Evaluation of Astigmatic Correction Using Vector Analysis after Combined FLACS and ISAK - Winter Symposium | ASCRS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Evaluation of Astigmatic Correction Using Vector Analysis after
Combined FLACS and ISAK
Sanghyu Nam, Su Young Moon , Jungyeob Han,
Hun Lee, Jae Yong Kim, Hungwon Tchah
Department of Ophthalmology,
University of Ulsan College of Medicine,
Asan Medical Center
* No financial interest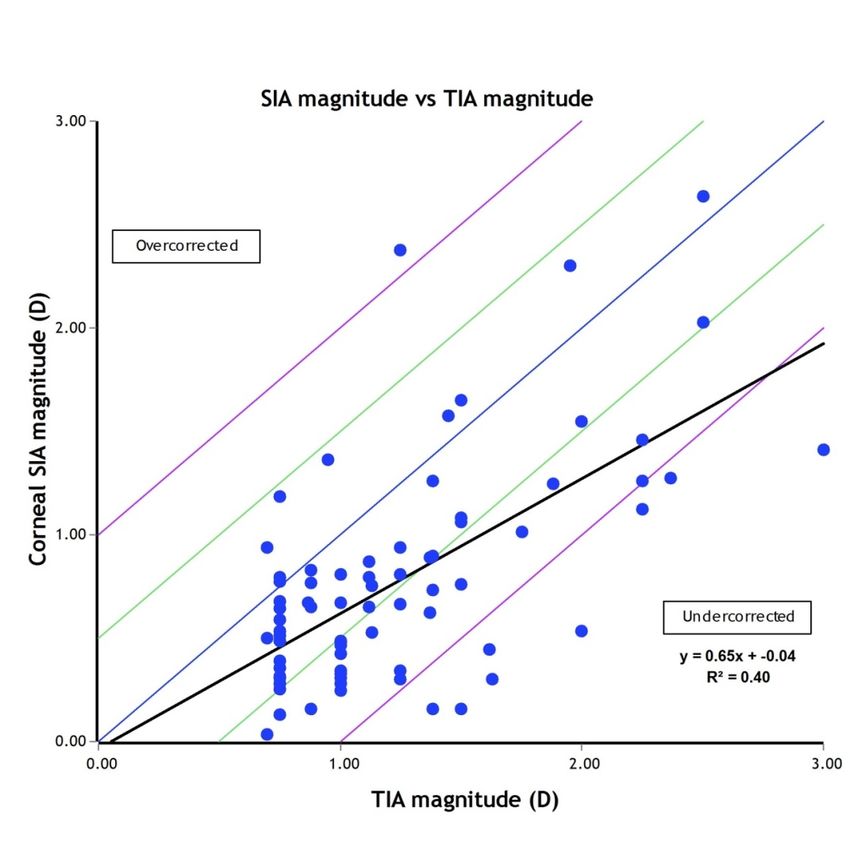
INTRODUCTION
Uncorrected astigmatism after cataract surgery significantly compromises a patient’s vision and leads to reduced quality of life.
JCRS 2010:36;9;1479-1485
More than 1/3 of Cataract patients have Cornea astigmatism between 1-3D, more than 2/3 above 0.5D.
JCRS 2011:37;3;454-460
The 2 major techniques for the Correction of Corneal Astigmatism during Cataract surgery
1. Toric intraocular lens
proved to have high accuracy and efficacy in correcting astigmatism Ophthalmology 2010;117:1228-1235
2. Corneal Arcuate incision
Relaxing incision
• Lack of precision and reproducibility of incision depth and length
• Potential for axis misalignment
Femtosecond laser Arcuate keratotomy
• Favorable accuracy, safety, and reproducibility
• Reducing astigmatism with keratoplasty, residual astigmatism from cataract and refractive surgery.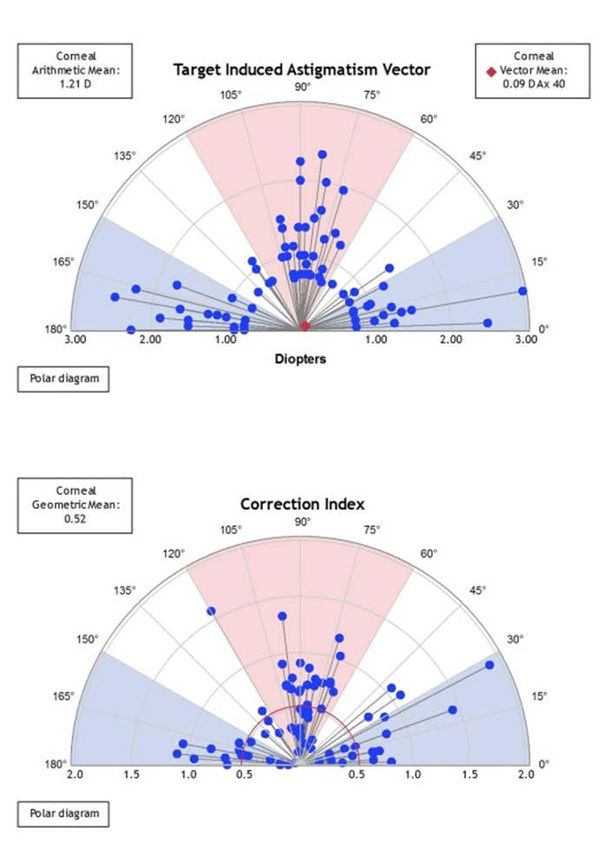
INTRODUCTION Intrastromal AK nomogram (v3 Julian Stevens)
PURPOSE The aim of our study was to evaluate astigmatic correction in patients with mild to moderate astigmatism using Alpins vector analysis method after combined FLACS(femtosecond laser-assisted cataract surgery) and ISAK(Intrastromal Arcuate keratotomy) using a nomogram provided by Dr. Julian Stevens. We aimed to investigate the aforementioned approach, in order to increase the accuracy of ISAK and to determine the adjustments needed for the nomogram.
METHOD
Retrospective study including patients who got combined FLACS and ISAK with corneal astigmatism (0.5-3.0D)
between 2017.04-2019.06, Asan Medical Center in Seoul, Korea
Preoperative & Postoperative Examination for corneal astigmatism.
① Autorefractive keratometer (KR-1®)
② Scanning slit topography (ORB scan)
③ Partial coherence interferometry (IOL Master 500)
④ Ocular aberrometry (OPD-scan)
The CCT and longest diameter of WTW were obtained during surgery on a laser platform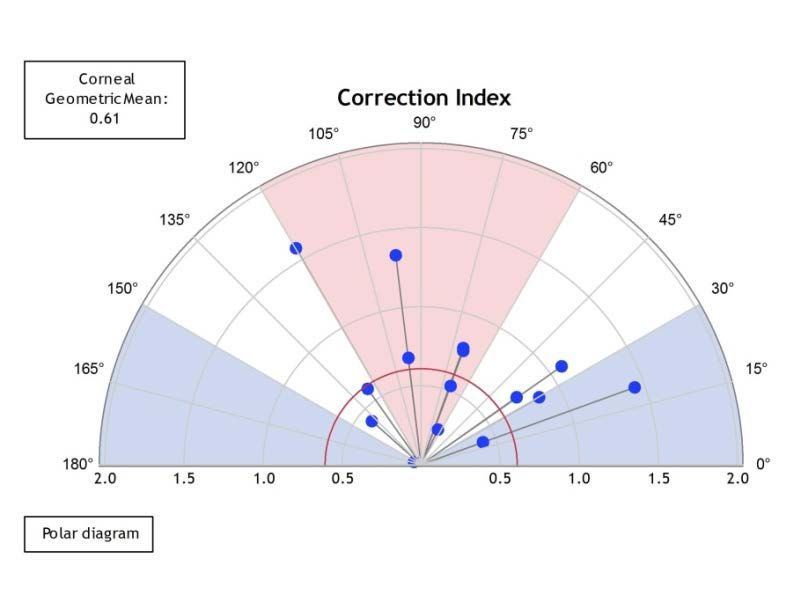
METHOD : Surgical technique
CATALYS ® Precision femtosecond laser system (AMO)
Horizontal limbal marker to avoid cyclotorsion
Align suction ring with corneal marks
Confirm the surgical site and depth using the incorporated OCT cross section
Capsulotomy & Lens fragmentation
Intrastromal Arcuate keratotomy
Paired symmetric (same length) incisions centered on the steep corneal axis
Diameter : 8.0mm
Depth : Central 60% of total corneal thickness (20-80% of the corneal thickness and a limbal-based flap)
Arc Length (30°-90°) depending on patient’s age & magnitude and axis of the astigmatism.
Main wound incision
Limbal incision with 2.2mm keratome, ant. capsule button was removed using forceps.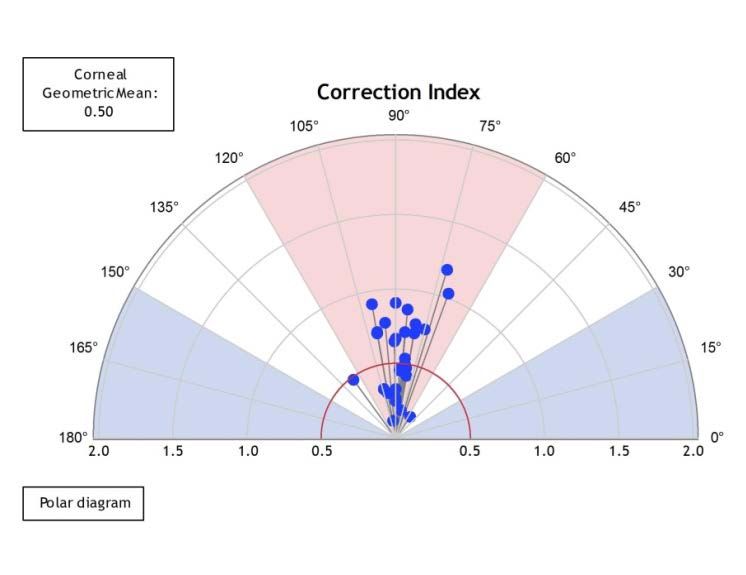
Introduction
RESULT preoperative patient demographics & ocular biometric parameters .
N = 79 Mean, SD
Age 66.95, 10.75
Sex (M:F) 35 : 44
Laterality (OS:OD) 23 : 56
Astigmatism axis
35 : 29 : 15
(WTR:ATR:OBL)
Pre-op endothelial cell count (cell/mm2) 2532.37, 424.47
Longest White to White (mm) 11.37, 0.50
Central corneal thickness (μm) 585.35, 32.49
ATR, against-the-rule; WTR, with-the-rule; OBL, oblique astigmatism.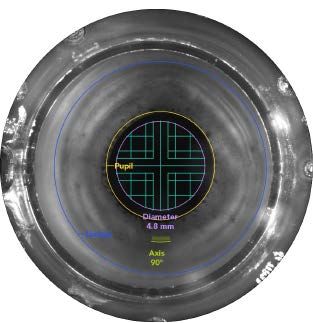
Introduction
RESULT preoperatively and at 1 and 3 months postoperatively
The values of the corneal astigmatism recorded
Autokeratometer (KR-1®) Topography (ORBscan®)
K astig Δ† K astig Δ†
p# p#
(Mean, SD) (Mean, SD) (Mean, SD) (Mean, SD)
Pre-op 1.23, 0.52 1.17, 0.66
Post-op 1 mo 0.85, 0.42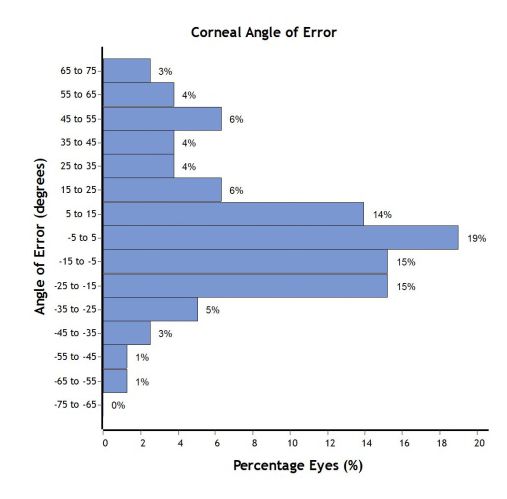
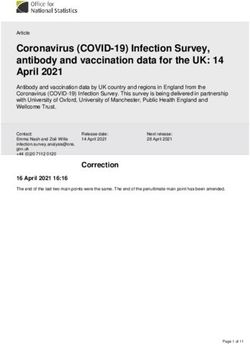
Introduction The outcomes of the vector analysis via the comparison of the preoperative with
RESULT the postoperative values measured by Autokeratometer
Mean, SD
TIA (D) 1.21, 0.52
SIA (D) 0.76, 0.53
DV (D) 0.86, 0.50
ME (D) -0.46, 0.45
AE (°) 4.02, 28.7
Absolute AE (°) 21.7, 19.0
CI 0.62, 0.34
CA 2.48, 2.61
FI 0.45, 0.21
ORA (D) 0.06, 0.47
TIA, target-induced astigmatism; SIA, surgically induced astigmatism; DV, difference vector; ME,magnitude of error; AE, angle of error; Absolute AE, absolute angle of error;
CI, correction index; CA,coefficient of adjustment; FI, flattening index; ORA, ocular residual astigmatism
The outcomes of the vector analysis via the comparison of the preoperative with
RESULT the postoperative values measured by Autokeratometer
Mean, SD
TIA (D) 1.21, 0.52
SIA (D) 0.76, 0.53
DV (D) 0.86, 0.50
ME (D) -0.46, 0.45
AE (°) 4.02, 28.7
Absolute AE (°) 21.7, 19.0
CI 0.62, 0.34
CA 2.48, 2.61
FI 0.45, 0.21
ORA (D) 0.06, 0.47
TIA, target-induced astigmatism; SIA, surgically induced astigmatism; DV, difference vector; ME,magnitude of error; AE, angle of error; Absolute AE, absolute angle of error;
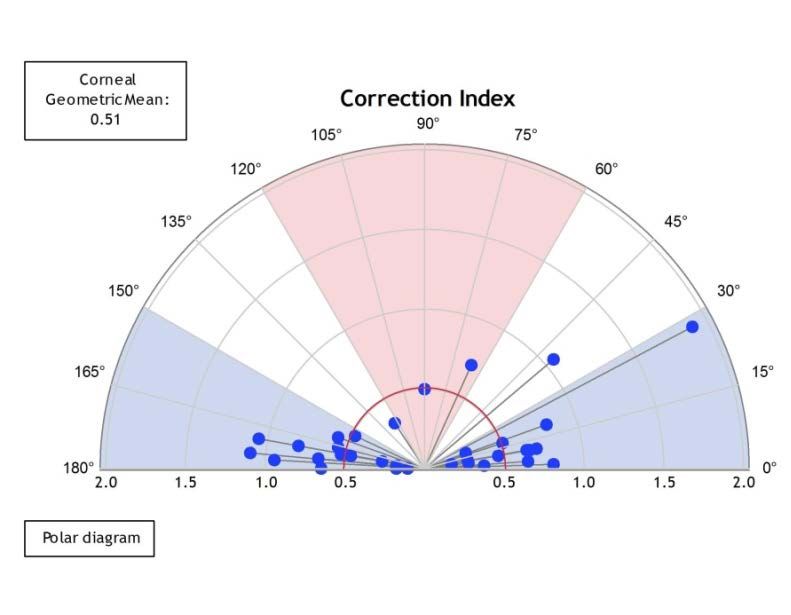
CI, correction index; CA,coefficient of adjustment; FI, flattening index; ORA, ocular residual astigmatismRESULT : The single angle polar plots displaying the distribution of the correction
index according to the astigmatism axis.
WTR ATR OBL
CI = 0.60 CI = 0.58 CI = 0.77
(a) WTR, With-The-Rule astigmatism; (b) ATR, Against-The-Rule astigmatism; and (c) OBL, oblique astigmatism.RESULT The correlation analysis between the SIA& TIA in subgroups according to the patient’s age (A)
and the longest WTW (B).
According to Univariate regression analysis, there was a negative correlation between the age and the CI ( p = 0.022*)
The WTW, CCT and axis of astigmatism did not show a significant correlation with the CI.RESULT The correlation analysis between the SIA& TIA in subgroups according to the patient’s age (A)
and the longest WTW (B).
According to Univariate regression analysis, there was a negative correlation between the age and the CI ( p = 0.022*)
The WTW, CCT and axis of astigmatism did not show a significant correlation with the CI.Discussion
IntraStromal keratotomy Group (Paired)
• Day et al. reported a CI of 0.63 ± 0.32 after 1m.
• Byun et al., reported a CI of 0.87 ± 0.50 after 6m. In the current study, the CI was 0.62 ± 0.34 after 3 m
Penetrating Keratotomy Group
• Chan et al. reported a CI of 0.85 ± 0.48 after 2yr.
Conventionally, recommended postoperative astigmatism has been targeted at 0.25 to 0.5 D WTR to accommodate
the gradual ATR drift expected with aging.
In mild to moderate astigmatism , the axis and amount of cornea astigmatism tends to appear in variable according
to measuring devices. It is more difficult to measure accurate and reliable value than in high cornea astigmatism.
Errors in the anterior corneal measurements might result in refractive surprises postoperatively
During femtosecond laser–assisted cataract surgery, clinically significant cyclotorsion error can occur.
Every degree of rotational error negatively affects the astigmatism treatment by approximately 3.5%.
The precise measure of the axis during the Femto-laser arcuate keratotomy is essential in order to increase
the accuracy of ISAK. Am J Ophthalmol 2021;221:97–104
JCRS 2008;34:1631-1636Conclusion Our study showed that FLACS and ISAK reduced postoperative cornea astigmatism effectively and safely. Precise preoperative and intraoperative measurement of the cornea astigmatism is essential for improving the outcome of the ISAK.
Thank you for attention
You can also read