Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM - Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Crizotinib in addition to Radiotherapy
and TMZ in newly diagnosed GBM
Juan M Sepúlveda Sánchez
Unidad Multidisciplinar de Neurooncología
Hospital 12 de Octubre
Madrid
GEINO 1402. Phase Ib, open-label, multicenter, dose-escalation study followed by an extension phase to evaluate the safety and activity of the combination of crizotinib with temozolomide and radiotherapy in patients with newly diagnosed glioblastoma Coordinators Dr. María Martínez. Hospital del Mar Dr. Juan M Sepúlveda. Hospital Universitario 12 Octubre Dose-scalation phase MTD Extension Phase 4 GEINO Centers: Hospital del Mar, Hospital Clinic, ICO Bellvitge, H 12 Octubre
Crizotinib (Xalkori ®) Protein kinase inhibitor by competitive binding with the ATP-binding pocket On August 2011, FDA approved Crizotinib to treat metastatic NSCLC with abnormal ALK gene Kinases inhibited: ALK (and its fusion proteins) ROS1 (and its fusion proteins) C-MET/Hepatocyte growth factor receptor (HGFR)
MET signaling in GBM.
C-MET amplification in 5% GBM
Chi AS, et al. JCO, Vol 30, No 3
(January 20), 2012: pp e30-e33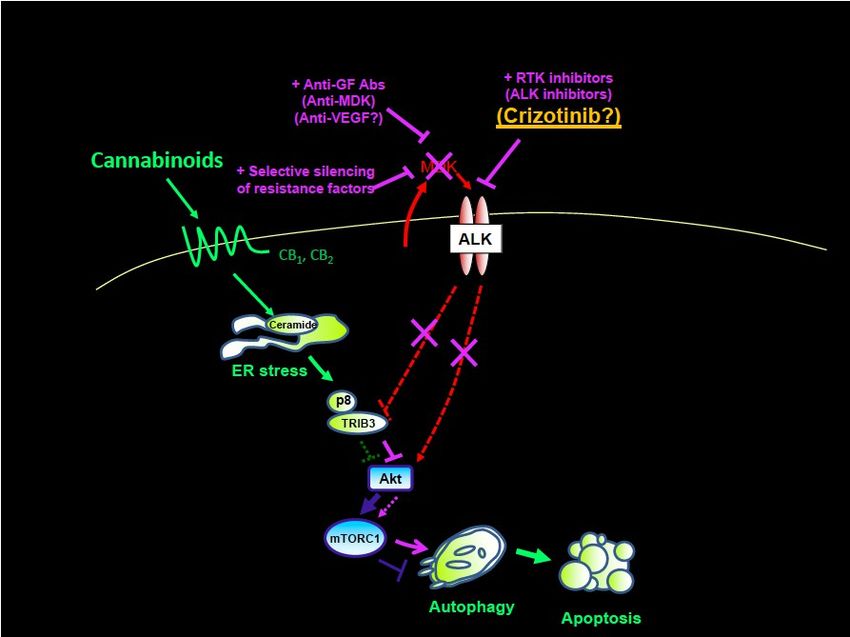
C-Met expression and function is associated with Cancer Stem Cell in GBM
• GBMs contains stem-like cells (GSC)
• Unlimited growth
• Self-renewal potential
• Multilineage differentiation
• Tumor recurrence
• Responsible for tumor progression and resistance to radiotherapy and chemotherapy
• MET activation
• Activates properties attributed to GSC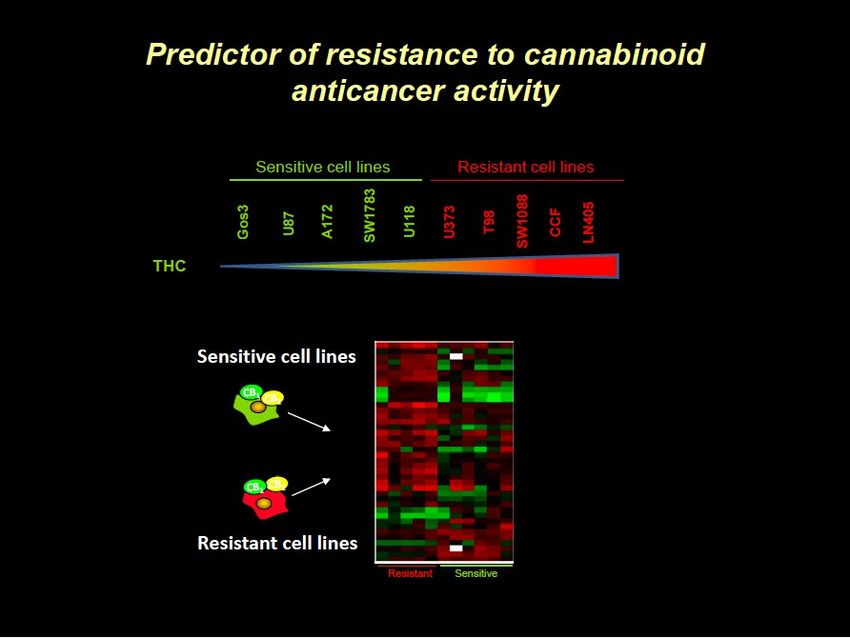
C-Met expression and function is associated with Cancer Stem Cell in GBM (in vitro
models)
• Met signaling can shift the heterogeneous composition of glioblastoma-derived neurosphere cells
Ly Y. c-Met signaling induces a reprogramming network and supports the
glioblastoma stem-like phenotype. PNAS June 2011
Rationale. ROS1 in GBM
30 GBM treated with
the Stupp regimen
Dorta M, et al. ASCO 2014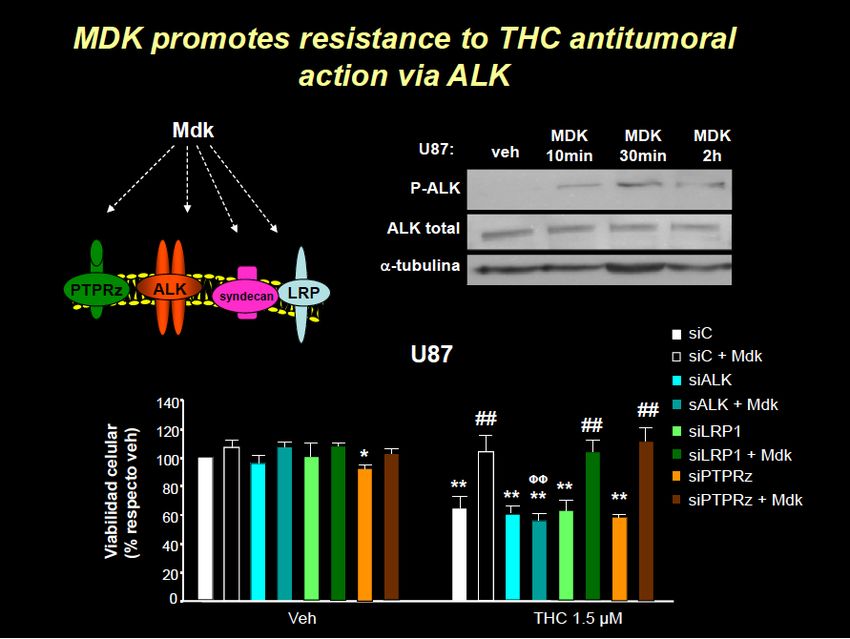
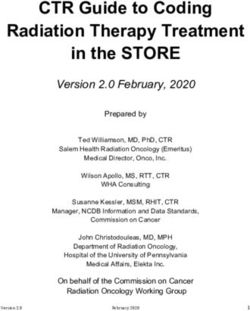
Rationale. ALK-MIDKINE Axis MIDKINE (MDK; MK;NEGF-2)
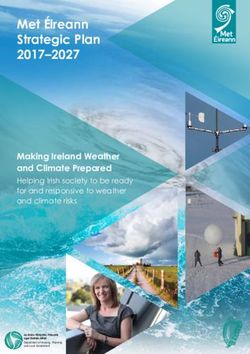
Midkine Receptors and signaling
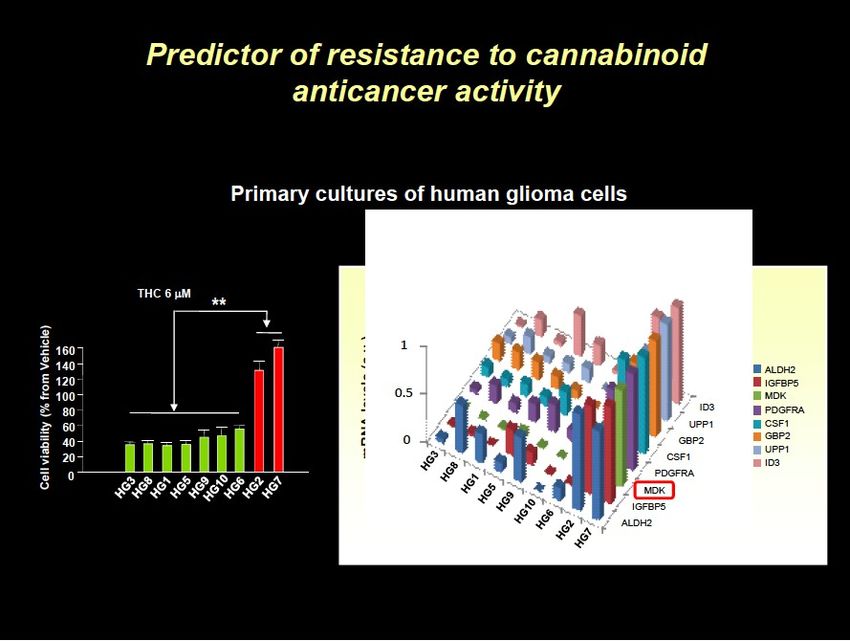
Identification of MDK as a factor of resistance to anticancer therapies
Slide Courtesy of Dr Guillermo Velasco (UCM)
Slide Courtesy of Dr Guillermo Velasco (UCM)
Lorente M et al, Cell Death Diff 2011.
Slide Courtesy of Dr Guillermo Velasco (UCM)
Slide Courtesy of Dr Guillermo Velasco (UCM)
Slide Courtesy of Dr Guillermo Velasco (UCM)
Blockade of MDK/ALK axis sensitizes Glioma Stem
Cells to treatment with anticancer agentsSlide Courtesy of Dr Guillermo Velasco (UCM)
Slide Courtesy of Dr Guillermo Velasco (UCM)
Slide Courtesy of Dr Guillermo Velasco (UCM)
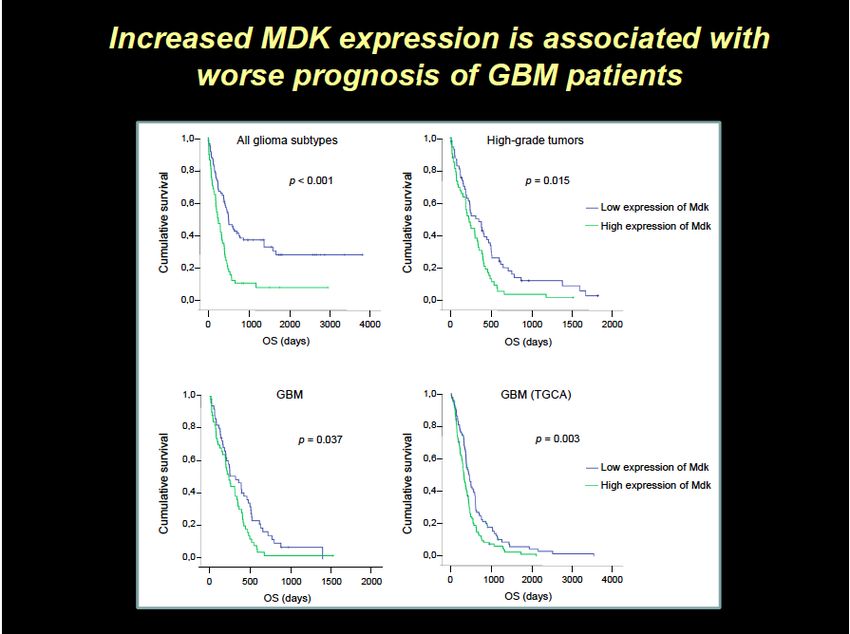
The role of the growth factor midquine (MDK) in
the resistance of glioma cells to anticancer
agents
• Midquine (MDK) is a factor of bad prognosis in GBM
• high expression of this protein is associated with lower survival of glioma
(Lorente et al. Cell Death Differ. 18:959-
973; 2011)
• Mdk promotes the resistance of glioma cells to anticancer agents
• This effect relies on the stimulation of ALK receptor
• "in vivo" silencing of Mdk or pharmacological inhibition of ALK sensitized these tumors to the
treatment with TMZHypothesis
• Crizotinib is a rational therapeutic agent. Mechanisms of action:
• Blocking MET signalling
• Decrease tumor cell proliferation, survival and migration
• Of special interest in the 5% of patients with MET amplification
• Targeting GSCs
• Cells related with chemo and radioresistance
• blocking MET and Mdk are of special interest for GSC activation
• Reverting temozolomide resistance induced by high levels of
Mdk
• Mdk is a recently discovered ALK ligand
• ROS1 inhibitionStudy Design
23STUDY DESIGN
• Escalation Phase
Standard “3+3” dose escalation
N~12 (based on currently estimated 4 cohorts x 3 patients)
Crizotinib will be administered under fasting conditions initially QD, on a
continuous schedule in successive dose-escalating cohorts at doses
ranging from 200 QD to 250 mg BID (1st level- 200 QD; 2nd level- 250 QD, 3rd level- 200 BID and 4th
level- 250 BID)
• Expansion Phase
Crizotinib+RT+TMZ at RPTD
N~12
Time to complete enrollment: 1 year (7 centers)DOSE ESCALATION PHASE (N=12, Sites=4)
Primary Objective
To determine the safety profile including the MTD, of
escalating doses of crizotinib administered with TMZ during
and after RT in patients with newly diagnosed GBM.
Secondary Objectives
To determine the recommended phase II dose (RPTD) and
schedule for crizotinib plus TMZ-RT.
To describe the preliminary anti-tumor activity of the
combination therapy through PFS (6 months PFS rate) and
the response rate in patients with measurable disease.
To analyze OS.EXPANSION PHASE (N=12 , and 2 aditional sites)
• Primary objectives:
To describe the safety profile of crizotinib administered with TMZ during
and after RT.
To determine the RPTD and schedule for crizotinib plus TMZ-RT
To assess PFS (PFS rate at 6 months)
Secondary objectives:
To assess anti-tumor response according to RANO criteria.
To assess changes in glucocorticoid use.
To assess changes in neurological status.PATIENTS
MAIN EXCLUSION:
MAIN INCLUSION:
Extracraneal metastatic
Newly diagnosed GBM
disease
confirmed by biopsy or resection
EIADs
no > 4 weeks before registration
GI abdnormalities, inability to
15 unstained slides or tissue
take oral medication
block
Significant cardiovascular
KPS ≥60%
disease
Adequate hematologic,
Leptomeningeal
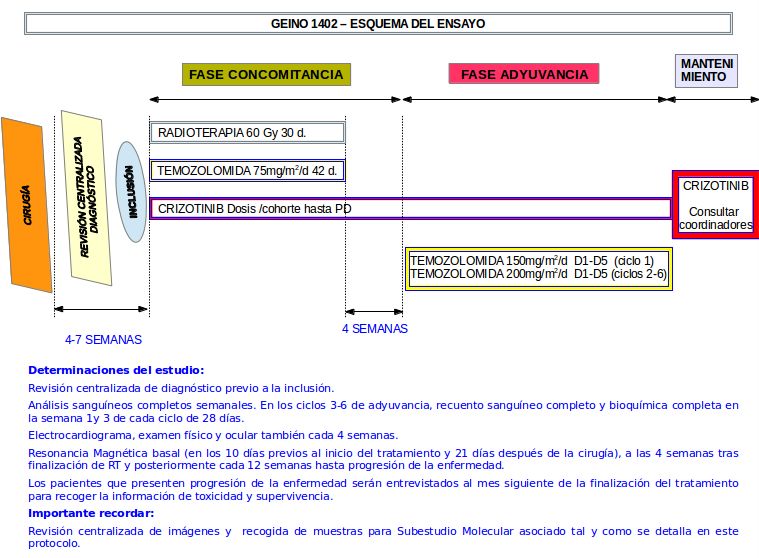
liver and renal function diseminationTREATMENT PLAN 4-6 weeks after surgery RT: 1,8-2 Gy/d, 5d/week, total dose 58-60Gy Concomitant TMZ 75 mg/m2, for max of 42 d, + Crizotinib (after RT continue) 4 weeks after RT: TMZ maintenance: 150 mg/m2 5d/28d, and after 200 mg/m2, total of 6 cycles. Additional Crizotinib beyond 6 cycles will be allowed.
STATISTICAL CONSIDERATIONS The primary objective of this trial is to find the RPTD of crizotinib in combination with radiotherapy and temozolomide A 6-month PFS rate between 50 and 70% will be considered of desirable interest for a further phase II clinical trial. The 6 months PFS rate in the Stupp trial was 54% in those patients treated with RT and TMZ.
DDI : TMZ and Crizotinib No pharmacological interactions are expected with TMZ and crizotinib. Plasma clearance of temozolomide is independent of age, renal function, liver function or tobacco use. Temozolomide is eliminated primarily in the urine. Temozolomide does not appear to affect the metabolism of drugs by CYP450.
Biomarker Study ROS1, ALK and c-MET alterations Frequency Association with response and Survival MK tissue expression MK Blood levels
Thank you for your attention
You can also read