AD Lemango ET. Maternity waiting homes in rural health centers of Ethiopia:
participated in the development of the study proposal, analysis and the situation, women’s experiences and challenges. Ethiop J Health Dev.
interpretation, revised drafts of the paper, revised the manuscript. All authors 2016;30:19–28.
read and approved the final manuscript. 14. van Lonkhuijzen L, Stekelenburg J, van Roosmalen J. Maternity waiting
facilities for improving maternal and neonatal outcome in low-resource
countries. Cochrane Database Syst Rev. 2012;10:CD006759.
Authors’ information
ME is a Health Service Management professional at the East Belessa District 15. Endalew GB, Gebretsadik LA, Gizaw AT. Intention to use maternity waiting
Health Office, North Gondar Zone, Ethiopia. home among pregnant women in Jimma District, Southwest Ethiopia.
MY is an Associate Professor of Health Service Management and Health GJMR-K. 2016;16:29–35.
Economics at the Department of Health Systems and Policy, Institute of 16. Vermeiden T, Braat F, Medhin G, Gaym A, van den Akker T, Stekelenburg J.
Public Health, University of Gondar, Gondar, Ethiopia. Factors associated with intended use of a maternity waiting home in
AD is Assistant Professor of Health Service Management in the Department southern Ethiopia: a community-based cross-sectional study. BMC
of Health Systems and Policy at the Institute of Public Health, College of Pregnancy Childbirth. 2018;18:38.
Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia. 17. Amhara National Regional State Finace Bureau: population estimation of
East Bellesa district,. 2017.
18. Lera T, Admasu B, Dirar A. Intention to use institutional delivery and
Funding
associated factors among ANC attendants in Wollaita Soddo town, southern
This is part of a master thesis funded by the principal investigator.
Ethiopia: a cross-sectional community based study, application of theory of
planned behavioral model. Am J Public Health Res. 2017;5:89–97.
Availability of data and materials 19. Creanga AA, Odhiambo GA, Odera B, et al. Pregnant Women’s intentions and
Datasets supporting the conclusions of this article are available upon request subsequent behaviors regarding maternal and neonatal service utilization: results
to the corresponding author. Due to data protection restrictions and from a cohort study in Nyanza Province, Kenya. PLoS One. 2016;11:e0162017.
participant confidentiality, we do not make participants’ data publicly 20. Mramba L, Nassir FA, Ondieki C, Kimanga D. Reasons for low utilization of a
available. maternity waiting home in rural Kenya. Int J Gynaecol Obstet. 2010;108:152–3.
21. Tsegay Y, Gebrehiwot T, Goicolea I, Edin K, Lemma H, San Sebastian M.
Consent for publication Determinants of antenatal and delivery care utilization in Tigray region,
Not applicable. Ethiopia: a cross-sectional study. Int J Equity Health. 2013;12:30.
22. Hailu D, Berhe H. Determinants of institutional childbirth service utilisation
Competing interests among women of childbearing age in urban and rural areas of Tsegedie
The authors declare that they have no competing interests. district, Ethiopia. Midwifery. 2014;30:1109–17.
23. Abeje G, Azage M, Setegn T. Factors associated with institutional delivery
Author details service utilization among mothers in Bahir Dar City administration, Amhara
1
East Bellesa District Health Office, North Gondar Zone, Amhara National region: a community based cross sectional study. Reprod Health. 2014;11:22.
Regional Health Bureau, Bahir Dar, Ethiopia. 2Department of Health Systems 24. Worku AG, Yalew AW, Afework MF. Maternal complications and women's
and Policy, Institute of Public Health, College of Medicine and Health behavior in seeking care from skilled providers in North Gondar. Ethiopia
Sciences, University of Gondar, P. O. Box, 196 Gondar, Ethiopia. PLoS One. 2013;8:e60171.
25. Fekadu GA, Kassa GM, Berhe AK, Muche AA, Katiso NA. The effect of antenatal
Received: 17 January 2019 Accepted: 30 April 2020 care on use of institutional delivery service and postnatal care in Ethiopia: a
systematic review and meta-analysis. BMC Health Serv Res. 2018;18:577.
26. Vermeiden T, Schiffer R, Langhorst J, et al. Facilitators for maternity waiting
References home utilisation at Attat hospital: a mixed-methods study based on 45
1. World Health Organization. WHO recommendations on health promotion years of experience. Tropical Med Int Health. 2018;23:1332–41.
interventions for maternal and newborn health. Geneva: WHO; 2015. 27. Ohashi A, Higuchi M, Labeeb SA, Mohamed AG, Chiang C, Aoyama A.
2. World Health Organization. Maternity waiting homes: a review of Family support for women’s health-seeking behavior: a qualitative study in
experiences. Geneva: World Health Organization; 1996. rural southern Egypt (upper Egypt). Nagoya J Med Sci. 2014;76:17–25.Endayehu et al. BMC Pregnancy and Childbirth (2020) 20:281 Page 10 of 10
28. Sialubanje C, Massar K, van der Pijl MS, Kirch EM, Hamer DH, Ruiter RA.
Improving access to skilled facility-based delivery services: Women’s beliefs
on facilitators and barriers to the utilisation of maternity waiting homes in
rural Zambia. Reprod Health. 2015;12:61.
29. Kyokan M, Whitney-Long M, Kuteh M, Raven J. Community-based birth
waiting homes in northern Sierra Leone: factors influencing women's use.
Midwifery. 2016;39:49–56.
30. Wild K, Barclay L, Kelly P, Martins N. The tyranny of distance: maternity
waiting homes and access to birthing facilities in rural Timor-Leste. Bull
World Health Organ. 2012;90:97–103.
31. Ruiz MJ, van Dijk MG, Berdichevsky K, Munguía A, Burks C, García SG.
Barriers to the use of maternity waiting homes in indigenous regions of
Guatemala: a study of users' and community members' perceptions. Cult
Health Sex. 2012;15:205–18.
32. Schooley J, Mundt C, Wagner P, Fullerton J, O’Donnell M. Factors
influencing health care-seeking behaviours among Mayan women in
Guatemala. Midwifery. 2009;25:411–21.
33. Shrestha SD, Rajendra PK, Shrestha N. Feasibility study on establishing
maternity waiting homes in remote areas of Nepal. Regional Health Forum.
2007;11:33–8.
34. Eckermann E, Deodato G. Maternity waiting homes in southern Lao PDR:
the unique ‘silk home’. J Obstet Gynaecol Res. 2008;34:767–75.
35. Gabrysch S, Campbell OM. Still too far to walk: literature review of the
determinants of delivery service use. BMC Pregnancy Childbirth. 2009;9:34.
36. Islam N, Islam MT, Yoshimura Y. Practices and determinants of delivery by
skilled birth attendants in Bangladesh. Reprod Health. 2014;11:86.
37. Wild K, Barclay L, Kelly P, Martins N. Birth choices in Timor-Leste: a
framework for understanding the use of maternal health services in low
resource settings. Soc Sci Med. 2010;71:2038–45.
38. Glanz K, Rimer BK, Viswanath K. Health behavior and health education:
theory, research, and practice. San Francisco: Jossey-Bass; 2008.
39. Millard L. Antenatal village stay and pregnancy outcome in rural Zimbabwe.
Cent Afr J Med. 1991;37:1–4.
40. Sialubanje C, Massar K, Hamer DH, Ruiter RA. Personal and environmental
predictors of the intention to use maternal healthcare services in Kalomo,
Zambia. Health Educ Res. 2014;29:1028–40.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in
published maps and institutional affiliations.You can also read