Nuovi target, nuove insuline - Elisabetta Torlone S.C. E.M.M. A.O. S. Maria della Misericordia Perugia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Nuovi target, nuove insuline
Elisabetta Torlone
S.C. E.M.M.
A.O. S. Maria della Misericordia Perugia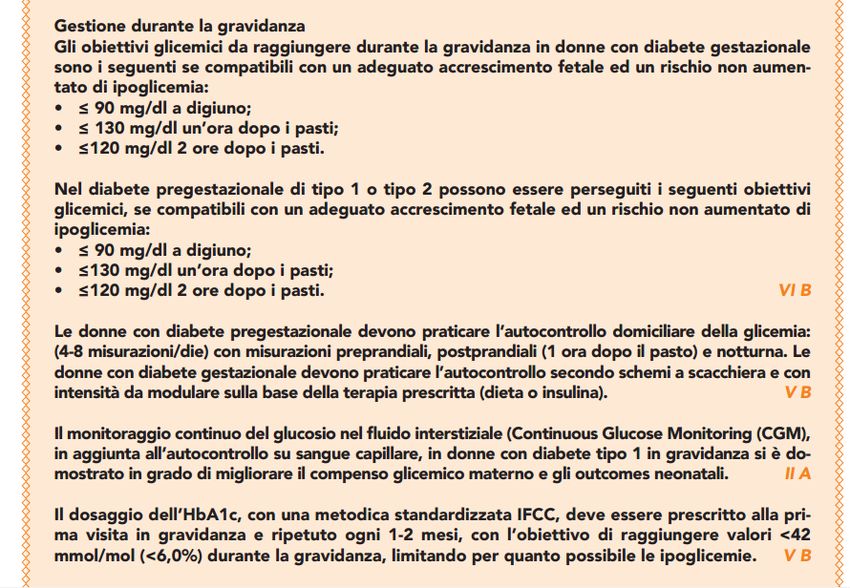
...
La dot.ssa Elisabetta Torlone dichiara di NON aver ricevuto negli ultimi due
anni compensi o finanziamenti dalle seguenti Aziende Farmaceutiche e/o
Diagnostiche:
Dichiara altresì il proprio impegno ad astenersi, nell’ambito dell’evento, dal
nominare, in qualsivoglia modo o forma, aziende farmaceutiche e/o
denominazione commerciale e di non fare pubblicità di qualsiasi tipo
relativamente a specifici prodotti di interesse sanitario (farmaci, strumenti,
dispositivi medico-chirurgici, ecc.)
2
SAINT VINCENT DECLARATION
10-12 OCTOBER 1989
“Achieve a pregnancy outcome in the
.
diabetic woman that approximates that
of the non-diabetic woman.”
40 years later
Congenital malformations RR 5.0
Perinatal mortality RR 3.7
Preterm delivery RR 4.2
Large for gestational age RR 4.5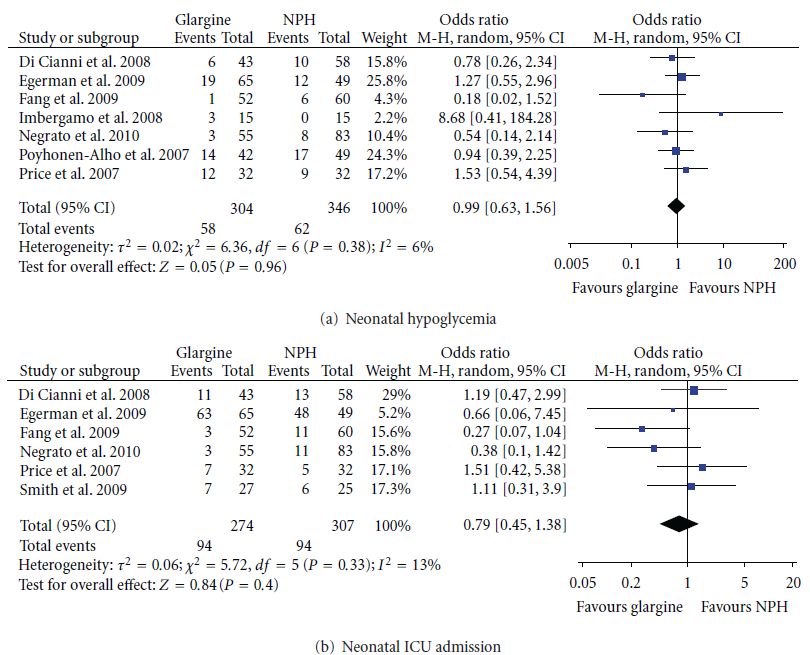
51 WOMEN
Daily mean
glucose values
Daily mean
71,9± 5,7 glucose
mg/dl
values
78,3± 5,4
mg/dl
Mean postprandial glucose peak/levels NEVER EXCEED 105,2 MG/DL
Glicemie Normali in Gravidanza
Picco della Glicemia dopo pasto (CGMS): 69,4±23.9’
Hernandez T.L et al. Patterns of glycemia in normal pregnancy: should the current therapeutic targets be challenged? Diabetes Care; 34(7):1660-68, 2011
Hernandez Teri L and Barbour Linda A. Review: A Standard Approach to Continuous Glucose Monitor Data in Pregnancy for the Study of Fetal Growth and Infant
Outcomes, Diabetes Technology & Therapeutics Volume 15, Number 2, 1-8, 2013
Monitoraggio dei Chetoni Una chetosi frequente e prolungata può avere effetti negativi sul feto e deve essere evitata durante la gravidanza; a questo scopo, devono essere effettuati controlli frequenti della chetonuria e/o chetonemia al risveglio, in caso di malattie intercorrenti, e comunque in presenza di valori glicemici persistentemente >180 mg/dl (Jovanovic L. Medical management ). Il principale corpo chetonico aumentato nella chetoacidosi è il beta-OHB (beta-idrossibutirrato); né l’acetone né il beta-OHB reagiscono fortemente col nitroprussiato (reagente utilizzato per evidenziare la presenza di chetonuria) come l’acetoacetato, pertanto i livelli di chetoni plasmatici di una paziente possono essere sottostimati dalla sola misurazione della chetonuria. Klocker e coll. hanno dimostrato che la misurazione del beta-OHBplasmatico rispetto a quella dell’acetoacetato urinario riduce i costi, ed è in grado di monitorare più precisamente la risoluzione della chetoacidosi (Klocker AA, 2013). Perciò il dosaggio dei chetoni plasmatici sarebbe da preferire a quello dei chetoni urinari (Gruppo interassociativo AMD-SIDSIEDP 2015). Le recenti linee-guida NICE sottolineano l’importanza di offrire il dosaggio della chetonemia alla donna con diabete tipo 1 sia in programmazione sia in gravidanza (NICE 2015; Dalfrà MG, 2015).
Black: Early pregnancy (12-16 week) Grey: Late pregnancy (28-32 week)

Postprandial Glucose Disposal Postprandial Insulin
peak
….. the optimal timing for prandial insulin is 15 min before meals in early pregnancy
and 30–40 min before meals in late pregnancy.
Black: Early pregnancy
Grey: Late pregnancyUltra-Fast-Acting Insulin: Approaching a
More Exact Physiological Insulin Profile
• First-generation rapid-acting
From the normal pancreas
insulins had improved action
Insulin Action (At Mealtime)*
'Faster-acting' insulin profile vs RHI
Rapid-acting insulin • Ultra-fast-acting insulins:
– Better approach physiological insulin
secretion in T1DM
– Replace early insulin secretion in T2DM
RHI
– Have a better profile for pump therapy
Time, h
*Schematic representation.
Home PD. Diabetes Obes Metab. 2015;17:1011-1020.Faster-Acting Insulin Aspart: A New Formulation of Insulin Aspart
Tyr Phe Phe
• Insulin aspart: reduced strength of the
Thr Gly
Asp Arg
Glu
Lys B28
insulin dimer leading to fast absorption[a] B30
Thr Gly
A21 SS Cys
• Faster-acting insulin aspart is a new Asn Cys
Tyr Val
formulation of insulin aspart, which Asn
Glu
Leu
contains 2 excipients, nicotinamide and A1 Gly
Tyr
Insulin aspart Leu Leu
arginine[b]
Ile
Gln Ala
Val
Tyr
• Nicotinamide acts as an absorption Glu
SS Leu
Glu
Val
modifier; arginine acts as a stabilizing Gln
Cys Cys Thr Ser Ile Cys
Ser
Leu
agent His
SS Ser
• Both ingredients are "generally Gly
recognized as safe" by the FDA B1 Phe Val Asn Gln His Leu
Cys
• The excipients result in a stable
formulation and faster initial absorption Nicotinamide: absorption modifier
after SC injection L-Arginine: added for stability
a. Brange J, et al. Diabetes Care. 1990;13:923-954.
b. Heise T, et al. Diabetes Obes Metab. 2015;17:682-688. Figure courtesy of Tim Heise, MD.Faster-Acting Insulin Apart Pooled Analysis: Onset and Offset
of Insulin Exposure
300 Faster aspart Ratio (95% CI)
Insulin aspart
Cmax (pmol/L) 1.04 (1.00, 1.08)
250
Insulin aspart serum conc. (pmol/L)
AUCIAsp, 0-12h (pmol·h/L) 1.01 (0.98, 1.04)
200 AUCIAsp, 2-12h (pmol·h/L) 0.89 (0.85, 0.93)*
Treatment Difference (95% CI)
150 –10/–12 min
t50%Cmax (min) -9.5 (-10.7, -8.3)*
tlate50%Cmax (min) -12.2 (-17.9, -6.5)*
100
50
0
0 1 2 3 4 5 6 7 8
Time (h)
*statistically significant.
(Faster-acting insulin aspart is approved in the US, Canada, EU, Australia [CSII only in the EU].)
Reproduced from Heise T, et al. Clin Pharmacokinet. 2017;56:551-559.Insulin Fiasp During
Pregnancy and Laction in
Women With Pre-existing
Diabetes
NCT03770767Study Description
Condition or disease Intervention/treatment Phase
Diabetes MellitusPregnancy Drug: Faster-acting Aspart insulin Phase 4
Complications FiaspDrug: Control (insulin Novorapid or
insulin Lispro)
Study Design
Study Type : Interventional (Clinical Trial)
Estimated Enrollment : 200 participants
Allocation: Randomized
Intervention Model: Parallel Assignment
Masking: None (Open Label)
Primary Purpose: Treatment
Estimated Study Start Date : September 1, 2019
Estimated Study Completion Date : August 31, 2022Arm and
Intervention/treatment
Arm Intervention/treatment
Active Comparator: Intervention with insulin Drug: Faster-acting Aspart insulin FiaspRandomization to
FiaspWomen randomized to insulin Fiasp treatment with insulin Fiasp
Active Comparator: Control (insulin Novorapid or Drug: Control (insulin Novorapid or insulin
Lispro)Women randomized to usual rapid-acting insulin, Lispro)Randomization to usual treatment with insulin
i.e. insulin NovoRapid or insulin Lispro. Novorapid or LisproEligibility Criteria
Ages Eligible for Study: 18 Years to 45 Years (Adult)
Sexes Eligible for Study: Female
Accepts Healthy Volunteers: No
Criteria
Inclusion Criteria:
•Duration of type 1 or type 2 diabetes ≥ 12 months at inclusion
•Pregnant with an intrauterine singleton living fetus (8 to 13 completed gestational weeks) at
inclusion confirmed by an ultrasound scan
Exclusion Criteria:
•A diagnosis with severe mental or psychiatric barriers or a concurrent disease on the decision of
the principal investigator
•No proficiency in Danish to understand oral and written informationPrimary Outcome Measures Birth weight standard deviation score [ Time Frame: At delivery ] Offspring birth weight (measured as standard deviation score) adjusted for gestational age and gender
Fabbisogno insulinico nel DM1 in
gravidanza
A.Garcia-Petterson et al, Diabetologia 2009
0,9-1,2 UI/kg/24 ore
+ 30-50%
Insulin requirement displayed a peak in week 9, a nadir in
week 16, a second peak in week 37. For the change in insulin
requirement the sharpest slope was observed from 16 to
week 37.ABBIAMO SDOGANATO GLI
ANALOGHI?
.
Maka S. Hedrington & Stephen N. Davis , 2017
BI: birth injury; DO: delayed ossification; FD:
fetal death; FGR: fetal growth retardation; FN:
fetal nephrotoxicity; LBW: large birth weight;
LI: labor induction; M: macrosomia, NH:
neonatal hypoglycaemia; PD: placental
dysfunction; RD: respiratory distress; SA:
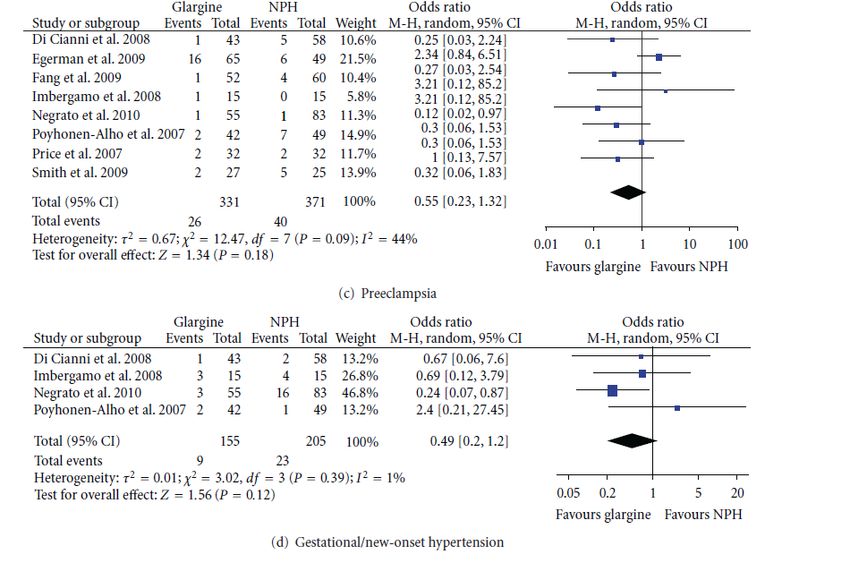
skeletal anomalies;DETEMIR vs NPH Nessuna differenza nelle complicanze materno-fetali, minor rischio ipoglicemico, glicemia a digiuno significativamente inferiore, controllo glicemico simile
2001-2009 79% R+RF 49%
Pregnancy
Insulin option Notes
Category
Basal (control of fasting/preprandial glucose)
NPH B
Detemir B
Not formally studied in pregnancy,
Glargine C
though frequently prescribed
Degludec C Not studied in pregnancy
Bolus (control of postprandial hyperglycemia)
Aspart, lispro B
Regular B
Glulisine C Not formally studied in pregnancy
Pump therapy with
rapid-acting B
NPH, Neutral Protamine Hagedorn; SMBG, self-monitoring of blood glucose
analogs
Handelsman YH, et al. Endocr Pract. 2015;21(suppl 1):1-87. ADA. Diabetes Care. 2015;38(suppl 1):S77-S79. Jovanovic L, et al. Mt
35
Sinai J Med. 2009;76:269-280. Castorino K, Jovanovic L. Clin Chem. 2011;57:221-230.DEGLUDEC .
NN1250-4300 EXPECT
Study Type : Interventional (Clinical Trial)
Estimated Enrollment : 300 participants
Allocation: Randomized
Intervention Model: Parallel Assignment
Masking: None (Open Label)
Masking Description: Sponsor staff involved in the clinical trial is masked
according to company standard procedures.
Primary Purpose: Treatment
Official Title: A Trial Comparing the Effect and Safety of Insulin Degludec
Versus Insulin Detemir, Both in Combination With Insulin
Aspart, in the Treatment of Pregnant Women With Type 1
Diabetes
Actual Study Start Date : November 22, 2017
Estimated Primary Completion Date : October 15, 2021
Estimated Study Completion Date : October 15, 2021Arm and Intervention/treatment
Arm Intervention/treatment
Experimental: Insulin Degludec Insulin Degludec Drug: Insulin degludec Injection for subcutaneous
once daily and Insulin Aspart 2-4 times daily (s.c., under the skin) use once daily. The total trial
duration for subjects will be maximum 25 months
Drug: Insulin Aspart Injection for subcutaneous (s.c.,
under the skin) use 2-4 times daily with meals. The
total trial duration for subjects will be maximum 25
months
Active Comparator: Insulin Determir Insulin Determir Drug: Insulin Aspart Injection for subcutaneous (s.c.,
once daily or twice daily and Insulin Aspart 2-4 times under the skin) use 2-4 times daily with meals. The
daily total trial duration for subjects will be maximum 25
months
Drug: Insulin detemir Injection for subcutaneous
(s.c., under the skin) use, once daily or twice daily.
The total trial duration for subjects will be maximum
25 monthsEligibility Criteria
Ages Eligible for Study: 18 Years and older (Adult, Older Adult)
Sexes Eligible for Study: Female
Accepts Healthy Volunteers: No
Exclusion Criteria:
-Criteria
Treatment with any medication for the indication of diabetes or obesity other than stated in
the inclusion
Inclusion criteria
Criteria: withinage
- Female, theatpast
least9018days prior
years to the
at the timedayofof screening
signing informed consent -
-Diagnosed
Pregnant with
and having
type 1 proteinuria as evaluated
diabetes mellitus by urine
for at least 1 yearprotein-to-creatinine ratio above
prior to the day of screening - or
equal to
Treated 300multiple
with mg/g indaily
urinesubcutaneous
sample measured insulinatinjections
screeningor continuous subcutaneous
-insulin
Subject being treated
infusion (CSII) oror became
inhaled pregnant
insulin for atwith
leastassistance of intovitro
90 days prior the fertilisation or other
day of screening
- medical infertility
The subject treatment
is planning - Receipt
to become of any concomitant
pregnant within 12 monthsmedication contraindicated
from randomisation in
and
pregnancy according pre-pregnancy
willing to undertake to local label within 28 daysorbefore
counselling screening
the subject and between
is pregnant with anscreening
and randomisation
intrauterine for non-pregnant
singleton subjects and
living foetus (gestational 28 days
week before
8 to 13 conception
(+6 days)) withoutandany
between
conception and randomisation
observed anomalies for pregnant
at randomisation, subjects
confirmed by -an
Proliferative
ultrasoundretinopathy
scan or
- maculopathy requiring
HbA1c at screening acute
below ortreatment.
equal to 8.0% Verified by fundus photography
(64 mmol/mol) or
by central laboratory
pharmacologically dilated fundoscopy performed within the past 90 days prior to
randomisation for non-pregnant subjects or within 28 days prior to randomisation for
pregnant subjects. - History of severe hyperemesis gravidarum (requiring hospitalization)NN1250-4300 EXPECT: ITALIA
Site
PI Name Site Number Status
Emanuela Orsi 301 Active
Marina Scavini 302 Active
Elisabetta Torlone 303 Active
Fabio Broglio 304 Approved
Annunziata Lapolla 305 Active
Angela Napoli 306 ActiveTake Home Messages • Il corredo di farmaci oggi a nostra disposizione ci permette di ottenere target glicemici più stringenti • Gli analoghi rapidi LisPro, Aspart e i lenti Datemir e Glargina possono essere usati tranquillamente nelle gravidanze complicate da diabete: i dati su Glulisina sono ancora modesti ma le gravidanze registrate apparentemente non hanno dimostrato effetti negativi. • Le stesse indicazioni sono applicabili anche ai biosimililari, e alle insuline concentrate LP U200 e Gla U300 • Le insuline ultrarapide potranno aiutarci a raggiungere più facilmente i target glicemici post-prandiali • Attendiamo i risultati dello studio EXPECT
I Have a dream…. “Achieve a pregnancy outcome in the diabetic woman that approximates that of the non-diabetic woman.”
GRAZIE PER L’ATTENZIONE
You can also read