Oral health status, dental needs, habits and behavioral attitude towards dental treatment of a group of autistic children in Riyadh, Saudi Arabia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SAUDI DENTAL JOURNAL SAUDI DENTAL JOURNAL SAUDI DENTAL JOURNAL 132
Oral health status, dental needs, habits and behavioral
attitude towards dental treatment of a group
of autistic children in Riyadh, Saudi Arabia
Ebtissam Zakaria Murshid, BDS, MS, MPH, DrPH
The purpose of the study was to obtain baseline information regarding the oral health status, dental needs, habits and
behavioral attitudes towards dental treatment of a group of autistic children attending a rehabilitation center in Riyadh,
Saudi Arabia. A self-administered questionnaire in Arabic was completed by the parents of each child involved and
was reviewed with the children’s trainers. Extra-oral and intra-oral examinations were performed in 20 autistic
children with a mean age of 9.6 years. The parents of all the 20 children (16 males and 4 females) responded to the
questionnaires. Extra-oral examination showed that 14 (70%) children showed different signs of trauma due to habits
and also expression of temporary madness. Intra-oral assessment showed poor oral hygiene (80%) and generalized
gingiva. The mean DMFT score was 1.6 and 7.25, and mean dmft score for males and females was 3.62 and 1.0,
respectively. Regarding the behavioral attitude to dental treatment, 56.25% of the children were definitely negative,
31.25% were negatively behaved and only 12.5 % reacted positively towards the dental examination. The following
conclusions were made: Oral health status of the examined autistic children did not show statistically significant
differences from the international groups reported in previous studies. Autistic children in the present study showed
similar behavior and habits as other autistic children around the world.
INTRODUCTION of such brain abnormalities might be due
to early prenatal insult such as
Autism, autistic syndrome (AS), autistic chromosomal abnormalities, intrauterine
disorder (AD), infantile autism (IA) and viral infections, and metabolic disorders
childhood autism (CA) are different terms suspected to play a role in the
given to the same condition of a pathogenesis of this syndrome.4
developmental disability. The condition In a recent epidemiologic study
was first described in 1943 by Leo Kanner, conducted in the United States, the
an American child psychiatrist.1,2 Kanner findings show a tremendous increase in
reported his observations of a group of the prevalence of autism between the end
children as they expressed impaired social of the 1980’s and the beginning of the
and behavioral interactions, verbal and 1990’s (1987-1994). The authors of the
nonverbal communication deficiencies, study could not determine if the observed
and developmental retardation.1-3 Later, increase in autism was due to
Kanner’s observations were identified as improvements in detection, changing and
an organic disorder characterized broadening of diagnostic criteria or a true
by abnormalities in the brain structure increase in prevalence. 6 Other
and function, especially the limbic epidemiological studies of autism reported
system and cerebellum. 3-5 Recently, that the main age at which autism was
researchers reported that the etiology diagnosed was 44 months, with a wide
variation of the expression of symptoms
Received 1 April 2005; Revised 13 June 2005
Accepted 20 August 2005 Address reprint requests to :
Assistant Professor Ebtissam Zakaria Murshid
Department of Preventive Dental Sciences P.O. Box 60169, Riyadh 11545, KSA
College of Dentisty, King Saud University, Riyadh, KSA Email : emurshid@ksu.edu.sa
Saudi Dental Journal, Volume 17, No. 3, September - December 2005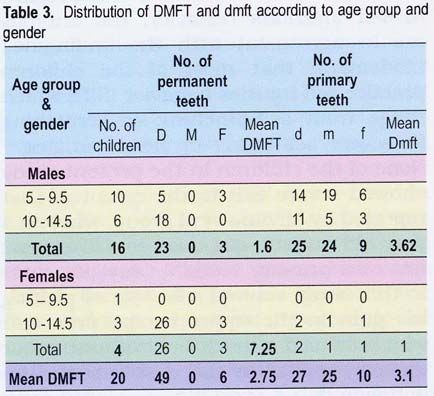
133 ORAL HEALTH STATUS AND BEHAVIOURAL ATTITUDE
among different individuals.3,7,8 Autistic and distribution of Saudi autistic children
children may express mental retardation, is available in brochures and flyers
abnormal emotional, social and linguistic published by various autistic
development, poor muscle tone, poor rehabilitation centers and the Saudi
coordination, as well as visual and hearing Autistic Society which was established in
impairment. 3,9,10 Klein and other 2003. These brochures provide definitions
researchers reported that males are four and some medical characteristics of this
to five times affected more than females, group of children with no information
but more severe symptoms are exhibited about their oral health status or dental
in females.3, 8, 11-13 needs. Recently, Yazbak reported that the
As part of the multiple unknown estimated number of autistic children in
developmental abnormalities, several Saudi Arabia was 42,500.22 However, no
studies reported that up to 70% of the reference was made as to how this
children diagnosed with autism practice estimate was obtained. The purpose of
self injurious behavior (SIB) at some stage this study was to obtain baseline
in their lives. This behavior is expressed information regarding the oral health
as a deliberate harm to the body that may status, dental needs, habits, and
lead to serious injuries without suicidal behavioral attitudes to dental treatment
intent. This repetitive behavior is more of a group of children diagnosed with
common in females, mentally and autism in a non-profit autistic
psychologically impaired individuals.14 It rehabilitation center in Riyadh, Saudi
usually affects the head and neck Arabia.
region.13, 15
Oral health and dental needs of METHODS AND MATERIALS
children with autism have been evaluated
by very few investigators. The studies This study was conducted in the first
conducted on this topic reported no center established in 1999 in Riyadh, the
statistically significant differences in the capital of Saudi Arabia, as indicated by the
prevalence of caries, fillings, gingivitis Saudi Autistic Society’s official website.
and degree of oral hygiene in comparison In Riyadh, there are about six non-profit
with non-autistic individuals8, 16-18 and centers that accept and offer
even a lower incidence of caries in some rehabilitation services for children with
of the reports.19, 20 autism. The center offers an intensive
Because of the widely aberrant rehabilitation program only for children
behavior and communication impairment diagnosed with autism and has 20
of children with autism, every child registered children. All the children (16
requires special behavior management males and 4 females) were included in the
with a great deal of patience and study. All the children had been previously
confidence. 8,17,21 The use of Tell-Show- examined and diagnosed medically as
Feel-Do technique with sedation or autistic patients according to the center’s
nitrous oxide was recommended in the medical records. A self-administered
literature to manage and treat the autistic questionnaire in Arabic was sent to 5 families
child in routine dental settings.21 to pre-test the reliability of the questions. The
An extensive review of the literature questionnaires included demographic
revealed no specific numbers regarding information (name, age and gender of the
diagnosed cases of autistic children in child), child’s oral hygiene practice, previous
Saudi Arabia. Most of the estimated dental experience, behavior during dental
infor m a t i o n a b o u t t h e p r e v a l e n c e examination and treatment, and habits
Saudi Dental Journal, Volume 17, No. 3, September - December 2005
MURSHID 134
including self injurious behavior. The (e.g. ulcer, abscess). Oral hygiene was
habits and behavioral patterns of every recorded as good, fair or poor according to
child were reviewed with the children’s the Simplified Oral Hygiene Index (OHI-
trainer. Every family was assured of the S).25
confidentiality of the collected data and The collected data were entered in the
that the resultant information would be computer using Statistical Package for
used only for the research purposes. Social Sciences (SPSS version 10)
Files of all the children were reviewed software for frequency distribution of all
and the medical status of each child was variables.
recorded in a special clinical examination A report of each child’s oral health and
form designed for this study. On the day dental needs as well as any special
of examination, each child accompanied instructions to improve the oral hygiene
by his/her trainer was brought to the of the child was sent to the parents.
designated examination room and was
informed by his/her trainers about the
RESULTS
procedure, and asked to cooperate with the
examiner. The children were seated on
an adjustable office chair or laid down flat The parents of all the 20 children, 16
on an exercise mattress depending on (80%) males and 4 (20%) females with a
mean age of 9.6 years participated in the
their physical condition.
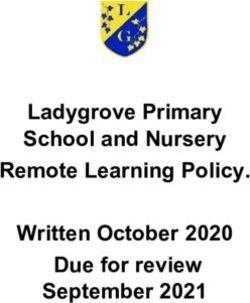
study. Results of the extra oral
During the examination procedure, the assessment, types of habits, trauma and
“Tell–Show–Feel and Do” technique was injuries as well as the given reasons are
used with all the children. Extra-oral shown in Table 1. Out of the 20 examined
examination included any scars, trauma children, 14 (70%) showed signs of
to the head and neck, hands and fingers. trauma. The injuries varied from
Intra-oral examination of the soft and hard scratches to one case of burned fingers.
tissues was done under flash light and Five males and one female had no signs
regular room light using disposable gloves, of trauma or injuries in the examined
mouth mirror, explorer and sterilized areas (Table 1).
gauze to clean and dry the teeth. Sound, Injuries to the head region were
decayed, missing and filled teeth were recorded in 6 (30%) of the children (4 males
recorded in the dental chart following the and 2 females) and it was due to self head
WHO criteria.23 banging on the walls and furniture, and
The gingival status was evaluated hitting by bare hands or with objects
according to the gingival index of Loe and during stressful moments or as
Silness (1963) which varied between mild expression of temporary madness and
(slight changes in color and texture) to discomfort. Three other children (15%)
moderate gingivitis (redness, edema, and showed signs of scratches on the sides of
bleeding on pressure).24 No probing or their faces due to head banging and hair
pocket depth measurement was conducted pulling.
to evaluate the periodontal health due to The most common trauma was recorded
the difficult behavior of the children. in the hands and fingers, as 15 (75%) of
Gingival status was recorded as the children (11 males and 4 females)
generalized or localized gingival showed different degrees of injuries. The
inflammation depending on the amount reasons given were repeated self biting
of gingival redness and bleeding during habit and touching hot beverages or food.
the examination. The examination also A 10-year old male had shown signs of
included any intra-oral soft tissue findings localized gum recession in the upper
Saudi Dental Journal, Volume 17, No. 3, September - December 2005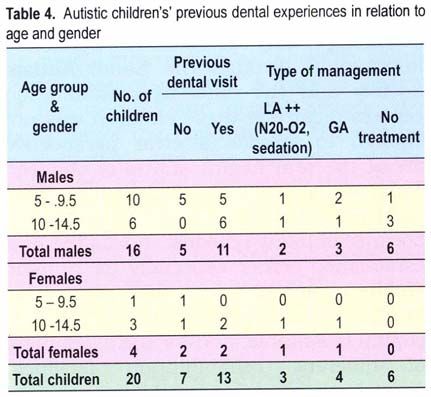
135 ORAL HEALTH STATUS AND BEHAVIOURAL ATTITUDE
children showed that, 16 (80%) of the
children (14 males and 2 females) had poor
oral hygiene. Only 4 (20%) of the children
(2 females and 2 males) showed fair oral
hygiene and none had good oral hygiene
(Table 2).
The gingival status was evaluated and
the results showed that all the children
had mild generalized gingivitis. Four of the
males and two of the females showed
gingival dryness and redness in the upper
front areas which could be due to mouth
breathing and/or open bite (Table 2).
Two males and two females were
considered as having fair oral hygiene.
The trainers as well as the parents
reported that these children do not mind
brushing their teeth and sometimes they
are able to brush by themselves. Difficulty
in practicing oral hygiene was reported by
the trainers and parents in males more
than females and in the older age group
(9 years and above). Four males and 2
females had clear protrusion of the upper
jaw associated with a mouth breathing
anterior region due to repeated picking habit. The results are illustrated in Table
with his nail. Another male reported that 2.
he had a habit of pinching himself and the
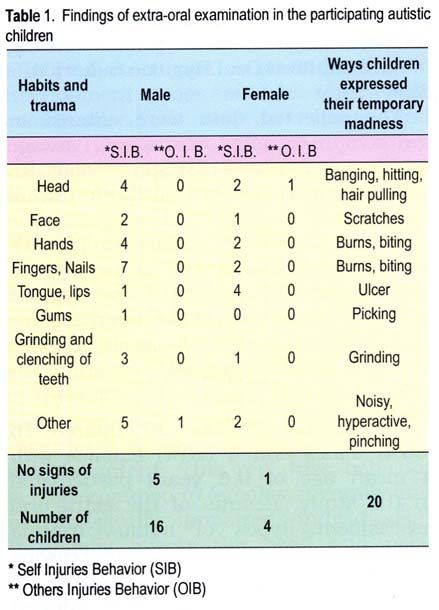
The hard tissue assessment showed
others when he was angry. Two of the
that thirteen children (65%) had multiple
females and one male children showed
decayed and untreated teeth (49
signs of ulcers in the lips and tongue
permanent and 27 primary). Only 6
regions which were difficult to diagnose
children (30%) had fillings in their teeth
as either traumatic or aphthous ulcers
(6 permanent and 10 primary), and five
(Table 1).
children (25%) showed no signs of clinical
The parents of the 6 (30%) children with decay or fillings. The mean DMFT score
no signs of trauma reported that their was 1.6 and 7.25, whereas, the mean
children do not practice self injury habits.
On the other hand, four of the males
expressed their anger with peculiar
repetitive hand movements and
hyperactivity without hurting themselves
or the others. The rest of the children had
repeated habits which were similar to
those of normal children such as nail
biting, grinding of teeth at night (Table 1).
The soft tissue assessment which
included evaluation of oral hygiene and
gingival status of the participating
Saudi Dental Journal, Volume 17, No. 3, September - December 2005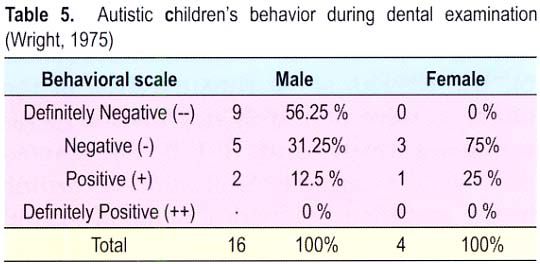
MURSHID 136
dmft was 3.62 and 1.0 for the males Regarding the behavior of the children
and females, respectively. The overall during the dental examination (Table 5),
means DMFT was 2.75 and the dmft was the results show that 9 (45%) of the
3.1(Table 3). children were definitely negative, 8 (40%)
were negatively and 3 (15 %) reacted
positively to dental examination according
to the modified behavioral scale of Frankl
and Wright.26 The children showed a great
a mount of fear towards the dental team
and a great resistance to the clinical
examination which was observed more in
the males than in the females.
Parents’ responses to the questionnaire
regarding dental visits (Table 4) indicated
that 13 (65%) of the children had been to
a dental clinic and had history of
treatment and follow up while 7 (35%)
other children did not make any previous
dental visits. Six of the thirteen families
who went for dental appointments had
tried several times but they faced great
difficulty with their children and only
minimum or no treatment could be The use of “Tell-Show-Feel and Do”
performed under regular dental setting. technique was not effective with the
This made the parents hesitant to take majority (85%) of the children even with
their children to the subsequent the trainers’ help and the introductory
appointments. Only seven children had visit of the team members to the center
managed to receive dental treatment, four before the day of the clinical examination.
were treated under General anesthesia The children were brought to the room
and 3 children were treated under local with their trainers and each one of them
anesthesia with nitrous oxide and was informed by his/her trainers about
physical restraint. The parents of the the procedure and asked to cooperate.
seven (35%) children who had never been During the clinical examination, the
to a dental clinic attributed this to their children were resisting and fighting,
children’s difficult behavior and lack of refusing to open their mouths. Only 3
compliance even during homecare. This children (2 males and one female) showed
led the parents to believe that nobody could positive behavior and they were willing to
manage to treat their children and so they open their mouths for only short periods
depended on home dental care only. of time without too much resistance.
Saudi Dental Journal, Volume 17, No. 3, September - December 2005137 ORAL HEALTH STATUS AND BEHAVIOURAL ATTITUDE
group showed more males registered in
the center than females, which might
reflect the higher prevalence of autism
in males as it was reported in other
studies around the world.3,12 With regard
to self injurious behavior, the findings are
in agreement with the findings of
Lindemann that most of the children
practice self injuries behavior (SIB) which
DISCUSSION range from self-pinching or scratching to
severe self-biting or head banging.27 None
The need for baseline information of the children in the present study
regarding the oral health status of showed severe SIB to the extent of that
children with autism in Saudi Arabia is reported by Medina et al group, where a 4
becoming clearly essential. The published year old autistic girl used to self extract
information through the Saudi Autism her own primary teeth.13 Only one male
Society and the different rehabilitation in this study showed a history of picking
centers regarding these children was not his gum in the upper canine area and
enough to provide a clear perspective which caused a mark but without major
about the oral health status of children damage similar to the case reported by
with autism in Saudi Arabia. This Johnson.28
particular autistic center was chosen The results of the gingival status of the
because of many reasons. It was the first children showed that all the children had
established center especially for autistic generalized gingivitis which could be
children in Riyadh, the geographic location related to many reasons such as the
in the middle of Riyadh the capital is irregular brushing habits because of the
suitable, and for the availability of difficulties the trainers and the parents
different rehabilitation facilities, special encountered when they brushed the
education certified trainers, and the children’s teeth. It could also be due to
range of the children’s age groups in lack of the necessary manual dexterity of
addition to the principal trainers and autistic children during brushing by
parents’ cooperation, the choice of the themselves, which made their tooth
center was appropriate. brushing inefficient. Furthermore, the
The history of scars and trauma findings of this study reflect poor dental
obtained during the clinical examination awareness, a lack of dental education and
was cross-checked with the parents’ deficiency in receiving oral hygiene
response for any possible findings of child instructions from dental staff. Care-givers
abuse or child neglect. The results showed need to know the different techniques
that all the scars or signs of trauma were and materials of tooth brushing with
due to repeated self injuries according to emphasis on behavior modification to
the parents’ report which was in harmony control the behavior of the children as well
with the trainer’s response. as diet control and regular dental visits.
The results of this study showed Another possible explanation of the
some similarities and differences in presence of generalized gingivitis might
oral health status, dental needs and be the side effects of medications used
behavior of this group of Saudi autistic to control the manifestations of
children when compared to other autistic autism. Examples are hyperactivity
children around the world. The studied (methylpheniadate), repetitive behaviors
Saudi Dental Journal, Volume 17, No. 3, September - December 2005MURSHID 138
(fluoxetine, sertraline, and pimozide) and The difficulties in controlling children
aggressive behaviors (lithium, valproate). with autism were reflected in the results
Although, the long term effects of of the previous dental experience where
instituting these medications in young nitrous oxide, physical restrain and
children remain unknown, it is reported general anesthesia were used to control
that these antidepressants inhibit certain the children’s behavior. The findings also
metabolic pathways and certainly have show that most of the children had
different side-effects.29 It is essential that negative to definitely negative reaction to
every dentist dealing with autistic the examination which was conducted
children should be familiar with the within an area familiar to them and
manifestations of the condition and its among their trainers. Our findings were
associated features and should be familiar in agreement with other studies
with the used medications to evaluate any conducted in the western world by Klein
possible side effects that may cause and Backman.3, 8
untoward orofacial and systemic reactions Therefore, it is important to obtain as
or precipitate adverse interaction with much information as possible about every
dental therapeutic agents. Even for the case of autism. A careful review of the
four children who were reported to be medical and dental history, the behavior
cooperating with the daily brushing they of the child during the clinical
had generalized gingivitis because they examination and the behavior of the child
were brushing only once a day and 3 of in general are essential. More studies
them had protrusion and incompetent lips. should be conducted about children with
This made them mouth breathers causing autism in Saudi Arabia. The studies
gingival inflammation especially in the should include the rest of the
upper anterior areas. rehabilitation centers around the country
Regarding the caries prevalence of this to provide better information regarding
autism in the Kingdom.
group of children, the results showed that
the mean dmf, and DMF for all the subjects
were 3.1 and 2.75, respectively. This level CONCLUSIONS
of dental caries is considered moderate
according to the WHO classification.23 It The findings of this study are limited to
would not be accurate to compare the one rehabilitation Center in Riyadh and to
results of the male and female subjects the convenient sample size; consequently
separately due to the small number of the results should be interpreted
female subjects in the study, but accordingly. Therefore, within the limits of
comparing the results of all the subjects the present study design, the following
with other studies conducted with different conclusions could be made:
groups of healthy children in Riyadh (dmft
= 5.0) area show a lower caries prevalence • The oral health status of the autistic
in the autistic study group.30 This finding children did not show significant
would be in agreement with Karmen and differences from the international
groups reported in the previous
Kopel findings who reported lower caries
studies.
prevalence in autistic children. 19, 20
However, the differences observed in • The autistic children in this study
caries prevalence can not be generalized showed similar repetitive behavior and
because of the convenience sample of self injuries habits as other autistic
children. children reported around the world.
Saudi Dental Journal, Volume 17, No. 3, September - December 2005139 ORAL HEALTH STATUS AND BEHAVIOURAL ATTITUDE
REFERENCES to undergo dental examination. ASDC J
Dent Child 1985; 3:29-35.
1. Kanner L. Autistic disturbances of effective 17. Shapira J, Mann J, Tamari I, Mester R,
contact. Nerv Child 1943; 2:217-250. Knobler H, Yoeli Y, Newbrun E. Oral health
2. Kanner L. Early infantile autism. J Pediatr status and dental needs of an autistic
1944: 25:211-217. population of children and young adults.
3. Klein U. Autistic disorder: A review for the Spec Care Dentistry 1989; 9:38-41.
pediatric dentist. Pedia Dent; 1998 18. Fahlvik-Planefeldt C, Herrstrom P. Dental
20(5):312-317. care of autistic children within the non-
4. Minshew NJ. Brief report: Brain specialized Public Dental Service. Swed
mechanisms in autism: functional and Dent J 2001; 25(3):113-118.
structural abnormalities. J Autism Dev 19. Kopel HM. The autistic child in dental
Disord 1996; 26:205-209. practice. ASDC J Dent Child 1977; 44:302-
5. Baumann ML. Brief report: Neuroanatomic 309.
observations of the brain in pervasive 20. Karmen S, Skier I. Dental management of
developmental disorders. J Autism Dev the autistic child. Spec Care Dentist 1985;
Disord 1996; 26:199-203. 5:20-23.
6. Croen LA. Crether JK, Hoogstrate J, Selvin 21. Braff MH, Nealon L. Sedation of the autistic
S. The changing prevalence of autism in patient for dental procedures. ASDC J
California. J Autism Dev Disord 2002;
Dent Child 1979; 46(5):404-407.
32:207-215.
22. Yazbak FE. Autism seems to be increasing
7. Smith B, Chung MC, Vostanis P. The path
worldwide, if not in London. BMJ 2004,328:
to care in autism: is it better now? J Autism
Dev Disord 1994; 24:551-563. 226-227.
8. Backman, Pilebro. Visual pedagogoy in 23. Barmes DE. Indicators for oral health and
dentistry for children with autism. ASDC their implications for developing countries.
J Dent Child 1999; 325-331. Int Dent 1983; 33:60-66.
9. Ornitz EM, Ritvo ER. The syndrome of 24. Loe H, Silness J. Periodontal disease in
autism: A critical review. Am J Psychiatry pregnancy. I. Prevalence and severity. Acta
1976; 133(6)609-621. Odont Scand 1963;21:533-551.
10. Gillberg C, Coleman M. The biology of the 25. Greene JC, Vermillion JR. The simplified
autistic syndromes. Lavenham: Lavenham oral hygiene index. J Am Dent 1964; 68:7-
Press Ltd., 1992 ISSN: 0069-4835. 13.
11. American Psychiatric Association. 26. Wright GZ. Behavior management in
Diagnostic and statistical manual of dentistry for children. Philadelphia: W.B.
mental disorders: DSM-IV, 4th ed. Saunders Co., 1975.
Washington, DC 1994; pp. 66-71. 27. Lindemann R, Henson JL. Self-injuries
12. Rapin I. Autism in search of a home in the behavior: Management for dental
brain. Neurology 1999; 52:902-904. treatment. Spec Care Dentist 1983; 3:72-
13. Medina AC, Sogbe R, Gomez-Rey Am, Mata 76.
M. Factitial oral lesions in an autistic 28. Johnson CD, Matt MK, Dennison D,
paediatric patient. Int J Paediatr Dent
Brown RS, Koh S. Preventing factitious
2003; 13(2):130-137.
gingival injury in an autistic patient. AJDA
14. Saemundsson SR, Roberts M. Oral self-
1996; 127:244-247.
injurious behavior in the developmentally
29. Friedlander A, Yagiela J. The
disabled: Review and case. J Dent Child
1997; 64(3):205-209. pathophysiology, medical management,
15. Vogel LD. When children put their fingers and dental implications of autism. CDA J
in their mouths. Should parents and 2003; 31:681-691.
dentists care? NY State Dent J 1998; 64 30. Al Dosari A, Abdulatif H, Al Refai A. Oral
(2): 48-53. health status of primary dentition among
16. Lowe Q, Lindemann R. Assessment of the 551 children aged 6-8 years in Jazan, Saudi
autistic patient’s dental needs and ability Arabia. Saudi Dent J 2000; 12(2): 67-71.
Saudi Dental Journal, Volume 17, No. 3, September - December 2005You can also read