Our Choices Our Voices - Australian Human Rights Commission
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Our Choices
Our Voices
A report prepared by the Lowitja Institute for the Close the Gap Steering Committee | March 2019
OUR VOICES, OUR CHOICES. | i
Contents
Acknowledgements
This report is a collaborative
effort of the Close the Gap
Campaign Steering Committee.
Funding for the report was provided Foreword...............................................................................................1
by Oxfam Australia.
Authors: The Lowitja Institute Introduction...........................................................................................2
Consulting team: Mary Guthrie,
Tahlia Eastman, Leila Smith, Romlie
Mokak PRIORITY THEME 1
Editors: Mary Guthrie,
Targeted, Needs-based Primary Health Care 6
Tahlia Eastman, Romlie Mokak Birthing on Country Project ...................................................................................7
Cristina Lochert, Fiona Walls
Institute for Urban Indigenous Health – Inner City Referral Service......................9
Design and Layout: Hyve Design
Family Wellbeing Empowerment Program for Young Aboriginal Men.................11
Printing: Indigi-Print
Published by: The Close the Gap
PRIORITY THEME 2
Campaign Steering Committee
Responsive Health Care System 13
@ Close the Gap Campaign
Steering Committee for Northern Territory Aboriginal Health Academy Project........................................14
Indigenous Health Equality, 2019
Health System Reform – Winnunga Prison Health Service.................................16
This work is licensed under the Anaemia Prevention Program, Katherine East, Northern Territory......................18
Creative Commons Attribution
– NonCommercial – ShareAlike IndigiLez Leadership and Support Group............................................................20
2.5 Australia License. To view a
copy of this license, visit: http://
PRIORITY THEME 3
22
creativecommons.org/licenses/
by-nc-sa/2.5/au or send a letter to Good Housing for Good Health
Creative Commons, 171 Second
Yawuru Home Ownership Program......................................................................24
Street, Suite 300, San Francisco,
California, 94105, USA. Torres Strait Island Regional Council....................................................................26
Copies of this report and more Mununjali Housing and Development Company Ltd...........................................27
information are available to
download at: www.humanrights.
gov.au/social_justice/health/ Endnotes.............................................................................................28
index.html and www.antar.org.au/
close-gap Acronyms and Abbreviations..............................................................32
Cover Photo: Smoking Ceremony,
Welcoming Waminda Goodjaga’s
on Yuin Country. L–R; Gemmah
Floyd, Elizabeth Luland, Patricia
De Vries and their babies. Photo
by Jerusha Sutton Photography;
courtesy Waminda South Coast
Women’s Health and Welfare
Aboriginal Corporation.
Aboriginal and Torres Strait Islander people should be aware that this document may
contain images or names of people who have since passed away.
ii | OUR VOICES, OUR CHOICES.
Foreword
It is of great concern to us, the Close the Gap
Campaign—as indeed it should be to the Australian
nation—that the target to close the gap in life
expectancy between Aboriginal and Torres Strait
Islander people and non-Indigenous people by 2031 is,
in 2019, widening rather than closing.1 In his Closing
the Gap Report 2019 to Parliament, the Prime Minister
acknowledged that this target is not on track.2
In the past, we have provided a ‘Shadow Report’ including a ten-year review
published in 2018. The review assessed the most significant national effort to
date to improve Aboriginal and Torres Strait Islander health—the 2008 Council
of Australian Governments’ (COAG) Closing the Gap Strategy—with its target
to achieve life expectancy equality by 2030.3
In 2019, the Campaign is taking a different approach to its report. After
identifying what we believe are urgent priority themes for addressing the
health gap, this year we are highlighting stories that illustrate success from
Aboriginal and Torres Strait Islander perspectives. The report addresses the
following three priority themes:
• Targeted, needs-based primary health care
• Responsive health care system
• Good housing for good health.
The stories profiled in this report demonstrate that when Aboriginal and Torres Ms June Oscar AO
Strait Islander people are involved in the design of the services they need, we Aboriginal and
are far more likely to achieve success. These stories illustrate that ‘our choice Torres Strait Islander
and our voice’ are vital if we are to make gains and start to close the gap. Social Justice Commissioner
The Campaign welcomes the announcement in December 20184 that
Mr Rod Little
governments will work in true partnership with Aboriginal and Torres Strait
Co-Chair
Islander peoples, and their appropriate organisations and representatives.
National Congress of
This is a critical time for the government to work hand-in-hand with us on
Australia’s First Peoples
solutions, to ensure we turn this gap around and do not allow it to widen any
further.
Co-chairs - Close the Gap
Finally, as Co-Chairs, we sincerely thank the almost fifty Close the Gap Campaign
Campaign members for their contribution to this work. We could not do
what we do without the enduring support and commitment to better health
outcomes from our membership.
OUR VOICES, OUR CHOICES. | 1
Introduction
To address the widening life expectancy gap between
Aboriginal and Torres Strait Islander people and non-
Indigenous Australians, we have identified three priority
areas that must be addressed. We have illustrated
what success looks like in these areas, from varying
Aboriginal and Torres Strait Islander perspectives, via
stories that highlight Aboriginal and Torres Strait Islander
voices and leadership.
The three areas of focus for this The overriding principle throughout
year’s report are: the stories is that the success
of these initiatives is based on
• Targeted, needs-based community governance and
primary health care leadership, which is imperative
• Responsive health care system to the success and longevity of
the programs. The stories also
• Good housing for good health. highlight the importance of cultural
FIGURE 1:
Gap between Indigenous and non-Indigenous life expectancy5
Gap between indigenous Gap between indigenous
and non-indigenous Males and non-indigenous Females
10.2 2001-2005 9.6
10.2 2006-2010 10
10.8 10.6
2011-2015
2 | OUR VOICES, OUR CHOICES.
determinants of health such as health and wellbeing. Overcrowded
strength, resilience, identity and and unhealthy housing is a major
importantly—self-determination. factor in the spread of diseases
and a strong contributing factor to
Aboriginal Community Controlled poor health, especially in young
Organisations (ACCOs) are an children. Again, as recommended in
essential success component of the our ten-year review, the Campaign
provision of holistic, affordable and sees it as vitally important to have
appropriate primary health care for a national, overarching health
Aboriginal and Torres Strait Islander infrastructure and housing plan to
people. ACCOs have a proven track address this need.
record in delivering effective and
cost-efficient primary health care. The Campaign welcomed the 2018
We, the Campaign, continue to Council of Australian Governments
urge investment in targeted, needs- (COAG) decision to establish formal
based comprehensive primary partnership arrangements between
health care. This is essential in COAG and Aboriginal and Torres
addressing the unacceptable health Strait Islander peoples through
disparities between Aboriginal and their peak bodies on Closing the
Torres Strait Islander and non- Gap.6 We support the work of the
Indigenous Australians. We strongly Aboriginal and Torres Strait Islander
support increased investment in peak bodies in their negotiations
ACCOs to increase the quality and with governments on the details
accessibility of culturally sensitive of the partnership. This will be an
and appropriate health care where it historic agreement and, if we get it
is needed most. right, Aboriginal and Torres Strait
Islander people will have shared
We call for governments to commit decision-making in the design,
to an Australian health care system implementation, monitoring and
that is responsive to the needs of review of Closing the Gap policies
Aboriginal and Torres Strait Islander and programs for the first time.
peoples. This means building a
robust, equitable and transparent The establishment of a Joint COAG
health care system where and Aboriginal Torres Strait Islander
institutional racism is acknowledged Council on Closing the Gap7 has
and addressed; where cultural the potential to be a significant
safety training is recognised milestone in the relationship
and valued as an important step between governments and
in closing the gap; and where Aboriginal and Torres Strait Islander
Aboriginal and Torres Strait Islander peoples and is a much-needed step
people are integrated in to health to make the necessary gains to
professions across workforce. close the gap.
Health and housing are inextricably There are many Aboriginal and
linked. It has long been understood Torres Strait Islander individuals
that housing is a significant and organisations whose everyday
determinant of Aboriginal and work is improving health outcomes.
Torres Strait Islander peoples’
OUR VOICES, OUR CHOICES. | 3
We urge governments to take peoples and communities, including
advantage of this important our young people.
source of leadership, expertise,
Importantly, the stories also reflect
guidance and networks, and to
the principles of the United Nations
recognise how these valuable
Declaration on the Rights of
qualities contribute towards the
Indigenous Peoples. They affirm the
success of programs included in
unique contribution that Aboriginal
this report and beyond.
and Torres Strait Islander peoples
This report draws on Aboriginal make to the diversity and richness
and Torres Strait Islander-designed of civilisations and cultures and
and led initiatives. The stories promote cultural diversity and
demonstrate enormous diversity in understanding.
the way Aboriginal and Torres Strait
The Campaign’s work is grounded
Islander peoples are making things
in a human rights approach to
work in our communities, tailored
health. We are committed to
for local aspirations and goals.
harmonious relations—based on
It is important to note that what
partnership, engagement and
works well in one community may
cooperation—between states and
not replicate in other communities.
Indigenous peoples, as well as
However, the principle of self-
mechanisms to support this at
determination must apply, and
national and international levels.
acknowledge that Aboriginal and
Torres Strait Islander peoples Working in genuine partnership
know what works for our own means that governments and
lives, families and communities. agencies must understand that
Success in this context means that Aboriginal and Torres Strait
Aboriginal and Torres Strait Islander Islander peoples have a deep
peoples have created, designed and and long-standing appreciation
implemented our own solutions, in of the issues and the solutions
our voice and choices. related to our health and wellbeing.
Governments have been attempting
The stories featured in this report
to resolve these issues, broadly,
were obtained through a referral and
for decades, and more specifically
a highly engaged interview process;
through the 2008 Closing the Gap
they highlight programs at various
targets. Aboriginal and Torres
stages of implementation.
Strait Islander people witness the
Throughout the interviews, we constant turnover in governments
heard repeatedly that insecure and agency arrangements, and the
and insufficient funding is a consequent changes in policy and
significant limitation to longer-term program approaches – not always
success. This confirms what the for the better. Funding cuts and
Campaign has always identified: freezes have a debilitating effect on
that funding limitations, especially effective delivery of programs and
where funds are not directed to services.
services delivered and designed by
It is critically important that
Aboriginal and Torres Strait Islander
governments commit to this matter
people, compromise the health,
beyond rhetoric. This can be
wellbeing, and the lives of our
4 | OUR VOICES, OUR CHOICES.achieved through closer alignment supporting Aboriginal and Torres
between words and actions. Strait Islander led initiatives and a
Aboriginal and Torres Strait Islander commitment to working in genuine
people can lead this process, with partnership, governments can
genuine support from governments. address this critical health policy
challenge for a population of 3
The Campaign remains committed per cent of Australia’s citizens. We
to addressing health outcomes for believe it is a matter of significant
Aboriginal and Torres Strait Islander urgency for the Australian nation.
people. We are optimistic that, by
The position and the work of the
Close the Gap Campaign is underpinned
by the following principles:
The Campaign is underpinned by a human rights approach
The Campaign believes that self-determination is a defining
factor in improving health outcomes, and that this should be
reflected in all efforts to close the gap
The Campaign reaffirms the recommendations of the 2018
Close the Gap Ten-Year Review to reset the future approach
to the Federal Government’s Closing the Gap strategy.
The Campaign fully supports The Uluru Statement from
the Heart (Uluru Statement), which resulted from wide and
meaningful dialogues across Aboriginal and Torres Strait
Islander communities in Australia
The Campaign is committed to empowering Aboriginal
and Torres Strait Islander voices, including calling for
an Indigenous representative voice to Parliament as
recommended in the Uluru Statement
OUR VOICES, OUR CHOICES. | 5PRIORITY THEME 1
Targeted, Needs-based
Primary Health Care
Aboriginal and Torres Strait Islander people have
a right to access the health care we need, in the
location we choose.
Yet, the life expectancy gap is widening, not closing8 and health
and wellbeing statistics are alarming. For example, the data
pointing to suicide rates,9 a burden of disease at 2.3 times that
of the non-Indigenous population,10 and chronic disease such as
diabetes,11 continue to be of serious concern to the Campaign.
We stand by the recommendations made in the ten-year review
and we remain committed to working with all governments to
achieve health equity for Aboriginal and Torres Strait Islander
peoples.
Aboriginal community controlled organisations are an essential
component of the provision of holistic, affordable and
appropriate primary health care to Aboriginal and Torres Strait
Islander peoples.
ACCOs provide holistic and comprehensive services, both
designed and led — by the community — for the community.
Services and programs include treatment and management,
prevention and health promotion, as well as addressing the
social and cultural determinants of health.
The stories that follow are representative of and designed
for local need. They are not always transferrable between
communities; however, some elements could be applied across
the country, and internationally. For example, the Institute for
Urban Indigenous Health (IUIH) Inner City Referral Service could
be seen as a potential model for cities and towns, adapted as
needed for individual settings.
Throughout this report, each story shares a common strength in
leadership, initiation and design by Aboriginal and Torres Strait
Islander peoples and incorporate our voices and choices. The
programs reflect the diversity of ACCOs measures of success
and echo the need for community control, with each story
highlighting how these measures have influenced the success of
their respective programs.
6 | OUR VOICES, OUR CHOICES.TARGETED, NEEDS-BASED PRIMARY HEALTH CARE PRIORITY THEME 1
Birthing on Country Project
The Birthing on Country While there is a long history of
Aboriginal and Torres Strait Islander
A metaphor
Project provides Aboriginal led birthing programs, the Birthing for the best
and Torres Strait Islander on Country Project is currently
women access to culturally piloting two programs in Australia: start in life.
and clinically safe, inclusive • South East Queensland in Birthing on Country
collaboration with Indigenous Workshop Report 201212
care that incorporates Urban Health Institute and
cultural birthing traditions Aboriginal and Torres Strait
within mainstream Islander Community Health
Services Brisbane, and
maternity services.13
• Nowra, New South Wales,
It was established by the Congress alongside Waminda South Coast
of Aboriginal and Torres Strait Women’s Health and Welfare
Islander Nurses and Midwives Aboriginal Corporation.
PHOTO: Smoking Ceremony; Welcoming
(CATSINaM), the Australian College Waminda Goodjaga’s on Yuin Country Mum
The Birthing on Country Project
for Midwives (ACM), and members and Bub; Elizabeth Luland & Nat McLeod;
develops the Aboriginal and photo by Jerusha Sutton Photography;
of the University of Sydney and
Torres Strait Islander workforce by courtesy Waminda South Coast Women’s
University of Queensland. Health and Welfare Aboriginal Corporation
OUR VOICES, OUR CHOICES. | 7PRIORITY THEME 1 TARGETED, NEEDS-BASED PRIMARY HEALTH CARE
offering a culturally safe workplace pregnancy. She also said that treated like a woman expecting
with opportunities for growth.14 having her second child using the a baby, and not a person with an
Aboriginal and Torres Strait Islander program was much easier, feeling illness’.
Health Workers in support roles confident knowing she had full
have options to upskill at the first support from the Aboriginal and A common thread shared by
Aboriginal and Torres Strait Islander Torres Strait Islander midwives participants was that the success
Birthing Centre in Nowra — set to and health workers: ‘The Birthing of the birthing programs was due
commence construction in 2020. Program is built on a background of to the leadership and ongoing
understanding – the Aboriginal and development by Aboriginal and
‘I’m aware of Aboriginal and Torres Torres Strait Islander midwives and Torres Strait Islander people.
Strait Islander health workers who health workers understood my family Program stakeholders felt that one of
have enrolled in a Bachelor of background and became my friends the main barriers of non-Indigenous
Midwifery since there is a guarantee during the process.’ led birthing programs was that they
that identified roles for Aboriginal operate out of a mainstream hospital
and Torres Strait Islander people will Accessible birthing programs or health service, making the
be available with the new Birthing increases the likelihood of process less culturally safe.
Centre opening in Nowra’ said Aboriginal and Torres Strait
Cherisse Buzzacott, an Aboriginal Islander women who were once The opening of the Nowra
midwife working with the ACM. cautious, didn’t feel comfortable, Aboriginal Birthing Centre is set to
Cherisse also commented that or refused to present at be ground-breaking. It will create
working for communities that are mainstream services, to now opportunities for Aboriginal and
driven and passionate fires her up. access complete care and feel Torres Strait Islander mothers to
‘It has been fulfilling to see how the culturally safe knowing that this experience holistic care outside
program has progressed in the past program nurtures individual needs mainstream services; it will expand
12 months, with the community in from the beginning of pregnancy the Aboriginal and Torres Strait
Nowra independently coming up to the end. Islander workforce; and will utilise
with ideas to ensure the program the skills and leadership found in
launches successfully.’ Hayley Longbottom used the Mums Aboriginal community controlled
and Bubs Birthing Program run by health services. The experience and
Karina Hogan, who participated Waminda and told us how ‘knowing hopes of participants and workers,
in the Birthing in Our Community that when I was to become a mum voiced by Karina, is that the Birthing
Program in Queensland, said that again, my experiences from my on Country project ‘is the bridge to
the program made her feel prepared previous children was going to be giving babies the best start in life’.
about what to expect for her first different. I was comfortable, I was
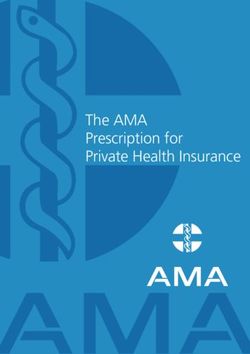
FIGURE 2:
Maternal and infant health outcomes of women in a Birthing on Country Program compared to Aboriginal and Torres
Strait Islander women nationally, ANC = antenatal care, graph taken from Birthing on Country case study.15
100 Aboriginal and Torres Strait
90 Islander women nationally 2013
80
Birthing on Country women 2013
70
Percentage
60
50
40
30
20
10
0
ANC in 5+ ANC Visits Casarean Low birth Preterm Neonatal
1st Trimester (babiesTARGETED, NEEDS-BASED PRIMARY HEALTH CARE PRIORITY THEME 1
Institute for Urban
Indigenous Health
– Inner City Referral Service
The Institute for Urban empathy. He said he ‘loves being
Indigenous Health’s (IUIH)
able to work with mob who may It works
because its
require extra support initially but
Inner City Referral Service who grow to be able to advocate for
(ICRS) is an outreach themselves and seek appropriate
supports and services as need
run for Mob
service that supports arises. Seeing someone who has by Mob.
Aboriginal and Torres Strait never had a place of their own obtain
and maintain their own housing and Randall Frazer, Team Leader
Islander people who have linking someone who hasn’t received
alcohol, tobacco and other any support for their health issues
drug and/or mental health with the appropriate continuing care
is very rewarding’.
and/or chronic health
As with many Aboriginal and
issues, living within a five-
Torres Strait Islander services, lack
kilometre radius of the of secure funding is a barrier to
Brisbane GPO. sustainable service delivery. With
extra funds and certainty of funding,
The program utilises a number ICRS could more effectively meet
of approaches – intensive case community needs. Other barriers to
management, assertive outreach greater success include the inability
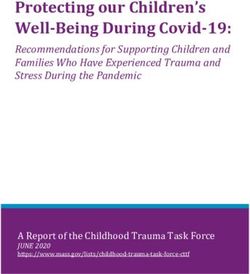
to provide brokerage and co- FIGURE 3:
and strengths-based, community Homelessness, Queensland, 2016 Census16
and family focused practice. Randall ordination with other agencies and
Frazer, a Bidjara man, Team Leader services, and a coherent strategy of
with the ICRS, said that ‘we have service provision across all levels. Homelessness Queensland
a network of twenty Aboriginal These would assist to address
community-controlled clinics and the needs of the community more
other services that we can link mob consistently.
into through our system of care Randall noted that ICRS is often
21%
which opens the door to medical, the only service to break through
allied health, dental and other health to people who do not or cannot
services. We can also link our mob access other services. ICRS have
to broader social services supports, successfully housed Elders back on
79%
including housing’. their own country at times of terminal
Resilience and dedication to working illness, supported young women to
with Aboriginal and Torres Strait access domestic violence services
Islander communities are strong and obtain their own housing in a
Aboriginal and/or
themes of the ICRS. Randall believes safe environment, and linked people
Torres Strait Islander people
that the program works because experiencing severe mental illness to
of the respect, compassion and appropriate specialised care. Non-Indigenous people
OUR VOICES, OUR CHOICES. | 9PRIORITY THEME 1 TARGETED, NEEDS-BASED PRIMARY HEALTH CARE
“Tony” (not his real name) is a consumption. ICRS also provides Aboriginal and Torres Strait Islander
33-year-old Aboriginal man who was guidance with paying rent and bills, people in Queensland comprise 4.9
removed from his single mother’s and with the support of ICRS, he per cent of population, and 21 per
care and had suffered physical has had not returned to prison. He cent of the total homeless population
and emotional abuse at the hands successfully maintains a tenancy, in Queensland.17 Nationally,
of carers. As a teenager he was he regularly accesses physical Aboriginal and Torres Strait Islander
sent to an institution where he was and mental health services and is people made up 20 per cent
sexually and physically abused. He connected back into the Brisbane of the total national population
spent his entire adult life either in Aboriginal community. experiencing homelessness.18
prison or homeless in the inner-city
area. He didn’t have the necessary Randall said that
skills or ability to self-regulate his ‘we respect the human rights and
emotions and was at risk of being the self-determination of our Mob
excluded from the support agency and value their autonomy to make
that referred him to ICRS at the start their own decisions and live the lives
of the year. they want to live. We intentionally
With the support of the ICRS, “Tony” challenge structures, systems
achieved his first tenancy. He now and organisations by encouraging
attends weekly sessions at his compassion, empathy and
local Aboriginal Health Service to respect for our Mob and the
manage with physical conditions ways they should be supported
and past traumas. ICRS also referred by these structures, systems and
him to outpatient counselling for organisations; and by supporting
his substance use issues at a our Mob on their pathways to
major hospital, and to positive transforming their lives – whether
social inclusion activities such as that be from the street or park to
a Men’s Group that have resulted places where they feel strong, safe
in a significant reduction in alcohol and empowered to live their lives.’
FIGURE 4:
Aboriginal and Torres Strait Islander homelessness, National19
120.0 Aboriginal and/or Non-Indigenous
Torres Strait Islander
100.0
Rate per 10,000
80.0
60.0
40.0
20.0
0.0
NSW VIC QLD SA WA NT ACT AUSTRALIA
10 | OUR VOICES, OUR CHOICES.TARGETED, NEEDS-BASED PRIMARY HEALTH CARE PRIORITY THEME 1
Family Wellbeing
Empowerment Program for
Young Aboriginal Men
Central Coast Primary Funded by the Primary Health
Care in New South Wales
Network (PHN), the FWB program Without the
program, male
is an avenue of support for young
has been facilitating a men in the area who may not have
Family Wellbeing Program expressed their vulnerability to
a doctor, an Aboriginal Medical
youth on the
(FWB) as an Aboriginal Service, or a counsellor. It is Central Coast
and Youth Social and
would fall apart.
beneficial that the people running
the program understand the different
Emotional Wellbeing situations young men present, and
Anthony Freeman – Program
project since 2012.20 the vulnerable and occasionally
Participant
reluctant nature in which some
The FWB program was originally young men may attend the program.
developed in 1993 by the Aboriginal
Nigel expressed how he genuinely
Employment Development Branch
relates to the young men – he shares
of the South Australian Department
his personal experiences with them
of Education, Training and
and says, ‘I’m vulnerable, and the
Employment. Over the last 21 years,
same as they are, I share my full story
the FWB program has continued and
from the highs to the lows – they
spread with little formal support and
don’t teach that in schools’.
is now nationally active across most
states and territories, along with Some of the topics discussed in the
some international uptake.21 program are around trauma-informed
practice and psychological tools,
Aboriginal Family Wellbeing
and aside from the experience Nigel
Coordinator Nigel Millgate has
brings to the program, there are
been running the program since its
Elders and community members to
inception. He has seen more than
call for support, offering knowledge
200 Aboriginal young men aged
and guidance for the young men.
between 13 and 18 participate
across eighteen programs. ‘I love One of the program’s first
this project, I’ve watered it and participants, Anthony Freeman,
nurtured it from the beginning’ shared his story about the impact
Nigel remarked as he explained the program has had on his life.
the empowerment, teachings and Anthony said he was ‘sceptical
development that weave through the about the program initially, that going
program, and how these learnings somewhere to talk about feelings
support young men who have often wasn’t really for him.’ After only a
experienced ‘a lack of positive male short time under the mentorship
role models in their lives’. of Nigel and others, Anthony was
OUR VOICES, OUR CHOICES. | 11PRIORITY THEME 1 TARGETED, NEEDS-BASED PRIMARY HEALTH CARE
so deeply engaged in the program parents and kids who might not
that he didn’t want to leave, and he have the capacity or means to get
hasn’t. Seven years later, Anthony to the program any other way. This
remains a mentor for the program. has helped with participation and
retention.
‘As a 25-year-old man talking to a
14-year-old knowing he’ll understand It is evident that people working
the emotional power and understand and participating in the program are
that different ages don’t matter, this passionate about nurturing young
will always be the first and last step – men in the community by providing
it’s our foundation’ said Anthony. ongoing support and encouraging
them to become emotionally
‘It is fundamental that the intelligent and proud young men.
program is community driven As one of the first participants,
and supported’ said Nigel. He Anthony advocates for the program
believes community engagement wholeheartedly saying — ‘this is
with the program is imperative to where I learned how to express my
the program’s success, though emotions, now let’s show the boys
expresses deep concern around the what we can do’.
way in which uncertain government
funding affects the program’s long
and short-term security. Highly
skilled staff members have ceased
working for the program due to
insecure funding.
Another challenge for the program
initially was transport, though the
FWB program has since coordinated
buses to relieve pressure from
12 | OUR VOICES, OUR CHOICES.PRIORITY THEME 2
Responsive Health
Care System
Australia has a fundamental responsibility to its
First Peoples to structure and resource its health
care system to be culturally safe, well-trained and
responsive to the needs of Aboriginal and Torres Strait
Islander peoples. As a wealthy nation,22 Australia has
no defence for not delivering on this fundamental right.
To deliver, Australia needs to grow the Aboriginal and Torres Strait
Islander health workforce, equip the broader health workforce with
the right training to deliver culturally safe health care, and invest in the
greater development of ACCOs satellite and outreach services.
Institutional racism in hospitals and health services continues to be
a crucial barrier to effective health service provision. Comprehensive
health workforce development and training strategies such as cultural
safety training are essential as is the growth of an Aboriginal and Torres
Strait Islander health care workforce.23
The Campaign welcomes Australia’s Health Ministers’ 2018
commitment to the development of an Aboriginal and Torres Strait
Islander-led, National Aboriginal and Torres Strait Islander Health and
Medical Workforce Plan.24
The National Aboriginal and Torres Strait Islander Health Plan (2013–
2023)25 and its Implementation Plan26 were developed to improve
the Australian health care system through meaningful engagement
with Aboriginal and Torres Strait Islander people and organisations.
However, the Campaign reiterates Recommendation 5 of our ten-year
review – that the Government renew its commitment to both Plans
and undertake a comprehensive costing of the Implementation Plan to
ensure it is properly resourced.
The Health Care and Social Assistance sector — covering areas such
as health services, aged and child care — was the largest employing
industry of Aboriginal and Torres Strait Islander peoples in the 2006, 2011
and 2016 censuses.27 This sector is also projected to remain the area of
greatest employment growth for the next five years, with the Government
estimating over 250,000 additional jobs.28 This offers an important
opportunity to support the Aboriginal and Torres Strait Islander workforce
across a range of sectors to help close the gap in health outcomes.
OUR VOICES, OUR CHOICES. | 13PRIORITY THEME 2 AUSTRALIAN HEALTH CARE SYSTEM
Northern Territory Aboriginal
Health Academy Project
It offers Indigenous Allied Health and increase high school retention to
Year 12.
Australia (IAHA), working in
more than Rikki Fisher has been involved
partnership with Aboriginal
the standard Medical Services Alliance
with the Academy since its
commencement and thinks that it has
pathway into Northern Territory been successful ‘due to the people
allied health.
involved, the support the program
(AMSANT), has developed has been getting from families and
Rikki Fisher, IAHA Director
an innovative project to the community and people seeing
and Academy mentor increase the number of the value and believing in what the
program is about’.
young Aboriginal and
‘I think it’s been a really
Torres Strait Islander
well-designed process, with
people completing Year commitment from families and
12 and entering the health communities.’ Rikki said, ‘but it
also needs funding commitment that
workforce. aligns with the values and integrity of
the program. We wouldn’t want it to
The Northern Territory Aboriginal be vulnerable to a lack of support or
Health Academy project (the governments funding cycles.’
Academy) was designed over four
years with Northern Territory (NT) Students are supported to achieve
students, families, community and a Certificate II in Health Support
key stakeholders. Services and a Certificate III in
Allied Health Assistant qualifications
The Academy is taking a new while working in a School Based
approach to education and training. Traineeship or a VET in schools’
This is a community-led learning pathway with a local employer.
model focused on re-shaping They attend one day a week for
and re-designing the way training theory and one day with their
is delivered to Aboriginal and employer on placement. Employers
Torres Strait Islander high school are encouraged to participate from
students. The Academy model diverse organisations including
centres on ensuring that training the public, NGO and community-
and education is delivered in a way controlled sectors in primary
that embeds culture, while having healthcare, rehabilitation and therapy,
a holistic approach to health with disability, aged care, wellbeing
Aboriginal and Torres Strait Islander services and oral health. Providing
health and wellbeing at its centre. a broader experience for students,
FIGURE 5: It works collaboratively across across sectors is important to ensure
Students in the Academy designed their
own logo, representing their different health disciplines and organisational that future workforce needs are met,
cultures and identities as well as the structures such as health, education, particularly where specific needs are
collective group.
training and employment to improve identified, such as disability services.
14 | OUR VOICES, OUR CHOICES.AUSTRALIAN HEALTH CARE SYSTEM PRIORITY THEME 2
Twenty-five Aboriginal students from IAHA and AMSANT support learning, the way in which they learn,
five Darwin high schools enrolled in the Academy through leading, and the environment in which they
the first intake, with the first cohort facilitating, coordinating and feel both safe and included. The
due to complete their Certificate III in collaborating with students and Academy is located on the Charles
Allied Health Assistance in December stakeholders; developing new ways Darwin University campus where
2019. of delivering mainstream courses to students engage in a tertiary setting,
our young people, focused on their gaining confidence and feeling
IAHA and AMSANT are driving aspirations, goals and needs, as well comfortable in attaining further
the project with IAHA and other as employment opportunities in their educational goals.
partner organisation and their region.
members actively participating as The Northern Territory Aboriginal
role models, guest speakers and The model assists in assessing Health Academy model could
mentors. These Aboriginal and/or and demonstrating the success potentially transfer to other
Torres Strait Islander members are of education and training communities where the community,
health professionals and support outcomes where social, cultural families and young people identify
workers who volunteer their time and environmental determinants that it would meet their needs. This
to share their experiences, skills are addressed with wraparound model provides opportunities for
and knowledge with students supports. Also, by embedding Aboriginal and Torres Strait Islander
through practical and interactive culturally safe and responsive high school students to consider,
activities that promote the diverse practices brought together explore and pursue a career in
opportunities within the health and led by local students, health. The delivery and coordination
workforce. Cultural mentors are families, community and partner of the Academy model can be
actively engaged with the students, organisations. The Academy contextualised to communities’
attending and hosting classes, promotes educational achievement aspirations through working in
functions and presentations on and leadership with students partnership with key Aboriginal and
building cultural capabilities. actively setting the direction for their Torres Strait Islander stakeholders.
0.4%
0.4 per cent of the allied health professionals Progress is on track
registered under the National Registration and to halve the gap
Accreditation Scheme (NRAS) in 2017 identified as in Year 12 attainment
Aboriginal and Torres Strait Islander. by 2020.
Data limitations mean it is not currently possible to obtain a While this is only a target to
precise count of the total allied health workforce in Australia, or halve the gap, it is progress
a profile of the Aboriginal and Torres Strait Islander allied health nonetheless, which present
workforce – registered and self-regulated – in Australia, or a potential to attract students
profile of the Aboriginal and Torres Strait Islander allied health into the Aboriginal and Torres
workforce. Nonetheless, it is clear from available data that allied Strait Islander health and
health continues to have among the lowest representation of medical workforce. There is a
Indigenous professionals. Allied health professionals are also significant take up of a health
among the least well distributed health professions, meaning degree by Aboriginal and
people health professions with the largest gap between Indigenous Torres Strait Islander people
and non-Indigenous professionals.29 studying at university.30
OUR VOICES, OUR CHOICES. | 15PRIORITY THEME 2 AUSTRALIAN HEALTH CARE SYSTEM
Health System
Reform – Winnunga
Prison Health Service
Institutional Winnunga Nimmityjah Ms Julie Tongs has been the CEO
at Winnunga for the past 21 years.
Aboriginal Health and
racism can be She said that ‘while Canberra is
Community Services considered to be a wealthy city,
an everyday (Winnunga) provides a behind the affluence there are people
issue for many
who struggle with poverty; who
range of medical and don’t have stable housing, perhaps
Aboriginal and social health services in don’t even have mobile phones, and
can find themselves in a destructive
the Canberra region and
Torres Strait cycle.’
has provided outreach
Islander people. corrections health services
Winnunga provides Aboriginal and
Torres Strait Islander support staff,
Julie Tongs, to surrounding districts in as well as support around child
CEO, Winnunga Nimmityjah protection issues. Winnunga staff
Aboriginal Health and Goulburn and Cooma for
provide court attendance support
Community Services many years. for detainees, via a hotline from
AMC to Winnunga. This means that
When the Alexander Maconochie detainees can have a free phone call
Centre (AMC) prison and remand to access staff at Winnunga and feel
centre was established in Canberra safer and better supported to have
ACT in 2008, it was a natural access to families (who often are
transition for Winnunga to provide also clients of Winnunga).
services to Aboriginal and Torres
Strait Islander detainees, though After the death of an Aboriginal man
services were never enough to in custody in 2015, a formal inquiry
meet needs. As of June 2017, the found that the broader treatment
incarceration rate for Aboriginal of the detainee was deficient,
and Torres Strait Islander people marred by a series of failings
accounted for 27.6 per cent of the involving corrections, police, and
total prison population.31 health authorities. Winnunga has
NATIONALLY ACT
27.6% As of June 2017, nationally, 22.4% In June 2017, in the ACT, Aboriginal
Aboriginal and Torres Strait Islander and Torres Strait Islander people
people accounted for 27.6 per cent accounted for 22.4 per cent of the
of the total prison population.34 total prisoner population. 35
The proportion of Aboriginal and Torres Strait Islander prisoners in the ACT, over the ten-year period
2008-2018, has more than doubled 10.1 per cent to 22.4 per cent as of June 2017.36
16 | OUR VOICES, OUR CHOICES.AUSTRALIAN HEALTH CARE SYSTEM PRIORITY THEME 2
been advocating for better prison counselling; there will continue to health services, including mental
health services for a very long time, be Aboriginal support staff in there, health and drug and alcohol
particularly following the death of and they will know when people are services, but that detainees have
this man. That inquiry found there going to court and be in court with access to a multi-disciplinary
was a need to reform the relationship them… Doctors are now available social health team.
between justice and health teams as needed, and the program will be
operating at the jail and introduce supported by four nurses including Winnunga is hopeful that this service
the Winnunga Prison Health mental health, who can commence will support the AMC to be a human
Service.32 their day at 6.30am, to be available rights compliant detention centre.
for detainees going to court.’ That comliance will go some way to
In 2018, the ACT Government helping detainees overcome a cycle
announced a 24/7 holistic model of A flexible arrangement has been of illness and hence be rehabilitated
care would be led by Winnunga for made with a local pharmacy which rather than come out of prison worse
all detainees in AMC.33 can deliver to the AMC. As the than when they entered.
Winnunga model roles out detainees
Julie explained: ‘this model will mean will also have access to a dentist,
that Winnunga will have an ongoing audiologist and optometrist. This
presence at the AMC. Aboriginal social health, wrap-around service
and Torres Strait Islander staff will be approach means not only that
there as support staff. There will be a detainees have better access to
psychologist to provide one-on-one
PHOTO: Mural outside
Winnunga Nimmityjah
Aboriginal Health and
Community Services,
Canberra. Reproduced with
permission from Winnunga.
OUR VOICES, OUR CHOICES. | 17PRIORITY THEME 2 AUSTRALIAN HEALTH CARE SYSTEM
Anaemia Prevention
Program, Katherine East,
Northern Territory
Kids are much Anaemia is a critical public significant significantly higher than in
Community A.
health issue in Australia
more active and The Anaemia Prevention Program
for Aboriginal and Torres
show interest Strait Islander people. It is
implemented in Community A is the
only anaemia prevention program
in learning and a complex, multifaceted in the NT. While it did not prevent
doing work.
anaemia in all participant children
condition and one of the (as there are other causes of
Katrina Mitchell,
most serious global public anaemia, such as infection),
health problems.37 anaemia was less prevalent and
Aboriginal Health
started later in children on the
Practitioner
prevention program, than those
Worldwide, pregnant women
who were not.
and children have the highest
anaemia rates and are the major Research has found that a
groups targeted for screening and prevention program needs to be
intervention programs. started early in life, before the age
of three months, with education
An Anaemia Prevention Program has
and an iron dose that is provided
been running in three communities
consistently by a dedicated
serviced by Sunrise Health in East
Aboriginal Health Practitioner
Katherine region in the Northern
with intimate knowledge of the
Territory (NT). An evaluation of this
community and the local social
program was conducted by the
determinant issues that hinder
Menzies School of Health Research
parents and primary health care
in 2016, supported by the Lowitja
services from providing the care
Institute.38
required to prevent an anaemic
Research for this program found episode.
that there were marked differences
An integral component of the
in the delivery of health services
success of the Prevention
between Community A (~350
Program has been the
people), B (~1000 people) and C
engagement of an Aboriginal
(~300 people). Community B and
Health Practitioner, Ms Katrina
C did not have a dedicated person
Mitchell, practicing at Sunrise
responsible for anaemia and thus
Health Service. Katrina is a local
opportunistically screen and treat
young mother and has close
children attending the primary
connections with other mothers
health care service in accordance
within the community She knows
with the CARPA manual.39 Anaemia
what’s happening with families in
rates in Community B and C were
the community, and as a local can
18 | OUR VOICES, OUR CHOICES.AUSTRALIAN HEALTH CARE SYSTEM PRIORITY THEME 2
explain the program, and encourage outcome in the health service and
mothers to attend the clinic. the whole wellbeing for all the kids
in the community.’
Katrina says: ‘As an Aboriginal
health practitioner my first job was Ms Raelene Brunette, an
monitoring for the yearly full child Aboriginal researcher working
health check, immunisation and the on the evaluation said: ‘One of
anaemia iron program for the under the key findings in the program
5 kids. I get lots of good positive being successful was due to the
feedback from the child health commitment from the Community
coordinator, teachers and mum’s, Health Centre local staff whom
aunts and other extended family held strong connections within
members.’ the community and who were well
respected by their people. Health
‘Because of the program, the and education go hand-in-hand, you
coordinator and teachers notice cannot have one without the other
a big difference in the kids who in order to create change. This is
had low haemoglobin counts. All very much so with Aboriginal Health
the kids are much more active and Practitioners who have a challenging
show interest in learning and doing and rewarding job at the frontline of
work. As a young Aboriginal person primary health care.
working and delivering the Anaemia
Program, sometimes it’s difficult We cannot achieve success in
and frustrating but also its good improving good health outcomes for
being patient and supportive. I am our people without Aboriginal Health
committed to achieving a positive practitioner’s involvement”.
PHOTO: Ms Katrina Mitchell,
Aboriginal Health Practitioner,
Sunrise Health, Anaemia
Prevention Program
OUR VOICES, OUR CHOICES. | 19PRIORITY THEME 2 AUSTRALIAN HEALTH CARE SYSTEM
IndigiLez Leadership
and Support Group
As Indigenous IndigiLez Leadership aiming to create a culturally safe,
healing space for Aboriginal and
and Support Group
lesbians we Torres Strait Islander women
was founded in 2008 by to discuss identity, gender and
are a minority Rebecca Johnson and sexuality, safely among peers.40
within a Tanya Quakawoot. Both Rebecca has worked at local, state
minority within
and national levels to advocate
founders volunteer their for Aboriginal and Torres Strait
time and funds to offer
a minority, Islander LGBTIQ women, including
through Tekwabi Giz — a national
support for Aboriginal
we’re black, and Torres Strait Islander
collaboration of Aboriginal and
Torres Strait Islander representatives
we’re women lesbian, gay, bisexual, from across each state and territory
and we identify transgender, intersex and around Australia.41
as lesbian or queer (LGBTIQ) women ‘It’s important to provide a space
for women to develop pride
where possible.
being same as Aboriginal and Torres Strait
Islander women as well as a deadly
sex attracted As part of the work with IndigiLez, and proud LGBTIQ+ women’,
the group has held a series of
women. Rainbow Dreaming Retreats at
Rebecca explained. She feels this
is fundamental because ‘building
Nungeena Aboriginal Women’s self-esteem provides opportunities
Rebecca Johnson,
Corporation in Queensland, each for women to feel empowered and
Co-Founder of IndigiLez
es Strait Islander
d Torr LG
l an BT
Iw
ina rigina l and T orres St
ir g f Abo rait el
lb
o n o Isl
b o i r Aborigina fo
an l and
at ety de
ei
saf Tor
nt
rA
r
ng
al res
r
ltu Isl
fo
e
LG
an
es
an
u nd T
orres Strait Islan
fc
ch
al a de
ep
rp
BT
n
dh
igi ro
de
o
or gr
rr
ear
Ip
n
Ab am
rL
NOTE: The rainbow represents
tio
ate
eal
s
GB
eo
ta
what is needed: there are
s
d
Res
ar
an
en
TI
Gre
ple
ow
minimal to no facts about
th
d
em
i
peo
gt
nit
Aboriginal and Torres Strait
din
iat
Impl
Islander LGBTIQ people.
ple
ives
Fun
FIGURE 6:
Recommendations to enhance the health and wellbeing of Aboriginal and Torres Strait Islander LGBTI people
20 | OUR VOICES, OUR CHOICES.AUSTRALIAN HEALTH CARE SYSTEM PRIORITY THEME 2
educated in areas of sexual health,
general health, and social and
emotional wellbeing’ which may
otherwise not be addressed if the
space is unsafe.
High on the list of priorities for
IndigiLez is to find resources to fund
research that investigates holistic
concepts of social and emotional
wellbeing (SEWB) and cultural
safety for Aboriginal and Torres
Strait LBGTIQ women. Rebecca
and the team want to know what
the most appropriate and effective
ways are, to create a safe care
pathway for Aboriginal and Torres
Strait Islander LGBTIQ mob. These
questions inform a larger discussion
around co design of frameworks and
strategies for Aboriginal and Torres
Strait Islander LGBTIQ people being
seen by mainstream health services,
Aboriginal Medical Services (AMSs),
PHOTO: L–R: Belinda Ott, Taz
and Primary Health Networks
Clay & Chantel Keegan
(PHNs).
‘Would a mainstream health
service or AMS understand the
use of a binder by a person who of Aboriginal and Torres Strait
is transitioning?’ Rebecca asks, Islander LGBTIQ women and
among a range of other questions communities. Success so far has
and concerns about understanding been demonstrated by witnessing
the particular health and SEWB women expressing pride in their
needs, and visibility of Aboriginal sexuality, gender, cultural identity
and Torres Strait Islander LGBTIQ and overall sense of feeling valued.
people. IndigiLez would like to IndigiLez co-designs programs with
see questions like this reflected Aboriginal and Torres Strait Islander
in reports that directly impact LGBTIQ women, which means
the community. Simply including that ‘mob saw themselves in the
Aboriginal and Torres Strait Islander programs, recognising that when
LGBTIQ people in health strategies we work together that it increases
is ‘not good enough’ said Rebecca, social inclusion and service access,’
who wants to see Aboriginal and Rebecca said. According to her,
Torres Strait Islander LGBTIQ women mobilising all that IndigiLez aims
included in governmental targets and to achieve is about recognising
not seen as a sub-category in the the importance of ongoing
overall strategies. funding in this space, investing in
research and listening to what the
Ultimately, IndigiLez will continue LGBTIQ+ community needs are, by
to focus on strategies that aim to acknowledging that ‘being part of
optimise the health and wellbeing the conversation is the prevention’.
OUR VOICES, OUR CHOICES. | 21PRIORITY THEME 3
Good Housing
for Good Health
As a campaign, we have long recognised housing
as a determinant of health,42 and we call on all
governments to invest in housing to ensure that
Aboriginal and Torres Strait Islander people have
the best chance of healthy and safe lives.
The linkage between affordable and appropriate housing and
health outcomes must be recognised in the Closing the Gap
Refresh strategy. It is clear that we will never achieve good
health outcomes while people live in poor quality, overcrowded
housing which can have profoundly adverse impacts on
Aboriginal and Torres Strait Islander health outcomes.43
We note COAG’s commitment in December 2018 to secure
appropriate, affordable housing as a pathway to better lives, and
the housing draft target under the Government Refresh process.
While this is a commendable goal, the Campaign reiterates
Recommendation 6 of our ten-year review44 for an overarching
health infrastructure and housing plan be developed, costed and
implemented as a matter of urgency.
The approach could be in the form of a ‘good housing for
good health’ strategy to improve home health and safety for
Aboriginal and Torres Strait Islander people, including the
‘Housing for Health’ program45 to eliminate third world diseases.
Again, we welcome COAG’s commitment to work in true
partnership with Aboriginal and Torres Strait Islander peoples.
We are committed to working with Commonwealth and state
and territory governments to ensure that remote, regional and
urban housing supply is responsive towards improving the
health of Aboriginal and Torres Strait Islander peoples.
The housing stories reflect the strength in community led and
community-controlled programs, and while there is nuance
in how this is presented, each program is equally committed
towards Aboriginal and Torres Strait Islander people driving the
process forward, using our own voice and choices. Living on
22 | OUR VOICES, OUR CHOICES.GOOD HOUSING FOR GOOD HEALTH PRIORITY THEME 3
Country was seen to be an important aspect for people we spoke to
about housing, while for some people, being close to family was the
most important even if that meant living off Country. Most importantly,
all Australians should have the protections that good housing offers for
good health.
20%
In the 2016 Census, 20 per cent
of the homelessness population in Australia were
Aboriginal and Torres Strait Islander people.46
Across all States and Territories, Aboriginal
and Torres Strait Islander households were
between 1.7 and 2.4 times more likely than other
households to live in rented dwellings.47
In the 2016 Census, almost one fifth of persons
living in Aboriginal and Torres Strait Islander
households (18 per cent) lived in dwellings that
required one or more additional bedrooms.
Overcrowding was worse in non-urban areas
(28 per cent) than in urban areas with (16 per cent).48
OUR VOICES, OUR CHOICES. | 23PRIORITY THEME 3 GOOD HOUSING FOR GOOD HEALTH
Yawuru Home
Ownership Program
Home There is a large disparity in program is consistent with this
objective and supports Yawuru
home ownership between
is home. individuals to be empowered home
Aboriginal and Torres owners.
Naomi Appleby,
Strait Islander people The YHOP program is a first for
home owner
and the non-Indigenous Australia. It allows Yawuru first
home owners to enter the housing
population.49 The Yawuru market, in a partnership with NBY,
Home Ownership Program by purchasing housing and land
was established in 2015 packages in a Yawuru-developed
housing area. In order to meet
to address this issue for Keystart’s minimum standard
Yawuru people in Broome. criteria, NBY can retain up to 50 per
cent equity in the house and land
Nyamba Buru Yawuru Ltd (NBY) is package.
a not for profit company owned by
Naomi Appleby is a home owner
the Yawuru Native Title Owners in
under the YHOP program. Yawuru
the Broome region. NBY partnered
made 50 per cent of the funds
with the Kimberley Development
available, and Naomi repays the
Commission and State Government
shared mortgage with Yawuru. Now
mortgage lender Keystart to develop
three years into the arrangement,
the Yawuru Home Ownership Project
she plans to, eventually, own her
(YHOP). YHOP made eight new
home outright. Naomi believes
homes available to local Yawuru
the program provides a very
families through a shared-equity
affordable option for home
purchase arrangement.
ownership and excellent options
Following the recognition of Yawuru for anyone seeking a home –
Native Title and the establishment single parents, young families,
of the Yawuru Native Title Holders and older people.
Aboriginal Corporation (PBC) in
For some people, YHOP has meant
2008, the Yawuru community
achieving accessible housing
highlighted housing as a key priority.
finance, when previous attempts
To deliver on this area of concern,
have failed. The program offers
NBY has a number of programs to
financial counselling for the home
assist Yawuru people to improve
owners so they can become good
their quality of life through improved
money managers and learn about
housing conditions. The YHOP
24 | OUR VOICES, OUR CHOICES.You can also read