Pharmacist Billing for Ambulatory Pharmacy Patient Care Services in a Physician-Based Clinic and Other Non-Hospital-Based Environments - FAQ
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pharmacist Billing for Ambulatory Pharmacy Patient Care Services in a Physician-
Based Clinic and Other Non-Hospital-Based Environments – FAQ
Date of Publication: May 2014
Contact:
Justine Coffey, JD, LLM
Director, ASHP Section of Ambulatory Care Practitioners
sections@ashp.org
Disclaimer:
The information contained in this FAQ is provided for informational purposes only and should not be
construed as legal, accounting, tax, other professional advice of any kind. No recipients of the report
should act or refrain from acting on the basis of any content included in the report without seeking the
appropriate legal or other professional advice on the particular facts and circumstances at issue from
an attorney licensed in the recipient's state. The content of the document contains general
information and may not reflect current legal developments, verdicts or settlements. The ASHP
expressly disclaims all liability in respect to actions taken or not taken based on any or all the contents
of the document. The content of the document addresses topics of interest to our membership and
other audiences, and is offered on a blind basis, without any knowledge as to your specific
circumstances. The application and impact of relevant laws will vary from jurisdiction to jurisdiction.
There may be delays or omissions in information contained in the document. The content should not
be relied upon or used as a substitute for consultation with professional advisers.
©2014 American Society of Health-System Pharmacists. All rights reserved.
1. How does billing ambulatory pharmacist patient care services in a physician-based clinic (non-
hospital based) differ from billing in a hospital-based clinic?
For Medicare patients, hospital-based outpatient services (including clinics) are governed by the
Hospital Outpatient Prospective Payment System (HOPPS) regulations. However, physician offices
and physician-based clinics providing services for Medicare patients are not governed by HOPPS, but
instead are governed by a number of CMS rulings that can be found at
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 1http://www.cms.gov/Regulations-and-Guidance/Regulations-and-Guidance.html. This site includes
the Medicare Benefit Policy Manual which describes who can bill under Medicare Part B and the
1995 and 1997 Documentation Guidelines for Evaluation and Management Services which describes
the documentation required for billing.
The Medicare Benefit Policy Manual describes which providers may bill under Medicare Part B.
Pharmacists are not recognized Medicare Part B providers except when providing immunizations.
The Medicare Benefit Policy Manual, Chapter 15 Section 601 describes physician delegation to others
working in their offices who provide care to Medicare patients and a mechanism for billing such
services. The title of this Chapter is “Services and Supplies Furnished Incident to a Physician’s/NPP’s
Professional Service” and governs the services pharmacists provide in a non-institutional setting.
These services are often termed “incident to.” Under these rules, pharmacists can bill for their
services in a physician-based clinic. These rules differ in their processes from the HOPPS regulations.
Non-institutional physician-based offices and clinics may negotiate specific contracts with private
payers that may include a different mechanism for payment to enable pharmacist reimbursement for
patient care services, 2 including utilizing a direct payment process incorporating the Medication
Therapy Management (MTM) CPT codes or another preferred mechanism.2, 3, 4 Alternatively,
pharmacist-based services may be folded into a capitated payment model and or associated with pay
for performance incentives. If there are no specific contracts with private payers, billing for
pharmacy services defaults to Medicare regulations. Medicare patients by law may not be treated
differently than other patients. In certain states, Medicaid rules and laws may allow payment for
pharmacist-provided patient care services in the ambulatory setting.
2. If I am employed by another entity (e.g. school of pharmacy), but also practice in a physician-
based clinic, how do I bill for my services?
In order for pharmacists to bill incident-to the physician, Medicare stipulates that nine requirements
must be met. As long as the following requirements are met, you may bill for your services using
incident-to billing in the physician-based clinic.1, 2
A. The patient must first be seen by the physician for an evaluation or a Medicare covered
service.
B. The physician must have provided authorization for the service in the medical record.
(Usually done by a standard referral process).
C. The physician must continue to see the patient at a frequency that reflects his/her active
participation in the management of the course of treatment. Review of the medical
record does not qualify. Although not defined, Medicare fiscal intermediaries may have
rules such as a “one of three rule,” or every third visit must be a physician visit. However
you choose to interpret this ruling, it should be reasonable and customary.
D. The service provided by you, the pharmacist, is commonly furnished in a physician or
Medicare Part B provider’s office or clinic.
E. The service must be medically appropriate to be given in the provider’s office or clinic.
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 2F. Services provided by a pharmacist incident to the physician must be within the
pharmacist’s scope of practice as dictated by the state’s Pharmacy Practice Act.
G. Services and supplies must be furnished in accordance with applicable State law. Any
other state laws besides the Pharmacy Practice Act that affect your service must be
adhered to.
H. A physician or Medicare Part B-approved practitioner must be on the premises, but not
necessarily in the room when incident-to services are performed. The supervising
practitioner must be part of the organization.
I. The pharmacist providing the incident-to service must be an employee, leased or
contracted to the physician or Medicare Part B-approved provider. The practice must
have some legal control over the person and his or her services, and the person must
represent an expense to the practice. (Expense may include salary, non-salary support
such an exam room, office supplies, staff support etc.)
3. Can a physician, nurse practitioner, physician assistant, or other recognized provider provide
direct supervision in a physician-based clinic?
FAQ 2 (F), above, states that a physician or Medicare Part B approved practitioner must be on the
premises to provide direct supervision. The Medicare Benefits Policy Manual describes those who
are Medicare Part B-approved practitioners, and that list does include nurse practitioners and
physician assistants.
It is important to note that this may vary in interpretation by the regional Medicare Fiscal
Intermediaries who are contracted by Medicare to administer the Medicare benefit in their region.5, 6
4. Must the supervising clinician review and sign off on all pharmacist notes?
There is no requirement that the physician or supervising provider must sign off on all pharmacist
notes. The requirement states that the physician or supervising provider establishes the plan of care
for the patient that authorizes your service, and the physician or supervising provider must continue
to be actively involved in that plan of care. How Medicare Fiscal Intermediaries and your
organization interpret that statement may vary, including requiring the supervising provider to sign
the pharmacist notes as an indication that she is aware of your activity, following up with a face-to-
face visit with the patient at a reasonable frequency indicating active involvement, or some other
process that would reasonably be considered to meet the active involvement requirement of the
regulations.2
5. Can a pharmacist use the MTM CPT codes when working in a physician-based clinic?
For Medicare beneficiaries seen in a physician office by a pharmacist, MTM CPT codes are not
recognized, since physician offices fall under Medicare Part B. Medicare recognizes MTM services
only under Part D. Under Medicare Part D, MTM services are paid through administrative fees to a
Prescription Drug Benefit Plan. If your physician office or clinic has a dispensing licensed pharmacy,
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 3there is the opportunity to contract with Prescription Drug Benefit Plans to provide MTM and use the MTM codes through that venue. The physician-based clinic may have specific private payer contracts or state Medicaid opportunities that will allow the utilization of the MTM CPT codes in this setting. If there are no such opportunities in your setting, the default is to Medicare billing.7 6. Whose NPI number should be assigned to the patient's billing information when a pharmacist sees a patient in a physician-based clinic? For Medicare patients, pharmacists are not recognized as Medicare Part B providers and can only bill “incident-to” the physician supervising in the practice or clinic. Consequently, pharmacists are restricted to billing at the 99211 code level. Therefore, the NPI of the Medicare provider (i.e. physician or Medicare Part B-approved practitioner) must be used on the paper or electronic CMS 1500 claim form.2 For non-Medicare patients, the clinic or non-Medicare payer may require the pharmacist to use his/her NPI number. This may be for internal tracking purposes or it may be required under the contract or state Medicaid rules.2 7. Can a pharmacist see and bill the patient on the same day as a physician visit? A pharmacist would not want to see and bill the patient on the same day as a physician visit in the same office or clinic as that would not be fiscally prudent to the organization. If the same clinic or physician office submits two separate bills to CMS on the same day, CMS will pay the lesser of the two bills which will always be the pharmacist bill at the 99211 code level. The result would be a significant loss of revenue. However, if a patient is seen in an endocrinology clinic and then sees you in a primary care clinic on the same day, two bills may be generated as these are two different clinics. 8. If I practice in a community pharmacy, how do I bill for my cognitive services? 8 There are a number of ways a community pharmacy may bill for cognitive services which may vary by state and the Medicare Part D Prescription Drug Plans (PDP) available to you at your location. Several states pay community pharmacists to provide various levels of cognitive services to State Medicaid beneficiaries. Certain Medicare Part D PDP plans contract with community pharmacists to provide MTM services required under Medicare Part D. Community pharmacists and pharmacies (as well as any other entity) may secure contracts with private payers. This has been most successful with local self- insured employers or self-insured business groups. Finally, community pharmacists (as well as any other entity) may submit bills to any provider, but they would need to determine which providers are eligible under a patient’s particular health insurance plan to submit bills, the rules of participation (they may need to sign a participation agreement) and then standard procedures would need to be followed in submitting the bill. The process is explained well in the following publication: Poirier S, American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 4
Buffington DE, Memoli GA. Billing Third Party Payers for Pharmaceutical Care Services. J Am Pharm Assoc. 199;33:50-64. Unfortunately payment return on billing is probably around 30%. 9. Beyond CPT “incident to" codes and MTM codes, which other codes or methods can pharmacists use to bill for clinical services in a physician-based clinic or in a community pharmacy? *Refer to reference 9 for up-to-date Physician Fee Schedules Diabetes Self- Management Training/Education (DSMT/E) 1 For complete information, refer to CMS Medicare Benefit Policy Manual Chapter 15, Section 300. G codes (e.g. G0108 and G0109) can be used for DSMT/E if you have an accredited Diabetes Self- Management Education program (accredited by American Diabetes Association or American Association of Diabetes Educators). These can be run and managed by one discipline (e.g. an RPh, RN, or RD), though a team approach is encouraged. Pharmacists who develop/manage these programs do not have to be CDEs. Billing must use the NPI of the practice or pharmacy, not the individual NPI of the pharmacist.10 The code G0108 is used for each 30 minutes of an individual DSMT/E session (reimbursement rate around $51). Medicare covers this if no group session is available within 2 months (plus other criteria). The code G0109 is used for each 30 minutes of a group (2 or more persons) DSMT/E session (reimbursement rate around $15/patient). Payment to non-physician practitioners for DSMT program services (G0108 or G0109) are paid at the full fee schedule (not at 85% of fee schedule). Insulin pump training11, 12 Billing for insulin pump training can be done as part of DSMT/E and billed under G0108 and G0109. In order to bill for this training, the facility must have an ADA or AADE recognized DSMT/E program. Instead of the above option, insulin pump training and education is often included in the price to the payer. The pump training is paid by the pump company to the individual pump trainer, or to the clinic. Aside from billing directly for insulin pump training, the counseling services provided as part of this education can count as a component of E&M services (99212-99215). Education-specific CPT codes, 98960-98962, are not paid by Medicare, but may be paid by private payers (these codes do not require a DSMT program to be recognized by ADA or AADE, but the program must have a standardized curriculum). A certified pump trainer can be reimbursed a fixed amount from the pump company that covers up to 2 months of training and management. If any additional education or management is required by the patient after the 2 months of initial training, the pharmacist educator may bill the patient’s individual insurance provider under diabetes education and self-management codes (Healthcare Common Procedure Coding System codes G0108 and G0109) provided the pharmacist practices in an ADA-recognized program. Most patients will have cost sharing through their payer that the pharmacist must collect in the form of a deductible. American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 5
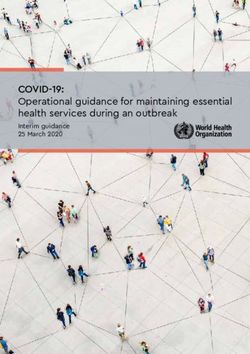
Medicare Annual Wellness Visits (AWV) 1,13,14,15
For complete information, refer to CMS Medicare Benefit Policy Manual Chapter 15, Section 280.5.
Annual Wellness Visits were established under the Affordable Care Act, effective January 1, 2011.
These services are provided by Medicare for beneficiaries who are no longer in the first 12 months of
their first Part B coverage period. Prior to an AWV, an Initial Preventative Physical Examination
(IPPE), “Welcome to Medicare Preventative Visit,” is completed by a physician or qualified non-
physician practitioner. A pharmacist may not provide or bill for this service. This initial preventative
visit is paid for completely by Medicare. Following the IPPE, other licensed, non-physician
practitioners working under the direct supervision of a physician may perform subsequent Medicare
Wellness. Pharmacists may provide and bill for these services. The HCPCS codes for these Medicare
wellness visits are G0438 and G0439. The 2013 Medicare reimbursement rates are: G0438=$169 and
G0439=$112.9
Visit Type Timing HCPCS Code
Welcome to Medicare (IPPE) Visit* Within 12 months of Medicare G0402
enrollment
First Annual Medicare Wellness Visit First MWV (>12 months from IPPE G0438
(MWV) visit)
Annual Medicare Wellness Visit Subsequent MWVs G0439
* Can only be performed by a physician or other qualified non-physician practitioner
CLIA-Waived lab1,16,17
CLIA-waived labs is a term used to describe laboratory procedures that can be completed in
ambulatory care practice settings (i.e. community pharmacies, hospital-based outpatient clinics,
etc.). A CLIA Certificate of Waiver can be obtained using form CMS-116. Receiving this Certificate of
Waiver gives the pharmacy, or sight of testing, a CMS Part B Identification Number (PIN) (cost of
obtaining this PIN is $150). Billing for these services is a charge submitted for the laboratory services
only, not for any cognitive services. This claim is submitted using the CMS 1500 form. To maintain a
CLIA-waived labs certification, the practice must maintain a manufacturer quality assurance log that
is available for inspection. In order to complete a laboratory test in a CLIA-waived facility, there must
be a statement of medical necessity and ICD-9 code from the physician for the laboratory test being
performed.
Immunizations18, 19, 20,
The vaccines that may be provided by a pharmacist, and the ages for which you are allowed to
vaccinate, vary by state law.
To administer Part B covered vaccines, you must be enrolled in a Medicare program with a provider
number. This Medicare provider number will be the pharmacy’s, not an individual pharmacist’s. A
specific immunization provider number will be obtained from a Medicare Part B Fiscal Intermediary
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 6for the pharmacy. If you are located in a physician office, immunizations administered at this site can
be billed with the physician’s Medicare Part B number. This Medicare provider number can be
obtained using form CMS-855.
In addition to Part B covered vaccines, pharmacists are also able to administer Part D vaccines.
Beginning January 1, 2008, the negotiated price for a Part D vaccine is comprised of the vaccine
ingredient cost, a dispensing fee (if applicable), sales tax (if applicable), and a vaccine administration
fee. Medicare Part D covered vaccines should NOT have a separate copay for the vaccine and its
administration. If a Part D plan charges coinsurance, it should be applied relative to the entire price
of both components. Listed below are commonly administered vaccines and further information
regarding their administration and diagnosis codes.
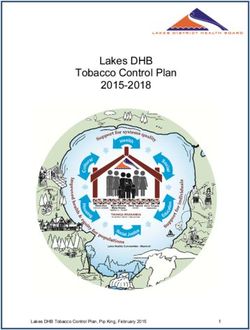
Commonly Administered Vaccines
Vaccine Code & Description Administration Diagnosis
Code Code
Influenza* 90657 – Split virus, 6-35 months dosage, for G0008 V04.81
intramuscular or jet injection use
90658 - Split virus, 3 years and above dosage,
for intramuscular or jet injection use
Pneumococcal* 90732 – Pneumococcal polysaccharide G0009 V03.82
vaccine, 23-valent, adult dosage, for
subcutaneous or intramuscular use
Hepatitis 90743 – Hepatitis B vaccine, adolescent (2 G0010 V05.3
dose schedule), for intramuscular use
90744 – Hepatitis B vaccine, pediatric/
adolescent dosage (3 dose schedule), for
intramuscular use
90746 – Hepatitis B vaccine, adult dosage, for
intramuscular use
*Medicare Part B covered vaccines
Transitional Care Management21, 22, 23
Transitional Care Management is a new Medicare program that went into effect on January 1, 2013
as part of the Affordable Care Act. The Transitional Care Management services can be used to bill
physician and “qualified non-physician providers” care management following discharge from an
inpatient hospital setting, observation setting, or skilled nursing facility. Pharmacists can serve as the
“qualified non-physician providers” to provide some of these services. However, the claim for these
services must be submitted under a Medicare recognized provider, so a pharmacist in this role must
collaborate with a licensed Medicare provider. Pharmacists may provide the non-face-to-face care
and coordination components of these visits. In addition, they may be involved in the face-to-face
visit and assist the Medicare recognized provider in medical decision making through services such as
medication reconciliation. To request reimbursement for these services, the pharmacist must meet
the “incident-to” requirements described in CMS Benefit Policy Manual Chapter 15 Section 60.
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 7Visit Type Timing HCPCS Code Complexity Claim Date
(Calendar Days)
Transitional Care Within 7 days of 99496 High 30 days from
Management discharge discharge
Transitional Care Within 14 days 99495 Moderate 30 days from
Management of discharge discharge
10. What is the billing process in a physician’s office and who are the key people that manage this
process? 2, 24
Most physician offices or clinics employ or contract with professional billers and coders. An
individual who holds the title of Compliance Officer usually leads this department or a contracted
entity. With regard to physician office-based services billing procedures, the Compliance Officer is
responsible for assuring that the billing process is consistent with and does not deviate from the rules
and regulations of federal and state law, Medicare and Medicaid, and the contractual rules and
obligations for any private payers. Additionally, there are professional coders who are trained to
correctly code and bill for services rendered by the physician office or clinic.
All payers, in particular the state and Medicare, may audit any participating practice. If billing
practices do not meet the laws, rules and regulations, the provider may be responsible for refunding
all payments for which the bill did not meet the established rules. For government payers, there may
be additional penalties including criminal judgments.
11. Which information or documentation must be included in order to bill in the physician office
setting? 2
Documentation required for billing is defined under the 1995 and 1997 Documentation Guidelines
for Evaluation and Management Services. Medicare Part B pays for the evaluation and management
of medical conditions and medical decision making based on disease states (ICD-9 codes). They do
not pay for medication management under Medicare Part B. Documentation must address the
medical condition and therapy plan that resulted in authorization for pharmacist services by the
physician. For “incident-to” billing, there are five billing levels (99211-99215). An increasing level of
complexity defines each of these levels, with 99211 being a simple patient encounter to 99215 being
a complex encounter. Each level above 99211 has certain requirements for documentation elements
in the history, physical exam and a hierarchy for the intensity of medical decision-making.4 The 99211
level, where pharmacists are restricted to billing, has no requirements for documentation elements.
However, it is still an evaluation and management code (E&M), and therefore a patient’s medical
conditions need to be evaluated and managed. Documentation must show evidence of patient
evaluation for their condition within the scope of the provider, and then subsequent management of
the condition. For example, a pharmacist seeing a patient and noting that the blood pressure was
120/80 in the medical record with no evaluation or management is not an acceptable 99211 bill.
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 8Evaluating whether that blood pressure is at the patient’s goal, evaluating for complications to the
medication regimen for hypertension and providing continued education on hypertension and
therapy would qualify as an evaluation and management. The Medicare Fiscal Intermediary may
have additional documentation rules as in this example for “incident to” billing:
Documentation Requirements:
1. The progress note must substantiate the service performed and be signed by the person
performing it.
2. When the physician is involved with a particular service, his or her contribution to the care
must be documented. This will assist in substantiating his or her continued involvement in the
patient's care.
3. The extent of physician involvement should reflect the patient's condition, increasing with
instability and uncertainly of the situation.
4. All documentation should support the level of care provided
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 9Authors Mary Ann Kliethermes, PharmD Vice Chair of Ambulatory Care Associate Professor Chicago College of Pharmacy Midwestern University Downers Grove, IL Ashley Marie Parrott, PharmD, BCPS Clinical Pharmacist ProMedica Toledo Hospital Family Medicine Residency Toledo, OH Gloria Sachdev, BS Pharm, PharmD Clinical Assistant Professor, Primary Care College of Pharmacy Purdue University; Adjunct Assistant Professor School of Medicine Indiana University Indianapolis, IN Renu F. Singh, PharmD., BCACP, CDE H.S. Associate Clinical Professor of Pharmacy University of California, San Diego Skaggs School of Pharmacy and Pharmaceutical Sciences La Jolla CA Zachary A. Weber, PharmD, BCPS, BCACP, CDE Clinical Assistant Professor Department of Pharmacy Practice Purdue University College of Pharmacy Clinical Pharmacy Specialist, Ambulatory Care Eskenazi Health Indianapolis, IN American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 10
References
1. http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf.
Accessed May 23, 2013 and http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1600-FC.html.
2. Building a Successful Ambulatory Care Practice – A Complete Guide for Pharmacists. Ed.
Mary Ann Kliethermes, Ed. Tim R. Brown. Bethesda: ASHP, 2012. Chapter 8. Print.
3. Summary of HR 1 Medicare Prescription Drug Improvement, and Modernization Act of 2003,
Public Law 108-173. http://www.cms.hhs.gov/MMAUpdate/downloads/PL108-
173summary.pdf. Accessed January 24, 2009.
4. American Medical Association. 2013 Current Procedural Terminology (CPT): Professional
Edition.
5. http://wpsmedicare.com/j5macpartb/policy/active/national/_files/phys004.pdf. Accessed May
23, 2013.
6. www.wpsmedicare.com. Accessed May 23, 2013.
7. American Pharmacists Association. Medication Therapy Management Services: A Critical
Review Executive Summary Report.
http://www.accp.com/docs/positions/commentaries/mtms.pdf. Accessed May 23, 2013.
8. Poirier S, Buffington DE, Memoli GA. Billing Third Party Payers for Pharmaceutical Care
Services. J Am Pharm Assoc. 1999;33:50-64
9. http://www.cms.gov/apps/physician-fee-schedule/overview.aspx. Accessed August 15, 2013.
10. AADE Diabetes Education Services: Reimbursement Tips for Primary Care Practice.
http://www.diabeteseducator.org/export/sites/aade/_resources/pdf/research/Diabetes_Education
_Services6-10.pdf. Accessed June 6, 2013.
11. https://www.diabeteseducator.org/Members/Reimbursement_QxA.html. Accessed June 6,
2013.
12. Boyd LC and Boyd ST. Insulin Pump Therapy Training and Management: An Opportunity for
Community Pharmacists. JMCP 2008;14:790-794
13. http://www.ashp.org/DocLibrary/MemberCenter/SACP/Spotlight/Spotlight-June-2012.aspx
14. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNProducts/downloads/AWV_chart_ICN905706.pdf. Accessed August 16, 2013.
15. http://www.cms.gov/Outreach-and-Education/Outreach/NPC/Downloads/IPPE-AWV-
FAQs.pdf. Accessed August 16, 2013.
16. https://www.cms.gov/Regulations-and-Guidance/Legislation/CLIA/. Accessed June 6, 2013
17. https://www.cms.gov/Regulations-and-
Guidance/Legislation/CLIA/Downloads/HowObtainCertificateofWaiver.pdf. Accessed June 6,
2013.
18. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNProducts/downloads/flupdf.pdf. Accessed June 6, 2013.
19. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNMattersArticles/downloads/se0727.pdf. Accessed June 6, 2013.
20. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNProducts/downloads/qr_immun_bill.pdf. Accessed August 14, 2013.
21. http://www.ashp.org/DocLibrary/MemberCenter/SACP/Spotlight/May-09-2013.pdf. Accessed
June 6, 2013.
22. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 11Payment/PhysicianFeeSched/Downloads/FAQ-TCMS.pdf. Accessed August 14, 2013.
23. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNProducts/Downloads/Transitional-Care-Management-Services-Fact-Sheet-
ICN908628.pdf. Accessed August 14, 2013.
24. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNMattersArticles/downloads/se0441.pdf. Accessed June 6, 2013.
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 12Developed in Cooperation with the Section Advisory Group on Compensation
and Practice Sustainability
Chair
Binita Patel, Pharm.D., M.S. Susan Conway, Pharm.D., BCPS, CACP, FASHP
Director of Ambulatory/Retail Associate Professor
Froedtert Health University of Oklahoma College of Pharmacy
Milwaukee, WI Oklahoma City, OK
Vice Chair Douglas F Covey, Pharm.D., FCCP, MHA
Clinical Pharmacy Specialist Am Care/Assoc Prof
Starlin Haydon-Greatting, MS, BSPharm, FAPhA Tampa VA/Univ of Florida
Clinical Program Coordinator for the Illinois Tampa, FL
Pharmacists Association’s (IPhA)
Diabetes/CV Health Patient Self Management Danny K Fu, Pharm.D.
Programs Ambulatory Care Clinical Pharmacist
Springfield, IL Carolinas Medical Center- NorthEast
Concord, NC
Immediate Past Chair Mary Ann Kliethermes, BS, Pharm.D.
Vice-Chair of Ambulatory Care
Kimberly Braxton Lloyd, Pharm.D. Associate Professor
Assistant Dean of Health Services Chicago College of Pharmacy
Auburn University's Harrison School of Midwestern University
Pharmacy Downers Grove, IL
Auburn University, AL
Christine Manukyan, Pharm.D., M.S.
Rachael M Boggs, Pharm.D., CPH, BCPS Outpatient Pharmacy Supervisor
Clinical Pharmacy Specialist Cedars-Sinai Medical Center
University of Colorado Hospital Los Angeles, CA
Aurora, CO
Santhi Masilamani, PharmD, CDE, MBA
Donald Brown, Pharm.D., BCACP, CPP Director, Ambulatory APPE
Ambulatory Care Clinical Pharmacist III University of Houston College of Pharmacy
Billings Clinic Houston, TX
Billings, MT
Emily Pherson, Pharm.D., BCPS
Mark B Collum, Pharm.D., CPh PGY2 Pharmacotherapy Resident
Director Ambulatory Pharmacy Services The Johns Hopkins Hospital
Lee Memorial Health System Baltimore, MD
Fort Myers, FL
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 13Jessica Skelley, Pharm.D . Executive Committee Liaison
Assistant Professor of Pharmacy Practice
McWhorter School of Pharmacy Samford Sandra Leal, Pharm.D., FAPhA, CDE
University Director of Clinical Pharmacy
Birmingham, AL El Rio Health Center
Tucson, AZ
Jane S Tennis, M.B.A., R.Ph.
Pharmacy Director ASHP Staff
CenterPointe Hospital and Pharmacy
Weldon Spring, MO Justine Coffey, JD, LLM
Director, ASHP Section of Ambulatory Care
Daniel B. Truelove, Pharm.D., BCPS (AQ-ID), Practitioners
BCACP, AAHIVP Bethesda, MD
Clinical Pharmacy Specialist - Ambulatory Care /
HIV
University of Louisville HealthCare
Louisville, KY
Beverly D Weaver, Pharm.D., BCACP, CDE
Clinical Pharmacist/Diabetes Educator; PGY-1
Pharmacy Practice Residency Program Director
Chickasaw Nation Division of Health
Ada, OK
Zachary Weber, Pharm.D., BCPS, BCACP, CDE
Clinical Assistant Professor of Pharmacy Practice
Purdue University College of Pharmacy
Indianapolis, IN
Student
Samantha Schmidt
West Palm Beach, FL
American Society of Health-System Pharmacists | 7272 Wisconsin Avenue, Bethesda, Maryland 20854 | 301-657-3000 14You can also read