RAPID RISK ASSESSMENT - Outbreak of yellow fever in Brazil - Europa EU
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
RAPID RISK ASSESSMENT
Outbreak of yellow fever in Brazil
Second update, 18 January 2018
Conclusions
The 2016/2017 yellow fever outbreak in Brazil was declared over in September 2017, yet the upsurge of
human cases since December 2017 and non-human primate epizootics since September 2017 indicate a
resurgence of yellow fever virus circulation in Brazil, particularly in São Paulo state.
The detection of non-human primate cases in the vicinity of the metropolitan regions of São Paulo and Rio de
Janeiro is of concern, particularly in light of the start of the mosquito activity season in December 2017 and
the suboptimal vaccination coverage in some areas. There is an increased likelihood of peri-urban or urban
cycles of yellow fever transmission, which significantly increases the number of potentially exposed people.
The Carnival, one of the largest international mass gatherings in Brazil, will take place from 9 to 14 February
2018. During the Carnival, the number of EU/EEA travellers to Brazil is expected to increase, hence the
number of travel-related cases among unvaccinated travellers may increase in the coming month.
The risk of yellow fever importation and subsequent transmission in the continental EU/EEA is currently very
low because the virus has to be introduced by viraemic travellers in an area with an established, competent
and active mosquito vector population.
Options for response
Advice to travellers
EU/EEA citizens who travel to, or live in, areas at risk of yellow fever in Brazil and other countries in South
America are advised to:
• check their vaccination status and get vaccinated if necessary, in accordance with national and WHO
recommendations. Vaccination against yellow fever is recommended for people visiting or living in yellow
fever risk areas [1-9], from nine months of age and without contraindication. An individual risk–benefit
analysis should be conducted by professionals in tropical or travel medicine prior to vaccination, taking into
account the period, destination, duration of travel and likelihood of being bitten by mosquitoes as well as
individual risk factors for adverse events following yellow fever vaccination;
Suggested citation: European Centre for Disease Prevention and Control. Outbreak of yellow fever in Brazil, Second update –
18 January 2018. Stockholm: ECDC; 2018.
© European Centre for Disease Prevention and Control, Stockholm, 2018
RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
• take measures to prevent mosquito bites indoors and outdoors, especially between sunrise and sunset
when mosquito vectors are most active [10]. These measures include:
− the use of mosquito repellent in accordance with the instructions indicated on the product label;
− wearing long-sleeved shirts and long trousers;
− sleeping or resting in screened/air-conditioned rooms or using mosquito nets at night and during the
day.
International travellers returning from affected areas may be requested to show proof of yellow fever
vaccination (or a contraindication certificate) when entering countries or territories infested with Aedes aegypti
mosquitoes.
Vaccination requirements and recommendations for international travellers are available from the World Health
Organization’s website [1-8].
Advice to health professionals
Physicians, health professionals and travel health clinics should be provided with, or have access to, regularly
updated information on areas with ongoing yellow fever transmission and should consider yellow fever in the
differential diagnoses for illnesses in relation to unvaccinated travellers returning from at risk areas.
To reduce the risk of adverse events following immunisation, healthcare practitioners responsible for yellow
fever vaccinations should be aware of the contraindications and follow the manufacturers’ advice on
precautions before administering yellow fever vaccine [11,12].
Option for the EU Overseas Countries and Territories and
Outermost Regions with presence of Aedes aegypti
In the EU Overseas Countries and Territories and Outermost Regions where Aedes aegypti is established or
has been introduced, yellow fever vaccination checks should be considered for travellers coming from Brazil in
order to reduce the risk of yellow fever importation.
Options for the safety of substances of human origin (SoHO)
Deferral of blood donors returning from areas affected by malaria will be sufficient to prevent most yellow
fever infectious donations. In addition, precautionary deferral of non-vaccinated blood donors is suggested for
28 days after returning from an area affected by yellow fever but non-endemic for malaria. Potential blood
donors should be deferred from donation for two weeks after live virus immunisation with the yellow fever 17D
vaccine.
For organs, tissues and cells, the risk of yellow fever transmission from a donor who may have visited an
affected area should be balanced with the likelihood of virus transmission. If an organ donor has received
yellow fever vaccine during the four weeks before donation, an individual risk assessment of the immune
status of all prospective recipients is mandatory. Yellow fever vaccination is contraindicated for
immunocompromised patients after solid organ and haematopoietic stem cell transplantation. Potential
transplant patients living in countries endemic for yellow fever or planning travel to endemic countries should
be immunised before transplantation.
There are no specific criteria for the deferral of a prospective SoHO donor with a history of yellow fever.
Therefore, it is suggested that a general recommendation be applied that donors must have recovered, be
afebrile and asymptomatic on the day of donation and may donate SoHO 14 days after full recovery.
Source and date of request
ECDC internal decision, 15 January 2018.
Public health issue
This is the second update of a rapid risk assessment originally produced on 25 January 2017 and updated on
13 April 2017. It assesses the risk to EU/EEA countries and citizens associated with the ongoing outbreak of yellow
fever in Brazil. It was triggered by the evolution of the epidemic in São Paulo state and reports of an imported case
into the EU/EEA from Brazil.
2RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
Consulted experts
ECDC: Céline Gossner, Joana Haussig, Bertrand Sudre, Johanna Young, Lara Payne, Dragoslav Domanovic, Denis
Coulombier.
Experts from WHO Regional Office for America/Pan American Health Organization (PAHO)*.
Disease background information
Background information on yellow fever can be found on the ECDC website: Facts about yellow fever.
Event background information
Epidemiological background of yellow fever in Brazil
In the Americas, yellow fever transmission is maintained through a sylvatic cycle involving non-human primates
(monkeys) and mosquitoes of two genera, Haemagogus and Sabethes. Humans can be infected after being bitten
by yellow-fever-infected mosquitoes of these two genera when they stay close to, or enter, forest areas. In Brazil,
this cycle occurs in a large part of the country, but the most affected locations are forested and rural areas
including the hydrographic basins of the Amazon, Rios Araguaia-Tocantin and Paraná [13].
Yellow fever has a cyclical pattern in forested areas of South America, with alternating endemic periods as seen in
Brazil (Figure 1) [14]. These cyclical intervals from three to seven years are the result of cyclical epizootics in non-
human primates [15]. The observation of deaths in monkey populations is considered as a sentinel event for
human cases of sylvatic origin and is used to define the priority areas for disease prevention and control [13,15].
Prior to the 2016/2017 outbreak, the last epidemic occurred between 2007 and 2009 [16]. The case fatality rate
during the period 1980 to 2016 was 52%. Onset of yellow fever cases in Brazil follows a marked seasonal pattern,
with the majority of the cases detected between January and June [13].
Figure 1. Distribution of confirmed human cases of yellow fever by year, Brazil, 1980 – January 2018
Number of cases
900
800
700
600
500
400
300
200
100
0 *
Year * As of 8 January 2018
Source: Adapted from Ministry of Health, Brazil
*
Experts from WHO reviewed this risk assessment, however the views expressed in this document do not
necessarily represent the views of WHO.
3RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
When infectious humans returning to urbanised areas are bitten by Aedes aegypti mosquitoes, an urban
transmission cycle can establish and spread rapidly in human populations with low vaccination coverage. Aedes
aegypti is present in all Brazilian states [17]. The season for the highest mosquito vector activity lasts from
December to July in the southern part of Brazil.
Since the outbreak of urban yellow fever in Acre in 1942, Brazil has only reported sylvatic yellow fever cases [18].
Entomological investigations conducted during the 2016/2017 outbreak in some of the affected states isolated
Haemagogus mosquitoes positive for yellow fever virus, but no evidence of transmission by Aedes aegypti was
found [19].
Outbreak of yellow fever in Brazil 2016/2017
From July 2016 to June 2017, 779 human yellow fever cases and 262 deaths were reported. In addition, 1 659
epizootics in non-human primates were reported, leading to the death of at least 2 504 animals [20]. The first
laboratory-confirmed cases were reported on 19 January 2017. In March 2017, a decreasing trend in yellow fever
cases was observed in the states of Minas Gerais and Espírito Santo, while an increasing trend was observed in the
state of Rio de Janeiro [16]. During the 2016/2017 outbreak, confirmed cases were reported in the states of Minas
Gerais, Espírito Santo, São Paulo, Rio de Janeiro, Pará, Distrito Federal, Goiás, Mato Grosso and Tocantins [21].
The 2016/2017 yellow fever outbreak in Brazil was declared over in September 2017 [22].
Upsurge of yellow fever cases in Brazil – 2017/2018
Between 1 September 2017 and 14 January 2018, 34 laboratory-confirmed cases, including 20 deaths (CFR=57%),
were reported by the Brazilian national authorities [23]. Four cases occurred between September and November
2017 and 30 cases in December 2017/January 2018. The confirmed cases were reported in the states of São Paulo
(20 cases, including eleven deaths), Minas Gerais (eleven cases, including seven deaths), Rio de Janeiro (two
cases, including one death) and in the Federal District (one fatal case).
The probable sites of infection of all confirmed human cases are areas with documented cases in non-human
primates [23]. Between 1 July 2017 and 8 January 2018, 2 242 yellow fever suspicions of epizootics among non-
human primates were reported, 411 of which were confirmed [23]. Confirmed non-human primate epizootics were
reported from the states of São Paulo (360 cases), Minas Gerais (47), Rio de Janeiro (3) and Mato Grosso (1). The
upsurge of epizootics among non-human primates has been observed since mid-September in São Paulo state.
In December 2017, non-human primates infected with yellow fever were detected in urban parks in the Greater
São Paulo [24]. As a consequence, the authorities closed several parks in the area [25]. In addition, the news
media reported the deaths of four monkeys near one of the access points to the urban Tijuca Forest, in the
northern part of Rio de Janeiro city. These four animal cases are being investigated for suspicion of yellow
fever [26].
A recent phylogenetic analysis of the south-eastern Brazilian outbreak of yellow fever in 2016/2017 suggests that
the outbreak was a result of the reintroduction of a modern-lineage (genotype I) variant from Venezuela or from
some endemic region in Brazil [27]. The genomic analysis of two complete yellow fever virus sequences from two
naturally infected howler monkeys from Espírito Santo state in 2017 showed an identical virus sequence. Seven
amino acid changes were identified by the alignment of the precursor polyproteins from Brazilian and Venezuelan
yellow fever viruses detected since 1980. Further investigations would be needed to asses if these genetic
modifications are found in other locations of the 2017 and current 2018 yellow fever outbreaks in Brazil. The
potential implications of these findings on infectivity and viral fitness remain to be determined [27].
Travel data and travel-related cases
Based on 2015 data from the International Air Transport Association (IATA), 940 000 travellers from the EU/EEA
are estimated to travel to Brazil by air during the period January to May. In 2015, countries of origin included Italy
(17%), Portugal (16%), France (15%), the United Kingdom (12%), Spain (12%) and Germany (12%).
The Carnival, one of the largest international mass gatherings in Brazil, will take place from 9 to 14 February 2018.
This event brings together millions of people throughout the country and an increased number of international
travellers, including travellers from the EU/EEA, is expected.
Since January 2017, three travel-associated cases of yellow fever have been identified among unvaccinated
EU/EEA travellers: one case in January 2017 returning from Bolivia, one case in March 2017 returning from
Suriname, and one case in January 2018 returning from Brazil (i.e. the surroundings of São Paulo city) [28-31]. By
comparison, there were six travel-related cases of yellow fever among EU/EEA travellers between 1999 and 2016,
highlighting an increased circulation of yellow fever virus in the Americas in 2017 [32].
4RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
Yellow fever vaccination
Yellow fever vaccination is not recommended universally in Brazil. WHO recommends vaccination to all
unvaccinated travellers aged above nine months and without contraindication who are travelling to at-risk
areas [33]. Vaccination should be obtained ten days prior to travelling [21]. On 16 January 2018, WHO revised the
areas at risk for yellow fever transmission and included the entire state of São Paulo in the list. Consequently,
vaccination is recommended for travellers visiting any area in the state of São Paulo [21]. Individuals who cannot
be vaccinated because they do not meet the vaccination criteria are of particular concern (e.g. babies under nine
months of age and people with underlying health conditions). These individuals should strictly apply personal
protection measures to prevent mosquito bites [21].
The countries with risk of yellow fever transmission and countries requiring yellow fever vaccination are listed on
the WHO International Travel and Health website [1-8].
Between 3 and 24 February 2018, the Brazilian health authorities intend to vaccinate 7.6 million people. Following
previous recommendations to increase the availability of vaccines in response to an outbreak or in settings where
the extension of the outbreak is imminent [34], the campaign will use fractional doses of the vaccine and will cover
54 cities in the regions of Greater São Paulo, Vale do Paraíba and Baixada Santista. In addition, conventional doses
will be made available to children between the age of nine months and two years, those who travel to countries
with vaccination requirements, pregnant women living in yellow fever risk areas, patients with a transplant history
and those with chronic diseases, such as diabetes, heart diseases or chronic renal failure [35].
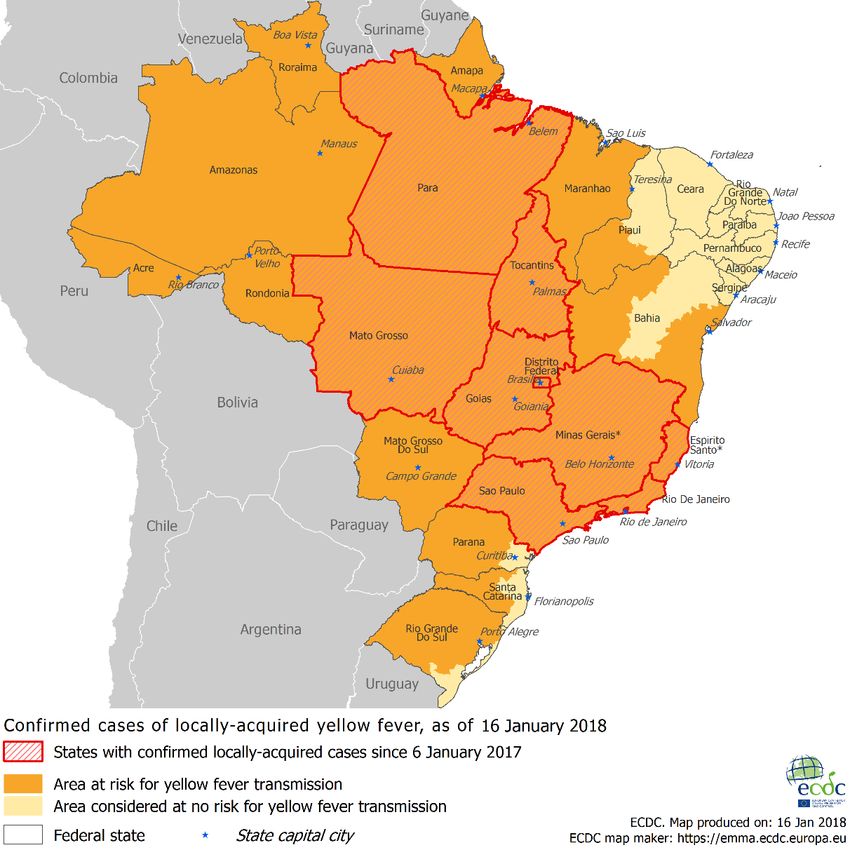
Figure 2. Distribution of confirmed yellow fever cases by municipality, Brazil, 6 January 2017 –
16 January 2018
Source: Adapted from [1-7,35]
5RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
ECDC threat assessment for the EU
Yellow fever risk in Brazil
The upsurge of human cases since December 2017 and non-human primate epizootics since September 2017
indicate a resurgence of yellow fever virus circulation in Brazil, particularly in São Paulo state.
The relatively high number of epizootics among non-human primates that occurred between September and
December 2017 – a period of lower vector activity – indicates continued viral circulation among non-human
primates and therefore a risk for human populations.
The detection of non-human primate cases in the vicinity of the metropolitan regions of São Paulo and Rio de
Janeiro is of concern, particularly in light of the start of the mosquito activity season in December 2017 and the
suboptimal vaccination coverage in some areas [23].
So far, the transmission cycle in Brazil has been sylvatic, and the centres of the metropolitan areas of São Paulo
and Rio de Janeiro have remained unaffected. With non-human primate cases being detected closer to city centres
and a high density of Aedes aegypti mosquitoes in Brazil (which were also responsible for a number of dengue,
zika and chikungunya outbreaks), there is an increased likelihood of peri-urban or urban cycles of yellow fever
transmission, which significantly increases the number of potentially exposed people [37].
Yellow fever risk for EU/EEA citizens travelling to/residing
in affected areas
During the Carnival, the number of EU/EEA travellers to Brazil is expected to increase. Unvaccinated travellers
visiting affected areas and EU/EEA residents living in affected areas are at risk of infection. Hence, an increased
number of travel-related cases among unvaccinated EU/EEA travellers may be reported in the coming month.
Risk of transmission in the continental EU/EEA
The likelihood of yellow fever virus being introduced to EU/EEA countries by viraemic travellers returning from
Brazil is considered low, as most travellers are likely to have been immunised. However, importation of yellow
fever remains possible through infected returning travellers, as demonstrated recently. The establishment of an
urban cycle of yellow fever transmission in Rio de Janeiro or São Paulo would increase the number of exposed
travellers and the likelihood of importation to EU/EEA countries.
The probability of local yellow fever transmission in the EU/EEA following introduction by a viraemic traveller is
currently considered very low as weather conditions during the winter season in continental EU/EEA are not
favourable to vector activity. Recent studies conducted in France have shown that Aedes albopictus mosquitoes,
which are already established in the southern part of the EU, can transmit yellow fever virus in laboratory
settings [38]. To date, yellow fever transmission via Aedes albopictus has not been observed in nature.
Risk of transmission in the EU overseas countries and
territories (OCT) and outermost regions (OMR)
French Guiana is endemic for yellow fever. The most recent locally acquired case was identified in 2017 in a person
who was most likely infected in the border region of French Guiana and Brazil [39]. Yellow fever vaccination has
been mandatory for residents since 1967 and is compulsory for people entering French Guiana [40]. Vaccination
coverage through routine vaccination is high, as demonstrated by an exhaustive coverage survey in schools in
2009, showing a coverage of 95.6% [CI 95%: 95.5–96.3%] in children aged 6 to 16 years [40].
Aedes aegypti is established in the British, French and Dutch OCTs and OMRs of the Caribbean region and in the
Portuguese OMR of Madeira. Recently, Aedes aegypti has been detected in the Spanish OMR of Fuerteventura,
Canary Islands [41]. In the northern hemisphere (e.g. in Madeira) vector activity is currently low. However, the risk
may increase towards the summer months.
The French High Council for Public Health has published guidelines for reducing the risk of importing yellow fever
into receptive areas (where Aedes aegypti is present). Recommendations include:
• vaccination of travellers to risk areas
• integrated vector management
• enhancement of clinicians’ awareness to facilitate early detection of suspected cases [8].
6RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
Yellow fever and safety of SoHO
The risk of yellow fever transmission via substances of human origin (SoHO) is merely theoretical. Transmission of
yellow fever through transfusion or transplantation has not been reported although a risk of infectious SoHO
donations from an unvaccinated asymptomatic viraemic donor cannot be excluded. The yellow fever attenuated
virus from the 17D vaccine has been transmitted through transfusion of blood donated by recently immunised
donors [42]. Donation of blood is possible four weeks after vaccination with attenuated viral vaccine [43].
7RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
References
1. World Health Organization. List of countries, territories and areas. Vaccination requirements and
recommendations for international travellers, including yellow fever and malaria. Geneva: WHO; 2017.
Available from: http://www.who.int/ith/2017-ith-country-list.pdf.
2. World Health Organization. Temporary yellow fever vaccination recommendations for international travellers
related to current situation in Brazil. Geneva: WHO; 2017 [cited 2017 Jan 31]. Available from:
http://www.who.int/ith/updates/20170131/en/.
3. World Health Organization. Updates on yellow fever vaccination recommendations for international travellers
related to the current situation in Brazil Geneva: WHO; 2017 [cited 2017 Feb 14]. Available from:
http://www.who.int/ith/updates/20170214/en/.
4. World Health Organization. Updates on yellow fever vaccination recommendations for international travellers
related to the current situation in Brazil Geneva: WHO; 2017 [cited 2017 March 6]. Available from:
http://www.who.int/csr/don/06-march-2017-yellow-fever-brazil/en/.
5. World Health Organization. Updates on yellow fever vaccination recommendations for international travellers
related to the current situation in Brazil Geneva: WHO; 2017 [cited 2017 March 17]. Available from:
http://www.who.int/ith/updates/20170317/en/.
6. World Health Organization. Updates on yellow fever vaccination recommendations for international travellers
related to the current situation in Brazil [Internet]. 2017 [cited 2017 Apr 4]. Available from:
http://www.who.int/ith/updates/20170404/en/.
7. Jentes ES, Poumerol G, Gershman MD, Hill DR, Lemarchand J, Lewis RF, et al. The revised global yellow fever
risk map and recommendations for vaccination, 2010: consensus of the Informal WHO Working Group on
Geographic Risk for Yellow Fever. Lancet Infect Dis. 2011 Aug;11(8):622-32.
8. World Health Organization. Countries with risk of yellow fever transmission and countries requiring yellow
fever vaccination, International Travel and Health, annex 1 – update – as of 16 February 2017. Geneva:
WHO; 2017. Available from: http://www.who.int/ith/2017-ith-annex1.pdf.
9. European Centre for Disease Prevention and Control. Yellow fever distribution in Brazil [Internet]. Stockholm:
ECDC; 2018. Available from: https://ecdc.europa.eu/en/publications-data/areas-risk-yellow-fever-brazil-16-
january-2018.
10. Pinto CS, Confalonieri UE, Mascarenhas BM. Ecology of Haemagogus sp. and Sabethes sp. (Diptera: Culicidae)
in relation to the microclimates of the Caxiuana National Forest, Para, Brazil. Mem Inst Oswaldo Cruz. 2009
Jul;104(4):592-8.
11. Gershman M, Staples J. Traveler's health – yellow fever [internet]. Atlanta: US Centers for Disease Control
and Prevention; 2016 [cited 17 Jan 2017]. Available from:
http://wwwnc.cdc.gov/travel/yellowbook/2016/infectious-diseases-related-to-travel/yellow-fever.
12. World Health Organization. Yellow fever (fact sheet) [Internet]. Geneva: World Health Organization; 2016
[cited 2016 May 26]. Available from: http://www.who.int/mediacentre/factsheets/fs100/en/.
13. Cavalcante KR, Tauil PL. Epidemiological characteristics of yellow fever in Brazil, 2000-2012. Epidemiol Serv
Saude. 2016 Jan-Mar;25(1):11-20.
14. Ministério da Saúde do Brasil. Situação Epidemiológica / Dados - Situação Epidemiológica no Brasil [Internet].
Ministério da Saúde do Brasil; 2017 [cited 2018 Jan 17]. Available from: http://portalms.saude.gov.br/saude-
de-a-z/febre-amarela/situacao-epidemiologica-dados.
15. Saad LD, Barata RB. Yellow fever outbreaks in Sao Paulo state, Brazil, 2000-2010. Epidemiol Serv Saude.
2016 Jul-Sep;25(3):531-40.
16. European Centre for Disease Prevention and Control. Rapid risk assessment: Outbreak of yellow fever in
Brazil, first update, 13 April 2017. Stockholm: ECDC; 2017. Available from:
https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/06-04-2017-
RRA%20UPDATE%201-Yellow%20fever-Brazil.pdf.
17. Lourenco-de-Oliveira R, Vazeille M, de Filippis AM, Failloux AB. Aedes aegypti in Brazil: genetically
differentiated populations with high susceptibility to dengue and yellow fever viruses. Trans R Soc Trop Med
Hyg. 2004 Jan;98(1):43-54.
18. Bacha HA, Johanson GH. Yellow fever. Rev Assoc Med Bras (1992). 2017 Apr;63(4):291-2.
19. Pan American Health Organization. 12 January 2018: Yellow Fever – Epidemiological Update [Internet].
Washington, DC: PAHO; 2018 [cited 2018 Jan 17].
20. Ministério da Saúde do Brasil. Informe nº 01 | 2017/2018 - Monitoramento do Período Sazonal da Febre
Amarela Brasil – 2017/2018 Brasília: Ministério da Saúde; 2017. Available from:
http://portalarquivos2.saude.gov.br/images/PDF/2017/novembro/14/Informe-FA-14-11-17.pdf.
8RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
21. World Health Organization. Updates on yellow fever vaccination recommendations for international travelers
related to the current situation in Brazil. [Internet]. Geneva: WHO; 2018 [cited 2018 Jan 16]. Available from:
http://www.who.int/ith/updates/20180116/en/.
22. Pan American Health Organization. Brasil anuncia fim do surto de febre amarela Washington, DC: PAHO;
2017 [cited 2018 Jan 17]. Available from:
http://www.paho.org/bra/index.php?option=com_content&view=article&id=5486:brasil-anuncia-fim-do-surto-
de-febre-amarela&Itemid=812.
23. Ministério da Saúde do Brasil. Monitoramento do Período Sazonal da Febre Amarela Brasil – 2017/2018.
Brasília: Ministério da Saúde; 2018. Available from:
http://portalarquivos2.saude.gov.br/images/pdf/2018/janeiro/16/informe-febre-amarela-9-16jan18.pdf.
24. Prefeitura de São Paulo. Parques das Zonas Sul e Oeste da capital são fechados por medida de precaução e
vacinação será intensificada: Capital, ; 2018. Available from: http://www.capital.sp.gov.br/noticia/parques-
das-zonas-sul-e-oeste-da-capital-sao-fechados-por-medida-de-precaucao-e-vacinacao-sera-intensificada.
25. Globo.com. SP tem 15 parques fechados por prevenção contra a febre amarela; veja lista: globo.com; 2018.
Available from: https://g1.globo.com/sao-paulo/noticia/sp-tem-15-parques-fechados-por-prevencao-contra-a-
febre-amarela-veja-lista.ghtml.
26. Metropóles. Rio investiga mortes de quatro macacos na Floresta da Tijuca Brazil 2018 [Jan 16]. Available
from: https://www.metropoles.com/brasil/meio-ambiente-brasil/rio-investiga-mortes-de-quatro-macacos-na-
floresta-da-tijuca.
27. Mir D, Delatorre E, Bonaldo M, Lourenço-de-Oliveira R, Vicente AC, Bello G. Phylodynamics of Yellow Fever
virus in the Americas: new insights into the origin of the 2017 Brazilian outbreak. Scientific reports.
2017;7(1):7385.
28. Bonaldo MC, Gomez MM, Dos Santos AA, Abreu FVS, Ferreira-de-Brito A, Miranda RM, et al. Genome analysis
of yellow fever virus of the ongoing outbreak in Brazil reveals polymorphisms. Mem Inst Oswaldo Cruz. 2017
Jun;112(6):447-51.
29. ProMED-mail post. Yellow fever - Americas (19): Bolivia (La Paz) 2017 [cited 2018 Jan 16]. Available from:
http://www.promedmail.org/post/4832508.
30. ProMED-mail post. Yellow fever - the Netherlands: ex Suriname, WHO. 2017 [cited 2018 Jan 16]. Available
from: http://www.promedmail.org/post/4937716.
31. ProMED-mail post. Yellow fever - the Netherlands: ex Brazil (Sao Paolo) 2018 [cited 2018 Jan 16]. Available
from: http://www.promedmail.org/post/5561671.
32. European Centre for Disease Prevention and Control. Rapid risk assessment: Yellow fever among travellers
returning from South America [Internet]. 2017 [cited 2017 Mar 14]. Available from:
http://ecdc.europa.eu/en/publications/Publications/14-03-2017-RRA-Yellow%20fever,%20Flaviviridae-
Suriname,%20Southern%20America.pdf.
33. World Health Organization. Disease outbreak news - Yellow fever – Brazil, 4 April 2017. [Internet]. Geneva:
WHO; 2017 [cited 2017 Apr 4]. Available from: http://www.who.int/csr/don/06-march-2017-yellow-fever-
brazil/en/.
34. World Health Organization. Fractional dose yellow fever vaccine as a dose-sparing option for outbreak
response [Internet]. Geneva: WHO; 2016 [cited 2018 Jan 16]. Available from:
http://www.who.int/immunization/sage/meetings/2016/october/3_Fractional_dose_secretariat_report_full_ver
sion.pdf.
35. Governo Do Estado São Paulo. SP reabre parques e promove ‘Dia D’ contra febre amarela em 3 de fevereiro
[Internet]. São Paulo: Governo Do Estado São Paulo; 2018 [cited 2018 Jan 16]. Available from:
http://www.portaldenoticias.saude.sp.gov.br/sp-reabre-parques-e-promove-dia-d-contra-febre-amarela-em-3-
de-fevereiro/.
36. Ministério da Saúde do Brasil. Febre Amarela: Brasil adota dose única da vacina por recomendação da OMS
[Internet]. Ministério da Saúde do Brasil; 2017 [cited 2017 Apr 5]. Available from:
http://portalsaude.saude.gov.br/index.php/cidadao/principal/agencia-saude/28003-febre-amarela-brasil-
adota-dose-unica-da-vacina-por-recomendacao-da-oms.
37. Cavalcante K, Tauil PL. Risk of re-emergence of urban yellow fever in Brazil. Epidemiol Serv Saude. 2017 Jul-
Sep;26(3):617-20.
38. Amraoui F, Vazeille M, Failloux AB. French Aedes albopictus are able to transmit yellow fever virus. Euro
Surveill. 2016 Sep 29;21(39).
39. World Health Organization. Yellow fever – France – French Guiana [Internet]. Geneva: WHO; 2017 [cited
2018 Jan 16]. Available from: http://www.who.int/csr/don/30-august-2017-yellow-fever-french-guiana/en/.
40. Haut Comité de la santé publique (France). Vaccination de rappel contre la fièvre jaune pour la Guyane.
Nouvelles recommandations [Internet]. 2014 [cited 2017 Apr 11]. Available from:
http://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=531.
9RAPID RISK ASSESSMENT Outbreak of yellow fever in Brazil – second update, 18 January 2018
41. ProMED-mail post. Invasive mosquito - Spain: (Canary Islands) 2017 [cited 2018 Jan 16]. Available from:
http://www.promedmail.org/direct.php?id=20171214.5503487.
42. Centers for Disease C, Prevention. Adverse events associated with 17D-derived yellow fever vaccination--
United States, 2001-2002. MMWR Morb Mortal Wkly Rep. 2002 Nov 8;51(44):989-93.
43. European Commission. Commission Directive 2004/33/EC implementing Directive 2002/98/EC of the
European Parliament and of the Council as regards certain technical requirements for blood and blood
components. Official Journal of the European Union, 30 Mar 2004, L91/25–L91/39.
Disclaimer
ECDC issued this risk assessment document on the basis of an internal decision in accordance with Article 10 of
Decision No 1082/13/EC and Article 7(1) of Regulation (EC) No 851/2004 establishing a European centre for
disease prevention and control. In the framework of ECDC’s mandate, the specific purpose of an ECDC risk
assessment is to present different options on a certain matter with their respective advantages and disadvantages.
The responsibility on the choice of which option to pursue and which actions to take, including the adoption of
mandatory rules or guidelines, lies exclusively with the EU/EEA Member States. In its activities, ECDC strives to
ensure its independence, high scientific quality, transparency and efficiency.
This report was written under the coordination of an Internal Response Team (IRT) at the European Centre for
Disease Prevention and Control (ECDC). All data published in this risk assessment are correct to the best of our
knowledge on 17 January 2018. Maps and figures published do not represent a statement on the part of ECDC or
its partners on the legal or border status of the countries and territories shown.
10You can also read

















































