Valvular Heart Disease in Pregnancy - Jennifer Lewey, MD, MPHa,*, Lauren Andrade, MDb, Lisa D. Levine, MD, MSCEc - BINASSS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Val v u l a r H e a r t D i s e a s e i n
Pregnancy
Jennifer Lewey, MD, MPHa,*, Lauren Andrade, MDb, Lisa D. Levine, MD, MSCEc
KEYWORDS
Valvular heart disease Pregnancy Mitral stenosis Aortic stenosis Mechanical heart valve
Anticoagulation
KEY POINTS
Pregnancy is well tolerated in most women with valvular heart disease. Cardiac output increases up
to 50% and can lead to clinical decompensation in high-risk women.
Women with mechanical heart valves need careful management of anticoagulation during preg-
nancy to minimize maternal and fetal risks.
Vaginal delivery with epidural anesthesia is recommended for most women with stable valvular
heart disease.
All women with valvular heart disease should be managed by a multidisciplinary Pregnancy Heart
Team before and during pregnancy.
INTRODUCTION are pregnant or considering pregnancy should be
managed by a multidisciplinary Pregnancy Heart
Cardiovascular (CV) disease complicates an esti- Team consisting of cardiologists and high-risk
mated 1% to 4% of all pregnancies and is the obstetricians.
leading cause of death in pregnant and post- Hemodynamic changes start early in pregnancy.
partum women in the United States.1,2 Valvular Cardiac output increases 30% to 50% and peaks
heart disease is a common cause of CV disease between the second and third trimesters.7,8
that affects women of childbearing age.3,4 Changes in cardiac output are driven by an in-
Congenital heart disease is the leading cause of crease in stroke volume in the first half of preg-
valvular heart disease in the United States; howev- nancy followed by a gradual rise in heart rate. As
er, rheumatic heart disease is a prevalent condi- a result of placental maturation, systemic vascular
tion especially among immigrant populations.5,6 resistance and blood pressure decrease in the first
Most women with valvular heart disease will do and second trimesters and returns to pre-
well during pregnancy, but high-risk conditions pregnancy levels in the third trimester. Women
such as severe mitral stenosis (MS) or aortic ste- with valvular heart disease, especially left-sided
nosis (AS), can be associated with significant obstructive lesions, may have limited cardiac
maternal morbidity and mortality. Management of reserve to accommodate these hemodynamic
anticoagulation of pregnant women with mechan- changes. As a result, close serial monitoring during
ical heart valves presents unique challenges to pregnancy is necessary to assess for clinical
reduce the risk of maternal and fetal complica- decompensation. The changes in flow can lead
tions. Women with valvular heart disease who
a
Division of Cardiology, Department of Medicine, University of Pennsylvania Perelman School of Medicine,
cardiology.theclinics.com
Perelman Center for Advanced Medicine, 3400 Civic Center Boulevard, 2-East Pavilion, Philadelphia, PA
19104, USA; b Philadelphia Adult Congenital Heart Center, University of Pennsylvania, Children’s Hospital of
Philadelphia, Perelman Center for Advanced Medicine, 3400 Civic Center Boulevard, 2- East Pavilion, Philadel-
phia, PA 19104, USA; c Department of Obstetrics and Gynecology, Maternal and Child Health Research Center,
University of Pennsylvania Perelman School of Medicine, 3400 Spruce Street, 2 Silverstein, Philadelphia, PA
19104, USA
* Corresponding author.
E-mail address: jennifer.lewey@pennmedicine.upenn.edu
Cardiol Clin 39 (2021) 151–161
https://doi.org/10.1016/j.ccl.2020.09.010
0733-8651/21/Ó 2020 Elsevier Inc. All rights reserved.
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.152 Lewey et al
to increases in mitral and aortic transvalvular gra- with newly diagnosed or newly symptomatic
dients and an overestimation of lesion severity. valvular heart disease and collaborative care be-
Direct valve planimetry for patients with AS or tween MFM, cardiology, anesthesia, and other
MS may more accurately reflect the degree of specialists is needed to reduce ongoing maternal,
valve stenosis, especially for patients newly diag- obstetric, and fetal risk.
nosed during pregnancy. The hypercoagulable
state of pregnancy increases the risk of thrombo- RISK ASSESSMENT
embolic events during pregnancy and the first 6
to 12 weeks postpartum, further complicating the The most common maternal complications of
anticoagulation management of women with me- valvular heart disease during pregnancy are heart
chanical valves.9 failure, arrhythmias, and thromboembolic compli-
Labor and delivery is associated with sudden cations. Postpartum hemorrhage can be a com-
hemodynamic changes and increases in oxygen mon complication for women on anticoagulation.
consumption. After delivery, dramatic changes in Cardiac symptoms can be managed in many
hemodynamics occur as a result of autotransfu- women with diuresis, medical therapy, and
sion of uterine blood volume, relief of caval pres- reducing level of physical activity. If symptoms
sure, and mobilization of dependent edema. The are refractory to conservative management, valve
sudden increase in preload can lead to clinical intervention during pregnancy may be necessary.
decompensation and women with high-risk le- Percutaneous balloon valvuloplasty performed by
sions will need to be followed closely immediately experienced operators is preferred for stenotic le-
after delivery and in the subsequent days post- sions. Ideally these interventions should be per-
delivery. formed after the fourth month in the second
trimester to minimize radiation exposure during
PRECONCEPTION COUNSELING organogenesis.6 Valve surgery with cardiopulmo-
nary bypass performed during pregnancy is asso-
Reproductive age women with valvular heart dis- ciated with rates of fetal death up to 30%,
ease should undergo counseling before concep- especially when surgery is emergent and/or per-
tion by a collaborative Pregnancy Heart Team formed at early gestational age.11,12 If surgery is
consisting of a maternal fetal medicine (MFM) needed, however, the second trimester is the
specialist and cardiologist with experience in car- preferred time frame with use of high flow on car-
ing for pregnant women with heart disease.10 diopulmonary bypass to provide adequate
The goal of preconception counseling is to review placental perfusion.13
and individualize the maternal and fetal risk of Maternal cardiac risk can be estimated using the
pregnancy. Baseline cardiac function should be lesion specific modified World Health Organization
assessed with an electrocardiogram and echocar- (WHO) classification (Table 1).6 Women with se-
diogram to start. Exercise stress testing can be an vere MS and severe symptomatic AS are consid-
important tool to assess exercise capacity, devel- ered to be at extremely high risk of maternal
opment of arrhythmias and symptomatic morbidity or mortality (WHO IV) and pregnancy is
response, which may guide risk stratification and contraindicated. Most other types of valvular heart
treatment before conception. Additional imaging disease in pregnancy are considered to be moder-
modalities such as cardiac MRI or computed to- ate to high risk (WHO II-III). Those with regurgitant
mography may be used to further assess valvular lesions such as aortic regurgitation and mitral
function, anatomy of structures not well seen by regurgitation usually tolerate pregnancy well due
echocardiogram, and associated aortopathies. to the decreased systemic afterload during preg-
For women planning pregnancy, medications nancy. Individualized risk can be further estimated
should be reviewed for safety during pregnancy. using pregnancy-specific risk indices developed in
Angiotensin-converting enzyme inhibitors and large cohorts, including the CARPREG II and the
angiotensin receptor blockers are teratogenic ZAHARA models.4,14,15 Contraception should be
and can be changed to medications with a better discussed with all women with valvular heart dis-
safety profile during pregnancy. Bosentan and sta- ease but highly effective contraception should be
tins are also considered teratogenic and should be particularly recommended for women at high risk
stopped before pregnancy. For women with me- of pregnancy complications. Estrogen-containing
chanical valves taking warfarin, shared decision contraception increases the risk of venous and
making will help guide the appropriate choice of arterial thrombosis and hypertension and should
anticoagulation in the first trimester. Beta blockers be avoided in women with cardiac disease, espe-
are generally considered safe in pregnancy. cially those at increased thrombotic risk. In such
Women may frequently present during pregnancy patients, long-acting progesterone-only methods
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.Valvular Heart Disease in Pregnancy 153
Table 1
Modified World Health Organization (WHO) classification of pregnancy risk
WHO Classification Maternal Risk
WHO I Morbidity: little to no increased risk
Mild pulmonary stenosis Mortality: no increased risk
Small patents ductus arteriosus (PDA)
Mitral valve prolapse with mild mitral
regurgitation
Repaired simple lesions: ASD, VSD, PDA,
anomalous pulmonary venous drainage
Isolated atrial or ventricular ectopic beats
WHO II Morbidity: moderately increased risk
Uncorrected ASD or VSD Mortality: mildly increased risk
Repaired Tetralogy of Fallot
Most arrhythmias
WHO II-III Risk varies based on individual patient
Mild LV impairment (EF >45%) Morbidity: moderately to severely increased
Hypertrophic cardiomyopathy risk
Valvular heart disease not considered WHO Mortality: intermediate increased risk
I or IV
Marfan syndrome, aorta154 Lewey et al
Women with stable cardiac disease can undergo Women with moderate or severe stenosis (mitral
full-term delivery at 39 weeks of gestation.1 valve area (MVA)Valvular Heart Disease in Pregnancy 155
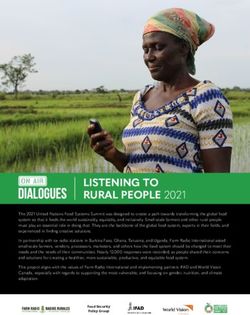
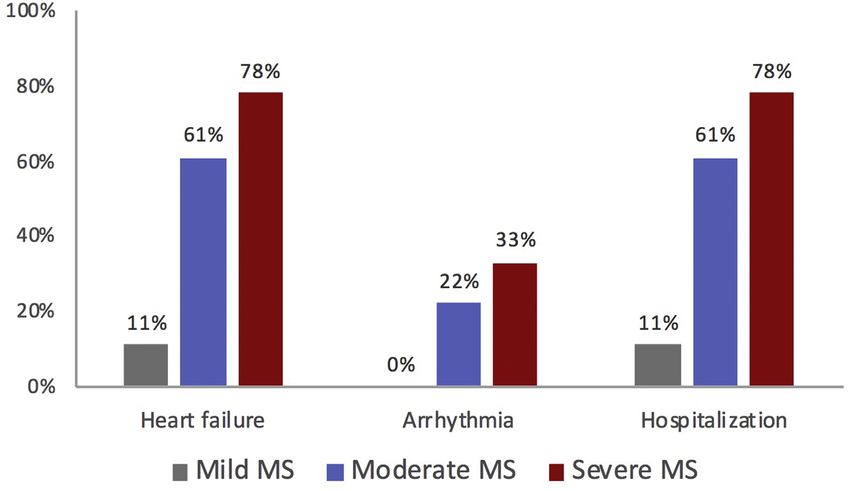
Fig. 1. Cardiac complication of MS according to severity. (Adapted from Hameed A, Karaalp IS, Tummala PP, Wani
OR, Canetti M, Akhter MW, Goodwin M, Zapadinsky N, Elkayam U. The effect of valvular heart disease on
maternal and fetal outcome of pregnancy. J Am Coll Cardiol. 2001;37:893–899; with permission.)
atrium, large left atrium (60 mL/m2), or conges- special care unit for at least 24 hours after deliv-
tive heart failure.1 Rate control with beta blockers ery is recommended.
or digoxin should be used as an initial strategy, Careful preconception counseling of women
though many women will ultimately undergo elec- with MS is critical in order to identify severity of
trical cardioversion (which is considered safe in stenosis, symptoms, and need for intervention
pregnancy) due to ongoing symptoms, poor rate before pregnancy. Similar to non-pregnant pa-
control, or hemodynamic instability. tients, the 2014 American Heart Association
Women who remain severely symptomatic (AHA)/American College of Cardiology (ACC)
despite adequate medical therapy and activity re- Valvular Heart Disease Guidelines recommends
striction may need to undergo mitral valve inter- PMBV, when feasible, in patients with severe
vention during pregnancy. Percutaneous mitral symptomatic MS (Class I recommendation) before
balloon valvotomy (PMBV) can be safely per- pregnancy. In order to avoid clinical decompensa-
formed during pregnancy and result in improved tion and need for intervention during pregnancy.
valve area and gradients.11,22 Due to risk of The AHA/ACC Guidelines also recommend
ionizing radiation to the fetus, PMBV should be PMBV in patients with severe MS who are asymp-
avoided during the first trimester, if possible, and tomatic (Class I recommendation). The decision to
performed by experienced operators. Surgical intervene in asymptomatic women before preg-
mitral valve replacement may be considered in nancy should depend on valve area, exercise
women with refractory symptoms who are not tolerance, and the presence of pulmonary hyper-
candidates for PMBV but is associated with high tension, especially among women who are not
rates of fetal mortality, estimated at 20% to candidates for PMBV.6,23,24
30%.11,12
Most women with MS can undergo a vaginal Aortic Stenosis
delivery with regional anesthesia, with preference
AS in pregnancy is most often caused by congen-
for epidural placement.23 An assisted second
ital bicuspid aortic valve and less commonly other
stage should be considered for women with mod-
congenital abnormalities or rheumatic heart dis-
erate to severe stenosis. Cesarean delivery is
ease.24,25 Pregnancy is well tolerated in women
reserved for obstetric indications and decompen-
with mild and moderate AS. Women with severe
sated heart failure. Due to the hemodynamic
AS are at higher risk of developing cardiac compli-
shifts that occur postpartum, monitoring in a
cations, such as heart failure or atrial arrhythmias,
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.156 Lewey et al
however the risk of maternal mortality and need for preload and systemic vascular resistance, which
aortic valve intervention during pregnancy is low. may poorly tolerated.
Women with congenital bicuspid valve or Marfan
syndrome may have an associated aortopathy MITRAL REGURGITATION AND AORTIC
which further increases maternal risk and warrants REGURGITATION
additional monitoring before and during preg-
nancy. Pregnancy is contraindicated in women The most common causes of mitral regurgitation
with bicuspid aortic valve when aortic dilation (MR) during pregnancy are rheumatic heart dis-
is >50 mm and in women with Marfan syndrome ease and mitral valve prolapse. Patients with pre-
when aortic dilation is >45 mm.6 viously repaired (or unrepaired) AV septal defects
In a Canadian cohort of 39 women representing may also have significant left-sided AV valve
49 pregnancies, cardiac complications, including regurgitation. In contrast, aortic regurgitation (AR)
heart failure or arrhythmias, were observed in is more commonly associated with congenital
10% of women with severe AS. Only 1 woman bicuspid aortic valve or aortopathy, and less
required aortic valve intervention during preg- commonly rheumatic heart disease. Both MR
nancy and no maternal deaths were reported.25 and AR are well tolerated during pregnancy, even
Other series have reported that heart failure oc- if severe, due to the fall in systemic vascular resis-
curs in 3.8% to 44% of patients, with the highest tance and blood pressure. Surgical intervention
rate observed in the smallest (n 5 12) before pregnancy is reserved for women meeting
cohort.19,26,27 Maternal complications are associ- routine indications for surgery, including severe
ated with severity of AS, especially when symp- symptomatic valve disease. Exercise testing
tomatic, and maternal age >30 years.26,27 before pregnancy can be considered to assess
Maternal mortality in contemporary cohorts and for exercise tolerance and symptoms.29 Women
need for valvular intervention during pregnancy is who develop heart failure symptoms or left ventric-
low. Valve deterioration and need for aortic valve ular dysfunction can be treated with diuretics and
intervention may be higher in women with severe vasodilators, such as hydralazine or nitrates, with
AS after pregnancy, although the causes for this care to avoid hypotension which can lead to
are not well-understood.25,26 Women with severe placental hypoperfusion. Angiotensin-converting
AS experience higher rates of preterm delivery, enzyme inhibitors and angiotensin receptor
low birth weight, and fetal death.19,26 blockers are contraindicated during pregnancy.
PULMONIC STENOSIS
Management Pulmonic stenosis (PS) is most commonly a result
Women who become symptomatic should be of congenital valve disease but may also occur as
managed with activity restriction. Diuretics should a result of homograft calcification after a Ross pro-
be carefully used in women who develop pulmo- cedure or prosthetic valve stenosis in patients with
nary edema so as to avoid a sudden drop in pre- repaired tetralogy of Fallot. Mild and moderate PS
load. Women who remain symptomatic despite are well tolerated during pregnancy. Severe PS is
conservative management may need valvular associated with high rates of hypertensive disor-
intervention during pregnancy with a preference ders, such as preeclampsia, preterm delivery,
for percutaneous aortic balloon valvuloplasty if and thromboembolic complications.30 Although
the valve anatomy is favorable and an experienced severe PS may be well tolerated during pregnancy,
team is available. Percutaneous transcatheter some women may experience right ventricular
aortic valve replacement for bicuspid severe AS heart failure or arrhythmias. As a result, women
has been successfully performed during preg- with severe PS, even if asymptomatic, should be
nancy, and may be preferred over valvuloplasty if considered for balloon valvuloplasty, surgical val-
significant aortic regurgitation is present.28 votomy, or percutaneous valve replacement
Women who develop severe symptoms early in before pregnancy.31
pregnancy may consider pregnancy termination.
Similar to patients with MS, vaginal delivery is PULMONIC REGURGITATION
the preferred mode of delivery with an assisted
second stage for women with moderate to severe Pulmonic regurgitation (PR) may be secondary to
stenosis, though Cesarean delivery may be prior tetralogy of Fallot repair, balloon valvulo-
considered for patients with severe symptoms.6,24 plasty for isolated PS, or develop in patients with
Regional anesthesia with an epidural is preferred a prior right ventricle to pulmonary artery conduit.
for pain control but hemodynamics should be PR is generally well tolerated during pregnancy.
monitored closely to avoid a sudden drop in Similar to the systemic vascular resistance,
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.Valvular Heart Disease in Pregnancy 157
pulmonary vascular resistance also decreases warfarin crosses the placenta and is associ-
during pregnancy. However, the increased plasma ated with an embryopathy, consisting of nasal
volume and CO associated with pregnancy can hypoplasia, stippled epiphyses, and choanal
lead to right-sided heart failure symptoms in atresia, when exposure occurs between 6
women with severe PR, especially in the presence and 12 weeks of gestation.37 Later exposure
of underlying right ventricular (RV) dysfunction, RV is associated with central nervous system ab-
hypertrophy, or additional obstructive lesions such normalities and intracranial hemorrhage. The
as branch pulmonary artery stenosis.32,33 Right- most common fetal adverse even is miscar-
sided heart failure can often be treated with di- riage and fetal demise can occur at any gesta-
uretics and activity restriction. Valve intervention tional age.
is rarely needed during pregnancy.6 In women Warfarin has a dose-dependent effect on fetal
with severe PR before pregnancy who are symp- outcomes with the highest risk associated with
tomatic or have progressive RV dilatation or daily warfarin doses >5 mg,38 though lower risk
dysfunction, pulmonary valve replacement is with lower doses has not been demonstrated in
recommended.31 all studies.36 In a 2017 meta-analysis, the rate
of livebirths among women taking 5 mg
TRICUSPID REGURGITATION compared with >5 mg of warfarin daily was
83.6% versus 43.9%, respectively.39 The rate
Isolated tricuspid regurgitation (TR) in young of embryopathy/fetopathy was 2.3% with lower
women is uncommon and, when present, occurs dose (5 mg) and 12.4% with higher dose
in the setting of Ebstein anomaly, rheumatic heart (>5 mg) of warfarin. Women treated with low mo-
disease, or endocarditis. Patients with AV septal lecular weight heparin (LMWH) alone during
defects commonly have right-sided AV valve pregnancy had the highest rate of livebirth at
regurgitation. The hemodynamic changes of preg- 92%.
nancy are usually well tolerated in women with TR, LMWH does not cross the placenta and is
even if severe. Ebstein anomaly is associated with therefore not associated with congenital malfor-
atrial septal defect and Wolff-Parkinson-White mations. Weight-based dosing is administered
syndrome. As a result, pregnancy may be associ- twice daily and cleared by the kidneys. Dose
ated with progressive cyanosis and/or arrhythmias adjustment in response to peak anti-Xa levels is
in women at risk.34 Ebstein anomaly is also asso- needed due to changes in renal clearance and
ciated with increased risk of preterm delivery.35 volume of distribution over the course of preg-
Secondary TR can occur as a result of RV pressure nancy.40 In contemporary studies, dose-
or volume overload as a result of left-sided heart adjusted LMWH is still associated with thrombo-
disease and pulmonary hypertension, cardiac embolic complication in 4% to 17% of
conditions associated with significantly elevated pregnancies.39,41,42
maternal risk during pregnancy. Thromboembolic complications occur
throughout pregnancy and may be related to
PROSTHETIC VALVES sub-therapeutic anticoagulation during transition
of anticoagulants, especially in the first
Pregnancy is a prothrombotic state and is associ-
trimester, or sub-therapeutic LMWH levels.
ated with an increased risk of valve thrombosis in
Fixed dose LMWH is associated with signifi-
women with prosthetic heart valves. Pregnant
cantly higher thromboembolic complications
women with mechanical heart valves require care-
compared with dose-adjusted regimens.43 The
ful anticoagulation management to prevent severe
measurement of peak anti-Xa levels may not
maternal morbidity while minimizing
sufficiently assure adequate anticoagulation.
anticoagulation-related risk to the fetus. Although
Among pregnant women with peak anti-Xa
hypercoagulability risk increases throughout preg-
levels within the recommended range of 0.8 to
nancy and peaks in the immediate postpartum
1.2 U/mL, 57% had sub-therapeutic trough
period, valve thrombosis frequently occurs in the
levels (158 Lewey et al
Comparing Anticoagulation Strategies pregnancy offers the lowest risk of maternal
thromboembolic complications but carries a
Four anticoagulation strategies were compared in
higher risk of miscarriage and embryopathy, as
a meta-analysis of contemporary studies repre-
described previously. The 2014 ACC/AHA Valvular
senting 800 pregnancies between 1974 and
Heart Disease Guidelines and the 2018 ESC Preg-
2014.42 Studies were excluded if fixed dose
nancy and Heart Disease Guidelines recommend
LMWH or unfractionated heparin (UFH) were
continuing warfarin at doses 5 mg/d during the
used or if ball-in-cage valves were present in
first trimester and transitioning to dose-adjusted
greater than 10% of reported pregnancies.
LMWH or intravenous (IV) UFH when the daily
Maternal risk was lowest in women using vitamin
dose is >5 mg/d, as summarized in Table 3.6,45
K antagonist (VKA) throughout pregnancy and 3-
Regardless of anticoagulant choice in the first
times-higher in women using alternative strate-
trimester, treatment with warfarin is usually recom-
gies, see Table 2. Maternal deaths were rare and
mended in the 2nd and 3rd trimesters. Discontinu-
adverse events were driven by systemic thrombo-
ation of warfarin and starting IV UFH before
embolism or valve thrombosis. Fetal risk was
planned vaginal delivery is recommended. Women
lowest in women using LMWH throughout preg-
who are therapeutically anticoagulated on warfarin
nancy or LMWH plus VKA. Differences in fetal out-
and need to be delivered should undergo Cesar-
comes were driven by spontaneous abortions;
ean delivery to minimize traumatic fetal
congenital defects were uncommon. Women tak-
hemorrhagic.
ing low-dose VKA throughout pregnancy had
The AHA/ACC guidelines recommend targeting
similar fetal outcomes compared with women tak-
a peak anti-Xa level of 0.8 to 1.2 U/mL 4 to 6 hours
ing LMWH or LMWH plus VKA. A similar meta-
after dosing for women treated with LMWH during
analysis (see Table 2) demonstrated that women
pregnancy. Given the higher risk of thromboem-
treated with VKA throughout pregnancy had the
bolic complications in women with sub-
lowest proportion of livebirths compared with
therapeutic anticoagulation, aiming for peak levels
women treated with LMWH (64.5% vs 92%) but
in the 1.0 to 1.2 U/mL range with trough levels
had a lower risk of thromboembolic complications
greater than 0.6 U/mL may be reasonable, and is
(2.7% vs 8.7).39
recommended in the 2018 ESC pregnancy and
heart disease guidelines (see Table 3).6 Because
Management
the safety profile of low-dose warfarin is based
Women with bioprosthetic and mechanical valves on a small number of studies and the risk of fetal
should be treated with a baby aspirin during the loss is present throughout pregnancy, even at
second and third trimesters. For women with me- lower warfarin doses, some investigators advo-
chanical valves, warfarin continued throughout cate for using LMWH throughout pregnancy with
Table 2
Comparison of maternal and fetal risk with different anticoagulation strategies among women with
mechanical valves
Steinberg et al42 D’Souza et al39
Maternal Fetal Maternal TE Livebirths,
Anticoagulation Strategy risk,a % risk,b % event,c % %
VKA only 5 39 2.7 64.5
Low-dose VKA only 5 15 83.6
LMWH 1 VKA 16 16 8.3 89.5
UFH 1 VKA 16 34 6.1 72.4
LMWH only 15 14 8.7 92.0
Abbreviations: LMWH, low molecular weight heparin; TE, thromboembolic; UFH, unfractionated heparin; VKA, vitamin K
antagonist.
a
Maternal death, systemic TE, or valve failure resulting in heart failure, arrhythmia, or surgery.
b
Spontaneous abortion, fetal death, or congenital defect.
c
Valve thrombus or extravalvular TE event.
Data from D’Souza R, Ostro J, Shah PS, Silversides CK, Malinowski A, Murphy KE, Sermer M, Shehata N. Anticoagulation
for pregnant women with mechanical heart valves: a systematic review and meta-analysis. Eur Heart J. 2017;38:1509–1516
and Steinberg ZL, Dominguez-Islas CP, Otto CM, Stout KK, Krieger EV. Maternal and Fetal Outcomes of Anticoagulation in
Pregnant Women With Mechanical Heart Valves. J Am Coll Cardiol. 2017;69:2681–2691.
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.Valvular Heart Disease in Pregnancy 159
Table 3
Recommendations regarding anticoagulation strategy for mechanical valves during pregnancy
1st Trimester 2nd and 3rd Trimesters Peripartum
45
AHA/ACC guidelines
Warfarin dose 5 mg Warfarin (IIa) or Warfarin (I) IV UFH (I)
LMWH (IIb) or
IV UFH (IIb)
Warfarin dose >5 mg LMWH (IIa) or Warfarin (I) IV UFH (I)
IV UFH (IIa)
Aspirin is routinely recommended starting in 2nd trimester
Target anti-Xa peak level: 0.8–1.2 U/ml 4–6 h post-dose (I)
ESC guidelines6
Warfarin dose 5 mg Warfarin (IIa) or Warfarin (I) IV UFH (I)
LMWH (IIb) or
IV UFH (IIb)
Warfarin dose >5 mg Warfarin (IIb) or Warfarin (IIa) or IV UFH (I)
LMWH (IIa) or LMWH (IIb)
IV UFH (IIa)
Aspirin is not routinely recommended
Target anti-Xa peak level: 1.0–1.2 U/mL (mitral and right-sided valves) or 0.8–1.2 U/mL (aortic valves)
4–6 h post-dose (I). Target anti-Xa trough level: >0.6 U/mL (IIb)
Both LMWH and IV UFH refer to dose-adjusted rather than fixed dosing.
Abbreviations: AHA/ACC, American Heart Association/American College of Cardiology; IV UFH, intravenous unfractio-
nated heparin; LMWH, low molecular weight heparin.
Data from Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, et al. 2018 ESC Guidelines for the management of car-
diovascular diseases during pregnancy. Eur Heart J. 2018;39:3165–3241 and Nishimura RA, Otto CM, Bonow RO, et al. 2014
AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:e57–e185.
closely monitored anti-Xa levels.46 Favorable clin- bioprosthetic valves. Younger age at bio-
ical outcomes have been demonstrated in women prosthetic valve implantation is associated
treated with this strategy, but high levels of medi- with accelerated valve degeneration, which
cation adherence and patient engagement are further shortens durability in women of repro-
needed. This strategy may be desirable for women ductive age.48 Preconception counseling
who are at otherwise low risk of thromboembolic regarding valve choice and implications for
complications (eg, mechanical valve in aortic posi- maternal and fetal risk in future pregnancies,
tion) or women who place higher value on avoiding especially for mechanical valves, is critically
potential fetal risk than maternal complications. important and should be performed by a cardi-
Valve thrombosis during pregnancy should be ologist familiar with treating pregnant patients
confirmed with transesophageal echocardiogram with heart disease.
and treated first with heparin and, if needed,
thrombolytic therapy for women with small
thrombus and mild symptoms. Tissue-type plas- SUMMARY
minogen activator is associated with hemorrhagic Pregnancy in the setting of mild to moderate
complications but has been successfully used in valvular heart disease is often well tolerated. Pa-
pregnant women.47 tients with severe mitral or severe symptomatic
Women presenting with large thrombus burden AS are at increased risk of severe maternal
and more severe symptoms may require emergent morbidity and mortality and pregnancy may be
surgery, which is associated with adverse prohibitively high risk unless valve intervention is
maternal and fetal outcomes. performed. Care by a multidisciplinary Pregnancy
Heart Team consisting of MFM specialists and
Choosing Prosthetic Valve Type Before
cardiologists can improve preconception coun-
Pregnancy
seling and coordinated pregnancy and post-
Mechanical heart valves offer superior hemody- partum care to minimize maternal and fetal
namic profile and durability compared with complications.
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.160 Lewey et al
CLINICS CARE POINTS 9. Kamel H, Navi BB, Sriram N, et al. Risk of a throm-
botic event after the 6-week postpartum period.
Women with severe mitral stenosis and symp- N Engl J Med 2014;370:1307–15.
tomatic severe aortic stenosis are at high risk 10. Mehta LS, Warnes CA, Bradley E, et al. American
of poor outcomes and should be evaluated for Heart Association Council on Clinical Cardiology;
valvular intervention before conception. Council on Arteriosclerosis, Thrombosis and
Mitral and aortic regurgitation are well toler- Vascular Biology; Council on Cardiovascular and
ated during pregnancy. Stroke Nursing; and Stroke Council. Cardiovascular
For women with mechanical valves, warfarin Considerations in caring for pregnant patients: A
offers the lowest risk of maternal thromboem- Scientific Statement from the American Heart Asso-
bolic complications, whereas low molecular ciation. Circulation 2020;141:e884–903.
weight heparin offers the lowest fetal risk. 11. de Souza JA, Martinez EE, Ambrose JA, et al. Percu-
Cardiac indications for Cesarean delivery taneous balloon mitral valvuloplasty in comparison
include symptomatic heart failure and pulmo- with open mitral valve commissurotomy for mitral
nary hypertension. stenosis during pregnancy. J Am Coll Cardiol
2001;37:900–3.
ACKNOWLEDGMENTS 12. John AS, Gurley F, Schaff HV, et al. Cardiopulmonary
bypass during pregnancy. Ann Thorac Surg 2011;
This study was supported by grants K12
91:1191–6.
HD085848 (Lewey) and R56 HL136730 (Levine)
13. Canobbio Mary M, Warnes Carole A, Aboulhosn J,
from the National Institutes of Health.
et al. Management of pregnancy in patients with
complex congenital heart disease: a scientific
DISCLOSURE statement for healthcare professionals from the
The authors have nothing to disclose. American Heart Association. Circulation 2017;135:
e50–87.
REFERENCES 14. Silversides CK, Grewal J, Mason J, et al. Preg-
nancy outcomes in women with heart disease:
1. ACOG practice bulletin No. 212: pregnancy and the CARPREG II study. J Am Coll Cardiol 2018;
heart disease. Obstet Gynecol 2019;133:e320–56. 71:2419–30.
2. Petersen EE, Davis NL, Goodman D, et al. Vital 15. Drenthen W, Boersma E, Balci A, et al. Predictors
Signs: pregnancy-related deaths, United States, of pregnancy complications in women with
2011-2015, and strategies for prevention, 13 states, congenital heart disease. Eur Heart J 2010;31:
2013-2017. MMWR Morb Mortal Wkly Rep 2019;68: 2124–32.
423–9. 16. Roos-Hesselink JW, Cornette J, Sliwa K, et al.
3. Roos-Hesselink J, Baris L, Johnson M, et al. Preg- Contraception and cardiovascular disease. Eur
nancy outcomes in women with cardiovascular dis- Heart J 2015;36:1728–34.
ease: evolving trends over 10 years in the ESC 17. van Hagen IM, Thorne SA, Taha N, et al, ROPAC In-
Registry of Pregnancy and Cardiac disease (RO- vestigators and EORP Team. Pregnancy outcomes
PAC). Eur Heart J 2019;40:3848–55. in women with rheumatic mitral valve disease: re-
4. Siu SC, Sermer M, Colman JM, et al, Investigators sults from the Registry of pregnancy and cardiac
on behalf of the CD in P (CARPREG). Prospective disease. Circulation 2018;137:806–16.
multicenter study of pregnancy outcomes in women 18. Silversides CK, Colman JM, Sermer M, et al. Cardiac
with heart disease. Circulation 2001. Available at: risk in pregnant women with rheumatic mitral steno-
https://www.ahajournals.org/doi/abs/10.1161/ sis. Am J Cardiol 2003;91:1382–5.
hc3001.093437. 19. Hameed A, Karaalp IS, Tummala PP, et al. The effect
5. Nanna M, Stergiopoulos K. Pregnancy complicated of valvular heart disease on maternal and fetal
by valvular heart disease: an update. J Am Heart outcome of pregnancy. J Am Coll Cardiol 2001;37:
Assoc 2014;3:e000712. 893–9.
6. Regitz-Zagrosek V, Roos-Hesselink JW, 20. Lesniak-Sobelga A, Tracz W, KostKiewicz M, et al.
Bauersachs J, et al. 2018 ESC Guidelines for the Clinical and echocardiographic assessment of
management of cardiovascular diseases during pregnant women with valvular heart diseases–
pregnancy. Eur Heart J 2018;39:3165–241. maternal and fetal outcome. Int J Cardiol 2004;94:
7. Sanghavi M, Rutherford JD. Cardiovascular physi- 15–23.
ology of pregnancy. Circulation 2014;130:1003–8. 21. al Kasab SM, Sabag T, al Zaibag M, et al. Beta-
8. Robson SC, Hunter S, Boys RJ, et al. Serial study of adrenergic receptor blockade in the management
factors influencing changes in cardiac output during of pregnant women with mitral stenosis. Am J Obstet
human pregnancy. Am J Physiol 1989;256:H1060–5. Gynecol 1990;163:37–40.
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.Valvular Heart Disease in Pregnancy 161
22. Joshi HS, Deshmukh JK, Prajapati JS, et al. Study of Research Programme (EORP) Team*. Pregnancy in
effectiveness and safety of percutaneous balloon women with a mechanical heart valve: data of the
mitral valvulotomy for treatment of pregnant patients European Society of Cardiology Registry of Preg-
with severe mitral stenosis. J Clin Diagn Res 2015;9: nancy and Cardiac Disease (ROPAC). Circulation
OC14–7. 2015;132:132–42.
23. Elkayam U, Goland S, Pieper PG, et al. High-risk 37. Alshawabkeh L, Economy KE, Valente AM. Anticoa-
cardiac disease in pregnancy. J Am Coll Cardiol gulation during pregnancy. J Am Coll Cardiol 2016;
2016;68:396–410. 68:1804–13.
24. Elkayam U, Bitar F. Valvular heart disease and preg- 38. Vitale N, De Feo M, De Santo LS, et al. Dose-depen-
nancy: Part I: native valves. J Am Coll Cardiol 2005; dent fetal complications of warfarin in pregnant
46:223–30. women with mechanical heart valves. J Am Coll Car-
25. Silversides CK, Colman JM, Sermer M, et al. Early diol 1999;33:1637–41.
and intermediate-term outcomes of pregnancy with 39. D’Souza R, Ostro J, Shah PS, et al. Anticoagulation
congenital aortic stenosis. Am J Cardiol 2003;91: for pregnant women with mechanical heart valves:
1386–9. a systematic review and meta-analysis. Eur Heart J
26. Yap S-C, Drenthen W, Pieper PG, et al, ZAHARA In- 2017;38:1509–16.
vestigators. Risk of complications during pregnancy 40. Quinn J, Von Klemperer K, Brooks R, et al. Use of
in women with congenital aortic stenosis. Int J Car- high intensity adjusted dose low molecular weight
diol 2008;126:240–6. heparin in women with mechanical heart valves dur-
27. Orwat S, Diller G-P, van Hagen IM, et al. Risk of ing pregnancy: a single-center experience. Haema-
pregnancy in moderate and severe aortic stenosis. tologica 2009;94:1608–12.
J Am Coll Cardiol 2016;68:1727–37. 41. Bhagra CJ, D’Souza R, Silversides CK. Valvular
28. Hodson R, Kirker E, Swanson J, et al. Transcatheter heart disease and pregnancy part II: manage-
aortic valve replacement during pregnancy. Circ ment of prosthetic valves. Heart 2017;103:
Cardiovasc Interv 2016;9:e004006. 244–52.
29. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ 42. Steinberg ZL, Dominguez-Islas CP, Otto CM, et al.
ACC Guideline for the Management of Patients With Maternal and fetal outcomes of anticoagulation in
Valvular Heart Disease: A Report of the American pregnant women with mechanical heart valves.
College of Cardiology/American Heart Association J Am Coll Cardiol 2017;69:2681–91.
Task Force on Practice Guidelines. J Am Coll Cardiol 43. Oran B, Lee-Parritz A, Ansell J. Low molecular
2014;63:e57–e185. weight heparin for the prophylaxis of thromboembo-
30. Drenthen W, Pieper PG, Roos-Hesselink JW, et al, lism in women with prosthetic mechanical heart
ZAHARA Investigators. Non-cardiac complications valves during pregnancy. Thromb Haemost 2004;
during pregnancy in women with isolated congenital 92:747–51.
pulmonary valvar stenosis. Heart 2006;92:1838–43. 44. Goland S, Schwartzenberg S, Fan J, et al. Moni-
31. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 toring of anti-Xa in pregnant patients with
AHA/ACC guideline for the management of adults mechanical prosthetic valves receiving low-
with congenital heart disease: a Report of the Amer- molecular-weight heparin: peak or trough levels?
ican College of Cardiology/American Heart Associa- J Cardiovasc Pharmacol Ther 2014;19:451–6.
tion Task Force on clinical Practice guidelines. 45. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/
Circulation 2019;139:e698–800. ACC guideline for the management of patients with
32. Greutmann M, Von Klemperer K, Brooks R, et al. valvular heart disease: a Report of the American
Pregnancy outcome in women with congenital heart College of Cardiology/American Heart Association
disease and residual haemodynamic lesions of the Task Force on Practice guidelines. J Am Coll Cardiol
right ventricular outflow tract. Eur Heart J 2010;31: 2014;63:e57–185.
1764–70. 46. Elkayam U. Anticoagulation therapy for pregnant
33. Khairy P, Ouyang DW, Fernandes SM, et al. Preg- women with mechanical prosthetic heart valves:
nancy outcomes in women with congenital heart dis- how to improve safety? J Am Coll Cardiol 2017;69:
ease. Circulation 2006;113:517–24. 2692–5.
34. Connolly HM, Warnes CA. Ebstein’s anomaly: 47. Özkan M, Çakal B, Karakoyun S, et al. Thrombolytic
outcome of pregnancy. J Am Coll Cardiol 1994;23: therapy for the treatment of prosthetic heart valve
1194–8. thrombosis in pregnancy with low-dose, slow infu-
35. Lima F, Nie L, Yang J, et al. Postpartum cardiovascu- sion of tissue-type plasminogen activator. Circula-
lar outcomes among women with heart disease from tion 2013;128:532–40.
A Nationwide study. Am J Cardiol 2019;123:2006–14. 48. Pibarot P, Dumesnil JG. Prosthetic heart valves: se-
36. van Hagen IM, Roos-Hesselink JW, Ruys TPE, et al, lection of the optimal prosthesis and long-term man-
ROPAC Investigators and the EURObservational agement. Circulation 2009;119:1034–48.
Descargado para Irene Ramírez (iramirez@binasss.sa.cr) en National Library of Health and Social Security de ClinicalKey.es por Elsevier en enero 08, 2021.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2021. Elsevier Inc. Todos los derechos reservados.You can also read