Mrs Anne Cushen Senior Specialist Childrens Allergy Dietitian Leeds Teaching Hospitals NHS Trust - 6th December 2019
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Mrs Anne Cushen
Senior Specialist Childrens Allergy Dietitian
Leeds Teaching Hospitals NHS Trust
6th December 2019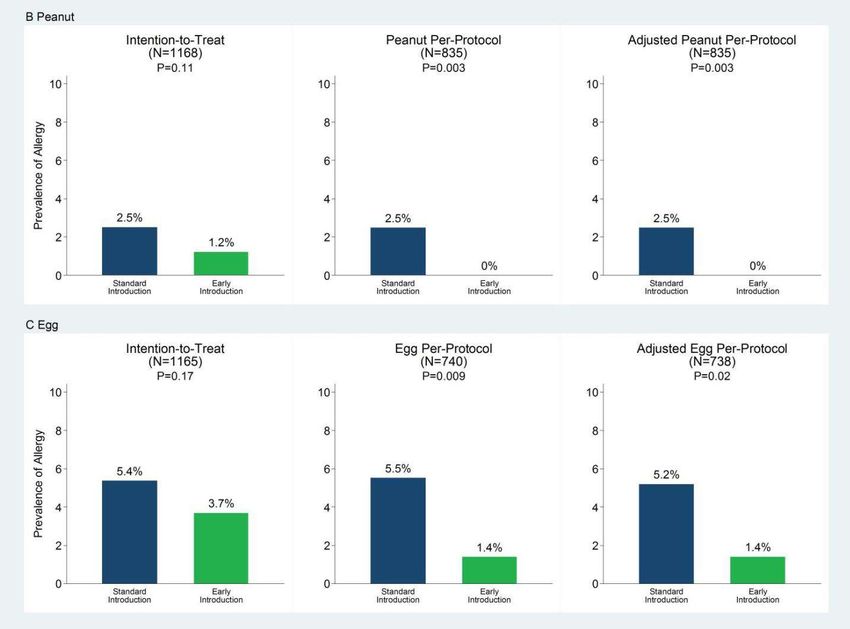
% of children diagnosed with allergic rhinitis and
eczema: trebled over last 30 years (Gupta R, 2007)
Peanut allergy among children in Western countries
has doubled in the past 10 years (Du Toit, 2015)
1:50 UK children now have peanut allergy
Children less likely to grow out of their allergies
than previous generations
Prescot, S, Allen K. (2011), Food Allergy: Riding the second wave of the allergy epidemic Pediatric
Allergy and Immunology 22: 155-160.
Allergy UK website: Allergy Prevalence: Useful facts and figures
Many theories including:
Breast-feeding rates
Weaning Age
Avoidance of Allergenic Foods
Poor food choices
Non Food: Hygiene hypothesis; antibiotic use, paracetamol
use in children, caesarean section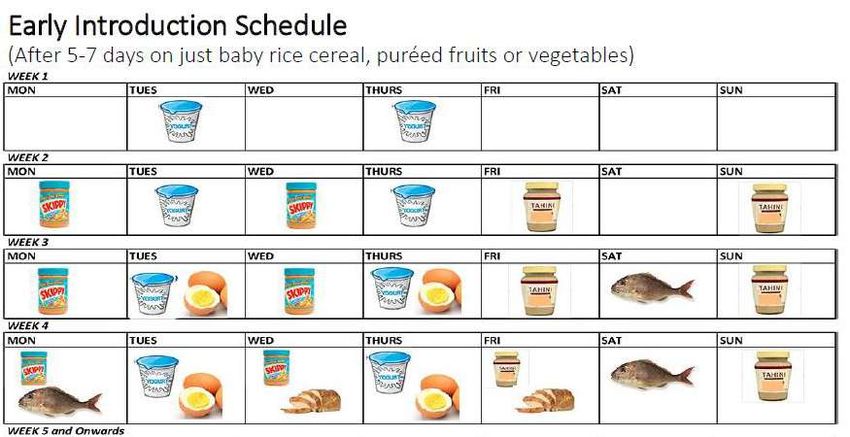
Part 1:
Pregnancy
Part 2:
Breast-feeding and Formulas
Part 3:
Weaning
Pregnancy
Maternal allergy is the stronger determinant of allergic infant
allergy than paternal allergy
Suggests that allergy may be determined by direct effects in
utero
Some evidence that women with allergy have a different
response to the foetus during pregnancy c/w non-allergic
women)
No need for mum to avoid any allergenic foods (unless she is
allergic) – avoidance has not been shown to prevent allergies
and may cause nutritional deficiencies
Prescot, S, Allen K. (2011), Food Allergy: Riding the second wave of the
allergy epidemic Pediatric Allergy and Immunology 22: 155-160.
EAACI Food Allergy and Anaphylaxis Guidelies. Primary Prevention of Food
Allergy. Position Paper (2014)
Up to 3 serves of oily fish per week: some evidence that
omega-3 fatty acids during pregnancy and breastfeeding may
help prevent eczema in early life
Due to high levels dioxins and PCBs (polychlorinated
biphenyls): 1-2 portions per week of oily fish for pregnant
women (SACN/COT (2004)
Supplements: may have a beneficial effect on atopy – higher
doses have more dramatic effects. No current dosage advice.
EAACI Food Allergy and Anaphylaxis Guidelies. Primary Prevention of Food Allergy. Position Paper (2014)
Ascia Guidelines 2016: Infant feeding and allergy prevention. : www.allergy.org.au Accessed Sept 2019
Proceedings of the Nutrition Society (2010) 69, 357-365. 3rd international Immunonutrition Workshop.
Session 5: Early Programming of the immune system and the role of nutrition immunology of pregnancy
Vitamin D: Important immunomodulatory role
Deficiency associated with atopic dermatitis, recurrent wheeze
and rise in food allergy
Vit D Deficiency in developmentally critical period increases
risk of intestinal colonisation of abnormal gut bacteria (affects
intestinal barrier and allows more exposure to allergens
Supplementation: conflicting results in allergy prevention
WAO: Currently no convincing evidence to supplement
routinely but do need to correct and prevent deficiency
WAO (2016). Guidelines for Allergic Disease Prevention: Vitamin D
FoodMu Per 100g (g) Portion size (g) Per Portion Food (mcg)
All Bran (Kelloggs) 1.6 40 0.6
Cornflakes (kelloggs) 2.6 30 0.8
Hens Egg 1.8 57 1.0
Mackerel 8.8 100 8.8
Margarine 7.9 10 0.8
Mushrooms 1.0 50 0.5
➢ Difficult to get enough from diet
➢ Sunshine main source
➢ Current Guidance: 10mcg per day
Manual of Dietetic Practice 2019
Cardwell et al (2018) A Review of Mushrooms as a Potential Source of Dietary Vitamin D
Nutrients. 2018 Oct; 10(10): 1498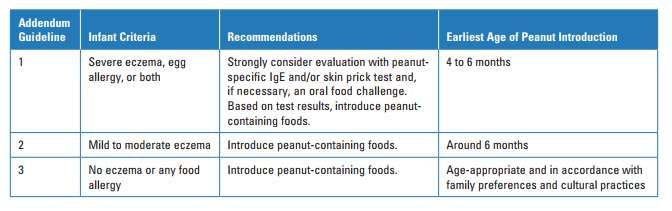
Low Maternal Zn intake associated with wheezing until 2 years of age
and asthma at 5 years of age
Low vitamin E: increased likelihood of wheezing until 5 years of age
Folate supplementation: Reduces risk of NTD in children but may
increase risk of asthma, wheezing and respiratory disease (animal study)
Unmetabolised Folic acid levels higher in children with allergy, Folate
levels lower (supplementation or genetic differences?) (Boston Birth
Cohort Study: 1349 children)
More research needed: Should mothers consume folate via F+V, lentils
and beans, rather than supplement form.
Proceedings of the Nutrition Society (2010) 69, 357-365. 3rd international
Immunonutrition Workshop. Session 5: Early Programming of the immune system
and the role of nutrition immunology of pregnancy
https://www.aaaai.org/about-aaaai/newsroom/news-releases/folic-acid Low Grade Evidence: probiotics during pregnancy and
breastfeeding may help prevent eczema in early life (WA0,
2015)
Recommendations cannot currently be made: The optimal
species and dose is unclear. More research needed before
specific recommendations can be made. (EAACI)
WAO (2015). Guidelines for Allergic Disease Prevention
EAACI Food Allergy and Anaphylaxis Guidelies. Primary Prevention of Food Allergy.
Position Paper (2014)Breast-feeding and
Formulas Relationship between breast-feeding and allergy – controversial
(evidence: observational studies, can’t randomise – ethics)
Breastfeeding is recommended for the many benefits it provides to
mother and infant (reduced infectious disease and severity)
Evidence: Protective against wheezing in earlier life and prevention of
upper and lower respiratory tract infections and may reduce asthma risk
Breastfeeding during the period that solid foods are first introduced to
infants from around 6 months may help reduce the risk of the infant
developing allergies, (although evidence low)
EAACI Food Allergy and Anaphylaxis Guidelies. Primary Prevention of Food Allergy. Position Paper (2014)
Matheson et al (2012): Understanding the evidence for and against the role of breast-feeding in allergy
prevention. Clinical and Experiemental allergy. 42: 827-851
ASCIA Guidelines: Infant Feeding and Allergy Prevention Approximately 200 different human milk oligosaccharides known.
Abundant in human milk
Composition of HMOs in breast milk is individual to each mother
and varies over the period of lactation
HMOs are mainly indigestible for the newborn child: Prebiotic
effect i.e. provide food for intestinal bacteria, esp. Bifidobacteria
A small fraction of HMOs absorbed
HMOs can bind to cell surface receptors expressed on epithelial
cells and cells of the immune system and thus modulate neonatal
immunity in the infant gut, and possibly other sites throughout the
body.
Also block attachment of various microbial pathogens to cells.
Triantis V, Bode L, van Neerven RJJ (2018) Immunological Effects of Human Milk
Oligosaccharides. Frontiers in Pediatrics. 6:190 Can be difficult initially
Top ups (formula) given during initial few days with ordinary
formula increase in milk allergy
If breast-feeding insufficient or not possible, high risk infants
should receive hypoallergenic formula until 4 months (some
evidence)
After 4 months: Standard formula
Primary Prevention of Cow's Milk Sensitization and Food Allergy by Avoiding Supplementation With Cow's Milk Formula at Birth: A
Randomized Clinical Trial. Urashima M1,2, Mezawa H1,2, Okuyama M1,2, Urashima T2, Hirano D2, Gocho N2, Tachimoto H2. JAMA
Pediatr. 2019 Oct 21. doi: 10.1001/jamapediatrics.2019.3544.
EAACI Food Allergy and Anaphylaxis Guidelies. Primary Prevention of Food Allergy. Position Paper (2014) No maternal Elimination diet recommended
Low maternal vitamin C alongside high intake of saturated
fats during breast-feeding may increase risk of allergies
Higher conc. Vit C in breast milk of atopic mothers assoc. with
reduced risk eczema and sensitisation at 12 months
Dietary intake improves concentrations better than
supplements
Therefore encourage healthy eating – plenty F+V!
Manual of Dietetic Practice sixth Ed. 2019 “SMA H.A.® “Babies who have a family history of allergy (for example a
parent or a sibling with allergy) are specifically at risk of developing
an allergic response to the protein in cows’ milk. Most infant milks
contain long chains of cows’ milk proteins. In SMA H.A.® Infant Milk
these proteins have been broken up into smaller pieces, which reduce
the risk of your baby developing an allergic response.”
Evidence: no consistent evidence that partially or extensively
hydrolysed formulas reduce risk of allergic or autoimmune
outcomes in infants at high pre-existing risk of these
outcomes.
Boyle et al (2016) Hydrolysed formula and risk of allergic or autoimmune disease:
systematic review and meta-analysis BMJ; 352 doi: https://doi.org/10.1136/bmj.i974
Crawley et al (2018) Specialised Infant Milks in the UK: Infants 0-6 Months. Information
for health professionals. October 2018.
Ascia Guidelines 2016: Infant feeding and allergy prevention. : www.allergy.org.au
Accessed Sept 2019 ”There is no evidence that soy or goat’s milk formula reduce
the risk of allergic disease when used in preference to
standard cow’s milk based formula.
Consider if formula really needed
May be a benefit to EHF but not Partially hydrolysed.
Ascia Guidelines 2016: Infant feeding and allergy
prevention. : www.allergy.org.au Accessed Sept 2019Weaning
1. When to wean 2. How to wean 3. What to wean
Current UK guidelines for introducing solid foods
◦ At around 6 months of age (WHO)
◦ When baby developmentally ready, not after 6 mo.
not before 17 weeks (4 months) (BDA)
◦ Individual variations
◦ Alongside continued breastfeeding
Not before 6 months:
◦ cow‘s milk, eggs (well-cooked), wheat and
gluten, nuts, peanuts, seeds, fish and shellfish:
◦ introduce them one at a time (DoH)
Start4Life: https://www.nhs.uk/start4life/baby/first-foods
The British Dietetic Association. Complementary feeding: introduction
of solid food to an infant’s diet. April 2013 ‘The introduction of complementary food into the diet of
healthy term infants in the EU between the age of 4 and 6
months is safe and does not pose a risk for adverse health
effects (both in the short-term, including infections and
retarded or excessive weight gain, and possible long-term
effects such as allergy and obesity).” (European Food Safety
Authority, 2009)
No need to avoid any allergenic foods past 6 months
And......early introduction beneficial…..?
Scientific Opinion on the appropriate age for introduction of complementary
feeding of infants 2009 EFSA Journal (2009) 7(12): 1423 [19 pp.].
http://www.efsa.europa.eu/en/efsajournal/pub/1423.htmPrevalence of Peanut
Allergy in Children
4 - 18 years
Peanut Protein Consumption
8 - 14 months
Du Toit G, et al. Early Consumption of Peanut in
Infancy is Associated with Low Prevalence of Peanut
Allergy. JACI 2008; 122: 984-91.Intervention group; SPT Positive (n=47) Peanut protein
n=319
6g/week
Intervention group; SPT Negative (n=272) (2g x 3)
until 60m
Recruitment:
2006-------------2009
2009
2014
--------------------------------------------------
Control group; SPT Positive (n=51)
n = 640 infants with 0g/week
severe eczema and / or until 60m
egg allergy n=319
Control group; SPT Negative (n=270)
Infants at high risk of peanut allergy!
Age at clinic visits: 4-11 months 12 months 30 months 60 months
Du Toit, G et al (2015), Randomized Trial of Peanut Consumption in Infants at Risk for Peanut Allergy. The New England
Journal of Medicine. Vol 372. No 9: 803-813 92% adherence to protocol
Peanut introduced between 4-11months
Mean and Median age to enter trial: 7.8 months
◦ Most children were > 6 months oldAfter one year peanut avoidance, previous consumers still displayed
significantly lower prevalence of peanut allergy
81% Relative Reduction 74% Relative Reduction 89% Relative Reduction
Du Toit et al, (2016) Effect of Avoidance on Peanut Allergy after Early
Peanut Consumption. N Engl J Med; 374:1435-1443 Earlier introduction of peanuts (4-11 m) significantly decreased the
risk of peanut allergy among children at high risk
This protective effect continued after a 12 month peanut avoidance
2g peanut protein 3 times/week is safe and acceptable for most
children
◦ had no negative impact on growth, nutritional intake or breastfeeding
duration
Can these findings be applied to the general population and to
other common allergenic foods?
◦ The EAT (Enquiring About Tolerance) Study was designed 1300 infants in the UK
Breastfed
◦ Exclusively from birth to 3 months (enrolment)
◦ Ongoing during intro of solids
Intervention group
◦ 6 potentially allergenic foods
◦ cows milk, egg, peanut, sesame, fish, wheat
◦ introduced into diets by 4 months of age
Control group
◦ standard UK government advice
Main outcome
◦ challenge proven diagnosis of allergy to one or more of the foods at 1 year and 3
years of age http://www.eatstudy.co.uk/
Perkins et al (2016) Randomized Trial of Introduction of Allergenic Foods
in Breast-Fed Infants. N Engl J Med 2016; 374:1733-1743Only 42& adherence Only 42% adherence to protocol (75% of required amount eaten)
Intention-to-Treat Per-Protocol Adjusted Per-Protocol
(N=1162) (N=732) (N=727)
P=0.32 P=0.01 P=0.03
8 7.3%
7.1%
7 6.4%
Prevalence of Allergy
6 5.6%
Standard
5 Introduction
4 Early Introduction
3 2.4% 2.4%
2
1
0
ITT – 20% Non-significant reduction in prevalence in EIG
PP – 67% Significant reduction in prevalence in EIGPP - 100% Significant reduction in Peanut allergy prevalence with 3g protein consumption/week PP - 75% Significant reduction in Egg allergy prevalence with 3g cooked egg protein consumption/week
https://www.niaid.nih.gov/sites/default/files/peanut-allergy-prevention- guidelines-clinician-summary.pdf
Choose British Lion stamped eggs Offer scrambled, omelette, soft or hard boiled Can mash into other foods e.g. pureed fruit/veg/baby cereals Aim for at least one per week
Smooth peanut butter, bamba snacks or grind whole peanuts
to a fine powder
Mix with pureed fruit/veg/porridge/baby cereals
Aim for two level teaspoons of peanut butter per week
Recipe: Mix one teaspoon of smooth peanut butter with 1 tbs
of warm water (boiled), or formula or pureed fruit and veg. www.readysetfood.com
“Give your child an allergy free future”
“Babies are picky eaters, and getting them to eat peanut, egg,
and milk several times a week can be very difficult.”
“50% of the parents in the studies weren't able to sustain
exposure! That's why we designed our packets to easily fit
into your baby's daily feeding routine.”
Recommend for at least 6/12
Does it work? Quote 3 studies: LEAP, EAT and PETIT
Are they necessary? £££ Gut bacteria feed on fibre
◦ Produce butyrate
◦ Influences the immune system and plays a role in allergy
development
Encourage fruit, vegetables, legumes, a variety of
wholegrains
◦ Avoid only/excessive amounts wholegrains
◦ Avoid added bran
◦ May need to limit fibre in some
children
Roduit et al (2014). Increased food diversity in the first year of life is inversely associated
with allergic diseasesJ Allergy Clin Immunol. 2014 Apr;133(4):1056-64. doi:
10.1016/j.jaci.2013.12.1044. Epub 2014 Feb 6.Food Fibre per 100g Portion Size (g) Fibre per portion (g)
Banana 1.3 40 0.5
Broccoli 2.8 40 1.1
Carrots 3.5 40 1.4
Houmous 2.4 40? 1.0
Lentils (boiled) 3.8 40 1.5
Peas 5.8 40 2.3
Pears (with skin) 2.2 40 0.9
Raspberries 2.5 40 1.0
Red kidney beans 7.5 40 3.0
Strawberries 3.8 40 1.5
Fibre recommendation for 1.5 years to 3 years: 15g per day General advice
◦ Start with pureed vegetables (Home-cooked (K. Grimshaw) et al. 2014)
◦ Start with small quantities (1-2 tsp), increase dose daily
◦ One new food at a time initially (all food introductions cumulative)
◦ Can mix foods with EBM or formula
No particular order in which to continue but from 6 months iron containing foods need to be included :
• Meat, e.g. lamb, pork, beef
• Poultry, e.g. chicken, turkey
• Fish, e.g. cod, haddock, salmon, tuna
• Legumes, e.g. beans, chick peas, lentils, peas
• Give parents confidence/reassurance to
enjoy weaning ☺
K. Grimshaw et al. (2014) Diet and food allergy development during infancy;
Birth cohort study findings using prospective food diary data.
Journal of Allergy and Clinical Immunology 133:511-519 · No need to avoid foods in pregnancy or during breast-
feeding– aim for a healthy diet with plenty of F+V
Breast-feeding should be encouraged and to continue
throughout weaning
Consider whether formula top ups are really
necessary/possibly use extensively hydrolysed??
Weaning should start between 4 and 6 months and
include introduction of peanut and egg
Weaning diet quality is important: fresh; fibre; prebiotics;
avoid commercial weaning products as much as possible.Any Questions?
You can also read