NUTRISYSTEM-D AS A LIFESTYLE INTERVENTION
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NUTRISYSTEM-D AS A LIFESTYLE INTERVENTION
Bruce Daggy, Ph.D., Anthony Fabricatore, Ph.D., Meghan Nichols, R.D., Amy Samuelson Ph.D.
This article reviews the recommendations of lifestyle intervention for the prevention and management of
diabetes, and describes the Nutrisystem-D Program in the context of these recommendations.
Nutrisystem-D Program Information
All Nutrisystem weight loss programs provide home delivery of shelf stable or frozen meal entrées, snacks and
desserts. These items, when complemented with grocery additions (including fruits, vegetables and low fat
dairy products), result in structured meal plans that are hypo-caloric, portion-controlled, low in glycemic index,
and consistent with national guidelines for general adult nutrition. The Nutrisystem structured meal plans are
combined with educational support and monitoring tools to assist members in adopting long term healthy
lifestyle habits.
Multiple peer reviewed clinical studies have demonstrated that the use of portion-controlled meal programs
result in better short-term weight loss among obese persons, when compared with diet plans designed to
deliver an equivalent number of calories (Jeffery et al., 1993; Ditschuneit et al., 1999; Heymsfield et al., 2003;
Hannum et al., 2004; Hannum et al., 2006; Wadden et al., 2007). Benefits for weight loss also have been
observed in patients with type 2 diabetes who consume portion-controlled meal programs, compared with
those who attempt to follow isocaloric self-selected diets. (Cheskin et al., 2008, Yip et al., 2001). Nutrisystem-D
is a weight loss program specifically designed to produce gradual, realistic, and clinically meaningful weight
loss in overweight and obese patients with type 2 diabetes. Further details of the program’s design and
effectiveness are given below, in the context of national guidelines.
The Role of Weight Control in the Prevention and Management of Type 2 Diabetes
Several professional and scientific organizations recognize the importance of weight loss for the prevention
and management of health complications, including type 2 diabetes, in obese and overweight individuals. The
National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH), for example,
concluded that a 5 to 7% reduction in initial weight (e.g., 10 to 14 pounds for a 200-pound person) can
significantly reduce obesity-related risk (National Heart, Lung and Blood Institute Obesity Education Initiative,
1998). This statement was supported by the Diabetes Prevention Program (among other trials), which found a
58% reduction in the incidence of type 2 diabetes with a modest (~7%) weight loss among participants with
impaired glucose tolerance (DPP Research Group, 2002).
The Look AHEAD Trial: The NIH is funding a multicenter randomized trial of the effect of modest intentional
weight loss on cardiovascular morbidity and mortality in persons with type 2 diabetes. Look AHEAD (Action for
Health in Diabetes) is an ongoing investigation that includes over 5000 overweight and obese patients with
type 2 diabetes, who were 45-74 years old at enrollment (https://www.lookaheadtrial.org/public/home.cfm).
Participants, who will be followed for up to 13.5 years were randomized to receive an intensive lifestyle
intervention (ILI), which was designed to help participants achieve and maintain a weight loss of at least 7% of
initial weight, or diabetes support and education (DSE), which is essentially a control group that receives four
educational sessions per year. The ILI included a dietary prescription of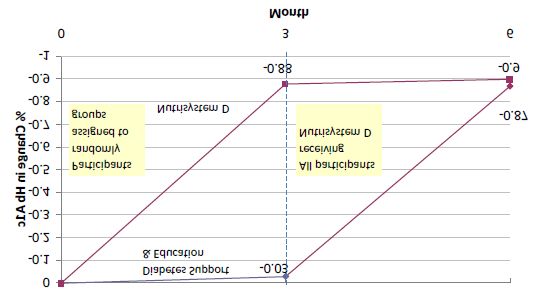
The American Diabetes Association (ADA), in its annual “Standards of Medical Care in Diabetes” emphasizes
the importance of weight control in patients who have, or are at risk of, type 2 diabetes. Selected quotations
from this position paper appear below.
“Because of the effects of obesity on insulin resistance, weight loss is an important therapeutic
objective for overweight and obese individuals with prediabetes and diabetes. Short-term studies have
demonstrated that moderate weight loss (5% of body weight) in subjects with Type 2 diabetes is
associated with decreased insulin resistance, improved measures of glycemia and lipemia, and
reduced blood pressure” (ADA 2010, pg. S24)
“In overweight and obese insulin resistant individuals, modest weight loss has been shown to reduce
insulin resistance. Thus weight loss is recommended for all overweight or obese individuals who are at
risk for diabetes.” (ADA 2010, pg. S23)
“Among individuals at high risk for developing type 2 diabetes, structured programs emphasizing
lifestyle changes that include moderate weight loss (7% of body weight) and regular physical activity
(150min/wk) with dietary strategies including reduced calories and reduced intake of dietary fat can
reduce the risk for developing diabetes and are therefore recommended” (ADA 2010, pg. S24)
Some of the key therapeutic goals of diabetes management to which nutrition can contribute are further
addressed in the ADA‟s 2010 Guidelines as noted below:
“Glycemic Control is fundamental to the management of diabetes.” (ADA 2010, pg. S20)
“Lowering A1C to below or around 7% has been shown to reduce microvascular and neuropathic
complications of type 1 and type 2 diabetes. Therefore, for microvascular disease prevention, the A1C
goal for non pregnant adults in general isIt is important to note that Foster et al. (2009) analyzed outcomes on an intent-to-treat basis, rather than
conducting a less stringent (less methodologically rigorous) completers’ analysis. Results among participants
who complete a program are typically more impressive.
Appropriate Nutrition for Type 2 Diabetes Prevention and Management
The ADA also takes a position on the nature of the diet that is appropriate for weight loss in type 2 diabetic
patients. Further quotes from the same 2010 position paper and a 2008 ADA position statement, “Nutrition
Recommendations and Interventions for Diabetes” state the following:
“Monitoring carbohydrate intake, whether by carbohydrate counting, exchanges, or experience-based
estimation, remains a key strategy in achieving glycemic control.” (ADA 2010, pg. S24)
“Low-glycemic index foods that are rich in fiber and other important nutrients are to be
encouraged.”(ADA 2010, pg. S64) “Saturated Fat intake should be less than 7% of total calories” (ADA
2010, pg. S24)
“Reducing intake of trans fat lowers LDL cholesterol and increases HDL cholesterol; therefore intake of
trans fat should be minimized” (ADA 2010, pg. S24)
“Limit dietary cholesterol toappropriate serving sizes to support weight loss. As noted in the first section of this paper, studies suggest that
providing some of the food for a weight loss attempt in the form of portion controlled packages improves short
term weight loss outcomes.
Conclusions: Expert opinion, as expressed in position statements from Federal health
authorities (e.g., NHLBI) and the American Diabetes Association, reveals a scientific consensus
as to the importance of weight loss for the prevention and management of type 2 diabetes. A
reduced-calorie, low-fat, portion-controlled diet designed to produce gradual weight loss of 1-2
pounds per week is generally recommended for overweight or obese type 2 diabetics or pre-
diabetics. The Nutrisystem-D program is consistent in design with the recommendations of
these expert bodies. The actual home delivery of the elements of the diet that pose the greatest
portion control challenges (entrees, snacks and desserts) is a key program feature that has
been consistently associated with improved short term weight loss. The clinical data for
Nutrisystem-D further support both the soundness of the national recommendations and the
efficacy of the program.
The Low Glycemic Index Diet for Type 2 Diabetes Management
The optimal diet to follow for all people with type 2 diabetes to manage their disease has not yet been
established. However, a statement issued by the American Diabetes Association in 2010 (ADA 2010) has
identified several critical components of effective medical nutrition therapy. They include: slow, moderate
weight loss (at least 5% of initial body weight); a nutrient-rich diet low in both saturated and trans fats; and
close monitoring of total carbohydrate consumption (by means of carbohydrate counting, food exchanges, or
individualized estimations of consumption). In addition, the ADA states:
“For individuals with diabetes, use of the glycemic index and glycemic load may provide a modest
additional benefit for glycemic control over that observed when total carbohydrate is considered alone.”
(ADA 2010, pg. S24)
Glycemic Index and Glycemic Load Defined
The term “glycemic index” was first used in a 1981 published manuscript by Jenkins et al.; the peer-reviewed
literature now contains hundreds of research papers and at least 69 review articles on the topic (for two recent
reviews, see Brand Miller et al, 2009, and Esfahani et al., 2009). The glycemic index (GI) is an empirically
derived measure of blood glucose response to carbohydrate intake. To calculate GI, the incremental area
under the glucose response curve following ingestion of a fixed, standard amount of carbohydrate in a
particular food is compared to the incremental area under the glucose response curve following consumption
of the same amount of carbohydrate from a control food (typically a glucose solution or white bread). An
additional tool, the glycemic load (GL), has recently been developed to determine the glycemic response to the
total carbohydrate load from consuming a particular food or diet.
Foods referred to as “low glycemic” are digested slowly, causing a gradual and prolonged increase in post-
prandial blood glucose levels. In contrast, “high glycemic” carbohydrate foods are rapidly digested, causing an
immediate and strong glycemic response. As a result, calorie-for-calorie, regularly consumed high glycemic
index meals in people with type 2 diabetes can result in higher blood glucose and insulin levels, in addition to
higher glycosylated hemoglobin levels, compared to results from low glycemic meal consumption (Ludwig,
2003). A recent meta-analysis found that reductions in A1c were 0.5 to 0.9% greater among patients with
diabetes who received low GI diets, compared with higher GI alternatives (Thomas & Elliott, 2009).
While the science supports recommending a low glycemic index diet for glycemic control and weight loss in
people with type 2 diabetes, adherence to this dietary approach may be challenging for patients. The primary
dietary need for everyone with type 2 diabetes is tight control of the total amount of carbohydrate consumed
(ADA 2010, pg S24). Some patients may become overwhelmed if they simultaneously try to master both the
amount and type of carbohydrates in their diets. In addition, the glycemic index of a food is affected by many
factors, including macronutrient content, food processing, and even food ripeness. It is not possible to
determine the glycemic index of a food by reading a nutrition facts panel. So, while it is possible to teach
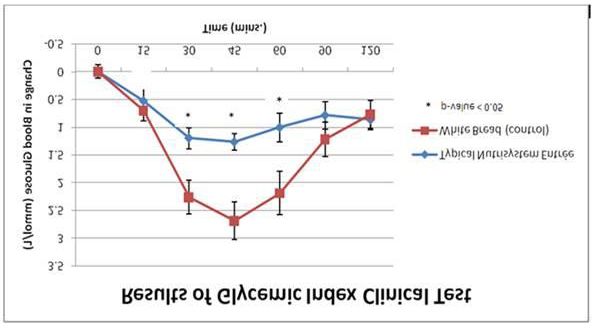
adherence to a low GI diet, use of the Nutrisystem-D program greatly reduces the guesswork and complexityof food selection and meal planning. Entrées in the Nutrisystem programs are tested by an independent laboratory for glycemic index, to ensure that the overall program is consistent with the GI profile that has been shown to be beneficial for glycemic control, among other benefits. The following graph represents a typical change in blood glucose over two hours when subjects are fed either a low glycemic index Nutrisystem entrée or an equivalent carbohydrate load from high glycemic index white bread. The data suggest slower carbohydrate digestion and absorption with the low glycemic index entrée, resulting in a significantly lower blood glucose concentration. Diets comprised primarily of low glycemic index foods have been associated with better glycemic control, satiety, and body weight management, compared to high glycemic index diets (Brand Miller et al., 2009; Esfahani et al., 2009; Thomas & Elliott, 2009). Conclusions: Managing calorie and carbohydrate intake is the primary intervention to produce weight loss and improve glycemic control in patients with type 2 diabetes. Research suggests combining this approach with a low glycemic diet further supports weight management and glycemic control in patients with type 2 diabetes. The Nutrisystem Program is evaluated to ensure the program is consistent with the GI profile that has been shown to be beneficial for glycemic control, among other outcomes. Efficacy of Behavior Therapy Techniques The NHLBI‟s Clinical Guidelines for the Treatment of Obesity recommend that dietary and physical activity recommendations be packaged with a behavioral intervention (National Heart, Lung and Blood Institute Obesity Education Initiative, 1998). This combined treatment is often referred to as a lifestyle modification program. The key difference between a diet (as commonly defined by patients) and a lifestyle modification program is the intent of the latter to implement reasonable changes that can be sustained indefinitely to promote health (Fabricatore & Wadden, 2003). Behavior therapy (alternatively referred to as cognitive- behavioral therapy in this context) refers to a set of principles and strategies that help patients adhere to their diet and physical activity goals. Such strategies include problem solving, stimulus control, cognitive restructuring, stress management and seeking social support (Fabricatore, 2003; National Heart, Lung and Blood Institute Obesity Education Initiative, 1998). Chief among these strategies, however, is self-monitoring. Self-Monitoring Regular self-monitoring – of food intake, physical activity, and body weight – has become a critical component of behavior therapy for weight management, as several studies have found more favorable weight loss
outcomes among those who self-monitor more consistently. (Baker & Kirschenbaum, 1993; Foreyt & Goodrick, 1994; Foreyt & Poston, 1998). Although food intake is the primary target of self-monitoring, researchers also have investigated the effects of self-monitoring physical activity. In a group of 40 obese, sedentary men and women who were participating in a six-month weight loss program, 43% achieved a consistent level of self-monitoring (Carels, 2005). Those who monitored their activity consistently completed twice as much physical activity each week and lost twice as much weight as those who monitored their activity inconsistently. Body weight also appears to be an important target of self-monitoring. Research on members of the National Weight Control Registry (NWCR), a database of successful dieters (i.e., individuals who have lost at least 30 lb and maintained that reduction for at least 1 year), has identified several behaviors that are characteristic of successful weight losers. One of the earliest studies conducted in the NWCR found that 44% of participants weighed themselves at least once per day and an additional 31% weighed themselves once per week (Klem, 1997). This finding was recently replicated in a larger NWCR sample (Butryn, 2007). NWCR participants reported using self-weighing as an opportunity for positive reinforcement when changes in behavior correspond to weight loss or avoidance of weight gain. Despite the evidence supporting the role of self-monitoring in meeting weight loss goals, achieving a consistent level of self-monitoring can be a significant challenge. Providing individualized, convenient and motivational tools to patients that support self-monitoring activity may enhance self-monitoring adherence. Conclusions: Self-monitoring of food intake, physical activity and weight can help increase self- awareness of target behaviors, illustrate progress towards goals, and serve as a warning system for problems that arise. Consistent adherence to self-monitoring practice at least 75% of the time increases the likelihood of weight loss and weight management success. More than half of people find it difficult to consistently self-monitor. The Nutrisystem Program provides access to both web- based and paper-based self-monitoring tools that have been designed to be motivational and customizable to members‟ individual goals in order to promote adherence to targeted self-monitoring behaviors. Evaluating the Efficacy of Telephone Counseling and Web-Based Behavior Therapy Behavior therapy is typically delivered in individual or group counseling sessions that are held on a weekly to monthly basis. These face to face sessions include a review of patient progress and discussion of methods and strategies to help patients adhere to recommendations for energy intake and physical activity. However, barriers such as program availability, patient proximity, transportation, and time constraints can limit program access and adherence. Current information and communication technologies, specifically web, email and telephone technologies have the potential to overcome these barriers and numerous studies have evaluated the efficacy of the various alternative channels (Wadden et al., 2007). A randomized controlled trial compared the efficacy of an in-person lifestyle modification program (consisting of weekly on-site group sessions) to an internet-based program (consisting of weekly chat room sessions and a variety of web based self-monitoring tools) and a hybrid program (consisting of the internet-based treatment plus monthly in-person group sessions; Harvey-Berino, 2010). The in-person group lost significantly more weight than the internet and hybrid groups (8 kg vs. 5.5 kg and 6 kg, respectively) at 6 months. The largest difference among study groups was perceived social support which was significantly higher for the in-person group. This suggests that social support may be one mechanism by which the in-person format produced superior weight loss. Despite lower mean weight reductions in the internet and hybrid groups, clinically meaningful weight losses were common; 38% of Internet participants and 44% of hybrid participants lost at least 7% of their initial weight. Telephone counseling may also be an alternative to face-to-face interventions. In a randomized trial, participants who received on-site counseling lost significantly more weight (median: 13.7%) at 3 months than those who received telephone counseling (median: 10.4%), but there were no differences between groups at 6
months (medians: 12.6% and 13.0% for the on-site and telephone counseling groups, respectively; Donnelly, 2007). Attrition was lower in the telephone group (26%) than in the on-site group (31%). With regard to weight maintenance, a recent randomized controlled study compared two weight loss maintenance interventions (a personal contact and an interactive technology intervention) with a self-directed control group over a period of 30 months (Svetkey, 2008). Both the personal contact and interactive technology intervention encouraged regular self-monitoring of weight, physical activity and caloric intake. The interactive technology group consisted of unlimited access to a host of online tools, and the personal contact group consisted of monthly 10-15 minute telephone sessions. Randomization into these maintenance programs occurred after a mean weight loss of 8.5 kg over 6 months. The primary outcome observed was change in weight since randomization into maintenance programs. At the end of the study, all groups had regained weight (means of 5.5 kg in self-directed group, 5.2 kg in interactive technology group, and 4.0 kg in personal contact group), however at 24 months both the interactive technology group and the personal contact group had gained significantly less weight (p values = 0.045 and
snacks and desserts) is a key program feature. The emphasis on portion-control is consistent with an approach
that has repeatedly been shown to be associated with improved short term weight loss. In addition, the
Nutrisystem-D program provides self-monitoring tools, physical activity programs, and online/telephonic
counseling consistent with recommendations for diabetes prevention and management.
References
American Diabetes Association. 2010. Standards of Medical Care in Diabetes. Diabetes Care. 33 Suppl:S11-
S61.
American Diabetes Association. 2008. Nutrition Recommendations and Interventions for Diabetes: A Position
of the American Diabetes Association. Diabetes Care. 31 Suppl:S61-S78.
Baker R and Kirschenbaum D. 1993. Self-monitoring may be necessary for successful weight control. Behavior
Therapy 24: 377 - 394.
Boutelle K and Kirschenbaum D. 1998. Further support for consistent self-monitoring as a vital component of
successful weight control. Obesity Research 6: 219-224.
Brand-Miller J, McMillan-Price J, Steinbeck K, Caterson I. 2009. Dietary Glycemic Index: Health implications. J
Am Coll Nutr. 28 Suppl:446S-449S.
Butryn M, Phelan S, Hill J, Wing R. 2007. Consistent Self-monitoring of Weight: A Key Component of
Successful Weight Loss Maintenance OBESITY 15(12):3091-3096.
Carels R et al. 2005. The Relationship Between Self Monitoring, Outcome Expectancies, Difficulties with
Eating and Exercise, and Physical Activity and Weight Loss Treatment Outcomes. Annals of Behavioral
Medicine 30(3):180-190.
Catenacci V, Wyatt H. 2007. The Role of Physical Activity in Producing and Maintaining Weight Loss. Nat Clin
Pract Endocrinol Metab CME 3(7):518-529.
Center for Disease Control and Prevention. 1996. Physical Activity and Health. A Report of the Surgeon
General: http://www.cdc.gov/nccdphp/sgr/pdf/sgraag.pdf
Cheskin et al. 2008. Efficacy of meal replacements versus a standard food-based diet for weight loss in type 2
diabetes: a controlled clinical trial. The Diabetes Educator 34: 118-127.
Curiono CC, Lourenco PM. 2005. Long-Term Weight Loss After Diet and Exercise: A Systematic Review. Int J
Obes 29: 1168-1174.
Ditschuneit et al.,1999. Metabolic and weight-loss effects of a long-term dietary intervention in obese patients.
Am J Clin Nutr 69(2):198-204.
Donnelly JE. 2007. Comparison of a Phone vs. Clinic Approach to Achieve 10% Weight Loss. International
Journal of Obesity 31: 1270-1276.
Esfahani A, Wong JM, Mirrahimi A, Srichaikul K, Jenkins DJ, Kendall CW. 2009. The glycemic index:
physiological significance. J Am Coll Nutr. 28 Suppl: 439S-445S.
Espeland M et al. 2007. Reduction in Weight and Cardiovascular Disease Risk Factores in Individuals with
Type 2 Diabetes: One- Year Results of the Look AHEAD Trial. Diabetes Care 30(6):1374-1383.
Esfahani A, Wong JM, Mirrahimi A, Srichaikul K, Jenkins DJ, Kendall CW. 2009. The glycemic index:
physiological significance. J Am Coll Nutr. 2009 Aug;28 Suppl:439S-445S.
Fabricatore A, Wadden T. 2003. Treatment of Obesity: An Overview. Clinical Diabetes 21(2): 67-72Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in Obesity Among US Adults, 1999- 2000. JAMA 2002;288:1723-27. Flegal KM, Carroll MD, Ogden CI, Curtin LR. Prevalence and trends in obesity among US adults, 1999--2008. JAMA 2010;303:235—41. Foreyt JP, Goodrick GK. 1994. Attributes of Successful Approaches to Weight Loss and Control. Applied and Preventative Psychology 3: 209-215. Foreyt JP, Poston WSC.1998. The Role of the Behavioral Counselor in Obesity Treatment. Journal of the American Dietetic Association, 98(10; Supplement 2): 27-30. Foster et al. 2009. The Effects of a Commercially Available Weight Loss Program Among Obese Patients with Type 2 Diabetes: A Randomized Study. PostGraduate Medicine 121(5). Hannum et al. 2004. Use of Portion Controlled Entrees Enhances Weight Loss in Women. Obesity Reseach 12(3). Hannum et al. 2006. Use of packaged entrees as part of a weight-loss diet in overweight men: an 8-week randomized clinical trial. Diab Obes Metab 8: 146-155. Harvey-Berino J, West D, Krukowski R, Prewitt E, VanBiervliet A, Ashikaga T, Skelly J. 2010. Internet delivered behavioral obesity treatment. Preventive Medicine. 51;123-128. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. 2004. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. JAMA;291:2847-50. Heymsfield et al. 2003. Weight Management Using a Meal Replacement Strategy: Meta and Pooling Analysis from Six Studies. Int J Obs 27: 537-549. Jenkins DJ, Wolever TM, Taylor RH, Barker H, Fielden H, Baldwin JM, Bowling AC, Newman HC, Jenkins AL, Goff DV. 1981. Glycemic index of foods: a physiological basis for carbohydrate exchange. Am J Clin Nutr. 34(3):362-6. Kanfer FH. 1970. Self-monitoring: Methodological limitations and clinical applications. Journal of Consulting and Clinical Psychology 35:148-152. Kirschenbaum DS. 1988. Treating adult obesity in 1988: Evolution of a modern program. The Behavior Therapist, 11:3-6. Kirschenbaum DS. 1992. Elements of effective weight control programs: Implications for exercise and sport psychology. Journal of Applied Sport Psychology 4:77-93. Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO. 1997. A descriptive study of individuals successful at long-term maintenance of substantial weight loss. Am J Clin Nutr, 66:239–46. Ludwig, DS. 2003. The glycemic index: physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA 287(18):2414-2423. National Heart, Lung and Blood Institute Obesity Education Initiative. 1998. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report. US Dept of Health and Human Services. NIH Publication No. 98-4083. National Heart, Lung and Blood Institute. Manage Diabetes: http://www.nhlbi.nih.gov/actintime/rhar/md.htm Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. 2006. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA;295:1549-55.
Svetkey LP, Stevens VJ, Brantley PJ, Appel LJ, Hollis JF, Loria CM, et al. 2008. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA, 299:1139-1148. Thomas D, and Elliott EJ. 2009. Low glvcaemic index, or low glycaemic load, diets for diabetes mellitus. Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No.: CD006296. DOI = 10.1002/14651858.CD006296.pub2. Wadden et al. 2007. Lifestyle modification for the management of obesity. Gastroenterology 132:2226-2238. Yip IAN, Vay Liang W, Go, Deshields S, Saltsman P, Bellman M, Thames G, Murray S, Want HJ, Elashoff R, Heber D. Liquid meal replacements and glycemic control in obese type 2 diabetes patients. Obes Res. 2001;9:341S–347S. Young LR & Nestle M. 2002. The contribution of expanding portion sizes to the US obesity epidemic. American Journal of Public Health 92(2): 246-249.
You can also read