Judiciary Reference Guide - NOTE: Pages two and three of this document can be used as a separate handout
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Judiciary Reference Guide
NOTE: Pages two and three of this document can be used as a separate handout
Version 03/2014 1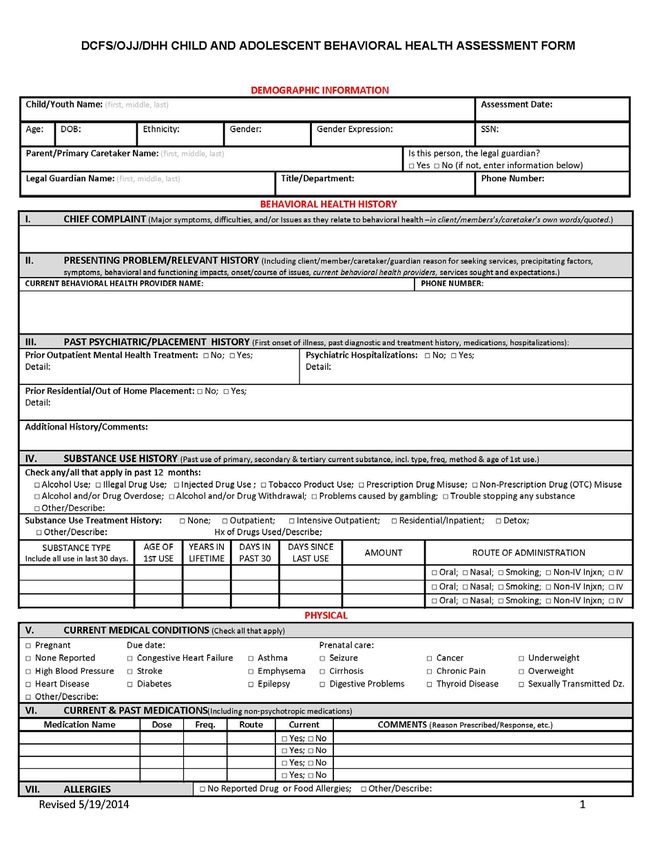
Quick Reference Sheet for
Magellan’s Judiciary Reference Guide
Who We Serve What We Do
• Children receiving Medicaid benefits • Provide a single point of entry available 24/7/365 with two
• Adults receiving Medicaid benefits in-state call centers
• Children in the Coordinated System of Care • Maintain a contracted and credentialed network of some
(CSoC) 1,700 providers at all levels of care
• Children served through the Department of • Coordinate care for members including referral, assistance
Children and Family Services (DCFS) with eligibility, treatment planning, utilization review,
• Children served through the Office of Juvenile follow-up care, assistance with discharge planning and
Justice (OJJ) placement and peer support.
• Uninsured children and adults served through • Provide a free electronic behavioral health record (Clinical
the State’s human services districts and their Advisor) to all eligible providers of the state’s uninsured
network of contracted providers • Provide intensive case management for people with special
• People in the Permanent Supportive Housing health care needs, such as pregnant women with addiction
program in the GoZone area of the State disorders or women with dependent children with co-
• Additionally, Magellan works with the occurring disorders
Department of Education to assist with • Manage dollars spent in the system to focus on community-
Medicaid reimbursement for children served based care
in schools by the school systems • Provide quality review of providers and technical assistance
to improve care
• Monitor quality of care concerns
How do I know if someone is • Investigate complaints of fraud and/or abuse
eligible for services?
• Process and pay claims for services for both adult and
Call 1-800-424-4399 children populations with Medicaid, as well as those
additional services funded through DCFS and OJJ
Subject Matter Experts (SMEs)
Expert Area Phone Email
Vice President of System (225) 367-3012 o
Kathleen Coenson krcoenson@magellanhealth.com
Transformation (225) 241-6798 c
Dr. Richard Dalton Chief Medical Officer (225) 367-3001 o rfdalton@magellanhealth.com
(225) 367-3006 o
Foley Nash Children System Administrator flnash@magellanhealth.com
(225) 241-2970 c
Chris Boling Adult System Administrator (225) 367-3024 o caboling@magellanhealth.com
Janel Dugas Juvenile Justice Liaison (225) 226-5790 c jdugas@magellanhealth.com
Children & Youth Population
There are two populations of children and youth eligible for services:
1. Children and youth with behavioral health needs eligible for services from OJJ, DCFS, DHH and DOE, including those
served by Medicaid (approximately 50,000 children)
2. Children and youth with significant behavioral health challenges or co-occurring mental illness and addictions in, OR
at risk of out-of-home placements, eligible for the CSoC (about 2,400 children)
o Out-of-home is defined as:
Detention, secure care facilities, psychiatric hospitals, residential treatment facilities, developmental disabilities
facilities, addiction facilities, foster care and alternative schools homeless, as identified by DOE
NOTE: New Medicaid definition of a child is birth until age 21, except for a foster child whose Medicaid
eligibility is until age 26.
2
1-800-424-4399 Call 24-hours a day/7-days a week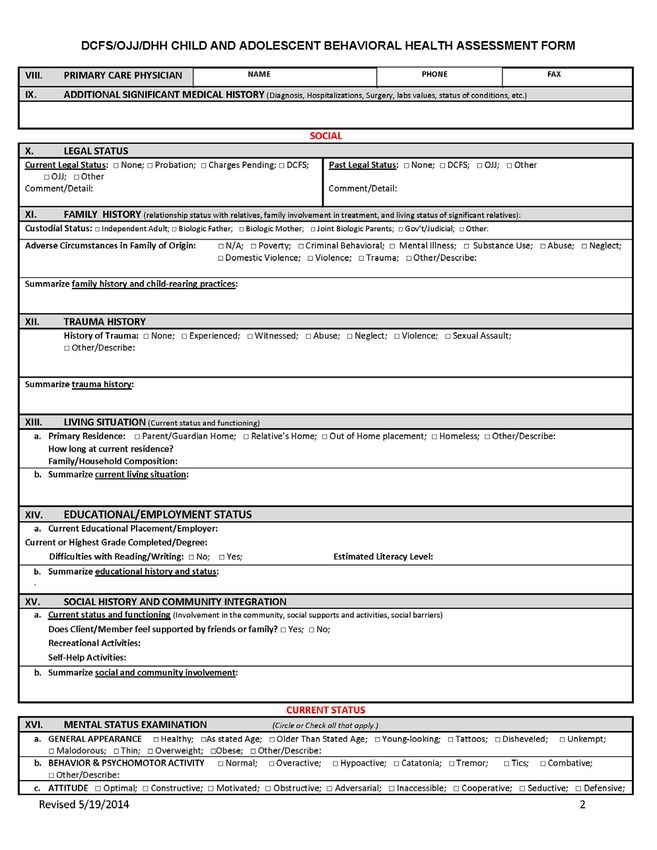
Quick Reference Sheet for
Magellan’s Judiciary Reference Guide
Services Available in the Louisiana Behavioral Health Partnership
Substance
Inpatient Crisis Adult Children CSoC Outpatient
Abuse
Detox IP
General Telephonic Outpatient
ACT /FACT TGH TGH Detox RTC
Hospital Crisis Triage CMHC/ FQHC
Detox OP
Free
Mobile
Standing
Services (Face- PSR PSR PSR SA RTC MHR
Psychiatric
to-Face)
Hospital
LSU
Crisis Individual
Teaching CPST CPST CPST IOP
Residential Family & Group
Hospital
State
CI CI CI CI OP Psychiatrist
Hospital
Licensed &
Emergency
Telepsychiatry Case Conference Case Conference Suboxone medical
Room
psychologist
FQHC NMGH NMGH LCSW
ECT TFC TFC LPC
ICM MST LMFT
Psychotherapy FFT FFT LAC
Psychological
PRTF PRTF APRN
Testing
Independent
Psychotherapy
Living/Skills Building
Psychological Parent/Youth Support
Testing & Training (FSO)
Information about these services is Wrap around
provided in Judicial Reference Facilitation (WAA)
Guide or the Service Authorization Short-term Respite
Manual or call 1-800-424-4399 Crisis Stabilization
Students With IEP About Coordinated System of Care (CSoC)
• The IEP must include behavioral health services • Collaborative approach offered to children and youth who are in
or at greatest risk of out-of-home placement
• The IEP serves as the authorization for select services
• Goal is for them to remain in or return to their home
• School Social Workers, School Psychologists, School • Five specialized services available through CSoC:
Counselors, Licensed Professional Counselors, etc. o Parent Support & Training (Family Support Organization)
provide the related services o Youth Support & Training (Family Support Organization)
o Independent Living/Skills Building
• These professionals are considered “service
o Short-Term Respite Care
providers” for the LEA and are required to enter the
o Crisis Stabilization
related services that they provide in the DOE • For non-CSoC implementing regions or when max enrollment is
electronic tracking system (RSMS) reached, Recovery and Resiliency Care Management (RCM) is
• The school system is able to claim a portion of available for those who meet CSoC eligibility criteria:
Medicaid reimbursement for these authorized o By a LMHP
o Individualized Care Coordination
services
o Can transition into CSoC when available
NOTE: This is the first time schools are able to claim
reimbursement for behavioral health services! NOTE: Family/Youth must agree to participate
3
1-800-424-4399 Call 24-hours a day/7-days a week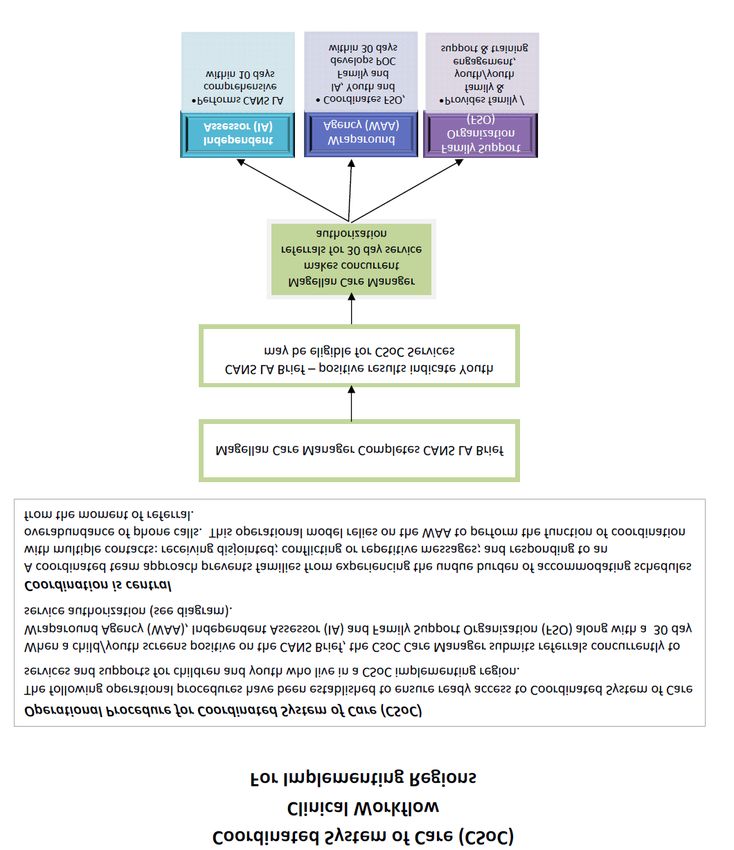
About This Judiciary Reference Guide
This guide is provided as a quick reference tool for those working with court involved member populations.
For comprehensive information regarding Service Authorization Criteria 1 Guidelines refer to the
www.MagellanofLouisiana.com website, at the following link:
http://www.magellanoflouisiana.com/media/84978/2012_louisiana_service_authorization_criteria__mnc_j
une_18_2012_v5.pdf.
For comprehensive information about the available services through the Louisiana Behavioral Health
Partnership go to the following link:
http://new.dhh.louisiana.gov/index.cfm/page/538/n/225
The LBHP Services Definition Manual located at that link contains information on:
• Service definitions
• Provider Qualifications
• Eligibility Criteria
• Limitations/ Exclusions
• Provider types allowed to deliver specific service
Magellan Contact Information
Regular Business Hours: 8 a.m. – 6 p.m. CT
After Hours: 6 p.m. – 8 a.m. CT and weekends for crisis and inpatient pre-certification
For Magellan Members
Toll-free: 1-800-424-4399
TTY: 1-800-424-4416
Fraud & Abuse: 1-800-488-2917
Email: LouisianaInfo@MagellanHealth.com
For Magellan Providers
Email Us at LAProviderQuestions@MagellanHealth.com or Call the Provider Service Line 1-800-424-4396
For Questions Related to Judicial Matters
Janel Dugas, Magellan’s Juvenile Justice Liaison, is available as a subject-matter expert. She can be reached
at 225-226-5790 or jdugas@MagellanHealth.com
See the following Subject-Matter Expert Directory for additional Magellan staff contact information.
1
Louisiana Service authorization criteria do not supersede state or Federal law or regulation concerning scope of
practice for licensed, independent practitioner, e.g., advanced practice nurses.
4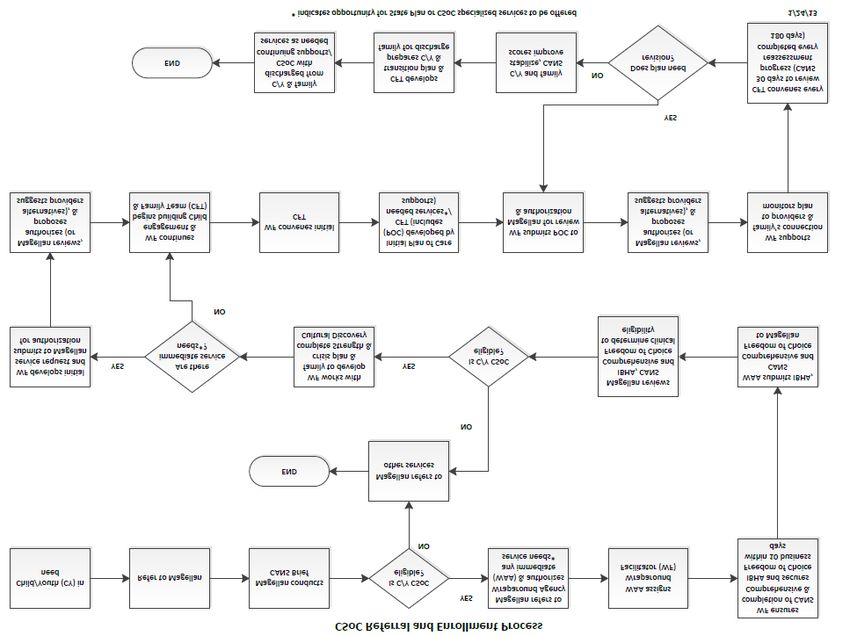
Magellan Subject-Matter Experts (SMEs) Directory
Subject Matter
Position Phone Email Areas of Expertise
Expert (SME)
Vice President of
225-367-3012 o
Kathleen Coenson System krcoenson@magellanhealth.com All areas of system transformation
225-241-6798 c
Transformation
Dr. Richard Dalton Chief Medical Officer 225-367-3001 o rfdalton@magellanhealth.com All clinical areas
Children’s System 225-367-3006 o
Foley Nash flnash@magellanhealth.com All areas of the Children’s System
Administrator 225-241-2970 c
Department of Education, Local
Department of Education Agencies, Charter
Donna Nola-Ganey 225-367-3014 o dnolaganey@magellanhealth.com
Education Liaison Schools, School Based Health
Centers
Office of Juvenile Justice, Families
Juvenile Justice
Janel Dugas 225-226-5790 c jdugas@magellanhealth.com in Need of Services, local Juvenile
Liaison
Probation and Diversion Offices
Department of
225-367-3008 o Department of Children and
Jennifer Jantz Children & Family jnjantz@magellanhealth.com
225-456-7292 c Family Services
Services Liaison
Coordinated System of Care (CSoC)
Donna Herren Sr. Manager, CSoC 225-367-3011 o dherren@magellanhealth.com Reporting and Data Analysis, SME
for 1915 (b3) & (c) HCBS Waivers
Wraparound 225-367-3022 o Coordinated System of Care
Kolletta Lee kdlee@magellanhealth.com
Coordinator, CSoC 225-337-5977 c Regions 1 & 2
Wraparound Coordinated System of Care
Tambria Hunt 318-524-8815 o thunt@magellanhealth.com
Coordinator, CSoC Regions 7,8,9
Wraparound
Katherine Poulin 225-226-3000 o kpoulin@magellanhealth.com Coordinated System of Care
Coordinator, CSoC
Director of Cultural
All areas related to Cultural
Robert Blue Awareness and 225-367-3152 o rgblue@magellanhealth.com
Awareness and Diversity
Diversity
Families, Wraparound Services,
Mary Ann Donovan- Director of Family 225-367-3010 o family involvement with the
mdmason@magellanhealth.com
Mason Involvement 267-716-8147 c Statewide Family Service
Organization
Family Empowerment, Support
Family Involvement and Training across systems with
Danielle Marshall 225-367-3018 o Dmarshall1@magellanhealth.com
Coordinator members, providers and other
venues, state-wide
Youth Empowerment, Support and
Youth Support 225-367-3243 o
Leslie Canady lcanady@magellanhealth.com Training across Children’s systems
Coordinator 225-250-9752 c
and programs
Magellan staff is comprised of Subject Matter Experts (SMEs) with extensive experience and training in their
perspective areas of expertise. In addition to the SMEs, Magellan has a team of licensed clinicians and
professionals identified as Member Service Representatives (MSR) and Care Managers (CM) located in our
Care Management Centers (CMCs) in both Baton Rouge and Shreveport, Louisiana. The table above includes
contact information for our SMEs, along with their areas of expertise.
5Magellan At A Glance
Who We Serve
Magellan manages care for:
• Children receiving Medicaid benefits
• Adults receiving Medicaid benefits
• Children in the Coordinated System of Care (CSoC)
• Children served through the Department of Children and Family Services (DCFS)
• Children served through the Office of Juvenile Justice (OJJ)
• Uninsured children and adults served through the state’s Local Governing Entities (LGEs) and
their network of contracted providers
• People in the Permanent Supportive Housing program in the GoZone area of the State
• Additionally, Magellan works with the Department of Education (DOE) to assist with Medicaid
reimbursement for children served in schools by the school systems.
What We Do
Magellan:
• Provides a single point of entry available 24/7/365 with two in-state call centers
• Maintains a contracted and credentialed network of some 1,700 providers at all levels of care
• Coordinates care for members including referral, assistance with eligibility, treatment planning,
utilization review, follow-up care, assistance with discharge planning, and placement and peer
support
• Provides a free electronic behavioral health record (Clinical Advisor) to all eligible providers of
the State’s uninsured
• Provides intensive case management for people with special health care needs, such as
pregnant women with addiction disorders or women with dependent children with co-occurring
disorders
• Manages dollars spent in the system to focus on community-based care
• Provides quality review of providers and technical assistance to improve care
• Monitors quality of care concerns
• Investigates complaints of fraud and/or abuse
• Processes and pays claims for services for both adult and children populations with Medicaid as
well as those services that state agencies have elected to fund
• Fosters transformation of the system with programs that include:
o Cultural competency standards and training
o Recovery, resiliency and peer support
o MY LIFE (Magellan Youth Leaders Inspiring Future Empowerment)
MY LIFE is made up of youth between the ages of 13 and 23 who have experience with
one or more of the following issues: mental health, substance abuse, juvenile justice, or
foster care. It affords youth leadership opportunities in their communities.
o Support for families
o Liaisons specialized to DCFS, OJJ, and DOE
6Table of Contents
About this Judiciary Reference Guide ....................................................................................................................... 4
Magellan Subject-Matter Experts (SMEs) Directory .......................................................................................... 5
Magellan At A Glance ........................................................................................................................................................... 6
CHAPTER 1: MAGELLAN BEHAVIORAL HEALTH AS STATEWIDE MANAGEMENT ORGANIZATION 9
ABOUT THE STATEWIDE MANAGEMENT ORGANIZATION (SMO) ................................................................................... 9
ELIGIBLE JUDICIAL POPULATIONS............................................................................................................................................ 10
MAGELLAN SERVICE AUTHORIZATION CRITERIA GUIDE................................................................................................... 11
CHAPTER 2: PARTNERSHIPS WITH STATE AGENCIES .....................................................................................12
OFFICE OF JUVENILE JUSTICE (OJJ) AND DEPARTMENT OF CHILDREN AND FAMILY SERVICES (DCFS)
PROTOCOL AND REFERRAL PROCESS ................................................................................................................................... 12
Collaborative Protocol ........................................................................................................................................................ 12
DEPARTMENT OF EDUCATION ......................................................................................................................................................... 13
Collaborative Protocol ........................................................................................................................................................ 13
School Based Behavioral Health Services for Students with Individual Education Plans (IEPs) ..................... 13
CHAPTER 3: THE IMPORTANCE OF MEDICAL NECESSITY IN JUDICIAL DECISION MAKING..........14
DEFINITION OF MEDICAL NECESSITY ...................................................................................................................................... 14
CHAPTER 4: SCREENINGS AND ASSESSMENTS............................................................................................... 16
ASSESSMENT AND SCREENING MATRIX 1 ............................................................................................................................. 16
BEHAVIORAL HEALTH NEEDS ASSESSMENTS ......................................................................................................................... 17
BEHAVIORAL HEALTH ASSESSMENT TEMPLATE ...................................................................................................... 19
PSYCHOLOGICAL TESTING ........................................................................................................................................................ 23
Criteria for Authorization ............................................................................................................................................................ 23
CHAPTER 5: LEVELS OF CARE................................................................................................................................ 24
Crisis Planning and Intervention.................................................................................................................................... 24
Outpatient Services ................................................................................................................................................................ 24
Out-of-Home Placement ................................................................................................................................................... 28
Adverse Incidents and Events........................................................................................................................................ 30
CHAPTER 6: COORDINATED SYSTEM OF CARE (CSOC) ............................................................................31
WHAT IS LOUISIANA'S COORDINATED SYSTEM OF CARE? .............................................................................................. 31
ELIGIBILITY FOR THE COORDINATED SYSTEM OF CARE (CSOC) ................................................................................... 32
WHO MIGHT THE COORDINATED SYSTEM OF CARE (CSOC) BE RIGHT FOR? .............................................................................. 33
WHAT IS THE WRAPAROUND PROCESS? ........................................................................................................................................ 34
SPECIALIZED SERVICES AVAILABLE THROUGH THE COORDINATED SYSTEM OF CARE ............................................. 35
What is Resiliency Care Management? ................................................................................................................ 36
CSoC Referral and Enrollment Process Diagram................................................................................................................ 37
CHAPTER 7: MAGELLAN JUDICIAL INVOLVEMENT MATRIX......................................................................39
7CHAPTER 8: MAGELLAN PROVIDER INFORMATION ....................................................................................40
MAGELLAN CONTACT INFORMATION............................................................................................................... 41
NOTE: A “Quick Reference Sheet for Magellan’s Judiciary Reference Guide” is provided at the beginning of this
document as pages 2-3 and can be used as an overview handout.
8Chapter 1: Magellan Behavioral Health as Statewide Management
Organization
About The Statewide Management Organization (SMO)
The Louisiana Behavioral Health Partnership managed by the Louisiana Department of Health and Hospitals
Office of Behavioral Health (DHH-OBH) oversees Magellan Health Services as the Behavioral Health
Statewide Management Organization (SMO). Magellan manages behavioral health services for Medicaid
and some Non-Medicaid eligible populations served by the Office of Behavioral Health (OBH), Department
of Children and Family Services (DCFS), the Department of Education (DOE), and Office of Juvenile Justice
(OJJ), including services for individuals with co-occurring mental health and addictive conditions.
Magellan helps to improve access, quality, and efficiency of behavioral health services for children,
regardless of eligibility for the Coordinated System of Care (CSoC), and adults with Serious Mental Illness
(SMI) and Addictive Disorders. Magellan also works to develop a qualified provider network to offer a full
array of services to meet the needs of people with behavioral health challenges.
Magellan Health Services, selected via the State of Louisiana Request for Proposals (RFP) process, is a
qualified behavioral health managed care organization with experience and demonstrated success in
providing managed behavioral health care services with complex, publicly-funded behavioral health
programs, and operates a pre-paid inpatient health plan (PIHP), as defined in 42 CFR 438.2, for behavioral
health services provided to children, youth, and adults.
Magellan assists the State of Louisiana in achieving their behavioral health system reform goals, which are
to:
1. Foster individual, youth, and family-driven behavioral health services.
2. Increase access to a fuller array of evidence-based, home- and community-based services that
promote hope, recovery, and resilience.
3. Improve quality by establishing and measuring outcomes.
4. Manage costs through effective utilization of state, federal, and local resources.
5. Foster reliance on natural supports that sustain individuals and families in homes and
communities.
Magellan’s duties include:
1. Manage care for eligible children/youth in need of mental health and addictive disorder
services, including children eligible for the CSoC, on a non-risk basis, utilizing Medicaid, DCFS,
DHH-OBH, DOE, and OJJ State General Funds and federal block grant financing in an effort to
maximize resources.
2. Manage behavioral health services for Medicaid adults with addictive disorders and adults with
functional behavioral health needs, including: persons with Serious Mental Illness and adults
who have previously met the above criteria and need subsequent medically necessary services
for stabilization and maintenance.
3. Manage mental health and addictive disorder services for adults funded through State General
Fund, Mental Health and the Substance Abuse Prevention and Treatment (SAPT) Block Grant.
9Eligible Judicial Populations
Populations who may be involved with the Judicial System and may be eligible for services include children
with complex needs such as:
• Insured by Medicaid
• Involved with multiple agencies (i.e., DHH-OBH, DCFS, OJJ)
• Diagnosed with a chronic mental health, emotional or behavior condition likely to require services
for a year or more
• Currently or recently served by one or more child serving agencies (i.e., Child Welfare, Juvenile
Justice, mental health or special education)
• Homeless as identified by the Department of Education
o The Stewart B. McKinney - Vento Homeless Assistance Act defines a homeless person as: An
individual who (1) lacks a fixed, regular, and adequate nighttime residence and (2) has a
primary nighttime residence that is (a) a supervised, publicly or privately operated shelter
designed to provide temporary living accommodations (including welfare hotels, congregate
shelters, and transitional housing for the mentally ill), (b) an institution that provides a
temporary residence for individuals intended to be institutionalized, or (c) a public or private
place not designed for or ordinarily used as a regular sleeping accommodation for human
beings (McKinney Act (P.L. 100-77, sec 103(2)(1), 101 sat. 485 (1987)).
o For eligibility purposes for assistance and education programs for homeless students, the
Louisiana Department of Education expands the Federal and U.S. Department of Education
definitions of a homeless person to include:
Children and Youth in Transitional or Emergency Shelters
Children and Youth Living in Trailer Parks, Camping Grounds, Vehicles
Children and Youth "Doubled-Up" in Housing
Children and youth living in motels and weekly-rates apartments
Foster Children and Youth
Incarcerated Children and Youth
Migratory Children and Youth
Unaccompanied Minors: Runaway and Abandoned Youth
Highly-mobile Families and Youth
• At imminent risk of out-of-home placement in a:
o Residential Treatment Center
o Local juvenile detention facility
o Secure care juvenile facility
o Psychiatric Inpatient Facility
o Developmental Disability Facility
o Alternative School
o Foster Care
10Magellan Service Authorization Criteria Guide
The Magellan Service Authorization Criteria Guide is for both providers and reviewers to identify the most
appropriate level of care for a member. While these criteria will assign the most effective and least
restrictive level of care in nearly all instances, an infrequent number of cases may fall beyond their
definitions and scope of the Guide. Thorough and careful review of each case, including consultation with
supervising clinicians, will identify these exceptions. Clinical judgment consistent with the standards of good
medical practice will be used in making service authorization determination in such instances.
Service authorization decisions about each member are based on the clinical information provided by the
treating practitioner or facility, the application of the service authorization criteria and available treatment
resources. Magellan recognizes that a full array of services is not available everywhere. When a clinically
necessary level of care does not exist or is not available, Magellan will make every attempt to connect the
member to an appropriate alternative level of care or service.
The comprehensive service authorization guide can be located at the www.MagellanofLouisiana.com
website, or at the following link:
http://www.magellanoflouisiana.com/media/84978/2012_louisiana_service_authorization_criteria__mn
c_jne_18_2012_v5.pdf.
11Chapter 2: Partnerships with State Agencies
Office of Juvenile Justice (OJJ) and Department of Children and Family
Services (DCFS) Protocol and Referral Process
Collaborative Protocol
Magellan, the Office of Juvenile Justice, and the Department of Children and Family Services have
established collaborative protocols that govern the ways in which they will conduct business that falls under
the Louisiana Behavioral Health Partnership. Referral, screening, eligibility, treatment planning, and
processes are important to providing seamless transitions throughout the coordinated systems of care and
are defined in the collaborative protocols.
A child/youth may be referred to Magellan by a family member, school, state agency, or other appropriate
person. When agency or department representatives make a referral through Magellan Member Services,
Magellan will conduct a screening to determine eligibility and obtain information from the legal guardian.
OJJ – Specific Referral Processes
If OJJ requests an expedited eligibility decision for a youth in Pre-Disposition Investigation (PDI), Magellan
will make every possible effort to complete the eligibility screening and communicate the decision regarding
CSoC or LBHP eligibility via telephone or fax. If OJJ needs expedited processing, OJJ will provide the
information to the Magellan Juvenile Justice Liaison, who will communicate the request to the Magellan
Care Management team.
Magellan will screen all referrals to determine if they fall into one of the Special Health Care Needs
categories, which are:
• Any individual with IV drug use, pregnant women with substance use disorders, substance-using
women with dependent children or co-occurring disorders;
• Children with behavioral health needs in contact with other child-serving systems, not eligible for
CSoC; and
• Children eligible for CSoC.
If a child is determined to be a child with behavioral health needs in contact with other child-serving
systems, or is eligible for LBHP services, and is not eligible for CSoC, Magellan makes a referral to or provides
information for an appropriate Magellan provider to develop a treatment plan and may also refer to
Magellan/Resiliency Case Management (RCM) for intensive case management if needed. Magellan will
authorize services in the Treatment Plan/Plan of Care based on eligibility validation and medical necessity,
using established service authorization criteria approved by the Office of Behavioral Health (OBH).
OJJ has the ability to make emergency residential placements for youth who are in need of such placement
in a Nonmedical Group Home level as long as bed capacity is not violated, and after lower level of placement
resources have been exhausted.
12DCFS – Specific Referral Process
For a non-Medicaid eligible child, Magellan will initiate the process of authorizing services only upon DCFS
entering a referral into Clinical Advisor. If Magellan has a referral from DCFS for services for a non-Medicaid
eligible child and the child later requires a higher level of care, Magellan will not authorize the higher level of
care until agreement has been obtained from DCFS for payment for those higher level of care services (to be
secured by telephone contact, and DCFS will make the needed changes in Clinical Advisor).
DCFS has the ability to make emergency residential placements for youth who are in need of such
placement in a Non-medical Group Home level as long as bed capacity is not violated, and after lower level
of placement resources have been exhausted.
Department of Education
Collaborative Protocol
Magellan and DOE work in collaboration to ensure that the Local Educational Agencies (LEAs) have the
knowledge and skills to appropriately refer children to CSoC and to partner with the Wraparound Agency
and the Statewide Family Support Organization. Magellan and DOE operate under a Data Sharing
Agreement that allows Magellan to access important data elements for those students identified under the
Individuals with Disabilities Act and receiving behavioral health services. By receiving this information,
Magellan is able to better coordinate the behavioral health services.
School Based Behavioral Health Services for Students with Individual Education Plans (IEPs)
Local Education Agencies are able to claim a portion of Medicaid reimbursement for behavioral health
services provided to students in accordance with a student’s IEP.
In order for the Local Education Agency to claim Medicaid reimbursement, the student must be Medicaid
eligible and the IEP must include behavioral health services.
• The IEP serves as the authorization for select services
• School Social Workers, School Psychologists, School Counselors, Licensed Professional
Counselors, etc. provide the related services
• These professionals are considered “service providers” for the LEA and are required to enter the
related services that they provide in the DOE electronic tracking system (RSMS)
• Three (3) categories of billable services in schools
1. Addiction Services
2. Community Psychiatric Support and Treatment
3. Other Licensed Practitioner Outpatient Therapy
More and more Local Education Agencies are partnering with Federally Qualified Health Centers, School
Based Health Centers, and private behavioral health providers to provide behavioral health services to
regular education students in the schools.
13Chapter 3: The Importance of Medical Necessity in Judicial Decision
Making
Definition of Medical Necessity
Medically necessary services are defined as those health care services that are in accordance with generally
accepted evidence-based medical standards, or that are considered by most physicians (or other
independent licensed practitioners) within the community of their respective professional organizations, to
be the standard of care.
A. In order to be considered medically necessary, services must be:
a. Deemed reasonably necessary to diagnose, correct, cure, alleviate or prevent the worsening
of a condition or conditions that endanger life, cause suffering or pain or have resulted or
will result in a handicap, physical deformity or malfunction.
b. Those for which no equally effective, more conservative and less costly course of treatment
is available or suitable for the member.
B. Any such services must be individualized, specific and consistent with symptoms or confirmed
diagnosis of the illness or injury being treated and neither more nor less than what the member
requires at that specific point in time.
C. Although a service may be deemed medically necessary, it does not mean the service will be
covered by the Medicaid program. Services that are experimental, non-FDA approved,
investigational or cosmetic are specifically excluded from Medicaid coverage.
Using Medical Necessity to Determine the Appropriate Level of Care
The Medicaid Director, in consultation with the Medicaid Medical Director, may consider authorizing
services at their discretion on a case-by-case basis. Medical necessity, along with criteria sets is used by
providers or reviewers to determine a clinically necessary level of care.
Medical necessity for admission into inpatient and residential levels of care require that the (1) severity of
need criteria, (2) intensity and quality of service criteria, and (3) continued stay criteria for particular levels
of care be met.
These Medical Necessity Guidelines were developed specifically for the Louisiana Behavioral Health
Partnership and are based on:
• Louisiana Medicaid definition of “medically necessary services”
• Louisiana Register and Administrative Code regarding inpatient services
• Service Definition Manual for all other levels of care and services
• Magellan Service Authorization Criteria
14Medical Necessity in Judicial Decision Making
Magellan follows medical necessity guidelines in accordance with generally accepted evidence based
standards. Service authorization decisions about each member who are eligible for services under the LBHP
and managed by Magellan are based on:
• the clinical information provided by the treating practitioner or facility
• the application of the service authorization criteria
• the availability of treatment resources.
Should judiciary deem someone in need of services that are outside of the scope of medical necessity
guidelines or outside of populations under the LBHP who are managed by Magellan, Magellan could assist
judiciary in locating services for that population although funding those services may not be within the
scope of management by the Statewide Management Organization. Magellan could assist with connecting
to services through the local Office of Behavioral Health (OBH) clinics or Federally Qualified Health Centers
(FQHCs). Magellan could also assist with connecting to providers who are able to conduct independent
assessments to identify if an adult might qualify for Medicaid services under the 1915(I) waiver, newly
expanded to cover types of severe mental illness.
15Chapter 4: Screenings and Assessments
Magellan is committed to the philosophy of providing treatment at the most appropriate and least
restrictive level of care necessary for the treatment to effectively and efficiently meet the member’s
bio-psychosocial needs. Magellan sees the entire service array as a fluid treatment pathway, where
members may enter treatment at any level and transition to more or less intensive levels of care as their
changing clinical needs dictate. At any level of care, treatment should be individualized and take into
consideration the member’s stage of readiness to change and participate in treatment. Screenings and
assessments are used as tools to determine the right treatment, at the right time, at the appropriate level of
care.
Below is a listing of commonly used tools and assessment processes, along with brief explanations.
Assessment and Screening Matrix 1
Assessment Defined Who Time Frame
Administers
Initial Screening Used to determine eligibility for Member Services Upon receipt of call
Medicaid enrollment status and/or Representative
Resiliency Care Management (RCM) (MSR)
Services. May refer to Brief CANS for
CSoC eligibility.
Brief Child and Preliminary assessment for CSoC Magellan Care Upon referral
Adolescent Needs and eligibility and appropriate level of Managers
Strengths (Brief CANS) care. Used in triage by Magellan
Care Managers.
Child and Adolescent Confirms CSoC eligibility and Certified Within 10 days of
Needs and Strengths appropriate level of care. Also used Providers Brief CANs
(CANS) in treatment planning.
When requested and
after authorized by
Magellan
Structured Assessment Assesses risk of violence in OJJ, Juvenile Dependent on person
of Violence Risk in adolescents. Justice Agencies who administers
Youth (SAVRY)
Independent Needs Uses biopsychosocial indicators to A Licensed When requested and
Assessment determine the need for further Mental Health authorized by
comprehensive assessments to Practitioner Magellan
determine the existence of mental (LMHP)
health disorder or serious mental credentialed by
illness and/or used for treatment Magellan
planning. Can also be used to
determine ongoing treatment.
Version 03/2014 16Psychological One mechanism used to better A licensed After completion and
Examination determine or understand the doctoral-level evaluation of initial
existence of mental health disorder psychologist or needs assessment
or serious mental illness. medical that includes a
psychologist diagnostic interview
(Ph.D., Psy.D.,
Ed.D. or M.P.) or
physician with
demonstrated
competence, who
is credentialed by
and contracted
with Magellan
Peer Review Used to determine appropriate level Magellan Within 7 days of
of care. Physician and/or request
Clinician.
Mental Health History/ Completed to determine eligibility Magellan As needed
Records Review for services or placement, Physician and/or
appropriate level of care, and for Clinician.
treatment planning.
Plan of Care Completed to determine goals and Juvenile Justice Prior to beginning
objectives of treatment and/or Agency, DCFS, or treatment services
services Service Provider
Treatment Plan Completed to determine goals and A Licensed Prior to beginning
objectives of evidence-based Mental Health treatment services
treatment Practitioner
(LMHP)
credentialed by
Magellan
Concurrent Review Used to determine progress toward Magellan Care As needed
meeting goals and objectives in Managers
treatment plan.
Discharge Completed (in conjunction with the Service Provider Prior to discharge
Summary/Plan family when applicable) when in collaboration
member is being discharged from with OJJ or DCFS
services. Describes reasons for when necessary
discharge, progress made toward
treatment goals, and plan for Magellan Care
discharge including follow-up Managers
services, if applicable. review/authorize
Behavioral Health Needs Assessments
Behavioral health needs assessments are used to get a comprehensive look at an individual to determine
behavioral health needs. The result is a psycho-social assessment. Behavioral health needs assessments are
not psychological tests or other mental health diagnostic tools. Behavioral health needs assessments are
intended to guide case planning and behavioral service provision, and are used to determine the need for
17psychiatric or other testing. Behavioral health needs assessments must be performed by a licensed mental
health practitioner.
Magellan and state agencies have collaborated to create a mental health assessment template that is
available for use by network providers who administer behavioral health assessments.
18Behavioral Health Assessment Template
1920
21
22
Psychological Testing
Criteria for Authorization
Service Authorization Criteria indicate that an individual must FIRST be assessed by a licensed mental health
practitioner who is credentialed by Magellan to be authorized for Medicaid reimbursable psychological
testing. This bio-psychosocial needs assessment determines the need for and extent of further additional
psychological testing.
Testing may be completed at the onset of treatment to assist in the differential diagnosis and/or help
resolve specific treatment planning questions. It also may occur later in treatment if the individual’s
condition has not progressed and there is no clear explanation for the lack of improvement. The reason for
testing must be based on a specific referral question or questions from the treating provider and related
directly to the psychiatric or psychological treatment of the individual. The specific referral question cannot
be answered adequately by means of clinical interview and or behavioral observations. The testing results
based on the referral questions are reasonably expected to provide information that will effectively guide
the course of treatment.
Psychological testing should serve the function of answering a specific question or solving a specific problem
to inform treatment. It is not meant to be used as a general screening and would only in a very rare
circumstance be rendered immediately. A licensed doctoral-level psychologist or medical psychologist
(Ph.D., Psy.D., Ed.D. or M.P.) or physician with demonstrated competence, who is credentialed by and
contracted with Magellan, administers the psychological tests.
23Chapter 5: Levels of Care
Magellan believes and research supports that optimal, high-quality care is best delivered when
members receive treatment that meets their needs in the least intensive, least restrictive setting
possible. Magellan’s philosophy is to endorse treatment that is safe and effective, and that maximizes
the member’s independence in daily activity and functioning.
Crisis Planning and Intervention
Crisis services do not require prior authorization. Crisis Intervention is available to all youth who meet
service authorization criteria. Crisis Stabilization is available to youth in the Coordinated System of Care.
Crisis response services are accessible 24 hours a day, 7 days a week, 365 days a year, by contacting
Magellan Member Services at 1-800-424-4399.
Written crisis plans will include:
• History of Crisis
• Triggers and Warning Signs
• Potential Crisis Situations
• Action Steps to prevent a crisis
• Action Steps to intervene in a crisis
• Responsibilities and agreements of the child/youth, family members, natural supports, and other
members involved with the family
• Contacts and phone numbers in the event of a crisis
Outpatient Services
The State of Louisiana has defined an array of outpatient services, including:
1. Assertive Community Treatment (ACT)
2. Community Psychiatric Support and Treatment
3. Crisis Intervention
4. Electroconvulsive Therapy
5. Functional Family Therapy
6. Homebuilders
7. Multisystemic Therapy
8. Outpatient Therapy
9. Psychosocial Rehabilitation
10. Psychological Testing
11. Outpatient Addictive Services
1. Assertive Community Treatment (ACT)
Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional
problems of individuals who have the most complex and/or pervasive conditions associated with a major
mental illness or co-occurring addictions disorder. These interventions are strength-based and focused on
promoting symptom stability, increasing the individual’s ability to cope and relate to others and enhancing
the highest level of functioning in the community. Interventions may address adaptive and recovery skill
areas, such as supportive or other types of housing, school and training opportunities, daily activities, health
and safety, medication support, harm reduction, money management and entitlements, and service
planning and coordination.
Version 03/2014 24ACT services are accessible to individuals who are 18 years of age and older and who meet functional
assessment criteria for target population under the 1915(i) Medicaid waiver. The individual must have one
of the following primary diagnoses (secondary diagnosis of substance abuse disorder or developmental
disability are not an exclusion): Schizophrenia or other psychotic disorder, bipolar disorder, and/or major
depressive disorder.
2. Community Psychiatric Support and Treatment (CPST)
Community Psychiatric Support and Treatment (CPST) are goal-directed supports and solution-focused
interventions intended to achieve identified goals or objectives as set forth in the individual’s individualized
treatment plan. CPST is a face-to-face intervention with the individual present; however, family or other
collaterals also may be involved. A minimum of 51 percent of CPST contacts must occur in community
locations where the person lives, works, attends school and/or socializes.
Services provided to children and youth must include communication and coordination with the family
and/or legal guardian. Coordination with other child-serving systems should occur, as needed, to achieve
the treatment goals.
3. Crisis Intervention (CI)
Crisis Intervention (CI) services are provided to a person who is experiencing a psychiatric crisis and are
designed to interrupt and/or ameliorate a crisis experience, via a preliminary assessment, immediate crisis
resolution and de-escalation, and referral and linkage to appropriate community services to avoid more
restrictive levels of treatment. The goals of CI are symptom reduction, stabilization, and restoration to a
previous level of functioning. All activities must occur within the context of a potential or actual psychiatric
crisis. CI is a face-to-face intervention and can occur in a variety of locations, including an emergency room
or clinic setting, in addition to other community locations where the person lives, works, attends school
and/or socializes. An episode is defined as the initial face-to-face contact with the individual until the
current crisis is resolved, not to exceed 14 days.
4. Electroconvulsive Therapy (ECT)
Electroconvulsive Therapy (ECT) is a medical treatment performed by highly skilled health professionals
including doctors and nurses under the direct supervision of a psychiatrist, who is a medical doctor trained
in diagnosing and treating mental illnesses. A course of treatment with ECT usually consists of six to twelve
treatments given three times a week for a month or less. The member is given general anesthesia and a
muscle relaxant. When these have taken full effect, the member's brain is stimulated, using electrodes
placed at precise locations on the member's head, with a brief controlled series of electrical pulses. This
stimulus causes a seizure within the brain, which lasts for approximately a minute. Because of the muscle
relaxants and anesthesia, the member's body does not convulse and the member feels no pain. The
member awakens after five to ten minutes, much as he or she would from minor surgery.
5. Functional Family Therapy (FFT)
Functional Family Therapy (FFT) services are targeted for youth (aged 10-18) primarily demonstrating
externalizing behaviors which affect family functioning. Youth behaviors include antisocial behavior or acts,
violent behaviors and other behavioral issues that impair functioning. Youth also may meet criteria for a
disruptive behavior disorder, Attention-Deficit Hyperactivity Disorder (ADHD), oppositional defiant disorder
and/or conduct disorder. Youth with other mental health conditions, such as anxiety and depression, also
25may be accepted as long as the existing behavioral health issues manifest in outward behaviors that impact
the family and multiple systems. Youth with substance use issues may be included if they meet the criteria
below, and FFT is deemed clinically more appropriate than focused drug and alcohol treatment. A youth
receives FFT for approximately three to four months. During the course of this three-month period, the
therapist works with the family in 9 to 14, one- to two-hour sessions for less severe cases and up to 26-32,
one- to two-hour sessions for youth with more substantial acting-out behaviors.
6. Homebuilders
Homebuilders is an evidenced based model of intensive home based services in order to provide family
preservation (prevention of out-of-home care), reunification and stabilization services. The intervention
takes advantage of family crisis situations to promote change in the family with intensive, brief services
(generally four to six weeks in duration with an average of 38-40 direct face-to-face hours), delivered
primarily in the family home. Therapists have very small caseloads (two) and they are available 24 hours a
day. Homebuilders is used for the most serious of situations where safety threats have been identified and
the child (0-17) is at imminent risk of being removed from the home and placed in foster care, group home
settings, residential treatment, psychiatric hospitals or juvenile justice facilities. Appropriate referrals also
include those where intensive services are needed in order for a child to return home from foster care, or in
order to stabilize a foster placement (thereby reducing the number of moves that can be very traumatizing
to a child).
Therapists engage, assess and intervene with families using cognitive and behavioral interventions and
direct teaching of skills tailored to each family (all while structuring for safety in high risk, multi-problem
families). Some therapeutic goals; improving parenting skills, family functioning, parent/caregiver and
children’s behavior and emotion management skill, and increase safety of all family members, in order for
children/youth to live safely at home. Family situations necessitating Homebuilders can range from out of
control substance abuse (parent or youth), domestic violence, physical abuse, sexual abuse to medical
neglect (to name a few). Two “booster sessions” (provided within six months of service closure) are also
available, as needed, in order to support the changes made by the family and reinforce skills taught.
7. Multisystemic Therapy (MST)
Multisystemic Therapy (MST) services are targeted for youth 12 to 17 years old. MST provides an intensive
home/family and community-based treatment for youth who are at risk of out-of-home placement or who
are returning from out-of-home placement. The MST model is based on empirical data and evidence-based
interventions that target specific behaviors with individualized behavioral interventions. Services are
primarily provided in the home, but workers also intervene at school and in other community settings. The
duration for MST services is three to six months but, typically no longer than six months. The therapist
meets with the youth and family at least weekly but often during a four-month period, as well as about 35
hours of non-direct contact provided to the ecology of the youth (e.g., consultation and collaboration with
other systems).
8. Outpatient Therapy
Outpatient Therapy is typically individual, family and/or group outpatient psychotherapy, consultative
services (including nursing home consultation), behavioral health needs assessment, evaluation and testing.
Times for provision of these service episodes range from fifteen minutes (e.g., medication checks) to fifty
minutes (e.g., individual, conjoint, family psychotherapy), and may last up to two hours (e.g., group
psychotherapy).
269. Psychosocial Rehabilitation (PSR)
Psychosocial Rehabilitation (PSR) services are designed to assist the individual with compensating for or
eliminating functional deficits and interpersonal and/or environmental barriers associated with their mental
illness. Activities included must be intended to achieve the identified goals or objectives as set forth in the
individual’s individualized treatment plan. The intent of PSR is to restore the fullest possible integration of
the individual as an active and productive member of his or her family, community and/or culture with the
least amount of ongoing professional intervention. PSR is a face-to-face intervention with the individual
present. Services may be provided individually or in a group setting. A minimum of 51 percent of a PSR’s
contacts must occur in community locations where the person lives, works, attends school, and/or
socializes.
10. Psychological Testing
Consistent with LAC, Title 46, Part LXIII, Chapter 17, Title 46, § 1702, psychological tests are defined as
intellectual, personality and emotional, and neurological instruments, which require the administration of a
psychologist/medical psychologist or of a qualified technician supervised by a psychologist/medical
psychologist (without limiting or restricting the practice of physicians duly licensed to practice medicine by
the Board of Medical Examiners). Tests of language, educational and achievement tests, adaptive behavior
tests or behavior rating scales, symptom screening checklists or instruments, semi-structured interview
tools, and tests of abilities, interests, and aptitude that may be administered by other appropriately licensed
or certified professionals are not deemed as psychological tests. Testing may be completed at the onset of
treatment to assist in the differential diagnosis and/or help resolve specific treatment planning questions. It
also may occur later in treatment if the individual’s condition has not progressed and there is no clear
explanation for the lack of improvement.
11. Outpatient Addiction Services
Addiction Services include an array of individual-centered outpatient and intensive services consistent with
the individual’s assessed treatment needs, with a rehabilitation and recovery focus designed to promote
skills for coping with and managing substance abuse symptoms and behaviors. Services for adolescents
must be separate from adult services, be developmentally appropriate, involve the family or caregiver and
coordinate with other systems (such as child welfare, juvenile justice and the schools). These services are
designed to help individuals achieve changes in their substance abuse behaviors. Services address an
individual’s major lifestyle, attitudinal and behavioral problems that have the potential to be barriers to the
goals of treatment. Outpatient services may be indicated as an initial modality of service for an individual
whose severity of illness warrants this level of treatment or when an individual’s progress warrants a less
intensive modality of service than they are currently receiving. Intensive outpatient treatment is provided
any time during the day or week, and provides essential skill restoration and counseling services for
individuals needing more intensive treatment. Outpatient, and intensive outpatient are delivered on an
individual or group basis in a wide variety of settings designed to help individuals achieve changes in their
substance use behaviors.
Addiction Services are reviewed utilizing the American Society of Addiction Medicine (ASAM) PPC-2R
criteria. These levels of care criteria are found in the ASAM PPC-2R manual, which will be used for
authorizing and reviewing addiction services. More information on the ASAM PPC-2R manual can be found
online at http://www.asam.org/publications/the-asam-criteria.
27Out-of-Home Placement
The State of Louisiana has defined several levels of out-of-home placement care. The levels of care are:
1. Residential Addiction Services
2. Non-medical Group Home (NMGH)
3. Therapeutic Foster Care (TFC)
4. Therapeutic Group Home (TGH)
5. Psychiatric Residential Treatment Facility (PRTF)
6. Inpatient Psychiatric Hospital (IP)
Medical necessity, along with criteria sets is used by providers or reviewers to determine a clinically
necessary level of care. Medical necessity for admission into inpatient and residential levels of care require
that the (1) severity of need criteria, (2) intensity and quality of service criteria, and (3) continued stay
criteria for particular levels of care be met.
1. Residential Addiction Services
Residential Addiction Services are residential/inpatient services consistent with the individual’s assessed
treatment needs, with a rehabilitation and recovery focus designed to promote skills for coping with and
managing substance abuse symptoms and behaviors. Services for adolescents must be separate from adult
services, be developmentally appropriate, involve the family or caregiver and coordinate with other systems
(such as child welfare, juvenile justice and the schools). These services are designed to help individuals
achieve changes in their substance abuse behaviors. Services address an individual’s major lifestyle,
attitudinal and behavioral problems that have the potential to be barriers to the goals of treatment.
Residential/inpatient services are delivered on an individual or group basis in a wide variety of settings,
including treatment in residential settings of 16 beds or less, designed to help individuals achieve changes in
their substance use behaviors.
Addiction Services are reviewed utilizing the American Society of Addiction Medicine (ASAM) PPC-2R
criteria. The level of care criteria is found in the ASAM PPC-2R manual, which is used for authorizing and
reviewing addiction services. More information on the ASAM PPC-2R manual can be found online at
http://www.asam.org/publications/the-asam-criteria.
2. Non-Medical Group Home
Non-Medical Group Home (NMGH) is a residential setting for up to 16 beds. This basic type of placement is
be limited to children whose needs cannot be met in their own home or foster home, or children who have
reached their treatment goals in a more restrictive setting.
Services provided in a non-medical group home setting must be provided by a community practitioner
certified and credentialed by Magellan to provide those services. For the child entering placement, group
home provides a chance to work on issues in a structured, safe, and orderly environment. Group home care
presents an opportunity to improve the safety, permanency and well-being of a child through a specialized
offering of services that are flexible to meet the particular needs of a child and his or her family or other
permanency resource.
28You can also read