MODELLI DECISIONALI Prof. Maurizio Iacobone - Società Triveneta di Chirurgia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Oderzo, 11 Maggio 2018
INQUADRAMENTO DIAGNOSTICO E TERAPEUTICO DEL
NODULO TIROIDEO TIR3 - UPDATE
MODELLI DECISIONALI
Prof. Maurizio Iacobone
Chirurgia Endocrina
Dipartimento di Scienze Chirurgiche, Oncologiche e Gastroenterologiche
Università degli Studi di Padova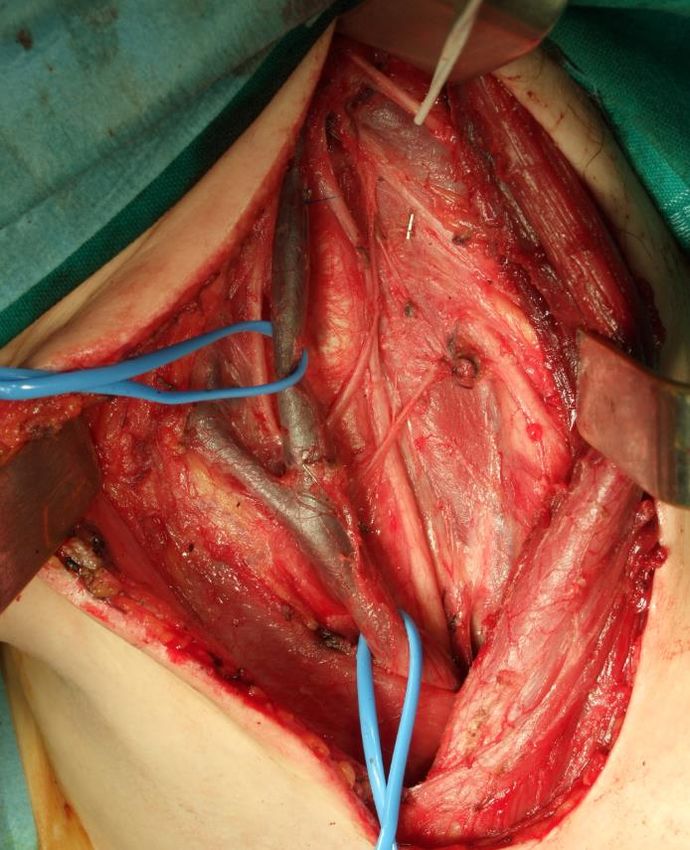
NO DISCLOSURE ✓ Il nodulo TIR3: questo “sconosciuto” ✓ Cosa fare: Chirurgia vs Follow up ✓ Come operare ✓ Dove operare

NODULO TIROIDEO TIR3
NODULO TIROIDEO TIR3
Bethesda (2009)
TIR1
TIR2
TIR3a
TIR3B
TIR4
TIR5
Thyroid Nodule - GUIDELINES
Association Year
US Preventive Service Task Force (USPSTF) 2016
AACE/ACE/AME 2016
American Thyroid Association (ATA) 2015
European Society of Endocrine Surgeons (ESES) 2014
British Thyroid Association (BTA) 2014
National Comprehensive Cancer Network (NCCN) 2013
French ENT Society 2012
European Society for Medical Oncology (ESMO) 2012
Japanese Society of Thyroid Surgeons 2011
Latin American Thyroid Society 2009
American Thyroid Association (ATA) 2009
Most Recommendations are based on Low-Moderate evidence!. These guidelines should not be interpreted as a replacement for clinical judgement and should be used to complement informed, shared patient–health care provider deliberation on complex issues… Finally, it is not the intent of these guidelines to replace individual decision-making, the wishes of the patient or family, or clinical judgment.
We encourage medical professionals to use this information in conjunction with their best clinical judgment. Any decision by practitioners to apply these guidelines must be made in light of local resources and individual patient circumstances and preference.
THYROID NODULE
Gharib, Endocr Pract 2016TIR 3a 7.3.2.1 Management of low-risk indeterminate lesions (AUS/FLUS, Thy 3a, or TIR 3A) • Consider conservative management in the case of favorable clinical criteria, such as personal or family history, lesion size, and low-risk US and elastography features [BEL 3, GRADE C]. • Repeat FNA for further cytologic assessment and review samples with an experienced cytopathologist [BEL 3, GRADE B]. • We do not recommend either in favor or against the determination of molecular markers for routine use in this category (see Section 7.6.3.3.) [BEL 3, GRADE D].
TIR 3b 7.3.2.2 Management of high-risk indeterminate lesions Surgery is recommended for most thyroid lesions in this category [BEL 2, GRADE A]. Thyroid lobectomy plus isthmectomy is recommended. Total thyroidectomy may be performed, depending on clinical setting, coexistence of contralateral lobe thyroid nodules, and patient preference [BEL 2, GRADE A]. Consider close clinical follow-up in a minority of cases with favorable clinical and US features, but only after multidisciplinary consultation and discussion of treatment options with the patient [BEL 4, GRADE C].
TIR 3a
RECOMMENDATION 15*
(A) For nodules with AUS/FLUS cytology, after consideration of worrisome clinical
and sonographic features, investigations such as repeat FNA or molecular
testing may be used to supplement malignancy risk assessment in lieu of
proceeding directly with a strategy of either surveillance or diagnostic surgery.
Informed patient preference and feasibility should be considered in clinical
decision-making. (Weak recommendation, Moderate-quality evidence)
(B) If repeat FNA cytology, molecular testing, or both are not performed or
inconclusive, either surveillance or diagnostic surgical excision may be performed
for an AUS/FLUS thyroid nodule, depending on clinical risk factors, sonographic
pattern, and patient preference (Strong recommendation, Low-quality evidence)
*The final draft for the sections (A15–A19) and recommendations (13–17) were revised and
approved by a subgroup of seven members of the task force with no perceived conflicts or
competing interests in this area.TIR 3b
RECOMMENDATION 16*
(A) Diagnostic surgical excision is the long-established standard of care for the
management of FN/SFN cytology nodules. However, after consideration of
clinical and sonographic features, molecular testing may be used to
supplement malignancy risk assessment data in lieu of proceeding directly
with surgery. Informed patient preference and feasibility should be
considered in clinical decision-making (Weak recommendation, Moderate-
quality evidence)
(B) If molecular testing is either not performed or inconclusive, surgical excision
may be considered for removal and definitive diagnosis of an FN/SFN thyroid
nodule surgical excision may be considered for removal and definitive diagnosis of
an FN/SFN thyroid nodule (Strong recommendation, Low-quality evidence)
*The final draft for the sections (A15–A19) and recommendations (13–17) were revised and
approved by a subgroup of seven members of the task force with no perceived conflicts or
competing interests in this area.TIR 3b RECOMMENDATION 19 When surgery is considered… thyroid lobectomy is the recommended initial surgical approach. This approach may be modified based on clinical or sonographic characteristics, patient preference, and/or molecular testing (Strong recommendation, Moderate-quality evidence) RECOMMENDATION 20 Total thyroidectomy may be preferred in patients with indeterminate nodules that are cytologically suspicious for malignancy, positive for known mutations specific for carcinoma, sonographically suspicious, or large (>4 cm), or in patients with familial thyroid carcinoma or history of radiation exposure (Strong recommendation, Moderate-quality evidence)… bilateral nodular disease, those with significant medical comorbidities, or those who prefer to undergo bilateral thyroidectomy to avoid the possibility of requiring a future surgery on the contralateral lobe
Consensus statement AIT, AME, SIE, SIAPEC-IAP 2014
ATA GUIDELINES
Meno Chirurgia
Meno Complicanze
• Major goal of these guidelines is to minimize
potential harm from overtreatment in a majority
of patients at low risk for disease-specific mortality
and morbidity, while appropriately treating and
monitoring those patients at higher risk.Surgeon experience and Morbidity
Surgeon experience likely influences the risks of thyroidectomy,
with higher volume surgeons having lower complication rates
• Low volume Surgeons (100 cases/yr) – Complications: 7.5%.
In USA Over 80% of thyroid resections were performed by low-
and intermediate-volume surgeons.
Kandil, Surgery 2013Tiroidectomie per
CARCINOMA TIROIDEO
Regione VENETO 2016
350
317
300
250
195
200
150
97
100
54
50 33
20 21 20 19 18 13 10 8 6 5
0
A B C D E F G H I L M N P Q RCHIRURGIA ENDOCRINA - PADOVA
2017
INTERVENTI n=564
✓SURRENECTOMIE n=49
✓PARATIROIDECTOMIE n=59
✓TIROIDECTOMIE n=456CHIRURGIA ENDOCRINA - PADOVA
www.eurocrine.euEUROCRINE (EUROPA), BAETS (UK)
CESQUIP (USA), SQRTPA (SVEZIA)
22 STATI, 314 DIPARTIMENTI DI CHIRURGIA,
Gennaio 2015 – Giugno 2017
n=21746 pazienti
(FNAC – Tiroidectomia – esame istologico)
FNAC Istologia (Carcinoma)
TIR1 19,2%
TIR2 12,7%
TIR3a 31,9%
TIR3b 31,4%
TIR4 77,8%
TIR5 96%
Iacobone 2018 (submitted)EUROCRINE (EUROPA), BAETS (UK)
CESQUIP (USA), SQRTPA (SVEZIA)
22 STATI, 314 DIPARTIMENTI DI CHIRURGIA,
Gennaio 2015 – Giugno 2017
n=21746 pazienti
(FNAC – Tiroidectomia – esame istologico)
FNAC Carcinoma
M 31-35 aa= 52,1%
TIR3a 31,9%
M 36-40 aa= 55,9%
TIR3b 31,4%
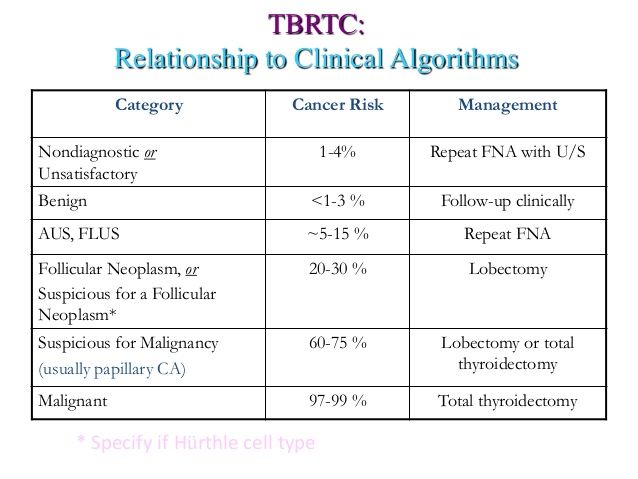
Iacobone 2018 (submitted)FNAC Rischio Malignità TIR3a 31,9% TIR3b 31,4%
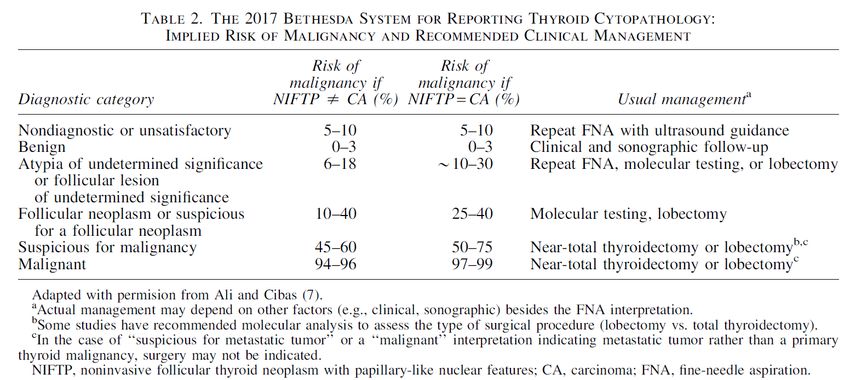
2017 BETHESDA SYSTEM
Thyroid, 2017CONCLUSIONI ✓ Il nodulo TIR 3: questo “sconosciuto” ✓ Cosa fare: Chirurgia vs Follow up ✓ Come operare ✓ Dove operare
CONCLUSIONI
✓ Il nodulo TIR 3: questo “sconosciuto”
TIR 3a vs TIR 3b
???CONCLUSIONI
✓Cosa fare: Follow up vs Chirurgia
Stratificazione del rischio
• Biologia molecolare
• Calcitonina
• Familiarità
• Precedenti irradiazioni
• Caratteristiche ecografiche
• Dimensioni del nodulo
• Preferenze del pazienteCONCLUSIONI
✓ Come operare - Dove operare
-Emitiroidectomia vs Tiroidectomia totale
Dimensioni del nodulo
Malattia mono/bilaterale
Familiarità
Irradiazione
Preferenze del paziente
-Chirurghi espertiUNIVERSITA’ DI PADOVA
CORSO DI PERFEZIONAMENTO
ottobre 2018- settembre 2019
CHIRURGIA ENDOCRINA
PER INFORMAZIONI:
http://www.unipd.it/corsi-perfezionamento
maurizio.iacobone@unipd.itChirurgia Endocrina - Padova maurizio.iacobone@unipd.it
You can also read