Natural History of Trisomy 18 and Trisomy 13: 11. Psychomotor Development
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
American J o u r n a l of Medical Genetics 49:189-194 (1994)
Natural History of Trisomy 18 and Trisomy 13:
11. Psychomotor Development
Bonnie J. Baty, Lynn B. Jorde, Brent L. Blackburn, and John C. Carey
Division of Medical Genetics, Department of Pediatrics (B.J.B., B.L.B., J.C.C.), and Department of Human Genetics
(LB.J.j, University of Utah School of Medicine, Salt Lake City, Utah
Developmental data were abstracted from KEY WORDS: trisomy 18, trisomy 13, chro-
medical records on 50 trisomy 18 individuals mosome 18, chromosome 13,
ranging in age from 1 to 232 months and 12 development
trisomy 13 individuals ranging in age from 1
to 130 months. Data on the age when trisomy
18 and trisomy 13 children achieved develop- INTRODUCTION
mental skills were collected from a larger
group of 62 trisomy 18 individuals and 14 tri- Little has been written regarding the developmental
somy 13 individuals whose families filled out assessment oftrisomy 18 and trisomy 13. Previous infor-
parent questionnaires. Developmental quo- mation comes mainly from individual case reports of
tient (DQ), defined as developmental age di- older individuals. A few of these case reports include
vided by chronological age, averaged 0.18 for some detailed information about developmental pro-
trisomy 18 and 0.25 for trisomy 13. There was a gress [Gerhard, 1976; Smith et al., 1978; Smith et al.,
dramatic drop in DQ from infancy to later 19891but most give sketchy information, if any. This is
childhood. The highest DQs and the greatest in large part due to the rarity of older individuals with
variation in DQs were in the first 2-3 years of full trisomies and the fact that any one practitioner is
life. Developmental ages in 7 skill areas were unlikely to see several older trisomy 18 or 13 children.
significantly different, with daily living and The parent support group offered an opportunity to
receptive language having the highest values study a series of surviving individuals. One recent pub-
and motor and communication skills having lication has reported on a series of older individuals,
the lowest. When chronological age was taken using the S.O.F.T. support group for identification of
into account, there was no significant differ- cases [Van Dyck and Allen, 19901.
ence in DQs in the same 7 skill areas, although
there was a trend that was similar to the pat- METHODS
tern of differences with developmental age. This study is part of a larger study of the natural
Older children could use a walker, under- history of trisomy 18 and trisomy 13. The initial part of
stand words and phrases, use a few words the study involved sending questionnaires to families
and/or signs, crawl, follow simple commands, registered with the Support Organization for Trisomy
recognize and interact with others, and play 18, 13, and Related Disorders, which is known as
independently. Walking and some toileting S.O.F.T. A total of 98 trisomy 18families and 32 trisomy
skills were also reported for trisomy 13. Al- 13 families with nonmosaic trisomy answered a 4-page
though individuals with trisomy 18 and tri- questionnaire, which included questions about demo-
somy 13 were clearly functioning in the severe graphics, birth data, growth, neonatal hospitalization(s)
to profound developmentally handicapped and operations, immunizations, psychomotor develop-
range, they did achieve some psychomotor ment, birth defects, medical complications, cause of
maturation and always continued to learn. death, and family history of other chromosome disor-
0 1994 Wiley-Liss, Inc. ders. Data concerning all aspects except development
have been reported in a separate publication [Baty et al.,
19941.Cytogenetjc confirmation was achieved for 97%of
trisomy 18 individuals and 97% of trisomy 13 individ-
uals. Ages at the time of the developmental assessment
Received for publication March 5,1993; revision received August ranged from 1 to 232 months (19 years, 4 months) for
16,1993. trisomy 18 and 1t o 130 months (10years, 10months) for
Address reprint requests to Bonnie Jeanne Baty, Department of trisomy 13. There were 41 trisomy 18 individuals (42%)
Pediatrics, University of Utah Medical Center, Salt Lake City, UT and 12 trisomy 13 individuals (38%)surviving to age 1
84112. year. The developmental questions consisted of a list of
0 1994 Wiley-Liss, Inc.190 Baty et al. developmental stages, and parents were asked the age or RESULTS date at which their child had achieved those stages. A total of 62 trisomy 18 families and 14 trisomy 13 fami- The psychomotor development reported by parents is lies provided information on psychomotor development. summarized in Table I. The table contains the mean, The second part of the study involved obtaining medi- standard error of the mean, range, number of individ- cal records from the same families that filled out the uals reporting each stage, and the normal age range parent questionnaires. The two groups did not com- [Frankenburg et al., 1976; Moyers et al., 19741 for each pletely overlap, because we could not obtain medical skill. records on some individuals whose parents supplied de- As is often the case with conditions associated with velopmental information, and we obtained medical re- mental retardation, the range of time in which a devel- cords on some individuals whose parents did not supply opmental level is achieved is wider than usual. Four of developmental information. The subset of individuals the trisomy 18 children and 1 trisomy 13 child were with developmental records all had confirmation of full reported to use a few consistent signs. Five trisomy 18 trisomy. If developmental testing had ever been done, children used a few consistent words. Many of the older records on the child's psychomotor development were children have a much more extensive receptive vocabul- requested. We obtained developmental records on 50 ary. Five of the trisomy 18 children walked with a individuals with trisomy 18 and 12 individuals with walker, and one trisomy 18 child and 2 trisomy 13 chil- trisomy 13. Of the individuals with developmental re- dren cruised around furniture. No individual with tri- cords, 29 with trisomy 18 and 8 with trisomy 13 were somy 18 was reported to walk, but one trisomy 13 child over the age of 1 year. walked at age 9. In addition to the child with trisomy 13 Data were abstracted from the developmental records reported, two of the authors have personally met an- and computerized using the Ingres database manage- other 13 year old with trisomy 13 who walks. ment program. Statistical analysis was performed using The remainder of the data reported was abstracted by the BMDP package. The information abstracted in- one of the authors (BJB)from the medical records. Table cluded chronological ages, developmental ages for spe- I1 shows the mean CA, mean DA, and mean DQ for cific skill areas on specific developmental tests, individ- various age groups, along with the standard error of the ual skills recorded by the developmental specialists mean for each. The number of observations in each evaluating the child, feeding skills, and IQs. Many chil- group and the number of children on which these obser- dren were evaluated at multiple ages using multiple vations were made are also reported. Figure 1 summa- tests, while some children had very few entries. There rizes the data on DQ in graphic form. For both condi- were 28 different developmental tests used. The most tions, mean DQs drop dramatically with age (one-way common (the Bayley Scales of Infant Development, the analysis of variance; P
Natural History of Trisomy 18 and 13: 11 191
TABLE 11. Mean ( t Standard Error) Chronological Ages, Developmental Ages, and Developmental Quotients
for Trisomy 18 and Trisomy 13
Chron age Dev age Number of Number of
Age (years) Trisomy (months) (months) DQ observations children
0-1 18 8.6 (20.6) 3.7 (k0.5) 0.42 ( t 0.04) 25 10
13 6.6 ( t 0.7) 3.3 (t 0. 5) 0.48 ( k 0.06) 11 3
1-3 18 25.2 ( t 0.8) 3.9 (t0.2) 0.17 (&0.01) 76 15
13 26.3 (kO.9) 7.7 (20.4) 0.31 ( k0.02) 53 5
3-5 18 46.8 ( k 1.2) 8.2 (t0.8) 0.18 (t0.02) 48 7
13 44.1 (irl.0) 7.3 ( k 0 . 5 ) 0.17 (tO.01) 26 5
>5 18 97.6 (24.4) 6.8 ( k 0.4) 0.08 (+0.01) 58 9
13 92.7 ( t 6 . 1 ) 13.3 ( k 1.9) 0.13 (20.01) 25 2
All ages 18 48.5 ( 2 2.6) 5.7 (&0.3) 0.18 (kO.01) 207 26
13 42.9 (k3.0) 8.4 ( k 0.5) 0.25 (20.01) 115 8
data. The highest individual DQs, as well as the great- ideally be a horizontal line at 1.0. The drop-off in the
est variation in DQs, clearly occur at the youngest ages. curve does not represent a loss of skills, but rather
There are many individual measurements above 0.5. greater distance from the normal curve. It is clear from
These higher DQs represent 6 different cases (4have the information derived from parent reports and from
trisomy 18 and 2 have trisomy 13).Three of the children these formal developmental assessments that these chil-
have only one measurement above 0.5, and 3 children dren generally continue to acquire new skills through-
have from 3 to 6 measurements above 0.5. The CAs of out their lives.
these high DQs range from 2 months t o 50 months. They An average DQ a t each CA for each child was also
represent several different tests and skill areas. Thus, plotted to determine whether multiple measurements
there seems to be no pattern of high DQ measurements, on the same child at the same age could bias the data. All
except that they are all at 50 months or below. The three plots (for trisomy 18, trisomy 13 and combined
measurements above 100 months represent 1trisomy 13 data) looked essentially the same. Once again, trisomy
child and 3 trisomy 18 children. The values for the tri- 13 appeared to have somewhat higher scores in the older
somy 13 child are higher than those of the trisomy 18 children.
children, but the numbers are too small to permit gener- Only two children had IQ scores recorded in their
alization. In general, there is a sharp “drop-off’in DQ, developmental records, both trisomy 18children with IQ
representing an increasing distance from the develop- scores of 20. The children were ages 5 and 12. We did not
mental curve of average normal children, which would find IQ scores useful, both because ofthe lack ofdata and
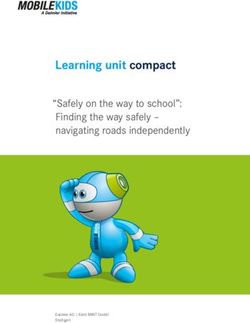
Developmental Quotient
0.5
0.4-
0.3 -
’
0.2 -
0.1 - ’
< 12 12-36 36-60
Age in Months
MTrisomy 18 HTrisomy 13
Fig. 1. Average developmental quotients a t different ages in trisomy 18 and trisomy 13.192 Batyet al.
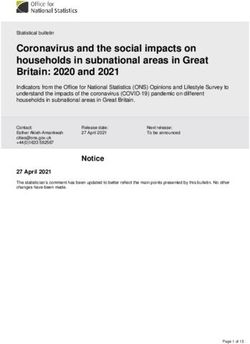
a Developmental Quotient
0.8
....
0.6 -
..
0.4
..
. ...
.. . . '
0.2
, , , c
..
0 I I . , I
0 50 100 150 200
Age in Months
Developmental Quotient
I[
0.61- . .
0.41 .. '.. . .
. '
I
I 1 1. , 1 I
0 20 40 60 80 100 120 140
Age in Months
Fig. 2. (a)Developmental quotients (individual developmental age measurements divided by chrono-
logical age) by age in trisomy 18. (b) Developmental quotients (individual developmental age measure-
ments divided by chronological age) by age in trisomy 13.
the relative lack of descriptive power of a single I& score showed that these 3 tests gave significantly different
in the lower end of the IQ range. mean values of both CA (PNatural History of Trisomy 18 and 13: I1 193
TABLE 111. Developmental Assessment the activities commonly documented in the first year
by Three Common Developmental Tests* were following, cooing, rolling, smiling responsively,
Mean ( & SE) Mean ( 2 SE) Mean ( 2 SE) reaching, and recognizing close adults. In the next 2
CA (months) DA (months) DQ (months) years, new activities included sitting supported, object
5.0 (f0.5) 0.19 (fO.02)
permanence, imitation, playing baby games, sitting in-
Bayley 40.0 (26.3)
Alpern 59.7 ( k 8.0) 6.3 ( ? 0.7) 0.22 ( f0.05) dependently, and recognizing words. In the next 3 years
Vineland 75.3 (k8.1) 6.9 (20.5) 0.13 ( 2 0 . 0 2 ) (at ages 4-6) commando crawling, independent playing,
* Some tests are combined. For example, a Bayley test may be given following simple commands, helping with hygiene
alone or in combination with any other developmental test, and it will tasks, standing, understanding cause and effect, and
be counted as a n entry. use of signs were reported. The older children could
identify common objects, use a walker, crawl, and under-
stand words and phrases. Trisomy 13 individuals at-
The data were divided into 7 main skill areas: recep- tained the same skills, and some also acquired some
tive language, expressive language, communication, toileting skills and walking ability. The data on specific
daily living, cognitive, social, and motor skills. There developmental skills which were collected from parents
were no significant differences in mean CAs between the of these same children were very consistent with the
7 skill areas. There were also no significant differences data obtained from formal developmental evaluations.
in CA between trisomy 18 and trisomy 13. We also abstracted information about feeding skills
There were highly significant differences in DAs be- from the medical records. For trisomy 18, 33/50 (66%)
tween many skill areas, using one-way analysis of vari- documented gavage feeding, 54% as newborns. Breast
ance (P194 Baty e t al.
TABLE V. Mean Developmental Quotient ( r Standard Error) by Skill Area
All Trisomy 18 Trisomy 13
Rec language 0.24 (20.04) Rec language 0.20 ( f0.05) Cognitive 0.33 ( ? 0.06)
Daily living 0.23 (h0.04) Cognitive 0.19 (kO.03) Rec lang 0.31 ( t 0.08)
Cognitive 0.22 (‘0.03) Daily living 0.19 (fO.05) Daily living 0.26 ( z 0.06)
Social *
0.21 ( 0.02) Social 0.18 (r0.03) Social 0.26 (t0.04)
Expr language 0.19 ( 2 0.03) Communication 0.15 (20.03) Expr language 0.23 ( 2 0.06)
Communication 0.18 (k0.03) Expr language 0.14 (-c0.03) Communication 0.23 (k0.05)
Motor 0.18 ( -t 0.01) Motor 0.14 (20.01) Motor 0.23 i? 0.021
data have a negative exponential distribution and accomplishments of their children are acknowledged by
are similar in both trisomy 18 and 13, although tri- the medical community. The range of DQ variation for
somy 13 had significantly higher DQs. The highest different developmental skill areas is relatively small
DQs and the greatest variation in DQs were in the and may even seem inconsequential. However, a differ-
first 2-3 years of life. The drop in DQ does not re- ence of several months of developmental skills in the
flect a loss of skills, but instead reflects an increased first year of life has great meaning to families. It could
lag in developmental progress compared to normal mean the difference between a child who sits alone vs. a
children. child who cannot sit unsupported, or the difference be-
2. Developmental ages in 7 skill areas were signif- tween nonresponsiveness vs. smiling, reaching out and
icantly different, with daily living and receptive lan- recognizing close adults. It is important that families
guage having the highest values and motor and have this information when a diagnosis of trisomy 18 or
communication skills having the lowest. When chro- trisomy 13 is made, either prenatally or postnatally.
nological age was taken into account, there was no
significant difference in DQs in the same 7 skill ACKNOWLEDGMENTS
areas, although there was a trend that was similar Dr. Jorde was supported by NIH Grant HG-00347 and
to the pattern of differences with developmental age. NSF Grant BNS-8720330. We would like to thank the
3. Although individuals with trisomy 18 and 13 many families who provided information about their
were clearly functioning in the severe to profound de- child’s development and/or developmental records.
velopmentally handicapped range, they did achieve
many skills of childhood, and always continued to REFERENCES
learn. Older children could use a walker, understand Baty BJ, Blackburn BL, Carey J (1994):The natural history of trisomy
words and phrases, use a few words andlor signs, 18 and trisomy 13: I. Growth, physical assessment, medical histo-
crawl, follow simple commands, recognize and inter- ries, survival and recurrence risk. Am J Med Genet 49:175-188.
act with others, and play independently. Walking Bos AP, Broers CJM, Hazebroek FWJ, van Hemel JO, Tjbboel D,
and some toileting skills were also reported for tri- Wesby-van Swaay E, Molenaar JC (1992):Avoidance of emergency
surgery in newborn infants with trisomy 18. Lancet 339:913-915.
somy 13.
Frankenburg WK, van Doorninck WJ, Liddell TN, Dick NP (1976):The
Denver Rescreening Developmental Questionnaire (PDQ). Pedi-
In the course of our contact with these families, it atrics 57344-753.
became clear that many parents resented the early mes- Gerhard M (1976): Development of motor skills in a child with tri-
sage that their child would never interact with his or her somy-18. Dev Med Child Neurol 18:538.
environment and family. Many professionals conclude Moyers R, Hartsook J, Kopel H (1974):Facial growth and dentition. In
that a diagnosis of trisomy 18 or trisomy 13 means a Lowey GH (ed): “Growth and Development of Children,” 6th ed.
Chicago: Year Book Medical Publishers, pp 354-384.
hopeless outlook with survival in a vegetative state, or Smith A, Silink M, Ruxton T (1978):Trisomy 18 in a n 11year old girl.
that the diagnosis is incompatible with life [Bos, 19921. J Ment Defic Res 22:277-286.
Many families with surviving trisomy 18 or trisomy 13 Smith A, Field B, Learoyd BM (1989):Trisomy 18at age 21 years. Am J
children think that the information they were given was Med Genet 34:338-339.
more discouraging than necessary, and ignored the hu- Van Dyke DC, Allen M (1990):Clinical management considerations in
manity of their child. It is important to parents that the long-term survivors with trisomy 18. Pediatrics 85753-759.You can also read