Intra-Cytoplasmic Sperm Injection (ICSI) - Information For Patients Saint Mary's Hospital
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Saint Mary’s Hospital
Department of Reproductive Medicine
Intra-Cytoplasmic Sperm
Injection (ICSI)
Information For Patients
INS/DRM/CLI/018 V5/01/11/2013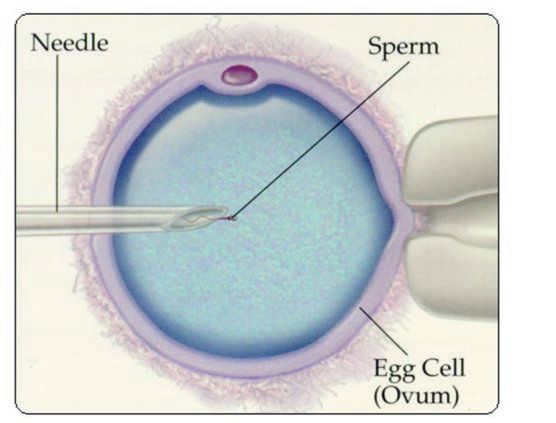
2
Contents Page
What is ICSI and why is it necessary? 4
Which couples require ICSI? 5
How is ICSI carried out? 5
How successful is ICSI? 6
What risks are associated with ICSI treatment? 7
Chromosomal abnormalities 7
What happens if my chromosome test shows a
rearrangement? 8
Birth Defects 8-9
Developmental delays 9
3What is ICSI and why is it necessary?
Intra-cytoplasmic sperm injection (ICSI) refers to the technique
of injecting a single sperm into the centre (cytoplasm) of the
egg. In natural conception a large number of sperm surround
the egg and many attach to the outside, but only one sperm
penetrates and fertilises each egg. In IVF we mimic nature by
adding a large number of sperm to the dish containing the egg.
When fertilisation does not occur, it is usually because the sperm
cannot attach to or penetrate the egg. This can be because of a
fault with either sperm or egg. When abnormal fertilisation
occurs, it is usually because more than one sperm has entered
the egg.
ICSI overcomes problems of failed or abnormal fertilisation by
placing a single sperm directly in the centre of the egg. Any
problems with ICSI arise because this one sperm may not be the
‘right’ one, or because the injection procedure damages the
egg.
ICSI is relatively new and as such should still be regarded as
experimental.
4Which couples require ICSI?
Currently we are using ICSI in couples with reduced semen
counts or where there is reduced sperm motility, in which the
risk of fertilisation failure is increased, and also those who have
previously had very low or no fertilisation in an IVF cycle.
ICSI is likely to be the treatment of choice if the sperm is sub-
optimal.
We also use ICSI in the following situations:
• Reduced fertilisation rate after conventional IVF: less than
40% normal fertilisation with at least 4 mature eggs
collected.
• Failed fertilisation after conventional IVF.
• Use of surgically retrieved sperm.
• Patients who have had ICSI in previous IVF cycles should
continue to have ICSI in future cycles.
How is ICSI carried out?
Except for the method of fertilisation, every other aspect of
your treatment cycle is identical for ICSI and conventional IVF,
including hormonal stimulation, egg recovery, producing the
sperm sample and embryo replacement.
On the day of ICSI, the embryologist carefully removes the outer
(cumulus) cells from each egg, using an enzyme normally
produced by sperm. This enables the embryologist to see inside
the egg using a high powered microscope and assess if the egg
is ‘mature’. All eggs can be inseminated by IVF, but only mature
eggs can be used in ICSI. In most treatment cycles,
approximately 80% of eggs are mature. The sperm are prepared
as normal for IVF. The embryologist then picks out individual
live sperm, of normal appearance and injects one into each egg,
using a special glass needle (see diagram on page 6).
5After ICSI the eggs are returned to the incubator overnight and
checked for fertilisation the following morning, as for
conventional IVF.
How successful is ICSI?
Approximately 6 out of every 10 eggs will fertilise successfully
by ICSI, similar to IVF. The reasons for ICSI fertilisation not being
100% successful include:
• Immature eggs cannot be injected.
• Some eggs may be damaged by the injection procedure.
This appears to be related to the properties of the inner egg
membrane.
• Even when injected directly into the egg, many sperm are not
capable of ‘activating’ the egg.
Following successful fertilisation, embryo development is similar
for ICSI and IVF. Following embryo transfer, pregnancy rates are
similar to IVF. Many clinics report higher success rates for ICSI
compared to IVF, but this is only because the women having ICSI
are more fertile.
6What risks are associated with ICSI treatment?
ICSI offers the opportunity of success for couples who could not
achieve it otherwise. However, it is still a relatively new
technique and was not preceded by long term animal studies, as
is usually required for new medical techniques or drugs.
It is known that abnormal sperm production, as is the case in
men with very low sperm count or absent sperm in the
ejaculate, can be associated with genetic defects in the male.
As ICSI bypasses the normal processes of sperm ‘selection’ and
fertilisation, these genetic defects may be transmitted to the
children.
It is also possible that the egg may be damaged by the injection
procedure. Theoretically, this can result in damage to the
resulting embryo if the damaged egg is fertilised normally.
Although the great majority of babies born by ICSI appear to be
normal, the full implications of treatment will not be known for
many years, and you should be aware of the possible risks of
this procedure as detailed below. For further information please
see our main Patient Information booklet.
Chromosomal abnormalities
Men with very low sperm counts are more likely to have a
rearrangement of their chromosomes – known as a balanced
translocation (approximately 3–5%). This will be discussed with
you in clinic and a blood test can be arranged if this is the case.
Many of these rearrangements involve the chromosomes
responsible for sex determination (XX for women and XY for
men). If there is a rearrangement, this can lead to a
chromosome abnormality in any baby conceived. Many men
with low sperm counts will have a small deletion of their Y
chromosome, that is, a tiny genetic fragment may be missing.
This will not be found in routine chromosome testing. This
deletion may be passed on to a baby boy and may cause him to
have a lowered sperm count when he grows up.
7What happens if my chromosome test shows a
rearrangement?
• If an abnormality is found, the chance of a pregnancy is less.
• The abnormality may increase your chance of miscarriage and
there may be implications for any child conceived.
• The child may be unaffected, it may display the same
abnormality as its father or it may inherit an abnormality,
which will affect the child more than the father.
• If an abnormality is found in your chromosomes this would
be discussed with you in detail by one of our genetics
counsellors.
Birth defects
The evidence on whether or not babies born after IVF or ICSI
treatment have a greater risk of birth defects is not yet
completely clear. More studies are needed in order to gain
further insight into these possible effects.
In 2005, a major European review of children born after ICSI
and IVF (followed up until 5 years of age) found that so-called
major birth defects involving the heart, lungs, musculoskeletal
or gastrointestinal systems, were present in about 2% of
naturally conceived offspring, 4% of children conceived by
routine IVF, and in 6% of children conceived after ICSI. A
substantial proportion of the abnormalities in the ICSI children
were problems in the development of the urinary or genital
organs, especially in boys. However, all of them were
correctable by surgery and they were found to be caused by
genetic factors from the father, rather than a result of the ICSI
procedure itself.
8Minor birth defects were present in about 20% of naturally
conceived offspring, 31% of children conceived by routine IVF,
and in 29% of children conceived after ICSI. Minor anomalies
are those which do not in themselves have serious medical,
functional or cosmetic consequences for the child. More recent
studies reported no difference in the risk for any anomaly or
specific anomalies after different types of IVF technologies
including ICSI.
Developmental delays
Some research papers concerning follow up of small numbers of
ICSI children suggest possible developmental delay in some
children conceived using the ICSI technique. This has not been
found in ongoing follow up studies in the UK and Europe.
Treatment will not be refused based on the results of above
tests or if a couple declines the offer of testing.
If you have any questions you feel need answering we would be
pleased to do this when you next attend clinic.
ICSI is relatively new and as such should still be regarded as
experimental.
9Own notes/questions
10Violence, Aggression and Harassment
Control Policy
We are committed to the well-being and safety of our patients
and of our staff. Please treat other patients and staff with the
courtesy and respect that you expect to receive. Verbal abuse,
harassment and physical violence are unacceptable and will lead
to prosecutions.
Suggestions, Concerns and Complaints
If you would like to provide feedback you can:
• Ask to speak to the ward or department manager.
• Write to us: Patient Advice and Liaison Services, 1st Floor,
Cobbett House, Manchester Royal Infirmary, Oxford Road,
Manchester M13 9WL
• Log onto the NHS Choices website www.nhs.uk - click on
‘Comments’.
If you would like to discuss a concern or make a complaint:
• Ask to speak to the ward or department manager – they may
be able to help straight away.
• Contact our Patient Advice and Liaison Service (PALS) –
Tel: 0161 276 8686 e-mail: pals@cmft.nhs.uk. Ask for our
information leaflet.
We welcome your feedback so we can continue to improve our
services.
11No Smoking Policy
The NHS has a responsibility for the nation’s health.
Protect yourself, patients, visitors and staff by adhering to our
no smoking policy. Smoking is not permitted within any of our
hospital buildings or grounds.
The Manchester Stop Smoking Service can be contacted on
Tel: (0161) 205 5998 (www.stopsmokingmanchester.co.uk).
Translation and Interpretation Service
These translations say "If you require an interpreter, or
translation, please ask a member of our staff to arrange it for
you." The languages translated, in order, are: Arabic, Urdu,
Bengali, Polish, Somali and simplified Chinese.
Follow us on
@CMFTNHS Facebook
www.cmft.nhs.uk
© Copyright to Central Manchester University Hospitals NHS Foundation Trust
TIG 125/13 Produced November 2013 Review Date November 2015 (SF Taylor CM14401)You can also read

















































