Québec Trauma System: An Integrated Model Promoting Quality Improvement - RedETSA November 2016
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Québec Trauma System: An
Integrated Model Promoting
Quality Improvement
RedETSA
November 2016
Catherine Truchon, Ph.D., MSc. Adm.
Coordinator and Principal Scientist
Trauma Unit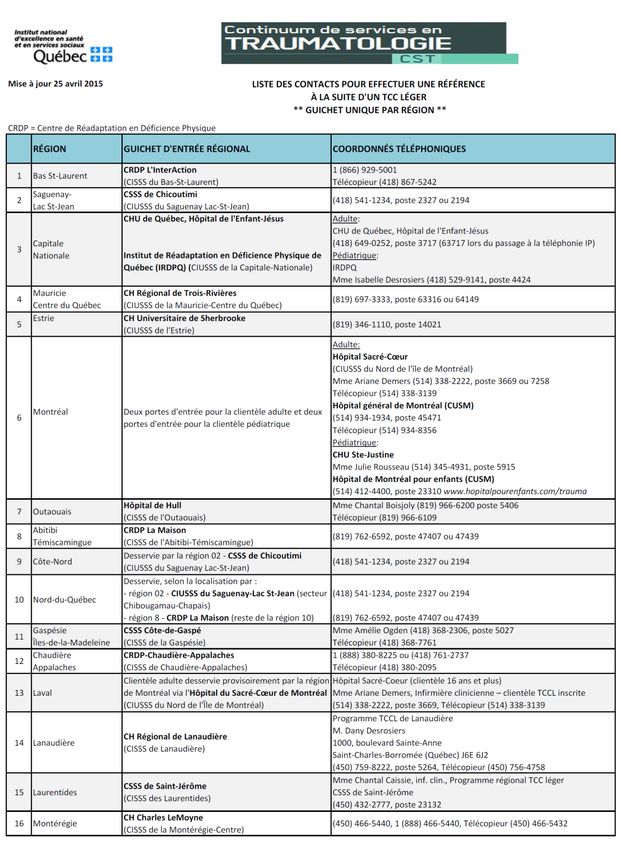
Outline
Trauma Unit Mandate
Trauma Care Continuum (TCC)
1. Designation of facilities
2. Consortiums / Centers of expertise
3. Services for mild TBI / MTI (musculoskeletal traumatic injuries)
Keys to success:
1. Innovative financial support
2. Governance and collaboration structures
3. Formal coordination mechanisms
MONITORING
4. Continuous quality improvement process
Conclusion
2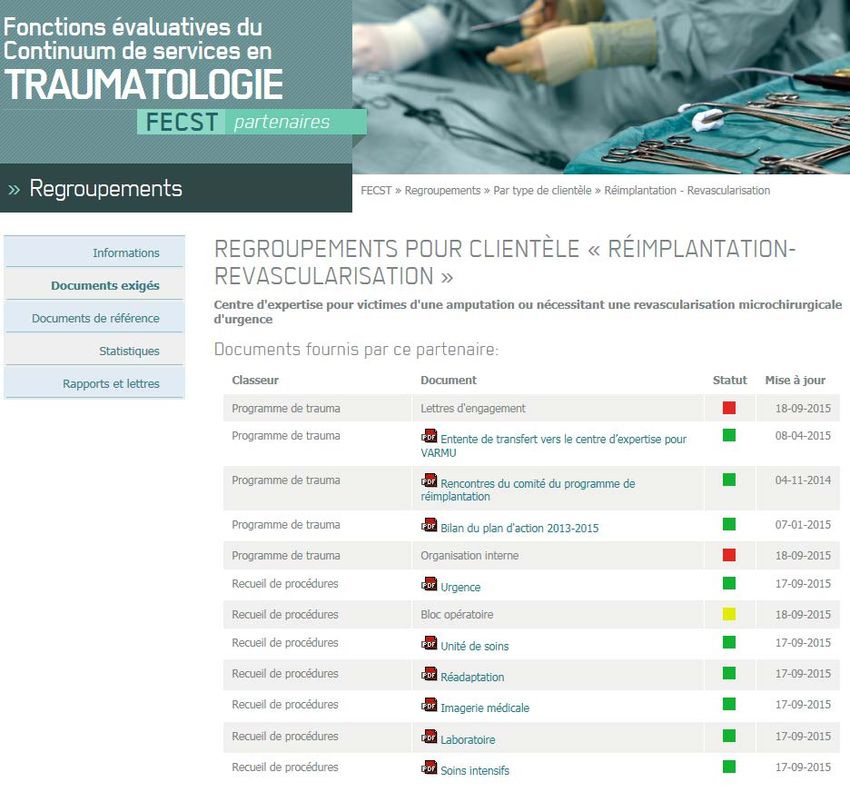
Trauma unit mandate
• Assessment and follow-up of the Trauma
Care Continuum by monitoring
conformity, quality and performance
TRAUMA CARE indicators
UNIT - • Development of protocols, guidelines and
INESSS tools to support clinical practice
• Support and guidance of ministerial
decisions and orientations from a
scientific and clinical standpoint
3
Background history
Prior to 1990, the mortality rate from severe trauma was over 52% in
Québec.
2 significant events:
•November 1989: Death of the athlete Victor Davis
•December 1989: Shooting at École Polytechnique
The MSSS and the SAAQ formed a partnership in 1992, and the Trauma
Advisory Council was established, leading to the creation of a model for
organizing trauma services in Québec, namely,
The Trauma Care Continuum (TCC)
4
Background history
Main objectives for the Trauma Care Continuum:
• Accessibility
• Continuity
• Efficacy
• Quality of services
Guiding principles:
• Time dependence ("golden hour")
• Reverse burden of proof
• Regionalization of services
5
Trauma Care Continuum
PRE-COLLISION 1. Accident prevention
COLLISION 2. Injury prevention
3. First responders (emergency – 911 calls)
4. Centres de communication santé Pre-hospital
5. First responders – police – extrication
POST-COLLISION 6. Ambulance services
7. Medical stabilization services
IMPACT 8. Primary trauma care centres In-hospital
9. Secondary trauma care centres
10. Tertiary trauma care centres / neurotrauma
11. Expert care centres
Rehabilitation
12. Inpatient rehabilitation and social
13. Outpatient rehabilitation integration
14. Community Participation Services
6
Historical perspective (cont’d)
1987: First agreement between the SAAQ and rehabilitation centres with regard to care and
services for MS TBI victims
1992-1995: First cycle of hospital designation process by the Trauma Advisory Council
(acute care)
1997: Designation of two centers of expertise (East and West) for care and services CEBM
for spinal cord injuries victims; and contract with the SAAQ
1999: Designation of rehabilitation centres by the Trauma Advisory Council to Regionalization
provide care and services for MS TBI victims of rehabilitation
services
2002-2006: Designation of Consortiums for MS TBI (continuum of care
and services: acute care and rehabilitation) Consortiums
2004-2005: Designation of two centers of expertise for severe CEVBG
burns victims (East and West)
2010: Designation of a center of expertise for replantations CEVARMU
(MUHC)
7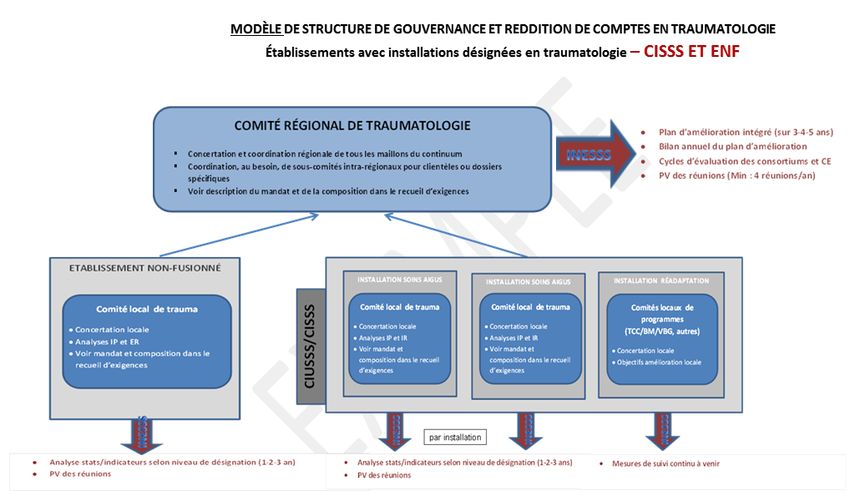
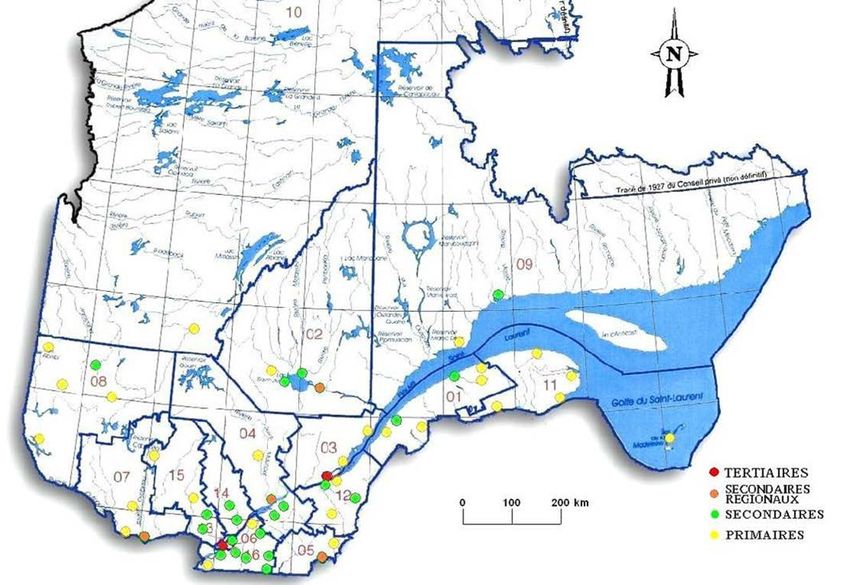
Designation of Institutions 8
Consortiums / Centers of
expertise
Consortiums moderate to severe TBI:
• Inter-regional consortiums (5 for adults and 5 for
children/adolescents)
• Regional consortiums (7 for adults
and 2 for children/adolescents)
Centers of expertise for spinal
cord injuries victims: Est
• 1 for western Québec Ouest
• 1 for eastern Québec
Québec
Montréal
9
Integrated trauma system
Tertiary trauma care centres
and designated hospitals
Acute-care hospitals offering
early rehabilitation services
Inpatient rehabilitation
Intensive functional rehabilitation,
Outpatient rehabilitation supraregional mandate
Regional base, social integration Specialized and highly specialized
and participation rehabilitation services
10Centers of expertise
2 CE for Spinal Cord Injury
CEVBGEQ (9 regions)
2 CE for Severe burns
• Hôpital de l’Enfant-Jésus du
CHUQ
• IRDPQ
CEVBGOQ (9 regions)
• Hôtel-Dieu de Montréal
(CHUM)
• Villa Médica Rehabilitation
Hospital
11Centers of expertise (cont’d)
A provincial Center of expertise for victims of traumatic amputation or
patients requiring emergency microsurgical revascularization (CEVARMU)
Designated hospital
Hôpital Notre-Dame
de Montréal (CHUM)
Regionalization of
rehabilitation services
12Services for mild TBI / MTI
Services for mild TBI
•2005-2010 Orientations of the Ministère de la Santé et des Services
sociaux (MSSS) (to be revised in 2016 – INESSS has been mandated to
perform a literature review)
•All the regions of Québec must develop and implement organized
services for mild TBI, in accordance with MSSS recommendations
Services for musculoskeletal traumatic injuries (MTI)
•Multiple diagnoses
•Rehabilitation receives referrals from several hospitals
13Single access
point in each
region
14Keys to success 15
Keys to success
1. Innovative financial support
2. Governance and collaboration
structures
3. Formal co-ordination mechanisms MONITORING
4. Continuous quality improvement
process
16Innovative financial support
Société de l’assurance automobile du Québec (SAAQ)
• Financing model
• Major commitment during the development and
implementation of the TCC
• Standing agreements throughout the phases of the
service continuum (including consumers associations)
• no refusal rights;
• Zero delay for transfers;
• Zero delay for return to the region
17Governance and collaboration
structures
• Ministère de la Santé et des Services sociaux (Department
of trauma and critical care, and Department for persons
with disabilities)
• Trauma programs in acute-care hospitals and
rehabilitation centres
• Regional and inter-regional trauma coordination tables
• INESSS Trauma Unit
18MSSS 19
Monitoring conformity and measuring
quality and performance
20Monitoring conformity and measuring
quality and performance
Quality and performance indicators
Donabedian Model
21Monitoring conformity and measuring
quality and performance
Quality and perfomance indicators MORTALITY
UNPLANNED
READMISSIONS
STRUCTURE PROCESSES
COMPLICATIONS
LENGTH OF STAY
Processes Mortality Readmissions LOS Complications
Structure 0.29 -0.19 0.11 0.19 -0.29
Processes -0.22 -0.30 -0.19 -0.48
Mortality 0.69 0.34 0.74
Readmissions 0.59 0.67
LOS 0.87
Moore L , Lavoie A , Bourgeois G , Lapointe J.
Donabedian's structure-process-outcome quality of care model : Validation in an integrated trauma system.
J Trauma Acute Care Surg. 2015 Jun;78(6):1168-75.
22Monitoring conformity and measuring
quality and performance
Conformity of structure elements
• Governance structure and continuous quality improvement
committee
o 4 meetings a year INESSS
o Continuous quality improvement plan and objectives INESSS
• Formal commitment
o Agreement protocols INESSS
o Letters of commitment from all the sectors (hospitals and rehabilitation
centres) INESSS
• Dedicated team
• Access to complementary expert opinions
• Facilities and equipment
23Required protocols Yes / No Location
Procédure pour le préavis du SPU avec description du rôle de chacun des intervenants et du
mécanisme de collecte de données (y inclus une communication directe entre le médecin à
l’urgence et le personnel ambulancier)
Procédure de mise en tension à trois niveaux avec description du rôle de chacun des intervenants
Procédure de mise en tension avec description du rôle de chacun des
intervenants
Procédure d’intubation difficile avec algorithme
Procédure pour l’hémopéritoine avec algorithme
Procédure pour l’échographie à l’urgence respectant le marqueur M30
Procédure pour accès veineux avec algorithme médical et infirmier
Procédure pour la stabilisation d’une fracture complexe du bassin avant le transfert
Procédure de prise en charge d’une patiente traumatisée enceinte
Procédure de prise en charge d’un traumatisé pédiatrique respectant les corridors de transfert
établis
Procédure pour l’antibiothérapie prophylactique dans le cas d'une fracture ouverte
Procédure pour la prise en charge d’un patient présentant un traumatisme pénétrant à la région
cervicale
Procédure de clairance de la colonne cervicale
Procédure de prise en charge avant transfert d’un patient présentant un
traumatisme craniocérébral modéré ou grave (TCCMG)
Procédure de dépistage et de gestion du risque de complications médicales graves pour les
patients ayant subi un TCCL
Procédure pour le maintien de la normothermie du patient
Procédure pour la détection du syndrome compartimental
Procédure pour la décontamination d’un patient
(biologique, chimique, nucléaire, radiologique)
24 Procédure d’accompagnement pour le déplacement interne du patientConformity of required structure
and process elements
25Monitoring conformity and measuring
quality and performance
QUEBEC
TRAUMA
REGISTRY
26Monitoring conformity and measuring
quality and performance
Surgical delay for long bones fractures < 24 hrs (example)
27Monitoring conformity and measuring
quality and performance
Adjusted mortality rate (example)
28Monitoring conformity and measuring
quality and performance
Adjusted complication rate (example)
29Monitoring conformity and measuring
quality and performance
Institution of TSC Overall outcomes
1992 2002 Fall in the MORTALITY RATE of
severe trauma from 52% to
8.6%
Additional 24% decrease in 200 extra
the mortality rate from all lives saved
trauma (all levels of severity) per year
1999 2012
A 16% decrease in length of stay LOS
(with no impact on the Savings of
complication or readmission $6.3M / year
rates)
Actuarial study by the SAAQ Estimated savings of $3 billion since
(2006) 1992
30Conclusion
Continuation … implications and issues:
• Reconfiguration of the current healthcare network
• Accountability model is complex and demanding
• Other priorities and issues (aging, stroke, etc.)
• Shared responsibility
• Emphasis on continuous monitoring of indicators
• Network support provided through tools, protocols, clinical
practice guidelines
31inesss.qc.ca
inesss@inesss.qc.ca
2535, boulevard Laurier, 5e étage
Québec (Québec) G1V 4M3
GRASIAS ! 2021, avenue Union, bureau 10.083
Montréal (Québec) H3A 2S9You can also read

















































