Predicting Changes in Depressive Symptoms from Pregnancy to Postpartum: The Role of Brooding Rumination and Negative Inferential Styles
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cogn Ther Res (2013) 37:71–77
DOI 10.1007/s10608-012-9456-5
ORIGINAL ARTICLE
Predicting Changes in Depressive Symptoms from Pregnancy
to Postpartum: The Role of Brooding Rumination
and Negative Inferential Styles
Sarah E. Barnum • Mary L. Woody •
Brandon E. Gibb
Published online: 11 April 2012
Ó Springer Science+Business Media, LLC 2012
Abstract The current study examined the role of cogni- Introduction
tive factors in the development and maintenance of
depressive symptoms from pregnancy into the postpartum Researchers estimate that approximately 7 % of women
period. One hundred and one women were assessed for meet criteria for major depression in the first 3 months
levels of rumination (brooding and reflection), negative postpartum (O’Hara 2009). Even more new mothers (up to
inferential styles, and depressive symptoms in their third 70 %) experience postpartum blues, a milder level of
trimester of pregnancy and depressive symptom levels sadness and associated depressive symptoms, which often
again at 4 and 8 weeks postpartum. We found that, remits within the first 10 days postpartum (Whiffen 1991;
although none of the three cognitive variables predicted Gotlib et al. 1989). In fact, 45–65 % of women report
women’s initial depressive reactions following childbirth experiencing their first depressive episode within 1 year of
(from pregnancy to 1 month postpartum), brooding rumi- giving birth (Moses-Kolko and Roth 2004). Furthermore,
nation and negative inferential styles predicted longer-term infants, toddlers, and school-age children of mothers with
depressive symptom changes (from pregnancy to 2 months postpartum depression are at risk for problems with emo-
postpartum). However, the predictive validity of women’s tion regulation, behavioral and psychological problems,
negative inferential styles was limited to women already insecure attachments, and delays in cognitive and language
exhibiting relatively high depressive symptom levels dur- development (Beck 1996; Murray and Cooper 1997). This
ing pregnancy, suggesting that it was more strongly related risk may be heightened with the mother’s subsequent
to the maintenance of depressive symptoms into the post- depressive episodes (Philipps and O’Hara 1991). Given
partum period rather than increases in depressive symp- that risk for future episodes increases with each depressive
toms following childbirth. Modifying cognitive risk episode experienced (Solomon et al. 2000), these findings
factors, therefore, may be an important focus of interven- suggest that the childbearing years may present a unique
tion for depression during pregnancy. opportunity for prevention and may be a time when vul-
nerable women and their families are likely to be at highest
Keywords Postpartum depression Rumination risk (Philipps and O’Hara 1991).
Inferential style Risk Maintenance A number of researchers have focused on risk factors for
postpartum depression; however, this research has gener-
ally proceeded separately from the larger depression liter-
ature and has typically focused on factors related to the
pregnancy itself (e.g. obstetric complications or hormone
levels) or demographic factors (such as previous history of
psychopathology, socioeconomic status, and parity), with-
out grounding these investigations in existing theories of
S. E. Barnum M. L. Woody B. E. Gibb (&)
depression (cf. Whiffen and Gotlib 1993). Although there
Department of Psychology, Binghamton University (SUNY),
Binghamton, NY 13902-6000, USA is substantial individual variability, childbirth and taking
e-mail: bgibb@binghamton.edu care of a new born are stressful. Therefore, broader
12372 Cogn Ther Res (2013) 37:71–77 vulnerability-stress theories of depression may help to formally evaluated the hopelessness theory within the increase our understanding of which women may be at context of postpartum depression. This said, there is evi- greatest risk for depression postpartum. Much of the dence that one of the three inferential styles featured in the research on depression risk more generally has focused on hopelessness theory—negative attributional styles for the cognitive risk factors. Two of the primary cognitive theo- causes of negative events as defined in the hopelessness ries of depression are the hopelessness theory and the theory’s predecessor, the reformulated theory of learned response styles theory. In the hopelessness theory of helplessness (internal, stable, global attributions; Abram- depression (Abramson et al. 1989), cognitive vulnerability son et al. 1978)—is associated with postpartum depressive to depression is defined as the tendency to attribute nega- symptoms (for a review, see O’Hara and Swain 1996). In tive events to stable, global causes and to infer negative each of these studies, however, it is unclear whether cog- consequences and self-characteristics following the occur- nitive risk factors predict increases in depressive symptoms rence of negative events. An example of this type of neg- following childbirth (development of symptoms) or whe- ative inferential style would be the explaining the ther they predict the maintenance of depressive symptoms occurrence of a negative event in one’s life by saying ‘‘I’m from pregnancy into the postpartum period. Across studies, worthless and can’t do anything right’’. This type of levels of depressive symptoms during pregnancy are one of explanation reflects an attribution of the cause of the event the most salient predictors of postpartum depression (cf. to stable (unlikely to change) and global (likely to affect O’Hara et al. 1991). In fact, forty to fifty percent of many areas of one’s life) factors and implies negative mothers who experience postpartum depression have sig- consequences (additional negative events in the future) and nificant symptoms of depression during their pregnancy negative self-characteristics about the individual. With (Whiffen 1992; Yonkers et al. 2001). regard to the response styles theory (Nolen-Hoeksema Our goal in the current multi-wave prospective study, 1991), the tendency to respond to negative mood by therefore, was to determine whether the vulnerabilities ruminating (or repetitively thinking about why one is featured in the hopelessness theory of depression (negative feeling sad or depressed and the consequences of depres- inferential styles) and the response styles theory (brooding sive symptoms) is hypothesized to contribute to the and reflection) could help to explain risk for postpartum development and maintenance of depression. Although depressive symptoms. In so doing, we specifically exam- early work testing the response styles theory focused on ined the development versus maintenance of depressive rumination generally, more recent research has focused on symptoms from pregnancy to postpartum. We also exam- two distinct components of rumination, brooding and ined women’s functioning at two time points postpartum— reflective pondering. Brooding is defined as ‘‘a passive 1 month and 2 months postpartum—to gain a better comparison of one’s current situation with some unac- understanding of relatively short-term versus longer-term hieved standard’’ whereas reflection is defined as ‘‘a pur- changes in depressive symptoms. poseful turning inward to engage in cognitive problem- solving to alleviate one’s depressive symptoms’’ (Treynor et al. 2003, p. 256). There is growing evidence that Method brooding and reflective rumination are distinct constructs and that brooding represents a more maladaptive form of Participants rumination than reflection, with stronger links to depres- sion (for a review, see Nolen-Hoeksema et al. 2008). Participants were 101 women in their third trimester of Both the hopelessness theory and the response styles pregnancy. Women were only excluded if they were under theory have garnered considerable support for predicting the age of 18 or were unable to read and write in English. the development and maintenance of depressive symptoms The average age of participants in this study was and diagnoses in general community samples (for reviews, 28.44 years (SD = 6.39), and 89 % were Caucasian. Par- see Haeffel et al. 2008; Nolen-Hoeksema et al. 2008). ticipants were generally well educated (53.5 % had a col- However, only one study of which we are aware has lege degree or higher) and had a median yearly household examined the link between rumination and postpartum income of $55,000 (range: \$5,000–[$200,000 per year). depressive symptoms (O’Mahen et al. 2010). This study Fifty-five percent of participants were pregnant with their focused on women with elevated depressive symptom first child and 73.5 % were currently married. levels during pregnancy and found that levels of brooding rumination predicted residual change in depressive symp- Measures toms from pregnancy to three months postpartum among women with low but not high social functioning during Levels of rumination were assessed with the Ruminative pregnancy. In addition, no study of which we are aware has Response Scale (RRS; Treynor et al. 2003). The RRS is a 123
Cogn Ther Res (2013) 37:71–77 73
self-report questionnaire that asks participants to rate the The Edinburgh Postnatal Depression Scale (EPDS; Cox
frequency with which they think or do certain things when et al. 1987) is a 10 item self-report questionnaire of
they feel sad, down, or depressed (e.g., ‘‘Go some place depressive symptoms in pregnancy and the postpartum
alone to think about your feelings’’). The statements are period. Individuals are asked to circle one of four responses
rated on a 4-point Likert-type scale from almost always to for each item, which correspond to increasing symptom
almost never. Given concerns that some of the RRS items severity. Responses to items are summed to create a total
overlap with depressive symptoms, factor analytic studies score (maximum of 30), with higher numbers indicating
have identified two subscales of the RRS—brooding and more severe symptoms. The EPDS was designed to be a
reflection—which are not confounded with depressive screening measure specifically for postpartum women and
content (Treynor et al. 2003). The current study focused on deemphasizes the somatic symptoms of depression, which
these two subscales. Both 5-item subscales have demon- are often experienced due to the pregnancy and birth alone.
strated good psychometric properties in previous research; A cutoff score of 12 or higher exhibits good sensitivity
however, as noted above, the brooding subscale is more (86 %) and specificity (78 %) in detecting depressive
strongly related to depression and related constructs diagnoses in postpartum women (Cox et al. 1987). The
(Nolen-Hoeksema et al. 2008). In the current study, the EPDS has been validated for use in both prenatal and
brooding and the reflection subscales exhibited adequate postnatal women. The EPDS has been shown to be reliable
internal consistency (as = .82 and .76, respectively). and valid across a number of studies (Evins and Theo-
Women’s negative attributional styles were assessed frastous 1997), displays good sensitivity and specificity
with the Expanded Attributional Style Questionnaire (Pet- (Eberhard-Gran et al. 2001; Evins and Theofrastous 1997),
erson and Villanova 1988).1 The EASQ is a self-report is sensitive to changes over time (Cox et al. 1987) and is
questionnaire that presents 12 hypothetical negative events. acceptable to administer over the phone (Zelkowitz and
For each event, the individual is asked to write down what Milet 1995). The EPDS demonstrated good internal con-
she believes would have been the cause of that event and sistency (as = .85, .81, and.83 at T1–T3, respectively).
then to rate that cause in terms of its internality, stability,
and globality. The EASQ was modified for the current Procedure
study in two ways. First, questions were added for each
hypothetical event to assess the other two inferential styles Pregnant women in their third trimester were recruited for
featured in the hopelessness theory—negative inferential this study via advertisements in the local newspaper, flyers
style for the consequences and self-worth implications of at local obstetrician’s offices, and information posted on
each event (i.e., ‘How likely is it that the [negative event] online parenting groups for new mothers. After giving
will lead to other negative things happening to you?’ and informed consent, participants completed the Time 1 study
‘To what degree does the [negative event] mean that you questionnaires (M = 49 days [SD = 28] before the baby’s
are flawed in some way?’). In addition, to reduce partici- birth). Participants then completed measures of depressive
pant burden, only the first six hypothetical negative events symptoms over the phone approximately 1 month
from the EASQ were used in this study. Previous research (M = 35 days [SD = 13]) and 2 months (M = 65 days
has found that equivalent concurrent and predictive validity [SD = 13]) postpartum. Mothers were compensated $25
are obtained using these six items as with the full EASQ for their participation.
(Whitley 1991). Consistent with other research testing the
hopelessness theory (see Haeffel et al. 2008), we created a
composite score by averaging participants’ inferences Results
regarding causes (stability and globality ratings), conse-
quences, and self-implication ratings for each of the Of the 101 women who completed the initial assessment,
hypothetical negative events. For this composite, higher 91 completed the Time 2 assessment and 93 completed the
scores indicate more negative inferential styles. The neg- Time 3 assessment. Given the presence of missing data, we
ative inferential style composite score exhibited good examined whether the data were missing at random,
internal consistency in this study (a = .87). thereby justifying the use of data imputation methods for
estimating missing values (cf. Shafer and Graham 2002).
1
Although negative inferential styles in adults are most commonly Little’s missing completely at random (MCAR) test, for
assessed with the Cognitive Style Questionnaire (Haeffel et al. 2008), which the null hypothesis is that the data are MCAR (Little
five of the 12 hypothetical negative events on this scale focus on and Rubin 1987) was nonsignificant, v2(67) = 65.74,
school work/academic performance, which may be less relevant for a
p = .52. Given this, Multiple Imputation was used to
general community sample of expectant mothers. Therefore, we chose
to use the EASQ instead because it focuses more broadly on negative generate 20 imputed dataset, which were used in all sub-
events that may be more typical for a community sample. sequent analyses. Following the standard approach, the
12374 Cogn Ther Res (2013) 37:71–77
results presented reflect the pooled estimates across these regressions by adding them in block 2 of the regressions.
data sets. This approach yields more reliable parameter Consistent with the recommendations of Joiner (1994), we
estimates than other methods of dealing with missing data, also examined interactions between the cognitive variables
including single imputation methods (see Shafer and Gra- and T1 EPDS scores to determine whether the cognitive
ham 2002). Descriptive statistics and correlations among variables predicted the development versus maintenance of
the study variables are presented in Table 1. We should depressive symptoms into the postpartum period. None of
also note that although the mean level of depressive these analyses were significant, indicating that none of the
symptom decreased across the follow-up, women reported cognitive risk factors predicted women’s short-term
a wide range of symptoms on the EPDS at all three depressive reactions during the postpartum period (lowest
assessment points (0–22 at Time 1; 0–20 at Time 2 and 3). p = .30).
Also, 21 % of women scored above the suggested cutoff of In contrast, the cognitive risk factors did predict longer-
12 (Cox et al. 1987) at Time 1, 7 % scored above this term depressive symptom changes. Specifically, levels of
cutoff at Time 2, and 5 % scored above the cutoff at Time brooding rumination assessed during the third trimester
3. Therefore, although drawn from the community, there predicted residual change in depressive symptom between
was a meaningful range of depressive symptoms displayed the third trimester and 2 months postpartum (T1–T3),
in our sample. t(98) = 2.81, p = .005, pr = .28. The interaction between
Next, hierarchical regression analyses were used to brooding rumination and initial depressive symptom levels
examine short term changes in women’s depressive was not significant, t(97) = 1.02, p = .31, pr = .12, sug-
symptoms from the third trimester to 1 month postpartum gesting that the predictive validity of brooding rumination
(T1–T2). For these analyses, T2 EPDS scores served as the was similar for women exhibiting higher and lower
criterion variable and T1 EPDS scores were entered as a depressive symptom levels at the initial assessment. The
covariate in block 1 of the regression, allowing us to results of this analysis are plotted in Fig. 1, which shows
examine residual change in depressive symptoms from T1 the relation between baseline levels of brooding rumination
to T2. As noted above, we also included women’s marital and residual change in depressive symptoms from T1 to
status and number of children as covariates in these anal- T3. As can be seen in the figure, although levels of
yses. The cognitive risk factors were examined in separate depressive symptoms decreased over the follow-up for the
Table 1 Correlations and descriptive statistics for study variables
1 2 3 4 5 6 7 8 9 10 11 12
1. T1 EPDS –
2. T2 EPDS .41 –
3. T3 EPDS .48 .56 –
4. EASQ .35 .24 .23 –
5. RRS-brooding .61 .26 .48 .42 –
6. RRS-reflection .54 .23 .35 .22 .54 –
7. Age -.25 -.24 -.31 -.17 -.13 -.15 –
8. Caucasian -.08 -.06 -.09 -.02 -.04 -.15 .17 –
9. Income -.49 -.06 -.40 -.13 -.35 -.33 .40 .21 –
10 Marital status -.50 -.23 -.42 -.09 -.31 -.34 .40 .11 .48 –
11. Children (#) .01 -.30 -.17 -.02 -.04 -.04 .42 .08 -.03 .05 –
12. Miscarriage .19 -.01 .07 .00 .15 .03 .06 .02 -.04 -.11 .05 –
Mean 8.07 5.96 4.53 3.33 9.56 8.85 28.81 – – – – –
SD 4.76 4.11 4.12 .88 3.44 3.17 2.20 – – – – –
Median – – – – – – – – $55 K – 0 –
% – – – – – – – 90 % – 74 % – 23 %
EPDS Edinburgh Postnatal Depression Inventory, EASQ Expanded Attributional Style Questionnaire, RRS-Brooding Ruminative Response
Scale—Brooding subscale, RRS-Reflection Ruminative Response Scale—Reflection Subscale. Caucasian was coded so that 1 = Caucasians and
0 = other racial/ethnic groups. Marital status was coded so that 1 = married 0 = unmarried. Children = number of children for each mother
prior to the index pregnancy. Miscarriage was coded so that 1 = prior miscarriage and 0 = no history of miscarriage
Correlations C |.22| significant at p \ .05. Correlations C |.26| significant at p \ .01. Correlations C |.31| significant at p \ .001
123Cogn Ther Res (2013) 37:71–77 75
High EASQ Low EASQ
0
Symtpoms from T1 to T3
Change in Depressive
-1
-2
-3
-4
-5
-6
-7
Low T1 EPDS High T1 EPDS
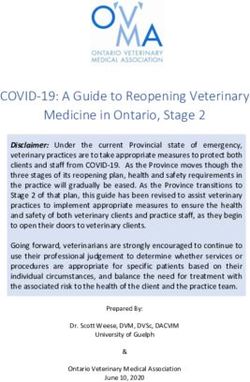
Fig. 2 Summary of inferential styles 9 T1 depressive symptoms
predicting change in depressive symptoms from the T1 (3rd trimester)
to T3 (2 months postpartum) assessment. EASQ Expanded Attribu-
tional Style Questionnaire. EPDS Edinburgh Depression Rating Scale
controlling for the potential influence of women’s age,
race, marital status, family income, number of other chil-
dren in the home, and history of miscarriage, Time 1 levels
of brooding rumination continued to significantly predict
Fig. 1 Prediction of residual change in depressive symptoms from residual change in women’s depressive symptoms from the
the T1 (3rd trimester) to T3 (2 months postpartum) assessment. RRS- third trimester of pregnancy to 4 months postpartum,
Brooding Ruminative Response Scale-Brooding subscale t(92) = 2.75, p = .006, pr = .28. Similarly, controlling
for each of these demographic variables, women’s infer-
majority of women, those with high levels of brooding ential styles continued to predict changes in depressive
rumination experienced an increase in depression during symptoms among those with relatively high depressive
the postpartum period. symptom levels at the initial assessment, t(91) = 2.73,
We also found a significant EASQ 9 T1 EPDS inter- p = .006, pr = .29.
action predicting T3 depressive symptoms, t(97) = 3.35,
p = .001, pr = .34. Examining the form of this interaction
(cf. Aiken and West 1991), we found that women’s infer- Discussion
ential styles predicted residual change in depressive
symptoms among those exhibiting relatively high (?1 SD), The goal of this study was to determine the ability of two
t(97) = 2.98, p = .003, pr = .31, but not low (-1 SD), leading cognitive theories of depression—hopelessness
t(97) = -1.40, p = .16, pr = -.15, depressive symptoms theory and response styles theory—to explain postpartum
at the initial assessment. As can be seen in Fig. 2, although depression risk. Adding to the growing body of depression
the majority of women experienced decreases in depressive research suggesting the important role of brooding rumi-
symptom across the follow-up, those with negative infer- nation (Nolen-Hoeksema et al. 2008; O’Mahen et al. 2010),
ential styles and relatively high levels of depressive we found that levels of brooding rumination predicted
symptoms during their third trimester of pregnancy main- residual change in women’s depressive symptoms from the
tained their levels of depressive symptoms across the fol- third trimester of pregnancy to 2 months postpartum, even
low-up (average EPDS in this group at T3 = 7.60). In after statistically controlling for the influence of demo-
contrast, levels of reflective rumination did not predict graphic variables. Also, adding to the existing literature
residual change in depressive symptoms from T1 to T3, suggesting that brooding rumination is a more maladaptive
either as a main effect, t(98) = 1.18, p = .24, pr = .12, or form of rumination than reflection (see Nolen-Hoeksema
interacting with T1 depressive symptom levels, et al. 2008), the effects were specific to brooding. Although
t(97) = 0.43, p = .67, pr = .05. reflective rumination was significantly related to depressive
Finally, given the strong links observed in previous symptoms concurrently during pregnancy, it did not predict
studies between demographic characteristics and risk for prospective changes in these symptoms. We also found
(postpartum) depression, we conducted additional analyses some support for the hopelessness theory. Specifically,
to determine whether the results reported above would be women’s negative inferential styles also predicted depres-
maintained even after statistically controlling for the sive symptom levels at 2 months postpartum. However,
influence of demographic variables. Even after statistically this finding was limited to women who already had
12376 Cogn Ther Res (2013) 37:71–77
elevated depressive symptom levels during their third tri- of cognitive vulnerability to depression can be applied to
mester, suggesting that inferential styles predicted the the prediction of postpartum depression risk, the multi-
maintenance of symptoms present during the third trimes- wave prospective design, and the specific examination of
ter rather than the development of new symptoms depressive symptom increases following childbirth versus
postpartum. maintenance of depressive symptoms from pregnancy to
In contrast to these results, none of the cognitive vari- postpartum. The study also had several limitations that
ables predicted residual change in depressive symptoms highlight important areas for future research. First, all of
from pregnancy to 1 month postpartum. The reason for this the assessments relied upon women’s self-reports, which
difference in finding is unclear and certainly warrants could have been subject to recall or response bias. Also, the
additional investigation. One possibility is that shorter-term mono-method assessment could have inflated relations
depressive reactions are more strongly influenced by con- among the study variables. Future studies testing cognitive
textual factors (e.g., health of baby, availability of social models of depression risk, therefore, would benefit from the
support, etc.) and that the predictive power of cognitive inclusion of interviewer-administered measures of depres-
risk factors emerges only after this initial period of sive symptoms. Second, although this study focused on
adjustment. Again, future research is need to more clearly leading theories of cognitive vulnerability to depression, we
understand influences on shorter- versus longer-term recognize that there are multiple levels of influence in
depressive reactions following child birth. women’s depression risk during pregnancy and postpartum,
Another finding from this study that warrants discussion is which we did not assess for in this study. Third, building from
that women exhibited the highest levels of depressive cognitive vulnerability-stress models of depression risk, we
symptoms during pregnancy (with 21 % of women scoring conceptualized childbirth as a common stressor shared by all
above the suggested cutoff of 12 on the EPDS). For the the women in our sample. However, the stress associated
sample as a whole, these symptoms reduced across the fol- with labor/delivery and with taking care of a newborn
low-up. However, there was significant variability in this obviously varies considerably across families. Therefore, to
pattern, with approximately 5 % of women still scoring provide a more powerful test of the cognitive models, future
above the cutoff on the EPDS at 2 months postpartum, which research should include a more detailed assessment of the
is consistent with rates of postpartum depression observed in contextual stress experienced by each woman so that these
previous research (for a review, see O’Hara 2009). The cur- idiographic differences can be captured.
rent results suggest that cognitive models of depression may In summary, the current results provide strong support
help to account for which women will maintain their for the role of cognitive risk factors in postpartum
depression following pregnancy (inferential styles) as well as depressive symptoms. They also suggest that inferential
those at risk for experiencing depressive symptom increases styles and brooding rumination may play different roles in
postpartum (brooding rumination). Cognitive models, women’s depression risk (maintenance and development of
therefore, may provide an important area of intervention, as depressive symptoms, respectively). Importantly, however,
many other known risk factors (such as demographic factors) the current results suggest that many women are already
are often difficult to modify during pregnancy. experiencing clinically significant levels of depressive
The current results also raise an interesting and impor- symptoms by their third trimester. Future research, there-
tant question. When is the best time to assess risk and fore, should focus earlier in pregnancy to determine the
intervene to reduce depression in pregnant women? To the most effective window during which to identify at-risk
extent that depressive symptoms are already elevated by women before they develop depression.
the third trimester, this suggests the utility of earlier
screening for depression and depression risk. Indeed, a Acknowledgments This project was supported by National Institute
of Child Health and Human Development grants HD048664 and
limitation of this study is that we did not conduct our initial HD057066 awarded to B.E. Gibb.
assessment until the third trimester of women’s pregnan-
cies. Future research is needed to examine risk precon-
ception and then throughout pregnancy to determine at
References
which point identification of those most at risk can be
maximized. For example, can levels brooding rumination Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopeless-
and/or negative inferential styles be used to predict which ness depression: A theory-based subtype of depression. Psycho-
women are at greatest risk for developing depression dur- logical Review, 96, 358–372.
ing pregnancy, which then may either be maintained or Abramson, L. Y., Seligman, M. E. P., & Teasdale, J. D. (1978).
Learned helplessness in humans: Critique and reformulation.
exacerbated during the postpartum period? Journal of Abnormal Psychology, 87, 49–74.
The current study exhibited a number of strengths, Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and
including the focus on determining whether leading models interpreting interactions. Newbury Park, CA: Sage.
123Cogn Ther Res (2013) 37:71–77 77
Beck, C. T. (1996). A Meta-analysis of the relationship between disorders: Psychological, environmental, and hormonal vari-
postpartum depression and infant temperament. Nursing ables. Journal of Abnormal Psychology, 100, 63–73.
Research, 45, 225–230. O’Hara, M. W., & Swain, A. M. (1996). Rates and risk of postpartum
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of depression—a meta-analysis. International Review of Psychia-
postnatal depression: Development of the 10-item Edinburgh try, 8, 37–55.
Postnatal Depression Scale. British Journal of Psychiatry, 150, O’Mahen, H. A., Flynn, H. A., & Nolen-Hoeksema, S. (2010).
782–786. Rumination and interpersonal functioning in perinatal depres-
Eberhard-Gran, M., Eskild, A., Tambs, K., Opjordsmoen, S., & sion. Journal of Social and Clinical Psychology, 29, 646–667.
Samuelsen, S. O. (2001). Review of validation studies of the Peterson, C., & Villanova, P. (1988). An expanded attributional style
Edinburgh Postnatal Depression Scale. Acta Psychiatrica Scan- questionnaire. Journal of Abnormal Psychology, 97, 87–89.
dinavica, 104, 243–249. Philipps, L., & O’Hara, M. W. (1991). Prospective study of
Evins, G. G., & Theofrastous, J. P. (1997). Postpartum depression: A postpartum depression: 4 –year follow-up of women and
review of postpartum screening. Primary Care Update, 4, children. Journal of Abnormal Psychology, 100, 151–155.
241–245. Shafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the
Gotlib, I. H., Whiffen, V. E., Mount, J. H., Milne, K., & Cordy, N. I. state of the art. Psychological Methods, 7, 147–177.
(1989). Prevalence rates and demographic characteristics asso- Solomon, D. A., Keller, M. B., Leon, A. C., Mueller, T., Lavori, P.
ciated with depression in pregnancy and the postpartum. Journal W., Shea, M. T., et al. (2000). Multiple recurrences of major
of Consulting and Clinical Psychology, 587, 269–274. depressive disorder. American Journal of Psychiatry, 157,
Haeffel, G. J., Gibb, B. E., Metalsky, G. I., Alloy, L. B., Abramson, L. 229–233.
Y., Hankin, B. L., et al. (2008). Measuring cognitive vulnera- Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumina-
bility to depression: Development and validation of the Cogni- tion reconsidered: A psychometric analysis. Cognitive Therapy
tive Style Questionnaire. Clinical Psychology Review, 28, and Research, 27, 247–259.
824–836. Whiffen, V. E. (1991). The comparison of postpartum with non-
Joiner, T. E., Jr. (1994). Covariance of baseline symptom scores in postpartum depression: A rose by any other name. Journal of
prediction of future symptom scores: A methodological note. Psychiatric Neuroscience, 16, 160–165.
Cognitive Therapy and Research, 18, 497–504. Whiffen, V. E. (1992). Is postpartum depression a distinct diagnosis?
Little, R., & Rubin, D. (1987). Statistical analysis with missing data. Clinical Psychology Review, 12, 485–508.
New York: Wiley. Whiffen, V. E., & Gotlib, I. H. (1993). Comparison of postpartum and
Moses-Kolko, E. L., & Roth, E. K. (2004). Antepartum and nonpostpartum depression: Clinical presentation, psychiatric
postpartum depression: Healthy mom, healthy baby. Journal of history, and psychosocial functioning. Journal of Consulting
the American Medical Women’s Association, 59, 181–191. and Clinical Psychology, 61, 485–494.
Murray, L., & Cooper, P. J. (1997). Postpartum depression and child Whitley, B. E. (1991). A short form of the Expanded Attributional
development. New York: Guilford Press. Style Questionnaire. Journal of Personality Assessment, 56,
Nolen-Hoeksema, S. (1991). Responses to depression and their effects 365–369.
on the duration of depressive episodes. Journal of Abnormal Yonkers, K. A., Ramin, S. M., Rush, A. J., Navarrette, C. A.,
Psychology, 100, 569–582. Carmody, T., March, D., et al. (2001). Onset and persistence of
Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). postpartum depression in an inner-city maternal health clinic
Rethinking rumination. Perspectives on Psychological Science, system. American Journal of Psychiatry, 158, 1856–1863.
3, 400–424. Zelkowitz, P., & Milet, T. H. (1995). Screening for postpartum
O’Hara, M. W. (2009). Postpartum depression: What we know. depression in a community sample. Canadian Journal of
Journal of Clinical Psychology, 65, 1258–1269. Psychiatry, 40, 80–86.
O’Hara, M. W., Schlechte, J. A., Lewis, D. A., & Varner, M. W.
(1991). Controlled prospective study of postpartum mood
123You can also read