National Partnership to Improve Dementia Care in Nursing Homes & Quality Assurance and Performance Improvement (QAPI) - June 15, 2017
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
National Partnership to Improve
Dementia Care in Nursing Homes &
Quality Assurance and Performance
Improvement (QAPI)
June 15, 2017
Disclaimer
This presentation was current at the time it was published or
uploaded onto the web. Medicare policy changes frequently so
links to the source documents have been provided within the
document for your reference.
This presentation was prepared as a service to the public and is
not intended to grant rights or impose obligations. This
presentation may contain references or links to statutes,
regulations, or other policy materials. The information provided
is only intended to be a general summary. It is not intended to
take the place of either the written law or regulations. We
encourage readers to review the specific statutes, regulations,
and other interpretive materials for a full and accurate statement
of their contents.
2
Agenda
Appropriate Assessment and Dr. Susan Levy, Medical
Evaluation for the Accurate Director/Consultant
Diagnosis of Schizophrenia
and Other Mental Disorders
National Nursing Home Quality Kaylie Doyle, Telligen
Care Collaborative Kelly O’Neill, Stratis Health
National Partnership & QAPI Michele Laughman, CMS
Updates Debbie Lyons, CMS
3
Welcome
4Appropriate Assessment and Evaluation for
the Accurate Diagnosis of Schizophrenia and
Other Mental Disorders
Susan M. Levy, MD, CMD
5Susan M. Levy, MD, CMD: Disclosure
Current Immediate Past President AMDA: The
Society for Post-Acute and Long Term Care
Medicine
Facility Medical Director, Sussex County, DE
Chief Medical Officer, Linked Senior
Health Quality Innovators, Consultant
6CMS Quality Measures and Federal
Requirements
Five Star Antipsychotic Medication Quality Measures
• Short-stay nursing home residents
• Long-stay nursing home residents
Federal Long-term Care (LTC) Requirements and
Interpretive Guidelines
• 483.45 Unnecessary Drugs
• F329
7Antipsychotic Medication Quality Measure:
Long-stay Residents
Numerator:
Long-stay residents with a selected target assessment where
the following condition is true: antipsychotic medications
received. This condition is defined as follows:
• For assessments with target dates on or before
03/31/2012: N0400A = [1]
• For assessments with target dates on or after
04/01/2012:N0410A=[1,2,3,4,5,6,7]
Denominator:
All long-stay residents with a selected target assessment,
except those with exclusions
8Antipsychotic Medication Quality Measure:
Long-stay Residents
Exclusions:
2.0 Any of the following related conditions are present
on the target assessment (unless otherwise
indicated):
2.1. Schizophrenia (I6000 = [1])
ϮϬϮϬ ϸ͉̠̑β̮̮βϯ̤ ϲ͛̊ή̠̑̉β ̒Iϱϯϱ = ̔ϭ])
ϮϬϯϬ ϸ͉̠̑β̮̮βϯ̤ ϲ͛̊ή̠̑̉β ̒Iϱϯϱ = ̔ϭ̓̕ ̑̊ ̮Ϯβ ̝̠ϱ̠̑
assessment if this item is not active on the target
assessment and if a prior assessment is available
ϮϬϰϬ H͉̮̊ϱ̊Ϥ̮̑̊ϯ̤ Dϱ̤βΖ̤β ̒IϱϮϱ = ̔ϭ])
9Diagnosing Nursing Home Residents with
Schizophrenia
• Incorrect interpretation of the federal
requirements and interpretative guidelines
To improve dementia care and decrease
antipsychotic medication use
• Failure to follow the care process:
Recognition
Assessment
Then Diagnosis
Monitoring
10Joint Summary Statement - Diagnosing
Schizophrenia in Nursing Homes
• Concerns were raised that diagnosis of
ϲΤϮϱ̝̑͠Ϯ̠β̊ϱΖ ͕Ζ̤ Σβϱ̊Ϥ ̉Ζήβ ̮̑ ϳϽ͉̤̮ϱμ͛ϳ ̮Ϯβ ͉̤β
of antipsychotic medications.
• American Health Care Association convened
stakeholder organizations and after discussion a
joint summary statement was developed and
approved.
http://www.paltc.org/newsroom/joint-summary-statement
diagnosing-schizophrenia-skilled-nursing-centers
11Joint Summary - Supporting Organizations
American Association for Geriatric Psychiatry
American Association of Nurse Practitioners
American Geriatrics Society
American Health Care Association
AMDA ̈ The Society for Post-Acute and Long-Term Care
Medicine
American Psychiatric Association
American Society of Consultant Pharmacists
Gerontological Advanced Practice Nurses Association
Leading Age
Society of Hospital Medicine
12Joint Summary Statement
• The development of schizophrenia is uncommon
in older adults.
A diagnosis of new onset schizophrenia in a post-
acute and long-term care setting should be made by
a qualified health professional, with mental health
training, using DSM-5 criteria.
• The diagnosis should be made only after
underlying causes of the symptoms have been
excluded through a careful review process.
13Joint Summary Statement (cont.)
• Clinicians need to be mindful of and avoid
labeling patients with diagnoses to justify the use
of medications or other treatments.
• It is important to acknowledge that some patients
with dementia may benefit from treatment with
psychotropic medications if they are clinically
indicated and non-pharmacological approaches to
care have been ineffective or are contraindicated.
14Primary Mental Health and Substance Use
Disorders
• Bipolar
• Major depression with psychosis
• Schizophrenia
• Schizoaffective disorder
• Brief psychotic disorder
• Drug abuse/intoxication
• Drug withdrawal (alcohol/opioids/other)
15General Medical Conditions (secondary)
• Neurologic Disorders:
Dementia ̒ϱϬβϬ !̃͠Ϯβϱ̉β̠ϯ̤
Dϱ̤βΖ̤β̀H͉̮̊ϱ̊Ϥ̮̑̊ϯ̤̀Lβ͕͛ body dementia)
Stroke
Brain tumor
Acute and chronic infections
16General Medical Conditions (cont.)
• Nutritional Deficiencies:
B 12
Pellagra
Wernicke-K̠̤̑Ζ̀̑μμϯ̤ encephalopathy
• Systemic illnesses
• Adverse drug effects
• Delirium
17A Guide to the Management of Psychotic Disorders and Neuropsychiatric Symptoms
of Dementia in Older Adults
From the American Geriatrics Society
18Primary Mental Health Disorders and Psychosis
Schizophrenia is a major mental health disorder that has
specific diagnostic criteria outlined in the DSM-5.
• Key criteria are the presence of psychotic symptoms,
hallucinations, and delusions.
• Other major mental health disorders may also have psychotic
symptoms, such as bipolar disorder, schizoaffective disorder,
and delusional disorder.
• Psychotic symptoms can also occur in the course of other
medical illnesses, including dementia and delirium.
• Residents with long standing mental health disorders can
also develop dementia as they age and have associated
symptoms related to dementia, that are superimposed on
their chronic mental health condition.
19Overlap of Psychotic Disorders
Primary
Mental Health
Disorder
Dementia Delirium
20Nursing Home Residents and Primary Mental
Health Disorders
• Typically admitted at a younger age than residents
without major mental health disorder.
• Maybe stable on long-term medication
management, but when additional medical
problems develop may exacerbate.
• Diagnosis may not be clear from preceding
hospital stay and may not be included, or may be
Ζ̊ ϱ̊ΖΤΤ͉̠Ζ̮β ϲ̃ΖΣβ̃ϳ ϱμ ̮̊̑ ̠β̃Ζ̮βή ̮̑ ̮Ϯβ ̠βΖ̤̑̊
for admission.
21New Diagnosis of Primary Mental Health
Disorder
ϲNβ͕ϳ ̠̑ Ζήήβή ήϱΖϤ̤̊̑ϱ̤ ̉Ζ͛ ̑ΤΤ͉̠ ϱ̊ ͉̠̤̊ϱ̊Ϥ
homes when:
• Initial psychosocial assessment reveals missed
information.
• Escalation of symptoms as part of the course of illness
leads to identifying prior history.
N̮̑βϫ ϲNβ͕ϳ diagnosis, late in life without prior symptoms
is unlikely.
22Evaluation of a Schizophrenia Diagnosis
• Review old records from the hospital, community
mental health center, primary care, or outpatient
psychiatry;
• Look for prior psychiatric diagnostic evaluations,
hospitalizations, and prior psychiatric treatment,
including antipsychotic medication use and the
use of other psychotropics.
23Evaluation of a Schizophrenia Diagnosis (cont.)
If there is no history of psychiatric treatment, and the
first symptoms or deterioration occur when the
resident is in a nursing home, it is more likely the
onset of a Minor or Major Neurocognitive Disorder
(Dementia), rather than a Psychotic Disorder, such as
schizophrenia.
24Elements of a thorough Diagnostic Evaluation:
• History from record review, facility staff, resident,
family, and/or resident representative
• Medical evaluation, including physical exam and
laboratory assessment, and psychiatric evaluation
from mental health professional
25Evaluation of the Treatment Process after
Diagnosis:
• Discussion about the diagnosis, including advance
care planning
• Discussion about treatment options, including
informed consent if an antipsychotic medication is
started
• Close monitoring of beneficial and/or adverse
effects after the start of any psychotropic
medication
• Reassessment of need to continue medication
26Better Approach to Behavioral Health in
Nursing Homes
• Behavioral health rounds/meeting
• Medical/Behavioral co-management
• Who manages the diagnosis list?
• Who manages psychotropic medications?
• Role of the Consultant Pharmacist
• Discussion of psychotropic medication usage in
QAA meetings
27Support for Behavioral Health Needs
Medical Director
Attending/Nurse
Mental Health
Practitioner/
Practitioners
Physician
Assistant
28National Nursing Home Quality Care
Collaborative (NNHQCC)
Aligned with other national nursing home quality initiatives, led by Quality Innovation
Network-Quality Improvement Organizations (QIN-QIOs),
79% of nursing homes participating
Kaylie Doyle, MBA, Telligen
Kβ̃̃͛ OϯNβϱ̃̃ϩ RNϩ ϲNϩ MP!ϩ Stratis Health
QIN National Coordinating Center (NCC)
29Questions We are Hearing
• What are the nursing home focus areas of QIOs?
• What is the NNHQCC?
• How does the QIN-QIO work support and align with the
National Partnership for Dementia Care and QAPI?
• What tools and resources are available to nursing
homes, partners, and other interested persons?
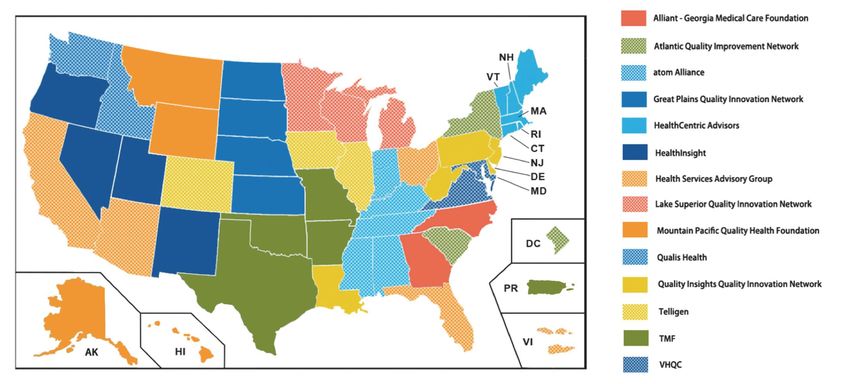
30QIN NCC
• The QIN NCC supports a national network of 14 QIN-
QIOs as they implement the national quality initiatives
of the QIO Program.
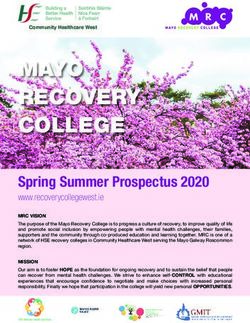
31QIN-QIOs
32QIN-QIOs work with Nursing Homes:
Alignment with National Initiatives
• Work with nursing homes to improve quality of
resident-centered care and safety.
• NNHQCC
Support recruited nursing homes:
◦ In using QAPI as a framework to achieve system wide improvement
◦ In reducing inappropriate use of antipsychotics
◦ In implementing antibiotic stewardship and preventing and managing
Clostridium difficile infections (CDI)
Use Quality Measure Composite Score to monitor progress.
33QIN-QIOs work with Nursing Homes:
Alignment with National Initiatives
• QIN-QIOs are sharing information and resources with
nursing homes to guide successful implementation of
NNHQCC and the regulation.
Focusing on QAPI methods and techniques ̈ to improve
systems and processes and meet the intent of the regulation.
• QIN-QIOs are aligning efforts with partners,
To provide support and education for nursing homes, and to
promote and share consistent messages.
34NNHQCC: CDI Cohort
• Utilizing the QIN-QIO led Collaborative, the CDI Cohort
will:
Increase the number of nursing homes that are consistently
reporting data into the Centers for Disease Control and
Prevention (CDC) National Healthcare Safety Network (NHSN)
database.
Establish a QIN-QIO-derived national Nursing Home CDI
baseline.
Improve quality of care outcomes for nursing home residents
through tracking CDIs, implementing antibiotic stewardship,
and effectively preventing and managing CDIs.
35Progress to Date – Recruitment
• As of March 2017 ̈ 12,217 nursing homes are
recruited to participate in the NNHQCC.
79% of the nation’s nursing homes
• Of the 12,217 ̈ 2,630 one-star nursing homes are
recruited to participate in the NNHQCC.
• As of April 10, 2017 ̈ 2,341 nursing homes are enrolled
ϱ̊ ̮Ϯβ Dϯ̤ NHϲN ήΖ̮ΖΣΖ̤βϬ
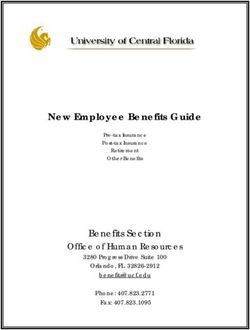
36Progress to Date – Nursing Home Quality
Measure Composite Score
Data based on rolling six-month QIES data.
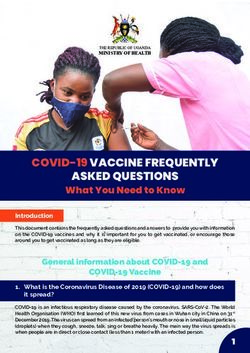
37Progress to Date – Antipsychotic Measure
August 2014:
18.73%
February 2017:
15.34%
Data based on rolling six-month QIES data.
38NNHQCC – Change Package
39Change Package Strategies
• Lead with a sense of purpose.
• Recruit and retain quality staff.
• Connect with residents in a celebration of their lives.
• Nourish teamwork and communication.
• Be a continuous learning organization.
• Provide exceptional compassionate clinical care that
treats the whole person.
• Construct solid business practices that support your
purpose.
40Change Package
• Success story template
• Bundles
Avoidance of Unnecessary Antipsychotic Medications in
Nursing Home Residents Living with Dementia
Encourage Nursing Home Rβ̤ϱήβ̮̤̊ϯ M̑Σϱ̃ϱ̮͛
Prevent Healthcare Acquired Infections
Prevent CDIs in Nursing Home Residents
QAPI
41Resources
http://qioprogram.org/nursing-home-training-sessions
42Topics Covered in the Online Training Sessions
• TeamSTEPPS® in LTC: Communication Strategies to
Promote Quality and Safety
• Exploring Antibiotics and their Role in Fighting Bacterial
Infections
• Antibiotic Resistance: How it Happens and Strategies to
Decrease the Spread of Resistance
• Antibiotic Stewardship
• Clostridium Difficile (C. Difficile) Part One: Clinical
Overview
• C. Difficile Part Two: Strategies to Prevent, Track, and
Monitor C. Difficile
43Purpose of the Online Training Sessions
• To provide nursing home leaders with a set of training
materials that they can use to enhance understanding
of important concepts and practices that promote
stewardship and C. difficile prevention, and to provide
information, tools, and resources to take action to
improve practices.
• To develop and disseminate materials that can be
accessed and used by LTC partners and stakeholders
interested in these topics.
44Use of the Online Training Sessions
• Nursing home leaders can decide:
Which components would be helpful for themselves and
which to include in educating other staff.
The appropriate staff to include for different components.
How to use the materials during education sessions or self
study.
How to customize the content to work for their audience; all
content is optional and may be adapted.
How to best provide this training over time; the intent is not
to review this content all at once.
45Each Online Training Session Includes
• Welcome and overview
• Objectives
• How you can use this session
• Orientation (list of sections and content)
• Topic information presented via text/narrative, video,
PowerPoint presentations with notes, or links to website
pages
• Interactive activities and scenarios, including discussion
questions
• Informational handouts
• Take home messages
• Links to additional optional resources
• Opportunity to apply for a certificate of participation or
nursing continuing education credits
46Thank You
• Kaylie Doyle, MBA, Telligen
Kaylie.Doyle@qinncc.hcqis.org
• Kelly OϯNβϱ̃̃ϩ RNϩ ϲNϩ MP!ϩ ϲ̮̠Ζ̮ϱ̤ Health
koneill@stratishealth.org
47National Partnership & QAPI Updates
Michele Laughman
Debbie Lyons
Centers for Medicare & Medicaid Services
48Question & Answer Session
49Acronyms in this Presentation
• CDC: Centers for Disease Control and Prevention
• CDI: Clostridium difficile infections
• C. Difficile: Clostridium difficile
• LTC: Long-term Care
• NCC: National Coordinating Center
• NHSN: CDC’s National Healthcare Safety Network
• NNHQCC: National Nursing Home Quality Care
Collaborative
• QAPI: Quality Assurance & Performance
Improvement
• QIN-QIO: Quality Innovation Network Quality
Improvement Organization
50Evaluate Your Experience
• Please help us continue to improve the MLN
Connects® National Provider Call Program by
providing your feedback about today’s call.
• To complete the evaluation, visit
http://npc.blhtech.com and select the title for
today’s call.
51Thank You
• For more information about the MLN Connects® National Provider Call
Program, visit https://www.cms.gov/Outreach-and
Education/Outreach/NPC/National-Provider-Calls-and-Events.html
• For more information about the Medicare Learning Network®, visit
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network
MLN/MLNGenInfo/Index.html
• For more information about the National Partnership to Improve Dementia Care
in Nursing Homes, please visit
http://www.cms.gov/Medicare/Provider-Enrollment
andCertification/SurveyCertificationGenInfo/National-Partnership-toImprove
Dementia-Care-in-Nursing-Homes.html or send inquiries to
dnh_behavioralhealth@cms.hhs.gov
The Medicare Learning Network® and MLN Connects® are registered trademarks of the U.S. Department of Health and Human Services (HHS).
52You can also read