Structural changes in the corneal subbasal nerve plexus in keratoconus - Augenklinik
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Acta Ophthalmologica 2020
Structural changes in the corneal subbasal nerve
plexus in keratoconus
Elias Flockerzi, Loay Daas and Berthold Seitz
Department of Ophthalmology, Saarland University Medical Center, Homburg, Germany
ABSTRACT. the disease. Corneal confocal micro-
Background: Corneal confocal microscopy (CCM) allows visualizing slightest scopy (CCM) allows visualizing slight-
alterations within the corneal subbasal nerve plexus (SNP). Recent CCM studies est alterations within the corneal
based on the analysis of three–five CCM images per eye assumed a reduced subbasal nerve plexus (SNP) (Richter
corneal nerve fibre length (CNFL) in keratoconus (KC). et al. 1997), which is formed by branches
Methods: The SNP of KC patients (n = 23, 13 contact lens wearing, 10 of the trigeminal nerve (M€ uller et al.
noncontact lens wearing) and patients without KC (n = 16) was examined by 10 1997). Corneal confocal microscopy
CCM images of one eye per patient. The CNFL per frame area was calculated, (CCM) studies based on the analysis of
and the SNP tortuosity was quantified by measuring (a) the amplitude of the three (Simo Mannion, Tromans &
O’Donnell 2005; Niederer et al. 2008;
curves and (b) the area under the curve (AUC) formed by the SNP.
Song et al. 2016) to five (Bitirgen et al.
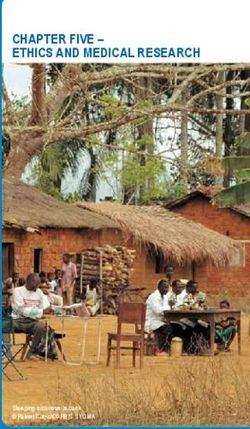
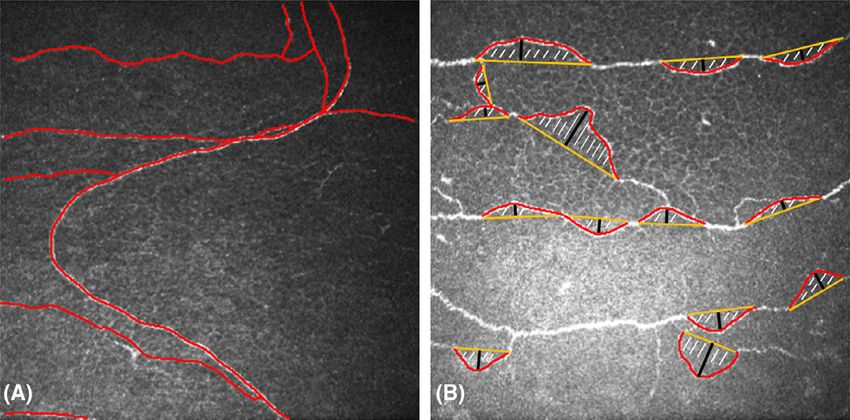
Results: Analysing 390 non-overlapping confocal images revealed the CNFL (mm/
2013; Bitirgen et al. 2015; K€ ohler et al.
mm2) to be significantly lower in KC (16.4 1.9 mm/mm2) than in healthy corneae 2017) corneal confocal images per eye,
(23.8 3.3 mm/mm2, p < 0.0001; mean SD; p-value calculated using the and patient indicated that there is a
Mann–Whitney U-test), without a difference between contact lens wearing and reduced corneal nerve fibre length
noncontact lens wearing KC patients (p = 0.4). Amplitudes and AUCs analysed as (CNFL) and an abnormal winding
median with 25th and 75th percentile were significantly increased in KC (amplitude course of the SNP in KC. But Allgeier
33/23/41 µm and AUC 2839/1545/3444 µm2) compared to healthy corneae et al. (2017) pointed out that reliable and
(amplitude 24/18/28 µm and AUC 1870/1193/2327 µm2, p < 0.0001). reproducible data should be based on
Conclusions: Corneal confocal microscopy (CCM) visualizes slightest alterations the analysis of at least 9.4 corneal
within the SNP in KC including (a) a significantly lower CNFL and (b) an enhanced confocal images corresponding to a
winding course of the SNP. The significantly lower CNFL observed in KC may minimum sampled area of 1.5 mm2 of
support the hypothesis of a neurodegenerative aspect of the disease and might be a the central SNP. Several parameters
measure to be correlated with the severity and progression of the disease. have been proposed and were used to
describe the abnormal structure of the
SNP in KC including the corneal nerve
Key words: corneal confocal microscopy – corneal nerve fibre length – keratoconus – subbasal
nerve plexus fibre density, the corneal nerve branch
density, the corneal total branch den-
sity, the corneal nerve fibre width and
Acta Ophthalmol.
the corneal nerve fibre area (Petropou-
ª 2020 The Authors. Acta Ophthalmologica Published by John Wiley & Sons Ltd on behalf of Acta Ophthalmologica
Scandinavica Foundation los et al. 2014; Bitirgen et al. 2015;
This is an open access article under the terms of the Creative Commons Attribution-NonCommercial License, which Pahuja et al. 2016). This study examined
permits use, distribution and reproduction in any medium, provided the original work is properly cited and is not used
for commercial purposes.
the SNP structure by analysis of 10
CCM images per eye in KC patients and
doi: 10.1111/aos.14432 healthy individuals and also proposes a
visual impairment (Goebels et al. 2015). novel way of quantifying the tortuous
Therapy depends on progression of the SNP course in KC visualized by CCM.
disease and includes contact lens fitting,
Introduction surgical treatment via cross-linking,
Keratoconus (KC) is an usually bilateral implantation of corneal ring segments, Patients and Methods
corneal ectasia of unknown aetiology deep anterior lamellar keratoplasty or In this cross-sectional study, the SNP
with progressive and presumed non- penetrating keratoplasty (Goebels, Seitz was examined in the central cornea of
inflammatory thinning of the cornea & Langenbucher 2013). Clinical signs of patients with KC (n = 23, 13 contact
resulting in irregular astigmatism and KC do vary and depend on the stage of lens wearing, 10 noncontact lens
1
Acta Ophthalmologica 2020
wearing) recruited from the Homburg patient or control were included for The study adhered to the principles
Keratoconus Center (Goebels, Seitz & further analysis. Before examination, of the Declaration of Helsinki and was
Langenbucher 2013) without history of the patients’ eyes were topically anaes- approved by the local ethics committee
hydrops corneae or ocular surgery, and thetized with proparacaine (proxymeta- of Saarland (Ethikkommission bei der
of healthy, age-matched patients with- caine) 0.5% (Proparakain-POS 0.5% €
Arztekammer des Saarlandes, approval
out KC or history of ocular surgery eyedrops; Ursapharm, Saarbr€ ucken, number 96/18).
(n = 16). Several CCM images Germany); a carbomer (polyacrylic All subjects were informed about the
(400 µm 9 400 µm, Figs 1 and 2) of acid)-based formulation (Visc-Ophtal nature of the study and provided written
one eye per patient were obtained by Sine, Dr. Winzer Pharma, Berlin, consent before CCM examination. The
CCM using the Heidelberg Retina Germany) was used as an epithelium- diagnosis KC was ensured by clinical slit
Tomograph (HRT, Heidelberg Engi- protective and coupling agent between lamp examination [central or paracentral
neering GmbH, Heidelberg, Germany) the tomograph and the cornea. The thinning, hemosiderin deposition (Fleis-
with the Rostock Cornea Module. patients were instructed to fixate on a cher Ring), Vogt Striae] and Scheimpflug
Thereafter, overlapping images or distance target during the examination imaging based on the Belin/Ambr osio
images affected by motion artefacts with the intention to reduce motion Enhanced Ectasia Display and the
were excluded after independent artefacts and to facilitate examination ‘Enhanced Reference Surface’ (Oculus
reviews by two authors (EF, LD). The of the central cornea. It was aimed to Pentacam; Oculus Optikger€ ate GmbH,
investigators were masked to the KC exclude CCM images of the whorl and 35582 Wetzlar, Germany) diagnosing
stage in the KC group during the exam- the corneal apex area in both healthy and KC in case of pathologic anterior or
ination and masked to the patient KC corneae because of the more tortu- posterior elevation values and a patho-
groups during the CCM image selection. ous course of the SNP in this region. logic final D value (Duncan, Belin, &
Finally, ten CCM images of one eye per Borgstrom 2016). Keratoconus (KC)
stages were classified according to Belin’s
KC stage classification (Belin & Duncan
2016) considering A the anterior radius
of curvature, B the back surface radius of
curvature, C the corneal pachymetry at
thinnest and D the distance best cor-
rected vision. Keratoconus (KC) stages
in our patient group reached from
A0B2C0D0 to A4B4C4D4 according to
this classification, which may also be
used to separate progressive from non-
progressive KC (Kosekahya et al. 2019).
Patient exclusion criteria were neurode-
generative diseases including diabetes,
ocular trauma, previous corneal surgery,
coexisting corneal pathology and kerati-
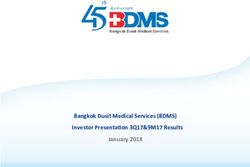
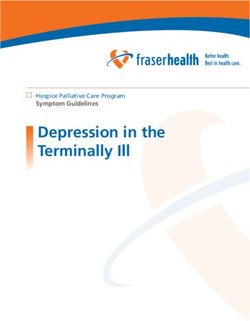
Fig. 1. Corneal confocal microscopy (CCM) images of the subbasal nerve plexus (SNP) tis. Patients wearing contact lenses have
(keratoconus, 400 9 400 µm). (A) SNP tracing (red) done by ImageJ software, long-range
not been excluded.
tortuosity. (B) SNP tracing (red), area under the curve (hatched), baseline (yellow), amplitude
under the curve formed by the SNP (black), short-range tortuosity.
Analysis of the images was performed
using the open-source software ImageJ
(version 1.51, Wayne Rasband,
National Institutes of Health, Bethesda,
MD, USA) and its plugin NeuronJ
(version 1.4.3, Erik Meijering, Univer-
sity of New South Wales, Sydney, Aus-
tralia, https://imagescience.org/meije
ring/software/neuronj/). The CNFL
was calculated as the length (mm) of
nerve fibres per total frame area
(400 µm 9 400 µm) extrapolated to
one square millimetre (Fig. 1A). Statis-
tical analysis was performed using the
Mann–Whitney U-test and Prism5 soft-
ware (GraphPad software Inc., San
Diego, CA, USA).
The analysis of the SNP revealed an
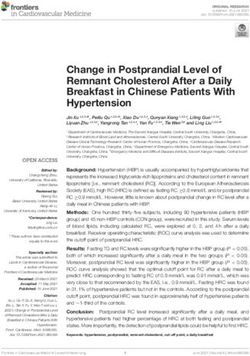
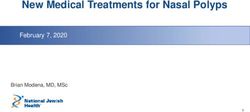
Fig. 2. Corneal confocal microscopy (CCM) images of the subbasal nerve plexus (SNP; alterated structure in KC corneae.
400 9 400 µm). (A) In a healthy cornea, the SNP is of long corneal nerve fibre length (CNFL) and Whilst the SNP in a healthy cornea is
less tortuous. (B) In keratoconus (KC), the SNP is of shorter CNFL with characteristic tortuosity
of less tortuosity (Fig. 2A), the SNP in
(example here A4B4C4D4 according to Belin’s KC classification, Belin & Duncan 2016).
KC is curved and tortuous (Fig. 2B).
2Acta Ophthalmologica 2020
An attempt to quantify this tortuosity healthy corneae (23.8 3.3 mm/mm2, concerning a standardized analysis of
using the open-source software Ima- p < 0.0001; mean SD; p-value cal- the SNP structure (Simo Mannion,
geJ was made by measuring manually culated using the Mann–Whitney U- Tromans & O’Donnell 2005).
(a) the amplitude of the curves formed test, Fig. 3A,B). There was no differ- Previous CCM studies estimated a
by the SNP and (b) the area under the ence in CNFL between contact lens reduced SNP CNFL (Simo Mannion,
curve (AUC) formed by the SNP wearing and noncontact lens wearing Tromans & O’Donnell 2005; Niederer
(Fig. 1B). To measure the amplitudes, KC patients (p = 0.4). Quantification et al. 2008; Song et al. 2016; K€
ohler et al.
an imaginary, ideally straight nerve of the SNP’s tortuosity was made by 2017) by 50% compared to corneae of
fibre course was simulated by ImageJ measuring the amplitude and the AUC healthy individuals (Niederer et al.
software and thereafter, the software of the curves formed by the SNP. The 2008), a rather oblique or horizontal
measured the amplitude (n = 130) of amplitudes and the AUCs were signif- orientation of the nerve fibres (Patel &
the curve formed by the SNP (Fig. 1B). icantly larger in KC (values given as McGhee 2006) and an abnormal nerve
The AUC (n = 130) of the nerve plexus median/25th/75th percentile for ampli- fibre morphology even in early stages of
was measured by manually tracing the tude 33/23/41 µm and AUC 2839/ KC (Patel & McGhee 2006). Even in
curved nerve course and by automati- 1545/3444 µm2) than in healthy cor- topographically inconspicuous partner
cally connecting the beginning and end neae (amplitude 24/18/28 µm and area eyes of advanced KC patients, the SNP
points of the traced line by ImageJ 1870/1193/2327 µm2, p < 0.0001, density was lower than in healthy con-
software (Fig. 1B). The enclosed area Fig. 4A,B). Amplitudes and areas trols (Pahuja et al. 2016), which indi-
was thereafter calculated by ImageJ under the curve were highly correlated cates that subtle changes in the SNP
software (Fig. 1B). Small curves with with a Spearman correlation coefficient structure precede clinical–morphologi-
an enclosed area of ≤1.000 µm2 have of r = 0.803 (p < 0.0001, Fig. 5). cal manifestations of the disease. Mea-
been excluded from analysis, as they suring and extrapolating SNP CNFL,
were present in KC and in healthy however, is not without limitations.
corneae. Curves running out of the
Discussion Lagali et al. (2018) found the CNFL
captured frame were also excluded. In Corneal confocal microscopy (CCM) is to be overestimated by 10% in depth-
snake-like appearances of the nerves, a non-invasive and valuable tool pro- corrected single images (20 images per
only the curves within the captured viding insights into structural changes eye) and to be underestimated by up to
frame were measured. within the human cornea. This study 35% in non-depth-corrected CCM
focuses on the alterations of the SNP in images (20 images per eye). This was
KC based on analysis of the CNFL attributed to a decreased visualization
Results and a quantification of the tortuous of the three-dimensional structure of the
Keratoconus (KC) is characterized by course of the SNP. Whilst the SNP in a SNP in non-depth-corrected CCM
a progressive and presumed non-in- healthy cornea has a longer CNFL and images. Another study found a CNFL
flammatory thinning of the cornea. In is less tortuous, the SNP in KC is of a of 19.6 4.2 mm/mm2 based on the
the patients’ eyes of the study group, significantly shorter CNFL with a analysis of 4.3 CCM images per eye
the central corneal thickness was sig- characteristic tortuosity, which is from 207 eyes of 106 healthy volunteers
nificantly lower in KC patients apparently subject to constant change: (age range 15–88 years, Parissi et al.
(429.8 81.1 µm) than in healthy cor- The SNP’s structure is not static but 2013). They reported an underestima-
neae (550.3 33.4 µm, p < 0.0001, rather dynamic with the nerve fibres of tion of 20% in density when being
Table 1). Statistical analysis of the the SNP centripetally sliding at 5.5– based on single images with minimum
CNFL in 390 CCM images of 23 eyes 17 µm every day (Patel & McGhee nerve density and an overestimation of
from 23 patients revealed that the 2008). The apex position and cone size +21% in density when analysing images
CNFL was significantly lower in KC in KC differ inter-individually and of maximum nerve density leading
(16.4 1.9 mm/mm2) compared to therefore also do form obstacles to an average CNFL of 23–24 mm/
mm2 in maximum density areas (Parissi
Table 1. Summary of patients included and analysed data (based on 10 non-overlapping images et al. 2013). An average CNFL of
per eye from 16 healthy controls and 23 KC patients) 22.4 6 mm/mm2 based on the analy-
sis of three CCM images per eye was
Healthy controls Keratoconus (n = 23
found by Niederer et al. (2008). The
(n = 16) patients) p
current study was based on the analysis
Age SD 36 19.1 36 10.6 of 10 raw non-overlapping CCM images
K-max SD 44.9 2.7 63.2 16.3Acta Ophthalmologica 2020
which could be because not all stadi-
ums were represented equally, but
another study reported a correlation
between advanced KC stages and
decreasing CNFL (Bitirgen et al.
2015). Because KC is characterized
by a progressive ectasia of the cornea,
it might be assumed that nerve fibres
are pulled towards the peripheral
cornea resulting in a rarification of
nerve fibres in the central parts of the
cornea. Ultrastructural studies of KC
Fig. 3. Subbasal nerve plexus (SNP) corneal nerve fibre length (CNFL) calculated as total length of by electron microscopy, however,
nerve fibres (mm) per frame area (mm2). (A) The SNP CNFL in keratoconus (KC) was significantly
pointed out that the degenerative pro-
lower than in control corneae. The p-value (*,Acta Ophthalmologica 2020
KC and control corneae based on 10 Bitirgen G, Ozkagnici A, Bozkurt B & Malik keratoconus: a 5-year longitudinal study.
CCM images per eye and per individ- RA (2015): In vivo corneal confocal micro- JAMA Ophthalmol 1: 70.
ual (a total of 390 CCM images). scopic analysis in patients with keratoconus. Patel DV & McGhee CNJ (2006): Mapping the
Int J Ophthalmol 3: 534–539. corneal sub-basal nerve plexus in kerato-
Wearing contact lenses or not in the
Duncan JK, Belin MW & Borgstrom M conus by in vivo laser scanning confocal
KC group did not influence the results (2016): Assessing progression of kerato- microscopy. Invest Ophthalmol Vis Sci 4:
in view of the differences of CNFL in conus: novel tomographic determinants. 1348–1351.
KC patients and healthy controls. Eye Vis 3: 6. Patel DV & McGhee CNJ (2008): In vivo laser
Corneal nerve fibre length (CNFL) in Goebels S, Seitz B & Langenbucher A (2013): scanning confocal microscopy confirms that
KC was about 24% lower than in Diagnostics and stage-oriented therapy of the human corneal sub-basal nerve plexus is
control corneae. Since mild KC stages keratoconus: Introduction to the Homburg a highly dynamic structure. Invest Ophthal-
were not excluded, it can be assumed Keratoconus Center (HKC). Ophthal- mol Vis Sci 8: 3409–3412.
mologe 9: 808–809. Patel SV, McLaren JW, Hodge DO & Bourne
that the actual difference is to be set
Goebels S, Eppig T, Wagenpfeil S, Cayless A, WM (2002): Confocal microscopy in vivo in
even higher in advanced stages. Mea- Seitz B & Langenbucher A (2015): Staging corneas of long-term contact lens wearers.
suring the amplitudes and the areas of keratoconus indices regarding tomogra- Invest Ophthalmol Vis Sci 4: 995–1003.
under the curves formed by the SNP phy, topography, and biomechanical mea- Petropoulos IN, Alam U, Fadavi H et al.
enables measuring the SNP’s tortuosity surements. Am J Ophthalmol 4: 733– (2014): Rapid automated diagnosis of dia-
itself in KC. Amplitudes and areas 738.e3. betic peripheral neuropathy with in vivo
under the curve were highly correlated, K€ohler B, Allgeier S, Bartschat A et al. (2017): corneal confocal microscopy. Invest Oph-
with the amplitudes’ measurement In vivo imaging of the corneal nerve plexus. thalmol Vis Sci 4: 2071–2078.
Ophthalmologe 7: 601–607. Richter A, Slowik C, Somodi S, Vick HP &
being more suitable in praxi.
Kosekahya P, Caglayan M, Koc M, Kizilto- Guthoff RF (1997): In vivo imaging of
Corneal cross-linking is the main prak H, Tekin K & Atilgan CU (2019): corneal innervation in the human using
stabilizing procedure among the thera- Longitudinal evaluation of the progression confocal microscopy. Ophthalmologe 2:
peutic options in KC disease. Although of keratoconus using a novel progression 141–146.
the CNFL remains reduced after cor- display. Eye Contact Lens 5: 324–330. Simo Mannion L, Tromans C & O’Donnell C
neal cross-linking, tortuosity and nerve Lagali N, Poletti E, Patel DV et al. (2015): (2005): An evaluation of corneal nerve
looping frequency do increase postop- Focused tortuosity definitions based on morphology and function in moderate ker-
eratively (Parissi et al. 2016). Especially expert clinical assessment of corneal sub- atoconus. Cont Lens Anterior Eye 4: 185–
basal nerves. Invest Opthalmol Vis Sci 9: 192.
early KC are reported to show an
5102. Song P, Wang S, Zhang P, Sui W, Zhang Y,
increased frequency of nerve loops, Lagali N, Allgeier S, Guimar~aes P et al. (2018): Liu T & Gao H (2016): The superficial
crossings and tortuosity (Parissi et al. Wide-field corneal subbasal nerve plexus stromal scar formation mechanism in kera-
2016). The subtle SNP changes as mosaics in age-controlled healthy and type toconus: a study using laser scanning in vivo
detected by CCM may therefore be 2 diabetes populations. Sci data 5: 180075. confocal microscopy. BioMed Res Int 2016:
helpful in the diagnosis, monitoring M€uller LJ, Vrensen GF, Pels L, Cardozo BN 7092938.
and progression assessment of KC & Willekens B (1997): Architecture of Teng CC (1963): Electron microscope study of
when the established topographic diag- human corneal nerves. Invest Ophthalmol the pathology of keratoconus. Am J Oph-
Vis Sci 5: 985–994. thalmol 55: 18–47.
nostics reach their limits as in topo-
Niederer RL, Perumal D, Sherwin T &
graphically inconspicuous partner eyes McGhee CNJ (2008): Laser scanning
of advanced KC patients, when doubts in vivo confocal microscopy reveals reduced
about progression do exist or even in Received on November 3rd, 2019.
innervation and reduction in cell density in
Accepted on March 16th, 2020.
advanced KC, when measurement all layers of the keratoconic cornea. Invest
inaccuracies occur. Ophthalmol Vis Sci 7: 2964–2970.
Correspondence:
Oliveira-Soto L & Efron N (2003): Morphol-
Elias Flockerzi MD
ogy of corneal nerves in soft contact lens
Department of Ophthalmology
wear. A comparative study using confocal
Saarland University Medical Center
References microscopy. Ophthalmic Physiol Opt 2: 163–
66421 Homburg
174.
Germany
Allgeier S, Winter K, Bretthauer G, Guthoff Pahuja NK, Shetty R, Nuijts RM, Agrawal A,
Tel: +49-6841-16-22302
RF, Peschel S, Reichert KM, Stachs O & Ghosh A, Jayadev C & Nagaraja H (2016):
Fax: +49-6841-16-22479
K€ ohler B (2017): A novel approach to An in vivo confocal microscopic study of
Email: elias.flockerzi@uks.eu
analyze the progression of measured corneal corneal nerve morphology in unilateral ker-
sub-basal nerve fiber length in continuously atoconus. BioMed Res Int 2016: 1–5. Loay Daas and Berthold Seitz declare that they do
expanding mosaic images. Curr Eye Res 42: Parissi M, Karanis G, Randjelovic S, Ger- not have any financial disclosures. Elias Flockerzi
549–556. mundsson J, Poletti E, Ruggeri A, Utheim has received a travel grant to the Second and Third
Belin MW & Duncan JK (2016): Keratoconus: TP & Lagali N (2013): Standardized baseline Ophthalmology Cystinosis Forum (Orphan Europe,
the ABCD grading system. Klin Monbl human corneal subbasal nerve density for Ulm, Germany) and an invitation to a seminar on
Augenheilkd 6: 701–707. clinical investigations with laser-scanning presentation training organized by the Santen
Bitirgen G, Ozkagnici A, Malik RA & Oltulu in vivo confocal microscopy. Invest Oph- GmbH (Munich, Germany). All authors con-
R (2013): Evaluation of contact lens-induced thalmol Vis Sci 10: 7091–7102. tributed to this work by providing data, revising
changes in keratoconic corneas using in vivo Parissi M, Randjelovic S, Poletti E et al. the manuscript, approving it for publication and
confocal microscopy. Invest Ophthalmol Vis (2016): Corneal nerve regeneration after agreeing to take full responsibility for all aspects of
Sci 8: 5385–5391. collagen cross-linking treatment of this work.
5You can also read