NCT HEIDELBERG NATIONAL CENTER FOR TUMOR DISEASES
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NATIONAL CENTER FOR TUMOR DISEASES NCT HEIDELBERG Sao Paulo, 28.04.2017 Standard post-operative treatment of high- grade gliomas in the elderly: is age a factor for change in treatment? Wolfgang Wick Neurology Clinic, University of Heidelberg Neurooncology Program German Cancer Research Center DKTK

Trial concepts for elderly patients To appreciate the differences in biology between tumors in different age groups Critically evaluate the concept of „elderly patients“ To understand patterns of care in elderly versus non-elderly patients Presentation of evidence and ongoing trials Future developments
Trial concepts for elderly patients • Incidence is raising (2020 > 50% of glioblastoma) • Age is a strong negative prognostic factor • Prognosis is dismal • „Cultural“ treatment differences • Differential tolerability • Co-morbidities • Differential biology?
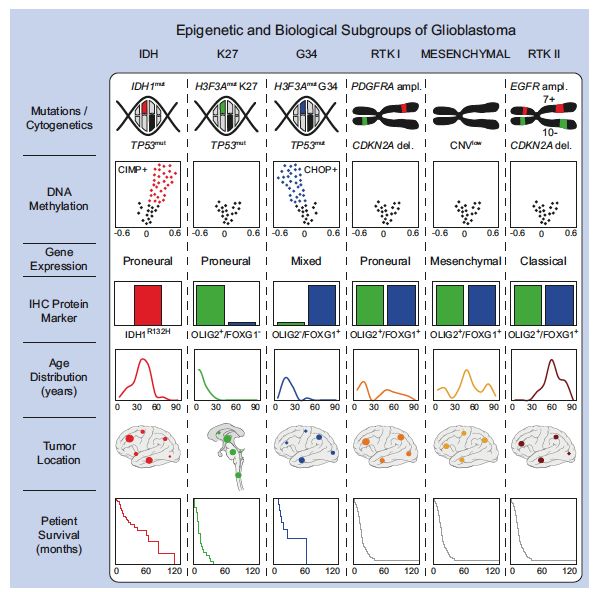
Sturm et al. Cancer Cell 2012

Sturm et al. Cancer Cell 2012
Sturm et al. Cancer Cell 2012
Sturm et al. Cancer Cell 2012
Absence of positive prognostic markers in glioblastoma of the elderly MGMT promoter methylation occurs at similar frequency IDH mutations occur at a lower frequency1 General methylation levels are low (e.g. PRDX, APNG)2 What is the impact of other biomarkers? Do gliomas in the elderly represent a separate disease entity?3 1. Reifenberger et al. Int J Cancer 2011 3. Sturm et al. Cancer Cell 2012 2. Wiestler B et al. Neuro Oncol 2013
Concept: the elderly brain tumor patient There might be molecular (genetic/epigenetic) differences n tumors of different age groups ≥ 50% of all glioblastoma patients will be > 65 years old The benefit derived from the addition of chemotherapy decreases with age Age per se is considered a risk factor for cognitive side effects from cranial irradiation Tolerability of combined modality treatment of RT plus TMZ in the elderly appears to be reduced
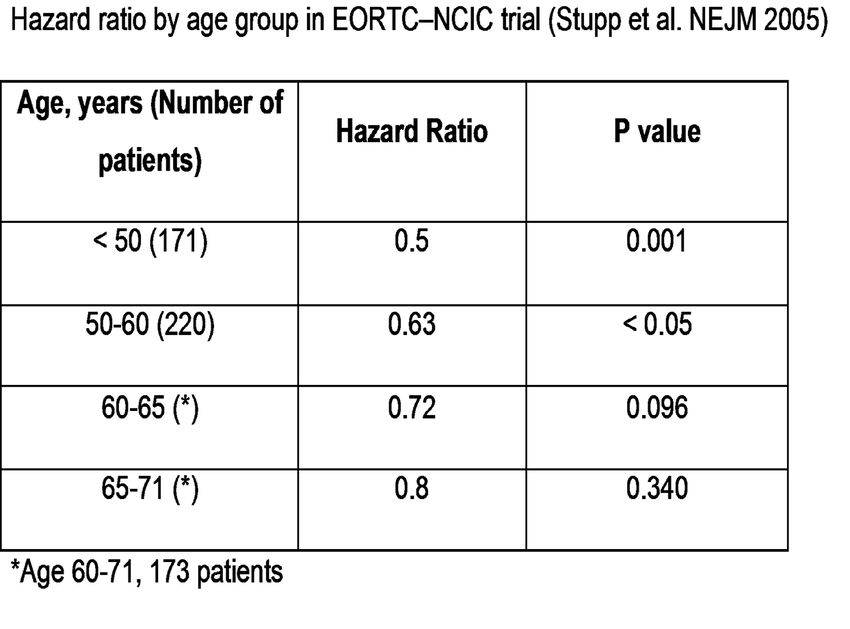
The benefit derived from the addition of chemotherapy decreases with age
Concept: the elderly brain tumor patient More limited life expectancy concern of compromising the quality of remaining lifetime by treatment-related toxicity It is not chronological age alone, but rather an age- associated increased prevalence of cardiovascular or neurological comorbidities that mainly limits the tolerability of treatments including surgery, radiotherapy and chemotherapy Increased risk of cognitive impairment Older patients may have a different view on the main value of therapy
Patterns of care Lower likelihood to be treated with a macroscopic resection Less aggressive secondary therapies Karnofsky Performance Status plus steroid treatment are relevant prognosticators Resection is superior to biopsy at least in selected patients Specific schedules of radiotherapy yield a modest but significant improvement over best supportive care Temozolomide has an acceptable tolerance, even when KPS
Standard of care – EANO guidelines There is no way around a histological/molecular diagnosis Maximal safe resection Age+MGMT status may/should be taken into consideration Radiochemotherapy with temozolomide (six maintenance cycles) irrespective of the MGMT status 2-3 monthly clinical and MRI F/U Multiple options but no standard at recurrence! Surgery/radiotherapy/nitrosoureas/bevacizumab Weller et al. The Lancet Oncol 2014 & 2017
NOA-08/Methvsalem
• Temozolomide (one week on/one week off) vs radiotherapy in
the primary treatment of anaplastic astrocytoma and
glioblastoma in elderly patients: a randomized phase III-study
Temozolomide
PD Radiotherapy
Histology
3 9 12 27 30 33 weeks
PD Temozolomide
Radiotherapy
TMZ 100 mg/m2 po/day for 7 days every 14 days
until failure of therapy, to be adjusted in 25-mg steps
Focal radiotherapy daily — 30 x 1.8-2 Gy to a
total 54–60 Gy
Gütesiegel AThe Nordic Elderly Glioma Trial
RT 60 Gy (2 Gy x 30)
R n=119 RT 34 Gy (3.4 Gy x 10)
TMZ x 6 (200 mg/m2 d 1–5 q 28d) Two phase III trials conclude from their prespecified biomarker
analyses a predictive role for MGMT
Challenges remain in the definition of the optimal test and cohort
Next steps should take these data into account
NOA-08
PFS
NORDIC
OS
Wick et al. Lancet Oncol 2012; Malmström et al. Lancet Oncol 2012Precision
Resistance to Therapy(TMZ) is
temozolomide
enhanced by corticosteroids
randomization
Mean tumor volume relative to average
volume of methylcellulose group
Tumor growth Remission
Methylcellulose
TMZ
NaCl Dexamethasone
Weiler, Blaes et al. PNAS 2014 Pitter et al. Brain 2016Precision
Steroids eliminate Therapy
the advantage from
MGMT promoter methylation
Event-free survival in elderly patients of the NOA-08
trial according to treatment and steroid useCCTG CE-6/EORTC 26062 – Elderly trial • RT alone is standard of care / control arm • 40 Gy/15 is a widely used schedule in elderly patients • Benefit of RT + TMZ clear if
CCTG CE-6/EORTC 26062 – Trial
design
Patient > 65 yrs with glioblastoma
Postsurgical randomization
RT 40.05 Gy in 15 Fx RT 40.05 Gy in 15 Fx -> TMZ
12 x TMZ 5/28 days
Perry et al. NEJM 2017CCTG CE-6/EORTC 26062 – Concept
• Objective: HR of 0.75 (= median survival from 6 to 8
months)
• 520 events for 90% Power, 2-sided test, a = 0.05
• Stratification factors
• center
• ECOG PS (0 or 1 vs 2)
• age (65-70 vs 71-5 vs >76yrs)
• extent of surgery (biopsy vs resection)
Perry et al. NEJM 2017CCTG CE-6/EORTC 26062 – Overall Survival
CCTG CE-6/EORTC 26062 – Overall Survival according to MGMT Perry et al. NEJM 2017
CCTG CE-6/EORTC 26062 – Summary • Addition of TMZ chemotherapy to standard short course RT significantly improves both PFS and OS in newly diagnosed elderly patients with glioblastoma • Benefit is particularly evident in patients with MGMT promoter methylation where median survival is nearly doubled • Remarkably, clinical benefit was also observed in pts with unmethylated tumours and these provide the strongest data to date for the use of TMZ in all elderly GB patient Perry et al. NEJM 2017
Wick A et al. in preparation
~30% ~60% ~10% PATIENTS MGMT methyl. MGMT unmethyl. undet. KPS / age ~10% SUPPORTIVE TREATMENT KPS 70 /
Elderly patients – open issues Definition of the elderly patient Clinically Biologically Be confident with the standard of care Comparison between RT/TMZ and TMZ MGMT? Next steps ARTE (BEV -> rather not, WFNO 2017) Immunotherapy? Precision therapy
Many thanks for your attention!
You can also read