Quality Account Photo courtesy of Mark Norman, BBC South East Today, Health Correspondent
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2020-21
Quality
Account
Photo courtesy of Mark Norman,
BBC South East Today, Health Correspondent 1
Contents
Foreword 4
Overview 4
About us 7
Our vision and values 9
Clinically led 9
Achievements in quality Statement on quality from the Chief Executive 11
CQC Registration 14
Delivering high quality care during the pandemic 15
SASH+ impact on quality of care 18
Quality priorities for improvement in 2021-22 19
Our Priorities
Safe Priority Overview 22
Incident reporting 22
Never Events 23
Falls 24
Healthcare Associated Infection 25
Pressure Ulcer prevention 30
Medicine safety 31
Safeguarding 31
Effective Priority: Overview 34
Clinical Audit 35
VTE (Venous Thromboelism) 38
Learning from Death 39
Research 42
Well-led Priority: Overview 46
Our people 46
National Staff Survey 46
Staff Friends and Family test 46
Developing our staff 49
Staff engagement 51
Equality and Diversity 51
Black, Asian, Minority Ethnic (BAME) staff 53
Freedom to Speak Up Guardian 56
Guardian for Safer Working 56
Information Governance 56
Payment by results 56
Data Quality 56
Income generated 57
Caring Priority: Overview 59
Patient Experience 59
COVID-19 60
Dementia 61
2
Personal needs 62
Responsive: Overview 65
Cancer waiting times 65
Referral to treatment standard 66
Cancer and Site Services Division
Compliance with the mental health act 67
Statement of directors responsibilities
Annexes Annex 1:
Stakeholder review 70
Annex 2:
Quality Account Indicator definitions 71
Conclusion pages Putting people first 75
Keep in touch 75
3
Foreword
Photo courtesy of Mark Norman,
BBC South East Today, Health Correspondent
Welcome to the Surrey and Sussex Healthcare The impact on all aspects of our teams’ work
NHS Trust Quality Account 2020/21, where has been immense. Words used to describe
you can read details about our performance, what our community and our staff went through
achievements and our plans for the coming year. do not really do them justice but we will try. We
It is a pleasure to be able to share with you so quadrupled our critical care capacity, converting
many examples of how our people are making a medical wards into spaces that could provide care
positive difference for our patients. for some of our most critically unwell patients. We
reorganised our estate and our services to create
This has been a year like no other. The COVID-19 the best environment possible to provide the care
pandemic has been the single greatest challenge our patients’ needed. At the same time, many staff
to public health and the NHS in a generation. adapted their roles to work in unfamiliar areas.
Our staff have responded with skill, dedication,
courage and compassion in abundance.
4
quality, safe care. As part of our approach to
this, we launched our response to the National
Patient Safety Strategy in the form of our ‘Safe
SASH’ campaign to coincide with World Patient
Safety Day in 2020. Alongside our established
Trust governance mechanisms, this encouraged
every department to make safety pledges based
on their safety and quality data. We were so
pleased to see how this was met with enthusiasm
and engagement from staff across all grades
and departments. To take this work onto the
next stage, we have now developed Trust-wide
safety goals as we look to continue to provide the
highest possible quality of care for our community,
always asking ‘in what way can we do better?’
With visiting to our site greatly restricted during
the pandemic, we have had to work in very
different ways to ensure loved ones could keep
in touch with relatives and carers. We rapidly set
up a messaging service to make sure that people
could send in correspondence for patients to read.
We invested in new technology to support all our
wards to provide video calls with loved ones. We
were shortlisted for a prestigious Nursing Times
award in the category of ‘care of older people’ for
a process we introduced to ensure relatives were
regularly updated on our patients’ conditions.
Alongside this, we were proud to continue to offer
visiting in exceptional circumstances wherever
possible.
During the year we were proud to have made
major contributions to national and international
research studies as part of our efforts to respond
to the pandemic. We recruited over 300 patients
Throughout this response we have taken pride in to the RECOVERY trial; the biggest global study
continuing to place great importance on the quality to find treatments to help coronavirus patients.
of care we have provided. We recruited the largest number of patients in the
country to the COVID:HAREM study looking to
On the one hand, this involved responding improve understanding of changes in treatment for
rapidly to changing guidance and requirements appendicitis, cholecystitis, pancreatitis and cancer
specifically related to the virus – medical and surgery. We were the third biggest contributor
nursing teams, allied health professionals, to CHOLE:COVID cholecystitis audit, while also
housekeeping, estates and facilities staff, contributing hundreds of data sets as part of
procurement and administrative staff all played an international effort to characterise severe
vital roles in this. emerging infections within the ISARIC study.
SASH+, our established approach to Quality
On the other hand, there was a very real need Improvement, has been invaluable throughout our
to ensure focus remained on providing high response.
5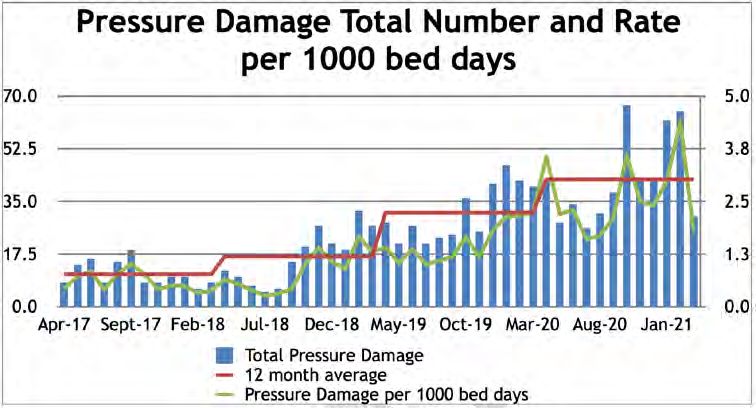
Richard Shaw Michael Wilson CBE
Chair Chief executive
We used our methods to support the supply We are very proud of our contribution to the
of personal protective equipment (PPE), to pandemic response and are pleased to reflect
decontaminate kit, to introduce twice-weekly many of our achievements within this account.
lateral flow tests for our staff and latterly to design In reflecting on these achievements, we also
and deliver our vaccination programme. remember those most affected by the last year.
Our colleagues, relatives, friends and patients
Alongside all of these efforts, we have placed a who lost their lives during the year remain at the
great deal of importance on the wellbeing of our forefront of our minds.
staff. Clearly the efforts of the last year have,
and will continue to have, a profound impact on
our teams. We have taken steps to provide them
with as much support as possible. Our peer-to-
peer Critical Incident Stress Management team
has been invaluable, and we have supplemented
this by investing in additional psychological
support. We have created new wellbeing spaces Richard Shaw
and created dedicated information about where Chair
to seek help and support. Our chaplaincy and
spiritual care team have provided immeasurable
support to colleagues of all faiths and none,
alongside the role they play in supporting
relatives, patients and carers.
We took a thorough approach to the ensuring
every member of our staff received a personal Michael Wilson CBE
COVID-19 risk assessment and we have put on Chief executive
a number of listening events, both trust-wide and
dedicated to different groups of colleagues. It is
paramount that this work continues and increases June 2021
over the coming months as our colleagues
continue to process the impact of our response.
Portrait photos displayed on this page were taken prior to
the pandemic
6
About us
Population of
535,000
Population of
535,000
5,000 • East Surrey Hospital, Redhill
staff
5,000
staff •• East Surrey Dene
Caterham Hospital, Redhill
Hospital
800 •• Caterham
Earlswood Dene Hospital
Centre
800
•• Earlswood Centre
beds
beds Crawley Hospital
• Crawley Hospital
14
14
operating
•• HorshamHospital
Horsham Hospital
operating
theatres
theatres
Croydon
Croydon
M20
M20
Woking M25
Woking M25
Caterham Dene Hospital
Caterham Dene Hospital
Guilford Earlswood
Guilford Earlswood East Surrey Hospital
East Surrey Hospital
Tonbridge
Tonbridge
Crawley Hospital Tunbridge
M23
Wells
Crawley Hospital Tunbridge
Horsham Hospital
M23
Wells
Horsham Hospital
7
Surrey and Sussex Healthcare NHS Trust (SASH)
provides acute and complex services at East
Surrey Hospital in Redhill alongside a range
of outpatient, diagnostic and planned care at
Caterham Dene Hospital, The Earlswood Centre
in Surrey and at Crawley and Horsham Hospitals
in West Sussex. Serving a growing population of
over 535,000 we care for people living, working
and visiting east Surrey, northeast West Sussex,
and south Croydon, including the towns of
Crawley; Horsham; Reigate and Redhill.
East Surrey Hospital is the designated hospital for
Gatwick Airport and sections of the M25 and M23
motorways. It has a trauma unit, which cares for
seriously injured patients in partnership with the
major trauma centres at St George’s University
Hospitals NHS Foundation Trust, Tooting, and
Royal Sussex County Hospital, Brighton. East
Surrey Hospital has 800 beds and ten operating
theatres, along with four more theatres at Crawley
Hospital and a day surgery unit.
We are a major local employer, with a diverse
workforce of over 5,000 staff providing healthcare
services to the communities we serve. The Trust
is an Associated University Hospital of Brighton
and Sussex Medical School and we are part of
educating cohorts of final year medical students
from the school each year under the supervision
of our consultants. Our involvement supports the
medical workforce of the future and the delivery of
high-quality patient care.
8
Our vision Our values
We will pursue perfection in the delivery Dignity and respect: we value each
of safe, high quality healthcare that puts person as an individual and will challenge
the people in our community first. disrespectful and inappropriate behaviour.
One team: we work together and have
a can-do approach to all that we do,
recognising that we all add value with equal
worth.
Clinically led
We are a clinically led organisation, Compassion: we respond with humanity
focused on putting people first. Our and kindness and search for things we can
services are led and managed through do, however small; we do not wait to be
four divisions. Each division is led asked, because we care.
by clinical staff, chiefs who are also
members of our executive committee. Safety and quality: we take responsibility
(see below) for our actions decisions and behaviours in
delivering safe, high quality care.
Cancer and Women and
Medicine Surgery
diagnostics children
Dr Tony Newman- Mr Ian Miss Karen Jermy
Chief Sanders
Dr Ben Mearns
Maheswaran
Associate Riyadh Seebooa
Alison James Cynthia Quainoo Natasha Hare
director
Michelle Cudjoe
Divisional Chief Hannah
Paula Tooms Jamie Moore (Director of
Nurse Thompsett
midwifery)
Key strategic and cross divisional themes are also
led by Clinical Chiefs
Chief Clinical Informatics Officer:
Dr Tony Newman-Sanders
Chief of Education:
Dr Sarah Rafferty
Chief of Innovation:
Dr Des Holden
9
Achievements in quality10
Achievements in quality Michael Wilson CBE
After the year that has just passed, it is a Chief executive
testament to the dedication of our staff that there
is much to describe in our achievements in quality.
I am very proud that, despite all that the pandemic
brought us, the focus on the quality of service we
provide has remained, with colleagues across
all areas working so very hard and continuing to
demonstrate the Trust’s values and behaviours.
Within this report you will be able to read many
examples of how our staff responded to the rapidly
evolving pandemic situation with adaptability and
innovation that was truly inspiring. From clinicians
enrolling patients in clinical trials and then
implementing new treatments and procedures
as knowledge about Covid-19 developed, to staff
working in unfamiliar environments such as our
expanded Intensive Care Unit, the Kaizen team
using SASH+ techniques to optimise various
pathways, the communication department relaying
important messages across the organisation
and the facilities team keeping all areas clean
and safe, everyone played an important role.
There were two innovations that reached national
attention as examples of outstanding practice.
The pharmacy, nursing and kaizen teams
designed a process of making up intravenous
antibiotics in a clean area, away from the wards,
and then delivering these to nursing staff ‘just safety strategy into targeted safety goals agreed
in time’, to release more time for direct patient by each division and corporate service and work
care, at a stage of the pandemic when antibiotic is underway to improve our safety performance
use was very high. During the second peak of against these. In line with the strategy, we have
the pandemic all admitted patients were given a appointed two patient safety specialists who have
letter from the Chief Nurse and Medical Director undergone the required training and are working
explaining the risks of exposure to Coronavirus with the corporate and divisional teams. We
and how they could help protect themselves have created the roles of patient safety partners
whilst in hospital by social distancing, strict hand (members of our local community who will help
hygiene and wearing a surgical mask at all times, guide and advise us) and we are looking to recruit
whenever possible, with the masks prescribed on these partners over the coming months.
patient drug charts, this was commended by NHS
England. It is no surprise that this year there was an ever
greater focus on infection prevention and control
Last year we set out a range of quality priorities. (IPC). During the year we had a visit from the
For patient safety we committed to implementing IPC team at NHS England and a focused IPC
the new national patient safety strategy. The inspection by the CQC. Both of these visits gave
safety section of this report sets out the progress very positive feedback about the work of our
we have made in that regard. The Trust has a staff during the challenging times they faced,
strong focus on learning from any safety incident particularly their attention to IPC measures and
and then sharing that learning, so it is particularly the quality of care provided. The Trust Covid-19
pleasing to see the results of the latest national vaccination programme has been very successful,
NHS staff survey: 91% of our staff agreed that designed and co-ordinated by our Pharmacy and
the Trust encourages incident reporting and 95% Occupational Health teams. All of our staff were
of staff would know how to report any incident of offered two doses of the vaccine and we extended
unsafe clinical practice. We have incorporated the
11this to other health and social care workers in our launched our new mental health strategy, after
local area and some of our vulnerable inpatients. consulting widely with external partners and our
community, with our underlying principle being
Last year we committed to improving our parity of esteem between physical health needs
response to learning from deaths by improving and mental health needs. In October we hosted a
the categorisation of deaths and also to maintain week long joint event with our local mental health
a better than expected mortality rate. We have provider, organised around the SASH+ principles
fully implemented the Medical Examiner system and attended by a diverse range of staff from both
by which all patient deaths at the Trust are organisations, representatives from the charitable
reviewed by a senior doctor not involved in sector, patients and carers. As a result of the work
their care and the patient’s family is involved in started in that week patient pathways have been
this review. Despite the pandemic leading to a optimised and joint working between us as the
significant overall increase in deaths, we met acute Trust and our local mental health provider
our improvement target of 75% of deaths being has improved significantly, with more work
categorised. This then identifies which need a planned to join us together even more closely, for
more in depth review to identify and share any the benefit of our community. There is more work
learning. Our mortality rate has remained better to be done, particularly in how we work across
than expected during this period. the system to tackle the increasingly unmet need
of mental health provision for children and young
We continue to be active in clinical research and people.
this was even more the case during the pandemic.
We were able to recruit more than 2,500 patients One of the groups within our community that
to research studies, many of which helped the was disproportionately affected by the pandemic
NHS and the wider world rapidly gain important for complex reasons was people with a learning
insights into Covid-19 and defined which disability. This year we launched our Learning
treatments were effective and which were not. Disability Strategy, after consulting widely,
including with patients and carers. Our Chief
One of our priorities last year was to ensure Nurse is working with partners across the system
inclusion was at the heart of all that we do, with at improving the integration of care for patients
a focus on the diversity of our staff, particularly with a learning disability. We have set up a
those from overseas or from a Black, Asian or working group, led by our Nurse Consultant /
Minority Ethnic background (BAME). We have Head of Safeguarding which is improving how
made progress in this regard. We have appointed we interact with patients. In outpatients we have
to the new post of Head of Inclusion who is set up a process that, prior to a forthcoming
already driving this work forward through our appointment, a senior nurse contacts patients
Inclusion Steering Group. We have a thriving with a learning disability and/or their carer and
BAME network where peer to peer support and finds out from them about any specific needs they
executive led listening events proved invaluable may have which can then be facilitated when
during the pandemic, advising and supporting staff they attend. We also launched the ‘Sunflower’
around Covid risk assessments, vaccinations and lanyards, in response to specific feedback, that
the understandable concerns about the possible patients can choose to wear to identify that they
effect of ethnicity on the risk of Covid. The Director have a disability or specific needs that may not be
of Corporate Affairs at SASH has also been visible to our staff, and this has been supported
appointed as the Surrey Heartlands Executive with additional staff training.
Sponsor for BAME issues and Chair’s the BAME
Alliance leading the work on inclusion across our The final quality priority we set ourselves last
local health system. We have launched our new year was to recover the timeliness of urgent and
LGBT+ staff network and introduced SASHability elective pathways following the pandemic and to
and Carer’s passports for staff. focus on delivering national access standards.
This is currently a high profile challenge across
Last year we set the ‘caring’ priority of being the NHS and there is still much work to do in
responsive to the needs of our whole community, this regard, which will take time, but we have
including by improving access to our services made significant progress towards recovery,
and the care provided for people with a learning working across all departments, the local health
disability or a mental health problem. In 2020 we system, the independent sector and with the
12national team. Our Emergency Department 4
hour performance at 94.6% made us one of the
best performing Trusts in the country. We are now
meeting all the national cancer access targets
except the need for 85% of patients to begin their
definitive treatment within 62 days of referral.
We continue to improve this performance and
prioritise the most time critical treatments.
The main standard for routine care is that 92%
of patients should wait less than 18 weeks from
referral to receiving planned treatment. As routine
treatments were suspended across the country
during the pandemic waiting lists have grown and
by the end of February 2021 we had over 800
patients waiting over 52 weeks. We now continue
to drive this down and at the time of writing the
number is 259 with more work to do over the
coming months.
As you will see through the rest of this report,
so much has been achieved this year. None of it
would have been possible without the hard work,
commitment and the focus of SASH colleagues
across our whole team on safety, quality of care
and patient experience. I commend this quality
account to you as evidence of this and with my
thanks.
Michael Wilson CBE
Chief executive
June 2021
13CQC registration
The Trust is rated as Outstanding overall by
the CQC and is registered with the CQC with
no conditions attached to its registration. This
includes overall Outstanding ratings for Well Led;
Caring; Responsive and the Use of Resources.
The Trust was inspected throughout quarter three
2018-19.
The Trust’s maternity, medical care (including
older peoples’ care) and surgery services were
rated as Outstanding overall. All other services
were rated as Good.
During 2020-21 the Trust continued to liaise
with the CQC as part of their ongoing monitoring
processes.
Surrey and Sussex Healthcare NHS Trust
is required to register with the Care Quality
Commission and its current registration status is
compliant.
The Care Quality Commission has not taken
enforcement action against Surrey and Sussex
Healthcare NHS Trust during 2020-21.
Surrey and Sussex Healthcare NHS Trust was
included in part of national programme of CQC
inspections in March 2021, focussing on Infection
Control. The report has been published and
identifies areas of outstanding practice, good
overall compliance. No immediate concerns were
identified or reported to the Trust; the report does
include areas for improvement.
14Delivering high
quality care during
the pandemic
15COVID-19 has had a significant impact on NHS with COVID screening such as the day 3 and
care and services for people with other health day 6 screening. Targeted work has improved
needs, and how it has affected the capacity and adherence with this. Wards have demonstrated
resilience of the health and care system. Surrey significant improvements with compliance now
and Sussex Healthcare NHS Trust has throughout over 90% in the majority of areas.
the pandemic ensured that pathways, systems
and processes have been regularly reviewed in Throughout the outset of the pandemic there have
conjunction with national guidance to ensure the been agreed pathways to ensure the segregation
safety of patients, staff and visitors. of patients through use of COVID and non-COVID
allocated areas and pathways to support minimal
The Trust has focused much effort on minimising movement unless clinically imperative and also
the risk of hospital transmission of COVID-19 to minimising contact between pathways. Key
during the 2020-2021 pandemic. PHE guidance to this is the essential triaging and assessment
has been followed throughout the pandemic with of infection risk at the front door so patients are
guidance regularly reviewed for changes and streamed appropriately alongside the benefits
disseminated throughout the organisation. of the LumiraDX screening protocol. The clinical
All key mitigation measures have been focused leads engagement and input to pathways has
on and continue to be to ensure safe high quality been imperative and to the regular review of
healthcare for SASH patients. pathway effectiveness, (adapting where required)
particularly in the context of fluctuating COVID
National guidance on patient COVID-19 prevalence; this clinical steer has been crucial
microbiological testing was regularly reviewed and engagement continues as part of the Trusts
and implemented with increasingly available response to the COVID-19 pandemic.
testing capacity through various testing platforms
throughout the pandemic. In addition to routine At times of high organisational prevalence
COVID-19 testing where test turnaround times of COVID there have been periods where
have been 24-48 hours (off site testing), the Trust cohorting of COVID patients has been required
has benefited from the availability of rapid on-site and this has been implemented in the context
PCR testing for COVID-19 which has supported of application of infection prevention control
the quicker turnaround of results, supporting the principles and monitoring of practice. This has
screening and timely diagnosis and appropriate been in conjunction with the IPC team’s regular
placement of patients. In November 2020 daily collaboration with the director of infection
we became one of the five Trusts in the early prevention control, consultant microbiology,
adoption programme of the Lumira DX screening head of operational flow and site team and
platform, allowing us since 16 December 2020 to also reviewed at regular tactical and strategic
have 12 minute turnaround results for COVID in COVID-19 meetings. Risk assessment in the
our Emergency Department, allowing much safer context of COVID-19 and patient safety has
streaming of patients. consistently been applied in decisions affecting
the patient pathway.
Trust protocols are in place for re-testing
negative in-patients on Day 3 and Day 6 and
weekly screening as per PHE guidance. There
Infection Prevention Control
The Director of Infection Prevention Control
are additional protocols for regular testing and
(DIPC) and IPC team has played a key role
availability of rapid testing where patients are
in collaboration with key stakeholders as one
having higher risk procedures (which would
team in advising on pathways and operational
increase transmission risk if positive) or where
flow of patients, and reviewing, communicating
patients may develop symptoms during admission
and educating on changing national Infection
(incubating on admission). In addition elective
Prevention Control guidance throughout the
SOPs are in place for elective surgical procedures
pandemic.
and also a process to ensure pre discharge
screening is in place for transfers to other care
Since the outset of the pandemic national
settings (e.g. Nursing home). We have worked
guidance has been implemented and monitored.
closely with our information and performance
Ensuring the provision and education on the
team who have been instrumental in designing
reports to enable us to monitor compliance
16correct use of personal protective equipment patients also through emphasis on all those key
(PPE) for staff was a priority including how to measures such as distancing, hand hygiene and
put on and remove PPE safely. Our standard face mask use. Patient mask use continues to be
FIT testing programme for FFP3 respirators actively promoted as per PHE guidance.
was escalated to ensure the Trust were meeting
Health and Safety and IPC requirements for the Mask use has been challenging and the Trust
fitting of respirators. A large part of work involved recognises that not all patients are able to wear
the procuring of hood respirators for those that masks due to clinical compromise or confusion
could not wear a respirator or failed a fit test for example. Since January 2021 all admitted
as an alternative option for staff. Procurement patients are given a letter from the Chief Nurse
has made monumental efforts throughout the and Medical Director setting out what they can
pandemic to ensuring the provision of PPE do to help protect themselves, such as hand
through procurement, monitoring of stocks and hygiene and mask wearing and the Trust has
liaising regularly at tactical and strategic meetings also implemented mask prescriptions to support
on the PPE situation. This has been fundamental compliance.
in the provision of appropriate PPE for staff
throughout the pandemic including at times of The Trust has focused much effort on reducing the
extreme national demands on PPE supply and the risk of healthcare onset COVID-19. Where cases
challenges this posed. have fulfilled definition for nosocomial COVID this
has been reported as per national requirements.
The Trust Kaizen team have played a significant Despite all key IPC measures we have had
role in implementing and transforming various ward outbreaks particularly in the context of
processes during the pandemic in collaboration the high organisational prevalence of patients
with the key stakeholders of that process. The admitted with COVID-19 and also patients
use of kaizen methods and implementation with asymptomatic infection or atypical clinical
of standard work for managing the significant presentation. During the second COVID-19 surge
numbers of hood respirators for staff was a key outbreaks reflected the high infectivity of the virus,
example of this in developing the ‘hood hub’. particularly the ‘Kent’ variant which became our
National guidance was followed with the use of endemic variant. The Trust ensured systems for
fluids-resistant surgical masks (FRSM) for all active follow up and isolation of COVID 19 cases
staff and use escalated throughout the pandemic and contacts to reduce the risk of onward spread
from use for caring for patient with suspected/ and also embedded systems to identify contacts
confirmed COVID, to use in all clinical areas and who may be readmitted. Any ward outbreaks are
then extending to all settings including non-clinical declared, reported and investigated and regular
settings. Current policy remains for all staff to outbreak meetings were held chaired by the DIPC.
wear FRSM.
The Trust has reviewed and continues to review
The communications department has been contributory factors and lessons from COVID-19
instrumental in communicating COVID messaging nosocomial cases and outbreaks to reducing
and in the production of visual reminders on key risk further for future potential COVID-19
policy points. surges. The trust has promoted use of natural
ventilation and trialled the use of air filtration
As part of assurance that COVID-19 IPC practice units to reduce the risk in multi-occupancy patient
and guidelines were being adhered to systems settings and IPC are working in conjunction with
were implemented to ensure monitoring of IPC Estates in assessing the estate to direct ongoing
practices including ward based daily COVID interventions to improve ventilation and meet
checks, weekly matrons audits and IPC nurse the environmental requirements as set out in the
auditing. The senior leadership team were also current PHE guidance.
engaged in check and challenge opportunities.
COVID-19 was incorporated as an integral part of Staff Lateral Flow testing has been in place since
IPC training sessions and regularly reviewed for the first week of December for twice weekly
updates. testing including bank and agency staff and
systems to monitor LFD uptake, compliance with
Not only has there been emphasis on the testing and positivity data. Staff uptake of LFD
importance of staff compliance with measures but testing is >90%.
17The Facilities team has played an extraordinary COVID-19 key mitigation measures continue
role implementing the additional cleaning required to be applied and monitored and the Infection
during this COVID-19 pandemic. In addition to prevention and control board assurance
attention cleaning standards and frequencies framework (assessing Trust compliance with
this has included the additional procurement of National Public Health England COVID-19
UV technology and also hydrogen peroxide to Infection Prevention Guidance) remains under
provide additional assurances regarding cleaning. regular review.
The UV technology has contributed to additional
decontamination assurances not only for the The safety and quality care of patients remains at
environment but also equipment such as hood the core of the Trust services and in the ongoing
respirators. There has been a focus on all staff monitoring and response to the ever changing
responsibilities for cleaning of high touch surfaces COVID-19 pandemic. Pandemic planning is
with provision of guidance, schedules and a key action area in the IPC strategy and the
monitoring to support compliance. experiences of the SARS CoV-2 will be used to
inform future pandemic preparedness for future
emerging diseases.
Antibiotics and healthcare
associated infection SASH+ impact on quality of care
Antimicrobial usage has increased in the
In March 2015, the NHS Trust Development
last 12 months; this is likely due to increased
Authority, now part of NHS Improvement, invited
numbers of bacterial co-infections in patients
expressions of interest from NHS Trusts to be
with COVID-19 during the pandemic. There has
part of a five-year development partnership,
been an increased usage of broad spectrum
which aimed to fundamentally improve the quality,
antibiotics, but this is largely in line with the
performance and financial sustainability of the
Trust antimicrobial guidelines for pneumonia. An
organisations selected to take part as well as
increase in healthcare associated infection (HCAI)
share learning with others.
has been noted for some infections and a positive
correlation observed with COVID-19 incidence.
Over the six years SASH, along with four other
HCAI cases are investigated through use of
Trusts have been working in partnership with the
root cause analysis (RCA). Understanding the
Virginia Mason Institute (VMI) in Seattle, USA who
impact on healthcare associated infections and
have developed a transformational management
its impact on HCAI continues to be investigated. A
system - the Virginia Mason Production
retrospective audit of COVID-19 and co-bacterial
System, which is based on lean methodological
infections is underway.
improvement techniques adopted and adapted
from the Toyota car manufacturing factory in
We monitor antimicrobial prescribing through our
Japan. Over the last 20 years the Virginia Mason
monthly Good Antimicrobial Prescribing (GAP)
Production System has enabled them to become
audit, and the results in the last 12 months have
one of the safest and highest rated hospital
been variable between divisions. Currently we are
organisations in the USA.
working on improving how we act on GAP results,
particularly when there are identified areas for
Our aim at SASH is to pursue perfection, putting
improvement. The AMS team are introducing
our patients at the forefront of everything we
antibiotic ward rounds to ensure a thorough
do, improving safety and quality by reducing
review of antimicrobial treatments in target areas
variation and waste in every process. SASH+ is
as identified by the GAP audit. Overall, we are
defined as a management system with an inbuilt
aiming to reduce antibiotic usage and ensure they
quality improvement methodology enabling
are prescribed appropriately, in line with NICE
kaizen to happen every day. Our SASH+ work
AMS guidance.
supports an accelerated transformation in quality
by providing us with a structured approach to
continue our improvement journey and has helped
to take us from being a CQC rated “good” to an
Ongoing care “outstanding” organisation.
Reducing risk of nosocomial COVID-19 remains
a priority for SASH alongside reduction in risk
Our Kaizen Promotion Office (KPO) team lead
of unintended consequences such as HCAI.
18SASH+; providing the structure, methods and The delivery and allocation of portable
rigor behind the successful implementation of oxygen cylinders with clear transparent
our management system, alongside training and processes for useage, delivery, cleaning
developing staff from across the organisation to and return
lead using their new skills and methods. Reporting of covid results to patients who
had been discharged from the hospital
Distribution of gifts and donations to staff
Education and training across the hospital
To share and embed a sustainable culture of
continuous improvement across the Trust, staff
We are very proud of the significant and
from Board to ward are undertaking a variety of
sustainable transformation changes we have
SASH+ training and development programmes.
successfully made and look forward to continuing
to improve the high quality of care we provide to
Kaizen and covid local people. This is reflected in the recent CQC
Over the last year the team have been deployed report:
across the Trust using SASH+ principles to
design, develop and implement to respond to “The SASH+ quality improvement programme
issues which have been highlighted by COVID-19. has empowered staff by equipping them with
The team designed and implemented a process the lean tools, methods and a structured
for the receipt, allocation, training and reporting process which has very successfully built a
of lateral flow tests for 5500 trust staff, students, culture of continuous improvement across
on site contractors, maternity patients and their the whole Trust. Investment in improvement
partners. They also develop a process for the and training has been a priority and this
effective management of FFP3s and powered had resulted in a culture where staff at all
air respirator packs and non powered respirators grades and from all disciplines felt involved
which included, the stock management, allocation, and enthused by the work streams and the
training, decontamination and maintenance of idea that they could make a real difference to
more than 250 items. The process ensured that patient safety and the patient experience”
staff had 24/7 access to effective PPE which was
decontaminated after use and always kept in good (CQC inspection report 2019)
working order. We are also proud of the empowering impact
involvement in making change has on individuals
In addition to these developments the team have and teams and feel that this is reflected in how
also worked in the following areas:- our staff rank the organisation in the national NHS
Staff Survey.
Designing and delivering a responsive
Family liaison service for patients in ICU
The development of an IV antibiotics
Quality Priorities for
reconstitution service which provided Improvements for 2021-2022
access for patients to anti biotics in a more In developing our priority areas we considered
timely way our key strategic challenges and national
The development and implementation of areas of focus including implementation of
a Clinical support hub which enabled non the National Patient Safety Strategy and the
clinical staff to support clinical areas potential impact of the COVID 19 pandemic on
Gown cleaning which implemented a safe the services we provide. We then considered the
process for the decontamination and re-use potential solutions and have these within our
of single use gowns priorities including developing engagement and
The design and development of a COVID ensuring our services are inclusive for protected
vaccination service which ensured a high characteristics.
quality responsive service was provided
with no queues This was done at all levels within the organisation
Revised patients property processes to with our staff through a mix of team meetings as
support the delivery of property to patients well as through monthly team talk discussions and
on wards when visiting by relatives was at Trust Board level. The priorities were developed
restricted during the initial period of disruption caused by
19pandemic and as such the views of our patients the Safety and Quality Committee will
and public were not able to be canvassed. These receive updates on the implementation of
priorities were taken to our Council of Governors, the national patient safety strategy,
for discussion at the beginning of the financial Mortality (HSMR) as an indicator will be
year as part of our Operating Plan review process. monitored by the effectiveness committee
The Council of Governors are representative of and will be regularly reviewed by the Board
our community and the population who use our the responsiveness of our services,
services. particularly recovery following the
disruption of the pandemic will be
For safe: monitored by the Safety and Quality
Committee and the Board.
Infection Prevention and Control is a top priority
for the Trust with a focus on good antibiotic
stewardship.
Improve the reporting of No harm and Near Miss
incidents and begin early implementation of the
national patient safety incident framework.
For effective:
To improve the fractured neck of femur pathway
ensuring timely access to surgery and outcomes
measured by the national hip fracture database
To improve clinical audit outputs and quality
improvement projects resulting from audits
For well led:
To increase midwifery staffing levels and further
improve midwife to birth ratio
Improve areas of equality, diversity and Inclusion
for our staff with a particular focus on the
workforce race equality standards
For caring:
To consistently meet the Trust goal in relation to
responding to patient complaints
To further enhance the patient voice by developing
our patient safety partners
For responsive:
We will recover and restore the timeliness of
urgent and elective pathways following the impact
of COVID-19 and focus on delivering national
access standards.
We will address areas of inequality in access to
our services.
The Trust will monitor the implementation of these
priorities through its quality committees using key
indicators and audits. Quarterly reports will be
presented to Public Board on the delivery of the
annual plan. For example;
20Safe 21
We will implement the national patient safety factors and just culture principles are embedded
strategy, in particular by involving patient in all safety strategies across the Trust. The Trust
safety partners in our governance processes. has appointed two patient safety specialists and
is currently scoping the role of patient safety
partners.
Overview
The number of incidents reported by staff
In the coming year we will focus on reducing
continues to rise year on year which reflects
health inequalities across our local care system
the Trust objective of increasing the number of
by exploring the extent to which the risk of clinical
incidents reported. This objective ensures we are
harm is experienced across different patient
well placed to strengthen systems and processes
groups and how we might best address any
to improve safety. Triangulating the learning from
inequalities.
incidents together with feedback from complaints
and our experiential surveys allows us to improve
As we look to the year ahead our Divisional
our services through understanding what goes
teams are working with the Information Team to
well for our service users and what goes wrong.
develop a ward-based tool to monitor the key
The Trust is particularly proud of the progress
indicators of quality across the Trust. This data will
made in managing patient falls - in 2018/19 the
underpin improvement patient care improvement
percentage of harm caused by patient falls was
strategies, from skin management and prevention
28%, this reduced to 20% in 2020/21.
of falls to surgical site infections. This will improve
outcomes for patients, and ensure a better overall
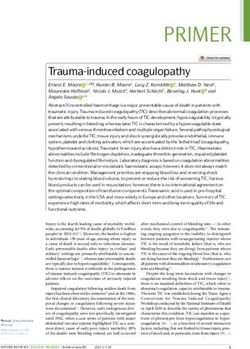
The Trust has not reported any grade 3 pressure
experience and satisfaction.
ulcers since May 2018. However, the reports
of pressure ulcers that develop in our care has
continued to rise. Our data has demonstrated a Incident Reporting
statistical relationship between Covid19 cases and The Trust is committed to providing the best
pressure damage rates. This remains a priority for possible care for patients and the continual
2021-22. improvement of our services. Despite the best
efforts of every healthcare professional, it is well
The Trust is looking forward to the release of known that people who are vulnerable through
the new patient safety curriculum and training illness can suffer harm while admitted to hospital.
programme that is being developed by Health When this happens, we encourage our staff to
Education England for all NHS staff. This will document each incident so that we can learn from
empower staff to take responsibility for patient them and decide whether we need to change the
safety in whatever role they undertake. Delivering way we do things to improve patient safety.
safe care is a complex mix of science and human In the financial year 2020-21 the Trust Incident
performance, so we will be encouraging our reporting system has recorded the following
colleagues to ensure that system thinking, human number of patient safety incidents:
Level of harm 2017-18 2018-19 2019-20 2020-21
None to moderate 7,536 7,337 8,008 8,308
Severe harm or death 35 21 25 88
Percentage of severe harm
0.46% 0.29% 0.31% 1.05%
or death
Total 7,571 7,358 8,033 8,396
22In line with guidance issued by NHS England and Trust’s reporting culture. Patient
NHS Improvement the Trust has documented safety data is continually reviewed and
each case of probable and definite healthcare triangulated with intelligence from a
associated Covid-19 infection as an incident. A number of valid sources including
number of these patients subsequently died which incidents, complaints, contact with our
accounts for the increase in incidents reported in Patient Advice and Liaison Service,
this category. dialogue with patient representative
organisations, input from our primary care
Surrey and Sussex Healthcare NHS Trust stakeholders and feedback from GPs,
considers that this data is as described for the alongside clinical performance
following reasons: benchmarking data.
This data is taken directly from the trust risk Surrey and Sussex Healthcare NHS Trust has
management system and is audited daily to taken the following action to improve this indicator:
check accuracy. Continue to educate staff on the positive
The Trust Management, Reporting and impact of reporting incidents and near
Investigation of Incidents Policy provides misses.
a clear framework for the reporting and Support clinical teams to identify and put in
reviewing of incidents in line with national place patient safety strategies to reduce
definitions. the type and incidence of harm.
The Trust actively promotes an open and Undertake thematic analysis of incidents
fair culture that encourages the honest causing moderate and severe harm.
and timely reporting of adverse events and Promote the benefit of safety huddles.
near misses to ensure learning and
improvement actions are taken.
The most recent national NHS Staff
Never event
We declared one ‘Never Event’ during 2020-21.
Survey (2020) found that 91.1% of
Never Events are a particular type of incident
respondents agreed that the organisation
that has been assessed by NHS Improvement as
encourages incident reporting. 94.8%
meeting all the following criteria:
stated that if they were concerned about
They are wholly preventable, where
unsafe clinical practice they would know
guidance or safety recommendations
how to report it.
that provide strong systemic controls have
Incident data is regularly uploaded to the
been implemented.
National Reporting Learning System
Each Never Event type has the potential
(NRLS). The NRLS collate six monthly
to cause serious patient harm or death.
performance reports, which are
However, serious harm or death is
published six months after the end of the
not required to have happened for
reporting period. These reports enable
that incident to be categorised as a Never
the Trust to benchmark incident data
Event.
against other Trusts in respect of three key
measures:
The patient, a 76 year old male, was admitted to
The Median Average Days between
ICU with suspected Covid-19 and his condition
occurrence of the Patient Safety Incident
continued to deteriorate. During the replacement
and date the Trust reports the
of a naso-gastric feeding tube, the tube was
Patient Safety Incident to the NRLS
inadvertently placed in the lung rather than in the
The Number of Incidents reported by a
stomach, but this was not identified by a chest
Trust to the NRLS
x-ray before feeding commenced.
The Ratio of the Number of Incidents
reported per 1,000 Bed Days delivered by
The investigation found that the protocol for
the Trust
the re-insertion of the NG tube and subsequent
The NRLS has assessed the data and
placement check by x-ray was followed correctly.
concluded that, the Trust is in the lower
The clinician had not been made aware that the
quartile, and there is no significant change
patient’s tube had recently dislodged and that a
in our reporting profile and this correlates
placement x-ray had just been taken. When he
with what our staff tell us about the
23checked the x-ray at 03:35 he viewed the x-ray
taken at 21:34 the previous evening. The most group. The patient, or their family/ carers, will
recent x-ray became available just 3 minutes later always be offered a copy of the report and the
at 03:38. opportunity to discuss the investigation at a face
to face meeting. These meetings give the Trust
The unit implemented a number of procedural the opportunity to ensure that the impact of these
changes immediately: incidents on patients and their families has been
No new NG feed regimes to be started considered and forms part of the learning from
between the hours of 8pm to 8am. these incidents.
The night team of doctors will review any
CXRs of naso-gastric tubes inserted Compliance with the statutory responsibility
between these hours and document for Duty of Candour is monitored at Divisional
on Cerner. Performance Meetings, is included on the Trust
The day team of doctors will undertake Scorecard and a summary position is reported
a double check of the placement to the Trust Board as part of the regular Serious
and confirm placement on CXR. Incident Report.
Following confirmation, NG feed will be
prescribed and commenced. Falls
The prevention and management of inpatient falls
Duty of candour continues to be a key patient safety theme and a
The Trust supports all our healthcare Trust priority for 2021-22.The Trust monitors the
professionals to be open and honest whenever falls rate and falls with harm per 1,000 occupied
mistakes are made and encourages staff ensure bed days. The national average for falls is 6.63
that patients always receive a full and sincere falls per 1,000 bed days; the Trust has remained
apology. Each clinical incident is investigated and consistently below this national average since
the findings are reviewed by a multi-professional August 2016.
Graph 1.0
1. National Audit of Inpatient Falls, Royal College of Physicians, 2015
24Graph 1.1
Graph 1.0 shows that the total number of falls has Looking at the months where there was higher
been on a downward trajectory. The average 12 Covid-19 inpatients, April 20 and January 21,
months for falls did increase in 2019/20 however whilst the number of falls in the high covid months
in 20/21 this has reduced. was lower compared to the same period in the
previous year (April 19 and January 20) the
The falls rate per 1000 bed days has remained difference was not statistically significant.
relatively static over time. In 2019-20 the Trust participated in the National
Falls CQUIN which consisted of three high impact
During the pandemic we saw an increase in actions. The Trust adopted a process of real time
the number of patients presenting with delirium auditing of patient notes and practice in relation
and for some patients this was protracted. The to falls prevention and management to ensure
admissions for all patients over 65 years with that challenges could be rectified immediately
a diagnosis of delirium trebled in June 2020 to improve the care for patients. The Deputy
compared to June 2019 and this is reflected in the Chief Nurse was nominated and shortlisted for
peak in falls rate in June 2020. The Florence Nightingale Nurse of the Year
Award for Audit in relation to this work. This
The Trust has historically observed an increase process is planned to continue looking at other
in falls during the summer months in particular specific actions as it demonstrably improved
June is a month where we observe this more the understanding of staff on the wards; the
specifically. In June 2020 falls increased from the audit results improved weekly and thus the
previous month and had the highest falls rate per management of patient risk.
1000 bed days for the whole financial year.
Graph 1.1 shows the number of falls alongside
Healthcare-associated infection
the percentage of falls which caused any level
of harm to patients. Over time the proportion of Clostridium difficile
harm caused as a result of falls has been on a 2020-2021 the Trust reported 56 cases of
downward trajectory. Clostridioides difficile Infection (CDI).
All diarrhoeal samples from hospital patients aged
While the falls numbers were lower in May 20 >2 years are reported. Cases are reported under
they did have a high proportion with some form of the Trust if considered Hospital-onset healthcare-
harm. associated (date of onset is ≥ 2 days after
admission) and Community-onset healthcare-
25Trust apportioned C. diff cases (aged two or over) 2018-19 2019-20 2020-21
Number of cases 27 47 56
Cases per 100,000 bed days 11.61 20.05 28.30
National average cases 33 37 89.30
Highest number of cases 177 165 328
Lowest number of cases 0 0 0
associated (date of onset is < 2 days after considers that this data is as described for the
admission and the patient was admitted to the following reasons:
trust in the 4 weeks prior to the current episode).
The increase in cases over the last two financial Each Clostridium difficile case has a root-cause
years may be reflection of a change in national analysis (RCA) carried out by members of
definitions for healthcare associated cases. the clinical team in conjunction with infection
There was no national Trust objective set by the prevention and control team.
Department of Health for 20/21 as in previous
years. The Trust continued however to ensure Surrey and Sussex Healthcare NHS Trust has
cases were assessed to determine any ‘lapses in taken the following actions to improve this rate,
care’ that may have been considered contributory and so the quality of its services:
to the cause of C. difficile or may have been
assessed as a lapse in the management of CDI Root Cause Analysis (RCA)
itself. Each CDI case has an RCA carried out by
members of the clinical team in
A ‘lapse in care’ is defined as evidence that conjunction with infection
policies and procedures were not followed, prevention and control team. The main
regardless of whether the lapse was contributory themes from these investigations
to the root cause of the infection. In 2020-21 there (from RCAs undertaken thus far)
is no evidence (on analysis thus far) of cross- include antibiotic prescribing lessons, a
infection where ribotyping is of the same type and delay to sending a stool samples, and a
cases linked epidemiologically. 3 cases were sample not saved for ribotyping.
assessed as lapse in care (compared to 8 for The lessons learned are disseminated
the previous year) of the 13 case investigations within the divisions and across the Trust to
undertaken. Completing root cause analysis of support organisation-wide learning. The
the remaining cases was challenged due to the lessons and summary from the remaining
concurrent COVID pandemic. Investigations and CDI case review that is underway will also
summary of the remaining cases is in progress. be shared.
Surrey and Sussex Healthcare NHS Trust
26A multidisciplinary review of all MRSA BSIs is
Methicillin-resistant undertaken to determine what factors could have
Staphylococcus aureus (MRSA) led to the infection and also how we can reduce
the risk of it happening again. Some themes
blood stream Infection in learning are evident with MRSA screening
The Department of Health objective is a zero
compliance (monthly screening compliance and
tolerance approach to avoidable MRSA blood
inclusion of all sites) and management of MRSA.
stream infections (BSI). For 2020-21, the Trust
Three of the cases were known to be positive
reported seven MRSA BSIs. One of the seven
for MRSA on admission so at increased risk
cases was considered potentially avoidable. A
already of MRSA BSI. There is a greater risk also
summary of the cases is below.
associated with the presence of invasive devices
(intravenous lines) or open sites (wounds). There
All cases have had a Root Cause Analysis
were lessons learned regarding documentation of
investigation for review of any contributory factors
cannula removal in 2 cases but in both cases the
or lessons. Five cases were within the Medical
cannula was either not assessed as the source
Division and two cases within the Surgical
of infection or not related to the cannula that was
Division.
the suspected source. Completion of twice day
phelibitis scoring was inconsistent in 2 cases
The first case was considered potentially
but again the cannula was not assessed as the
unavoidable. The patient was a long term carrier
source in these cases. There were no lessons
of MRSA and the admission screen was positive.
pertaining to other devices (either causing or
Skin tears were probable entry sites. There was a
lesson associated with) in the 6 patients that
potential earlier opportunity to swab skin tears on
developed a BSI. There has been no evidence
the arms, which were present on admission.
of cross infection/colonisation from other known
The second case was an orthopaedic patient
MRSA positive patients.
admitted post fall and sustaining a patella fracture.
The patient developed a MRSA BSI 11 days in to
MRSA screening and management is included in
admission and following knee surgery. There were
all the mandatory infection prevention and control
lessons learned regarding this case although at
training programmes and this focus will continue
the time the case was deemed as unavoidable.
to ensure all patients are screened as per
Lessons were incorporated in to an action plan.
policy. The Trust also monitors MRSA screening
Case three and four were considered blood
compliance.
culture contaminants (i.e. not true blood stream
infections).
Sustained focus on MRSA screening and
interventions to reduce the risk of infection or
Case five was a long term in patient. The BSI was
spread of MRSA will continue to be a priority area
regarded as significant although a source/focus
for reducing risk of healthcare associated infection
was not confirmed. There was a lapse in care
(HCAI). We will continue to analyse all cases of
identified but this was not considered to be linked
HCAI and disseminate learning.
to development of the BSI.
The sixth case was assessed as a lapse in care, Gram negative blood stream
linked to development of the BSI and potentially
avoidable. This was a prolonged hospital
infection (GNBSI):
The Department of Health objective was to
admission. The cannula was one suspected
reduce Gram-negative blood stream infection
source (and was removed promptly when signs
(E.coli, Klebsiella and pseudomonas) by 50%
of concern) with consideration also to hospital
by 2021, across the healthcare economy. Data
acquired pneumonia. The patient had a persisting
is being consolidated at the time of writing but in
positive blood culture and was subsequently
2020-21 (to the end of January 21) there were
confirmed to have infective endocarditis as
80 GNBSI. The Trust did experience an increase
a persisting source. This same patient had
in GNBSI during the COVID-19 pandemic
a subsequent positive culture considered a
and surge in activity. E.coli BSIs tend to be
continuous infection but is still reportable as
predominantly community onset, with Klebsiella
another case (case 7).
and Pseudomonas BSIs more frequently hospital
27You can also read