Outcome of concomitant left atrial ablation during valvular heart surgery: an African perspective - the Cardiovascular Journal of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
AFRICA CARDIOVASCULAR JOURNAL OF AFRICA • Advance Online Publication, September 2021 1
Cardiovascular Topics
Outcome of concomitant left atrial ablation during
valvular heart surgery: an African perspective
Dambuza Nyamande, Risenga F Chauke, Siphosenkosi M Mazibuko, Shere P Ramoroko
Cardiac ablation is a non-pharmacological treatment
Abstract
modality for atrial fibrillation, which is commonly done by
Objectives: The aim of this study was to determine the success cardiologists using catheter techniques. However, in patients with
rates of left atrial radiofrequency cardiac ablation for atrial atrial fibrillation undergoing valvular heart surgery, concomitant
fibrillation during heart valve surgery.
cardiac ablation is a class IIA recommendation (American
Methods: This was a three-year retrospective study of
Heart Association/American College of Cardiology guidelines,
53 patients who had valve surgery and cardio-ablation.
2014).3 Radiofrequency cardio-ablation during heart surgery is a
Immediate and long-term overall outcomes were analysed at
commonly used modality.
three, six, nine, 12 and 24 months. The results were tested for
significance by comparing to a chance outcome (50:50 prob- Since the description of the classical maze procedure in 1987
ability) using the Z-test for the normal approximation of the by Cox, the procedure has evolved through modifications up to
binomial distribution. the Cox IV procedure. This modification uses radiofrequency
Results: A total of 56.9% of patients converted immedi- energy instead of the original cut-and-sew method. Despite
ately to sinus rhythm, with that number increasing over time. several modifications, the standard maze procedure has remained
Pre-operative poor ejection fraction was the only predictor a bi-atrial procedure with ablation lines on both the left and right
of low success rates following ablation. Long-term rhythm atria.4 Cox explains the importance of bi-atrial ablation in the
was determined by the patient’s rhythm between three and treatment of atrial fibrillation and atrial flutter. An isolated left-
six months. sided cardio-ablation will not produce the same high success rates
Conclusions: Concomitant left atrial ablation during valve for atrial fibrillation, and the non-ablated right atrium may cause
surgery is effective in treating atrial fibrillation. Routine use an atrial flutter rhythm, according to his experimental models.4 As
of anti-arrhythmic medication after surgical ablation is not a result, bi-atrial cardiac ablation is regarded as the gold-standard
recommended. ablation modality for atrial fibrillation and atrial flutter.5
International guidelines on atrial fibrillation treatment
Keywords: atrial fibrillation, cardio-ablation during valve surgery recommend a full (bi-atrial) modified maze
procedure to be done whenever possible, as opposed to the lesser
Submitted 9/5/20, accepted 15/7/21 ablation procedures.3 However, many cardiac surgeons still perform
Cardiovasc J Afr 2021; 32: online publication www.cvja.co.za isolated left atrial cardiac ablation, backed by several publications
showing outcomes that are not inferior to the bi-atrial procedure.6
DOI: 10.5830/CVJA-2021-038 Simplicity and shorter operation times make left atrial ablation an
attractive option, despite controversial results.6
Most publications on the management of atrial fibrillation
Atrial fibrillation is a global heart rhythm disorder, with are from non-African countries. The available information on
prevalence rates in 2010 of 596.2 and 373.1 per million population non-pharmacological treatment of atrial fibrillation in Africa
for men and women, respectively.1 Of those presenting in atrial is from cardiologists, and is only on catheter ablation for atrial
fibrillation in emergency rooms, about 2.2% in North America fibrillation in non-valvular heart disease.7 For the subset of
and 21.5% in Africa had valvular heart disease as a predisposing patients who present for valvular heart surgery complicated
pathology.1 In the South African urban black population, an by atrial fibrillation in Africa, information is needed on the
estimated 13% of valvular heart disease patients are complicated outcome of either unilateral or bilateral cardio-ablation.
by atrial fibrillation.2 Unilateral left atrial cardiac ablation is the treatment modality
offered at Dr George Mukhari Academic Hospital, Pretoria,
South Africa. This research outlines the findings of isolated left
Department of Cardiothoracic Surgery, Sefako Makgatho atrial radiofrequency ablation in valvular heart surgery patients
Health Sciences University, Ga-Rankuwa, Pretoria, South in an African setting.
Africa
Dambuza Nyamande, MB ChB, drnyamande@yahoo.com
Risenga F Chauke, MMed, FC Cardio Methods
Siphosenkosi M Mazibuko, MMed, FC Cardio
Shere P Ramoroko, MMed We conducted a retrospective quantitative study on 53 atrial
fibrillation patients who underwent concomitant left atrial2 CARDIOVASCULAR JOURNAL OF AFRICA • Advance Online Publication, September 2021 AFRICA
cardio-ablation during heart valve surgery between March 2013 in the same period. Late success was a patient who had an
and April 2017. The study was conducted at Dr George Mukhari initial failure but subsequently converted to sinus rhythm in
Academic Hospital in Pretoria, South Africa. Ethical clearance the subsequent follow-up period. Relapse was a patient with
was obtained from Sefako Makgatho Health Sciences University an initial success in the first three months and then any other
Research Ethics Committee (SMUREC/M/81/2018:PG). rhythm in the subsequent follow-up period.
Peri-operative and at least 24-month follow-up records were
obtained from hospital records. Patients were eligible if they had
had pre-operative atrial fibrillation and heart valve pathology as
Statistical analysis
documented by a cardiologist, concomitant left atrial ablation Statistical analysis was performed on SAS (SAS Institute Inc,
done during heart valve replacement(s) and/or repair, if unipolar Carey, NC, USA), release 9.4 or higher, running under Microsoft
radiofrequency ablation was used, and they had been offered Windows, by the statistician Prof HS Schoeman of Clinistat
surgery between 1 March 2013 and 30 April 2017. Exclusion (Pty) Ltd. The percentage of sinus rhythm at each of the time
criteria included patients with isolated ablation without valve points was tested for significance by comparing it to a chance
surgery, the ablation and surgery were offered during separate outcome, using the Z-test for the normal approximation of
operative settings (staged procedure), if the procedure was the binomial distribution. Statistical significance testing was
done outside the study period, and bi-atrial cardiac ablation two-sided and a p-value < 0.05 was considered significant.
or an alternative energy source was used other than unipolar
radiofrequency.
The standard procedure was saline-irrigated unipolar
Results
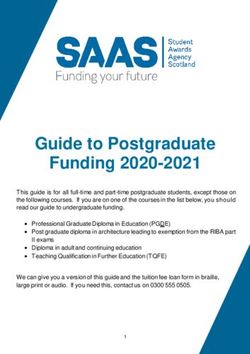
radiofrequency left atrial ablation during cardiopulmonary A total of 53 patients was analysed, with 67.9% (n = 36) being
bypass with an arrested heart. During the procedure, ablation female and 32.1% (n = 17) male. The mean age was 43.6 years,
was done after valve excision (for replacement) and before valve median was 48.0 years and standard deviation was 13.8 years.
replacement(s) or repair(s). A Medtronic® ablation pen was used The interquartile range (IQR) was 34 to 53 years, minimum age
to make a pulmonary vein isolation line, which was joined to the was 16 years and maximum age was 70 years (Fig. 1). Moreover,
P2 mitral annulus (isthmus line). A running 4/0 Prolene® suture 83.0% of patients (n = 44) were below the age of 60 years, with
was used to close the left auricle ostium from the endocardial 35.9% (n = 19) of the whole study population falling in the 50- to
side. 59-year age range.
A 12-lead ECG was used by the cardiologist to record the The majority (81.1%) of patients had no pre-operative
patients’ rhythm. Possible post-operative rhythm outcomes co-morbidities (Table 1); 62.3% (n = 33) of patients had an
included normal (sinus), atrial fibrillation, atrial flutter or other. ejection fraction (EF) of 50% and above, while 37.7% (n = 20)
These were categorically recorded every three months, between had a poor ejection fraction of less than 50% (median EF 55%;
zero and three months, three and six months, six and nine mean EF 53%, SD ± 9.0). About 62% (n = 33) of patients had
months, nine and 12 months and then annually thereafter, at 12 left atrial (LA) sizes between 50 and 70 mm, with 17 patients
to 24 months and more than 24 months. At least one cardiologist in the 50- to 59-mm range and 16 measured 60 to 69 mm. The
interpreted and recorded the patients’ rhythm at least once mean LA size was 57.3 mm (SD ± 11.2) with a median of 56
during these intervals during routine follow up. mm, while three patients were in the largest LA size range of
A successful outcome was sinus rhythm during the zero- to 80 to 89 mm. The largest LA size was 87 mm, as measured by
three-month period, while initial failure was any other outcome echocardiography (Table 2).
Rheumatic mixed mitral valve disease (MMVD) made up
a total of 67.9% (n = 36) of patients, either alone (n = 21) or
in combination with aortic valve disease (n = 15), as shown in
0–19 7.6 4
Table 3. Combinations of MMVD with aortic regurgitation
20–29 15.1 8 (AR) and MMVD with mixed aortic valve disease (MAVD) were
second and third most common after MMVD alone, with eight
Age in years
30–39 13.2 7
and seven patients in each category, respectively. With regard to
40–49 18.9 10
right-sided valve disease, 34.0% of patients (n = 18) had severe
50–59 35.9 19
60–69 7.6 4
Table 1. Patient pre-operative co-morbidities
70–79 1.91
Co-morbidities Frequency (n) Percentage Cumulative %
0 15 30 45 60 Diabetes 1 1.9 1.9
Median (± SD) = 43.6 (± 13.82); Epilepsy 1 1.9 3.8
Median (IQR) = 48 (34–53); min/max = 16/70 HIV 2 3.8 94.3
Hypertension 2 3.8 7.6
Percentage Frequency
Hypertension and diabetes 1 1.9 9.4
None* 43 81.1 90.6
Fig. 1. T
he overall age distribution for all 53 patients Re-do surgery 2 3.8 98.1
(males and females combined). More than one-third Stroke 1 1.9 100
of patients were between 50 and 59 years of age. Total 53 100
Frequency is the absolute number of patients in each HIV: human immunodeficiency virus.
age range. *More than 80% of patients had no co-morbidities.AFRICA CARDIOVASCULAR JOURNAL OF AFRICA • Advance Online Publication, September 2021 3
Table 2. Patients’ pre-operative left atrial sizes Table 3. The frequency of pre-operative left-sided
valve disease and specific valve lesions
Left atrial size (mm) Frequency (n) Percentage
30–39 1 1.9 Mitral valve disease Aortic valve disease Frequency (n)
40–49 13 24.5 – AR 1
50–59 17 32.1 MMVD – 21
60–69 16 30.2 MMVD AR 8
70–79 3 5.7 MMVD MAVD 7
80–89 3 5.7 MR – 7
Total 53 100 MR AR 1
MS – 6
MS AR 1
tricuspid regurgitation, while 30.2% (n = 16) and 28.3% (n = 15) MS AS 1
had mild and moderate tricuspid regurgitation, respectively. Four Total 53
patients (7.8%) had no tricuspid regurgitation, and no tricuspid MR: mitral regurgitation; MS: mitral stenosis; MMVD: mixed mitral valve disease;
stenosis was noted. AR: aortic regurgitation; AS: aortic stenosis; MAVD: mixed aortic valve disease.
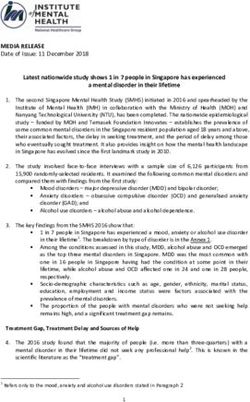
The immediate success rate of left atrial radiofrequency
cardio-ablation in this study was 56.9% (n = 29) at zero to three an ejection fraction of 50% and above, while only 27.6% (n =
months on 51 analysed patients, as the rhythm status was not 8) had a poor ejection fraction below 50% (p = 0.016; Z-test).
recorded on two other patients. The procedure had a 43.1% (n = Therefore, there were significantly more patients with a good
22) failure rate between zero and three months, 39.2% (n = 20) ejection fraction who converted to sinus rhythm after cardiac
of patients having atrial fibrillation, while 3.9% (n = 2) had atrial ablation compared to those with a poor ejection fraction (Fig. 4).
flutter rhythm (Fig. 2). Regarding left atrial size, there was no difference from a 50:50
The percentages of success and failure however did not differ probability in outcome of ablation as there was a 59.1% (p =
significantly from a 50:50 ratio (p = 0.325; Z-test). Therefore, 0.395; Z-test) and a 55.2% (p = 0.575; Z-test) success rate for
there were not significantly more patients in sinus rhythm than
those with non-sinus rhythm at three months after cardio-
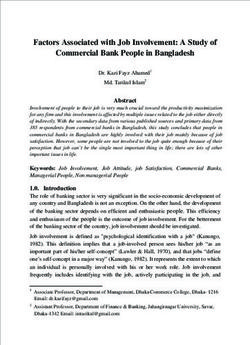
ablation. Beyond three months, the results showed an increase in
the percentage of patients in sinus rhythm, although the actual 75
Percentage of patients
71.4
numbers of patients analysed declined substantially from 51 at 64.9 63.3
in sinus rhythm
56.9
zero to three months to 21 at a period above two years (Fig. 3).
This was due to unrecorded rhythm status in some patients at
each period, and loss to follow up as some patients were referred
back to their district hospitals.
The immediate post-operative success rate of the procedure
during the first three months shows a greater success rate of
0–3 3–6 6–12 12–24 Above 24
65.6% in the good ejection fraction than the poor ejection Duration post cardio-ablation (months)
fraction group (42.1%). However, the result marginally failed to
reach statistical significance with a p-value of 0.07 (Z-test). All Fig. 3. Proportions of patients in sinus rhythm over time,
patients who were in sinus rhythm at three months were further which increased over time and did not fall below the
analysed to establish those with good versus poor ejection initial baseline success rate.
fraction. Of the 29 patients in sinus rhythm, 72.4% (n = 21) had
80
39.2
Rhythm at 0–3 months
Percentage of sinus rhythm
AF 72.4
20 60
3.9
Flutter
2
40
56.9
Sinus
29 27.6
20
0 15 30 45 60
Percentage
0
Percentage Frequency 0 20
Ejection fraction categories
Fig. 2. T
he overall immediate success rate. An initial 56.9%
success rate was achieved with concomitant ablation. Fig. 4. Proportions of patients in sinus rhythm according to
The percentage of the total number of patients is ejection fraction. More than 72% immediate success
shown, whereas frequency is the absolute number of was achieved in patients with good ejection fractions
patients in each category. (p = 0.016; Z-test).4 CARDIOVASCULAR JOURNAL OF AFRICA • Advance Online Publication, September 2021 AFRICA
as unilateral ablation.9 Such similarity in outcomes can be
80 explained by similar patient pre-operative characteristics. The
Percentage sinus rhythm per group
patients in these studies had rheumatic valvular heart pathology.
60
Brazil particularly has patient characteristics comparable to
those in Africa.
Other researchers however had higher success rates than those
40 in our study. Raman et al. in Australia reported an 84% success
rate at three months, which is comparable to the success rate
reported by Cox et al. in 2000.10 Similarly, Ad et al. reported 82,
20 87 and 79% success rates at six, 12 and 24 months, respectively,
after left atrial ablation.11 Favourable pre-operative factors
0
may be a major contributor to such good success rates. Firstly,
0–3 3–6 6–12 patients in these two studies had small left atrial sizes compared
Months (%) to our study population, with all patients in the study by Ad et
0/mild Moderate/severe al. having less than 4.5 cm atrial size. In comparison, about 60%
of our patients had left atrial sizes of 5 cm and above, with the
Fig. 5. T
rends of sinus rhythm (success rate) over time largest being 8.7 cm. This suggests that our patients had long-
according to tricuspid regurgitation severity. Although standing valvular disease compared to those in the above two
not statistically different up to 12 months of follow up, studies, hence the higher risk of failure.
the diverging nature of the curves suggest a possible The general trend of initial improvement in the success rate
wider separation of the curves with a longer follow up. from the first three months to about 12 months, followed by a
decline in the success rate beyond 24 months, was also noted by
other researchers. Ad et al. showed an initial improvement in
patients with left atrial sizes of 60 mm and above versus less than success from 82 to 87% from six to 12 months, which declined
60 mm, respectively. to about 79% at 24 months after ablation.11 Our success rates
Patients with moderate to severe tricuspid regurgitation had were about 63, 75 and 71%, respectively, for the same periods.
a lower immediate success rate at zero to three months after This may confirm what Cox et al. suggested, that the long-term
surgery compared to those without or with mild regurgitation success rate of an incomplete (unilateral) ablation tends to fall
[54.8% (p = 0.596; Z-test) and 60.0% (p = 0.373; Z-test), significantly after two years, as opposed to that of a bilateral
respectively]. This was not statistically different from a 50:50 ablation.4
probability, even at the six- and 12-month periods. Although Although not statistically significant, we found patients with
conclusions cannot be made without statistical significance, the poor ejection fraction (less than 50%) to have poor success
diverging curves suggested possible wider differences with longer rates compared to those with good ejection fraction. However,
periods beyond 12 months (Fig. 5). The same trend was noted for among patients with immediate ablation success (sinus rhythm at
moderate to severe pulmonary hypertension. three months), there were significantly more patients with good
The percentage of patients who reverted to atrial fibrillation pre-operative ejection fraction of 50% and above (72.4%, p =
and/or flutter at any other period after the initial success (sinus 0.016). This suggests that patients with good outcomes are likely
rhythm) at three months, was analysed. Four patients had no to be those with good ejection fractions. This can be explained
record of their rhythm status at any other period other than by the chronicity of the disease before the operation and the
the initial sinus rhythm at three months. Therefore, the rate of amount of structural and electrical remodelling of the atrium.
relapse could only be calculated on 25 instead of 29 patients. Whereas most studies in the literature tended to have patients
Of the 25 patients who were in sinus rhythm at zero to three with good ejection fraction, our study included about 37% of
months, only four (16%) reverted to atrial fibrillation. Of note, patients with poor ejection fraction.
the long-term rhythm of the patients was determined by their The controversial use of anti-arrhythmic medication after
three- to six-month rhythm. Therefore, 100% of patients in sinus cardiac ablation was also evaluated in our study, and it was
rhythm between three and six months remained in sinus rhythm found not to have any effect on the outcome. Patients’ rhythm
in every other future rhythm recording. Similarly, there was a status was not related to the use or not of such medication. The
92.9% probability that patients with atrial fibrillation during the majority of patients were on oral amiodarone, and a few were
same period remained in atrial fibrillation thereafter. Only two on beta-blockers and digoxin upon discharge. The literature
patients (3.9%) out of the 51 available patients at zero to three findings on this matter remain inconclusive, with Henrica and
months had atrial flutter. colleagues not finding any benefit from the use of amiodarone
after bi-atrial ablation, while the results of Raman et al. show
beneficial effects of such medication.10,12
Discussion The lack of effect of anti-arrhythmic medication in our
Success rates of 56.9 and 64.9% at zero to three months and six study and others can be explained scientifically as follows.
to nine months in this study fall in the reported ranges by other Once standard cardiac ablation is done by making appropriate
researchers. Blackstone et al. found success rates of about 59 transmural ablation lines, the flow of electrical current in the
and 63% for the same periods.8 Moreover, Chavez et al. found atrium is directed by physical barriers, which do not allow the
initial sinus rhythm in 63.1% of patients with bi-atrial ablation, current to make continuous circles between the new compartments
suggesting that bi-atrial ablation has the same initial outcome (re-entry phenomena). Therefore, a pharmacological drug is notAFRICA CARDIOVASCULAR JOURNAL OF AFRICA • Advance Online Publication, September 2021 5
expected to allow the electrical current to cross such physical influence on the mortality and morbidity rates, which were not
barriers, hence no effect of medication on the success rate. analysed. There was no randomisation of patients into different
The effect of immediate post-operative (first 24 hours) use of categories, which would have assisted in comparing left atrial
amiodarone infusion however was not evaluated in our study. ablation with a different technique, such as the bi-atrial (maze)
Large left atrial size is one traditionally poor prognosticator, technique.
according to some literature. However, there was no influence
of left atrial size on the success rate of ablation in our study. A
cut-off value of 60 mm was used in this study, as opposed to
Conclusions
the 4.5 cm of Pecha et al. and Ad et al.11,13 Pecha et al. found a Left atrial cardiac ablation during valvular heart surgery was
higher success rate with sizes less than 4.5 cm, as opposed to our effective in the treatment of atrial fibrillation in patients with
findings, which were uniform with each category of left atrial a good ejection fraction undergoing valve surgery. However,
size, above or below 60 mm.13 about 16% of patients relapsed back to atrial fibrillation after
According to Ad et al., left atrial size was a predictor only successful left atrial ablation. Atrial flutter occurred in less than
of success at six months, otherwise, similar to our study, the 5% of patients after left atrial cardio-ablation. The patient’s
left atrial size had no influence on success rates earlier or later rhythm status between three and six months after left atrial
than six months.11 This can be explained again on the basis ablation determined his/her long-term rhythm, which was not
of completeness of transmural ablation lines to form physical affected by anti-arrhythmic medications.
electrical barriers, hence compartmentalising the atrium and
leaving only one corridor to direct the flow of electrical current. This article represents Dr D Nyamande’s mini-dissertation for the MMed
Therefore, the maze principle of remaining with only one Cardiothoracic Surgery degree submitted at Sefako Makgatho Health
electrical pathway is what is important for any left atrial size. Sciences University in 2019. He acknowledges the supervisor and head of
Only three patients had atrial flutter rhythm after left atrial department, Prof RF Chauke and co-supervisors Dr SM Mazibuko and
ablation in our study, two in the first three months and one Dr PS Ramoroko, as well as the departments of Cardiothoracic Surgery
between six and nine months. The 5.9% atrial flutter rate in our and Cardiology and the staff at Dr George Mukhari Academic Hospital.
study is comparable to the 10% found by Chavez et al.,9 which He thanks the Sefako Makgatho Health Sciences University research and
used bi-atrial ablation. This suggests that the hypothesis by Cox library staff, and Prof Schoeman for statistical analysis, as well as his family
et al., that there is a risk of converting atrial fibrillation to atrial for support.
flutter, is a reality and not a myth.4
The long-term rhythm status of a patient was determined
by the rhythm status of the patient recorded in the three- to References
six-month period. There was a 100% probability that patients 1. Lip GYH. Antithrombotic therapy in AF with valvular heart disease.
remained in sinus rhythm provided that they were in sinus Eurospace 2017; 19: 1757–1758.
rhythm between three and six months. Similarly, there was a 2. Jardine RM, Fine J, Obel IWI. A survey on the treatment of atrial fibril-
93% probability that patients would remain in atrial fibrillation lation in South Africa. S Afr Med J 2014; 104(9): 623–627.
for more than two years if they were in atrial fibrillation in the 3. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton
three- to six-month period. This was not influenced by the use or RA, et al. 2014 AHA/ACC guideline for the management of patients
non-use of anti-arrhythmic medication. Therefore, follow up of with valvular heart disease: executive summary. Circulation 2014;
patients can be done less frequently after the first six months post 129(23): 2440–2492.
cardiac ablation. In this South African community, rheumatic 4. Cox JL, Ad N. New surgical and catheter-based modifications of the
MMVD was responsible for more than two-thirds of the surgical maze procedure. Seminars Thorac Cardiovasc Surg 2000; 12(1): 68–73.
valvular heart patients complicated by atrial fibrillation. 5. Ruaengsri C, Schill MR, Khiabani AJ, Schuessler RB, Melby SJ,
Damiano RJ Jr. The Cox-maze IV procedure in its second decade: still
the gold standard? Eur J Cardiothorac Surg 2018; 53: 19–25.
Limitations of the study 6. Li H, Lin X, Ma X. Biatrial versus isolated left atrial ablation in atrial
As a retrospective study done at a referral hospital, it was not fibrillation. Biomed Res Int 2018: 1–3.
possible to control the variables already in the patient files. 7. Talle MA, Bonny A, Scholtz W, Chin A, Nel G, Karaye KM, et al.
Where information was not recorded, conclusions were drawn on Status of cardiac arrhythmia services in Africa in 2018. Cardiovasc J Afr
the basis of available data. The number of missing recordings of 2018; 29(2): 115–29.
ECG status on patients increased over time, with fewer patient 8. Blackstone EH, Chang HL, Rajeswaran J, Parides MK, Ishwaran H,
rhythm statuses from 12 months onwards. This may have affected Li L. Biatrial maze procedure versus pulmonary vein isolation for atrial
the long-term outcomes recorded in this study. The lack of a fibrillation during mitral valve surgery. J Thorac Cardiovasc Surg 2019;
24-hour Holter monitor, which the studies by Ad et al. and Pecha 157(1): 234–243.
et al. had, makes our rhythm status less comprehensive than that 9. Chavez EK, Colafranceschi AS, Monteiro AJ, Canale LS, Mesquita ET,
of other studies, although standard by definition.11,13 Rhythm Weksler C, et al. Surgical treatment of atrial fibrillation in patients with
monitoring was dependent on the available doctor at that time, rheumatic valve disease. Braz J Cardiovasc Surg 2017; 32(3): 202–209.
not a dedicated, independent and blindfolded monitoring team, 10. Raman J, Ishikawa S, Storer M, Power JM. Surgical radiofrequency
as used by Blackstone et al. in the USA.8 ablation of both atria for atrial fibrillation. J Thorac Cardiovasc Surg
Although our study focused on the surgeon factor in ablation, 2003; 126(5): 1357–1366.
it did not compare how much more time left atrial ablation adds 11. Ad N, Holmes SD, Shuman DJ. Left-sided surgical ablation for patients
to valvular heart surgery. Such information may have an overall with atrial fibrillation who are undergoing concomitant cardiac surgical6 CARDIOVASCULAR JOURNAL OF AFRICA • Advance Online Publication, September 2021 AFRICA
procedures. Ann Thorac Surg 2017; 103: 58–65. 175: 290–296.
12. Van Breugel HNAM, Gelsomino S, de Vos CB, Accord RE, Tieleman 13. Pecha S, Ghandili S, Hakmi S, Willems S, Reichenspurner H, Wagner
RG, Lucà F, et al. Maintenance of sinus rhythm after electrical cardio- FM. Predictors of long-term success after concomitant surgical abla-
version for recurrent atrial fibrillation following mitral valve surgery tion for atrial fibrillation. Semin Thorac Cardiovasc Surg 2017; 29(3):
with or without associated radiofrequency ablation. Int J Cardiol 2014; 294–298.You can also read