Revie w - Leipzig Interventional Course
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

over run
caption
Rev iew
2020 Continued on page 1
LINC Review Publishing and Production MediFore Limited Course Chairman Dierk Scheinert Editor-in-Chief Peter Stevenson Editors Tatum Anderson Ryszarda Burmicz Becky McCall Caroline Chambers Design Peter Williams Industry Liaison Manager Lorraine Tighe Project Manager Fiona Campbell Head Office 51 Fox Hill London SE19 2XE United Kingdom Telephone: +44 (0) 20 8771 8046 editor@medifore.co.uk www.medifore.co.uk Copyright © 2020: LINC and Provascular GmbH (Paul – List – Str. 11, 04103 Leipzig). All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, transmitted in any form or by any other means, electronic, mechanical, photocopying, recording or otherwise without prior permission in writing of LINC or Provascular. The content of the LINC Review does not necessarily reflect the opinion of the LINC 2020 Course Directors or the LINC Organisational Committee.

Introduction Contents
LINC in numbers 5
The 16th Leipzig Interventional Course, held 28–31 January 2020, saw almost 5,000 participants Lutonix data: No link between paclitaxel & mortality 6
fill the Trade Fair Leipzig in order to witness a renowned international meeting committed to ARIVA trial updates on anticoagulation & venous stents 10
advancing the scientific and clinical evaluation and treatment of patients with complex vascular Good patient selection is key to PVE 12
disease through an interdisciplinary discussion of novel endovascular techniques. EKOS™ tackles deep vein thrombosis 14
Over four days, all in attendance were exposed to explorations of cutting-edge interventional ‘Incredible efficacy’ of DES in long BTK lesions 18
practice, formed over a multidisciplinary programme of lectures, debates, trial updates, device Treating traumatic aortic injuries 20
innovations and expert-driven narrative. Of course, LINC also included dedicated “First-time Lesion type informs decision in fem-pop atherectomy 22
data release” sessions, running throughout the programme, which offered the first glimpses of How to be safe in BTK atherectomy 24
data from the latest important studies and technologies. Total IN.PACT from pooled DCB data 26
Live cases also featured in abundance, with satellite transmissions from Italy, Ireland, USA, Limitations & risks with CO2 angio 28
France, Switzerland, as well as centres in Leipzig and across Germany. Ever engaging, and always Failing TEVAR, keep up the surgical work 30
exciting to watch, these cases placed a spotlight on the latest-and-greatest techniques, devices,
Endo AV access 32
tips and tricks, and demonstrated how to tackle challenging situations head on.
EVAR in nonagenarians? 34
LINC also welcomed collaborators from leading vascular courses around the world, including: Snapshots from LINC 2020 36
The Charing Cross (CX) Symposium, Vascular InterVentional Advances (VIVA); the International
The pave-and-crack technique at seven years 37
Congress of Interventional Surgery (CICE); the International Symposium on Endovascular
TIPS improves transplant survival 38
Therapeutics (SITE); Complex Cardiovascular Therapeutics (CCT); the China Endovascular
Course (CEC); the Japan Endovascular Treatment (JET) Conference; the VEITHsymposium; the First presentation of global, real-world Lutonix data 40
Pan Arab Interventional Radiology Society (PAIRS); the German Society for Angiology/Vascular Endovascular treatment for genetic aortic disorders 42
Medicine (DGA); as well as the online learning Vascupedia platform and the Aortic and Peripheral Pedal-plantar loop techniques 44
Surgery “How to do it” congress. Impressive Tack record for TOBA trials 47
The LINC Review brings you just some of the highlights from the hundreds and hundreds of First-time data from COMPARE trial 50
presentations, cases, discussions and debates that took place during the entire LINC 2020 Cutting-edge CLTI approaches 52
meeting. For even more, we encourage you to head to the LINC website and dedicated LINC App TOPOS takes on DVTs 56
to view a selection of key sessions, live cases and presentation slides. Diagnosis is key in PCS 58
Thank you to all delegates and industry sponsors for your continued support. We look forward AAAs: Endo or open? 60
to seeing you next year at LINC 2021, held January 25–30! Taking a DETOUR into long lesions 62
LOCOMOTIVE: long lesions & spot stenting 64
Venous stents given the bench test 66
Faculty at LINC 2020 68
Industry support 71
Society and association accreditation
LINC 2020 was accredited by:
The Sächsische Landesärztekammer with The Swiss Society for Angiology with The Dutch Association for Vascular Surgery
21 cmE points. 20 Credits. with 20 accreditation points in Category I.
www.slaek.de www.angioweb.ch www.vaat-chirurgie.nl
LINC 2020 was endorsed by
The Italian Society of Vascular and The National Education Course for The European Society for
Endovascular Surgery Vascular Intervention and Medicine Vascular Medicine
www.sicve.it https://vivaphysicians.org/ www.vascular-medicine.org
LINC 2020 has been rated compliant
LINC 2020 was under the patronage of: with the Medtech Europe Code of
Ethical Business Practice
The German Society for Angiology The German Society of Vascular Surgery www.ethicalmedtech.eu
www.dga-gefaessmedizin.de www.gefaesschirurgie.de
LINC 2020 – Organisation and production
Congress production Congress organisation AV support the LINC Review
Provascular GmbH, Congress Organisation and More GmbH mediAVentures MediFore
Paul-List-Strasse 11 Ruffinistrasse 16 St. Jozefstraat 18 51 Fox Hill
04103 Leipzig, Germany 80637 Munich 9820 Merelbeke London
www.provascular.de Germany Belgium SE19 2XE
E-mail: info@cong-o.de E-Mail: info@mediaventures.be United Kingdom
Phone: +49 89 23 75 74-65 Phone: +32 9 239 0110 Telephone: +44 (0) 20 8771 8046
Fax: +49 89 23 75 74-70 Fax: +32 9 231 8920 editor@medifore.co.uk
4 www.cong-o.com www.mediaventures.be www.medifore.co.uk
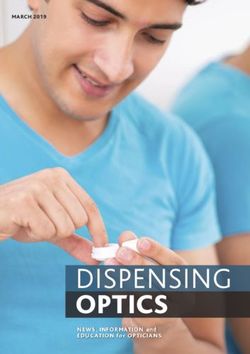
LINC in numbers
50 100 150 200 250 300 350 400 1,265
Germany
United States
Italy
Spain 5,027
United Kingdom +2.3% 4,956
Netherlands 4,913 4,913 +0.9%
4,837 +1.6% 4,866 +1.0%
Poland -3.2%
Switzerland 4,734 +2%
Belgium +17%
Japan
France
Russian Federation
Participants at LINC
Austria
Brazil 2012–2020
Egypt
Islamic Republic of Iran
Israel
Turkey
Ireland
India
Sweden
4,028
Continents from which
China +11%
Greece
Czech Republic Distribution of medical
Saudia Arabia
Denmark professionals by country delegates originated 3,607
Republic of Korea +26%
Norway
Thailand
Slovenia
Hungary
Finland
Australia Europe
Portugal 3,625
South Africa
United Arab Emirates
Argentina
Bulgaria
Ukraine
Croatia
Lebanon
Singapore
Costa Rica
Iraq
Distribution of medical
Lithuania
New Zealand
Romania
Australasia
Serbia
Colombia
Hong Kong
professionals by specialty 27
North America
Indonesia Asia 445
Jordan
618 Africa
Mexico South
Peru 109 America
Slovakia
Taiwan, Province of China 122
Canada
Latvia
Angiologists/
Luxembourg Cardiologists
Tunisia
Costa Rica Vascular 27%
Estonia
Kazakhstan Surgeons
Pakistan
Bangladesh 47%
Iceland
Republic of Moldova
Uruguay
Azerbaijan
Bahrain
Interventional
Belarus Radiologists
Bolivarian Republic of Venezuela
Bosnia and Herzegovina 26%
Burkina Faso
Curaçao
Georgia
Guinea
Kuwait
Kyrgyzstan
Malaysia
2012 2013 2014 2015 2016 2017 2018 2019 2020
Morocco
Nigeria
Saint Barthélemy
5
Swaziland
Syrian Arab Republic
United Republic of Tanzania LINC 2020 was a great success with a registration count of 4,946 from more than 80 countries
Independent analysis of Lutonix DCB
Data reveals no plausible
link between paclitaxel
and mortality
L
atest insights into the in-depth independent safety
safety and efficacy of analysis of the Lutonix (BD, USA)
drug-coated devices took drug-coated balloon (DCB) – a
centre stage on the first 2 µg/mm2 paclitaxel-eluting
day of LINC 2020, with balloon catheter which has been
a large proportion of the session extensively studied in the LEVANT
dedicated to paclitaxel safety. 11, LEVANT 22 and LEVANT Japan3
Speaking during the session series of trials.
was Kenneth Ouriel, Founder, “Lutonix was the first DCB
President and CEO of Syntactx approved by the Food and Drug
(New York, NY, USA), a full-service Administration in the US,” said
Clinical Research Organisation Dr Ouriel. “Approval was based
(CRO) that delivers high-quality on a rigorous preclinical and
clinical research services, clinical scientific programme
including heading-up clinical that demonstrated both safety
trials for medical device and and effectiveness.”
pharmaceutical companies. The independent Lutonix
“The need for a CRO is exactly analysis Dr Ouriel presented is in
what my talk is about because it part a response to the questions
is useful for medical device and raised about paclitaxel safety by
pharmaceutical companies to the Katsanos et al. meta-analysis two groups of patients, one with
have an independent assessor (2018) which found a late all- “There is no significant increase in an uncoated balloon and one
of data,” Dr Ouriel told the LINC cause mortality signal for patients
the hazard ratio for mortality in any with a paclitaxel-coated balloon,
Review ahead of his presentation. treated with paclitaxel balloons why there is a mortality signal?
“And the reason for that is more to and stents.4 As Dr Ouriel noted, analysis of the Lutonix DCB, nor any Some of the smartest people in
do with perceived, rather that real, Syntactx has since been doing the field have been asking the
conflicts of interest.” an independent analysis of the
plausible mechanism for mortality or same question. There definitely
In other words, CROs ensure Katsanos data as well – a task evidence of paclitaxel causation.” is a signal there, but not a single
that any perceived bias that which has proven challenging clinician that I know believes that
people may have of company- indeed: “It’s been a lot of work Kenneth Ouriel it’s related to the small amount
sponsored trial data is put to bed but it has been intellectually of paclitaxel which is found on
via robust and independently rewarding,” he said. the balloon.
verified analyses of datasets. “However, we haven’t been “Most of us, myself included,
6 In his talk, Dr Ouriel presented able to figure out, when you have Continued on page 7
believe that it’s probably related to some facet of trial design – more than likely due to missed follow-up visits (that are not at random). As we work towards more complete follow-up on virtually every patient, the mortality signal almost disappears once the vital statistics on patient survival become clear.” Indeed, several of the trials from leading manufacturers that fed into the meta-analysis had patients lost to follow-up, noted Dr Ouriel, which could have impacted the apparent mortality signal observed. Not least, he added, given that follow-up was different for the DCB cohorts versus non-DCBs. Crucially, patient-level data was not included in the Katsanos et al. meta-analysis, leading many to question if differences in follow-up care in DCB versus percutaneous transluminal angioplasty (PTA) comparators could be driving at least some of the mortality signal. Focusing back on Syntactx’s when pooling the data from the signal could be seen with the of death within a category, (does mortality increase following independent analysis of Lutonix Continued Access cohort,” noted Lutonix data, Dr Ouriel asserted causation is not supported.” index procedure?) and analogy data, Dr Ouriel relayed that Dr Ouriel. “This is an appropriate that, of the 173 deaths seen in Staying on the topic of (could the effects be due to patient-level data was used way to remove the bias associated the LEVANT 1 and 2 datasets, no causality, Dr Ouriel underlined immunogenic particulates?). to compare safety outcomes with differences in the make-up of deaths were classified as related the importance of using Bradford Save for the last two criteria from 1,093 Lutonix and 250 PTA patient groups that are not from to paclitaxel based upon the Hill criteria – a nine-point system (temporality is present, and patients across the LEVANT series the same RCT. We also performed known side-effects of the drug. that explores epidemiologic particulates have been implicated of trials, including the LEVANT time-dependent analyses to “Mechanistically, if paclitaxel evidence of a causal relationship in other situations), the rest 2 Continued Access cohort – account for factors that change caused death, there should be between a presumed cause and of the criteria can be ruled enrolled specifically to assess over time, and performed a disproportionate frequency an observed effect. Criteria span out, commented Dr Ouriel: paclitaxel safety. multivariable analyses to identify of mortality in one category or consistency, strength of effect, “The absence of seven of the “We utilised additional statistical key predictors of mortality.” a group of related categories,” specificity, plausibility, coherence, nine criteria is consistent with methods to assess the data, Cutting to the chase with explained Dr Ouriel. “That was not biological gradient (dose association, but not causation.” including propensity adjustment regards to whether any mortality observed. Thus, without clustering response), coherence, temporality Continued on page 8 7

Independent analysis of Lutonix DCB
“People have market isn’t anywhere near what it
was before,” he said.
felt reasonably “I think this has really impressed
comfortable going upon people that you do need
complete follow-up beyond the
back to using primary endpoint, especially given
the primary endpoint for many
paclitaxel devices, trials was a year or less. Even
although I’m though the primary endpoint is
earlier, people are pretty much
sure the market doing five-year trials now in the
isn’t anywhere lower extremities.”
He concluded: “There is
near what it was no significant increase in the
hazard ratio for mortality in any
before.” analysis of the Lutonix DCB, nor
any plausible mechanism for
Kenneth Ouriel mortality or evidence of paclitaxel
causation. Based on all of our
Continued from page 7 thus superseded paclitaxel as with paclitaxel devices, which study was lower than that of the analyses to date in a large dataset,
He went on to explore whether predictors of outcome. increases drug exposure,” PAD population as reported in the the Lutonix DCB continues to
there were patient or treatment- As such, the burning question continued Dr Ouriel. “Some of Swedish Vascular Registry (Sartipy offer meaningful benefit relative
related variables associated remains: “Is there a relationship the other analyses that have et al. 2018) at five years.” to risk in indicated patients.”
with increased risk, i.e. is there a between additional exposure to been reported did not account What this boils down to is that
plausible mechanism for mortality paclitaxel and risk of mortality?” for reinterventions. Almost 20% subjects in clinical trials may do References
associated with paclitaxel – or said Dr Ouriel. of subjects in the LEVANT 2 RCT better with additional clinical 1. Scheinert D, Duda S, Zeller T, et al.
management, said Dr Ouriel, while The LEVANT I (Lutonix paclitaxel-
with any other biological feature Looking at the LEVANT 2 RCT were treated with a paclitaxel
coated balloon for the prevention of
of DCB treatment – even through and Continued Access data, the device at some point during their reducing subsequent interventions femoropopliteal restenosis) trial for
some unknown mechanism? effect of initial paclitaxel dose on five-year follow-up. is beneficial for patients, it also femoropopliteal revascularization: first-
in-human randomized trial of low-dose
Using a propensity-adjusted survival was analysed in four dose “Subjects in both groups, DCB reduces additional “touch points”
drug-coated balloon versus uncoated
multivariate analysis of mortality groups: > 0 to ≤ 2 mg; > 2 mg to and PTA, who subsequently with health care providers. balloon angioplasty. JACC Cardiovasc
out to five years in the LEVANT ≤ 3.5 mg; > 3.5 mg ≤ 5 mg; and underwent an intervention with Commenting on the outlook Interv. 2014;7(1):10–19.
2. Rosenfield K, Jaff MR, White CJ, et al.
2 data, Dr Ouriel and colleagues > 5 mg. “No significant dose- a paclitaxel device had higher for paclitaxel, Dr Ouriel noted Trial of a Paclitaxel-Coated Balloon for
identified several variables as response relationship was five-year survival rates than those that as more data is added into Femoropopliteal Artery Disease. N Engl J
analyses, the proposed signal Med. 2015;373(2):145–153.
predictors of mortality, including identified,” commented Dr Ouriel, that did not. This finding was
3. ClinicalTrials.gov. LEVANT Japan Clinical
age, Rutherford category, left adding that when adjusting confirmed in our other studies, for mortality using paclitaxel Trial. Available at: https://clinicaltrials.
limb, diabetes, anticoagulants at for age – the most significant and would be counter-intuitive if becomes even weaker, thus he gov/ct2/show/NCT01816412
4. Katsanos K, Spiliopoulos S, Kitrou P, et al.
discharge and prior treatment. predictor of mortality in both DCB additional paclitaxel exposure is is optimistic that the reputation
Risk of Death Following Application of
However, these variables or PTA groups – no identifiable indeed harmful in the long-run. of paclitaxel will recover. “People Paclitaxel-Coated Balloons and Stents in
were shown to be predictors dose-relationship could be seen. “It should be noted that the have felt reasonably comfortable the Femoropopliteal Artery of the Leg:
A Systematic Review and Meta-Analysis
of mortality irrespective of We also looked at the effect mortality rate in both the PTA going back to using paclitaxel of Randomized Controlled Trials. J Am
8 treatment arm, i.e. DCB or PTA, of subsequent interventions and DCB groups in the LEVANT 2 devices, although I’m sure the Heart Assoc. 2018;7(24):e011245.

ARIVA trial updates on anticoagulation after venous stenting
A
n eagerly awaited
update from the “ARIVA is very important because to date
Aspirin® Plus we do not have any prospective randomised
Rivaroxaban Versus
Rivaroxaban Alone for controlled studies on antithrombotic or
the Prevention of Venous Stent
Thrombosis in Patients With PTS
anticoagulant treatment in patients after
(ARIVA) trial was showcased at venous stenting.”
LINC, giving all in attendance
an insight as to what to expect Oliver Schlager
from the multicentre study being
conducted in sites in Austria, ago1 in which medical experts best and could be recommended
Germany and Switzerland. were asked what anticoagulation in patients.”
Running through the details treatment or antithrombotic Back then, the authors of the
of the trial was Oliver Schlager, treatment they would recommend survey wrote that although a
a medical interventionalist from after venous stenting, and the number of studies have focused
the General Hospital and Medical results were analysed to achieve a on technical factors associated
University in Vienna, Austria. Delphi consensus. with stent occlusion, there is a
Dr Schlager, who specialises in But the survey revealed that paucity of research examining the
patients with a range of chronic amongst experts in the UK, role of antithrombotic therapy
conditions from chronic post- between 10 and 15 different in maintaining stent patency.
thrombotic venous occlusion to anticoagulation regimes were They also commented that there
non-thrombotic iliac vein lesions used after venous stenting, were no controlled studies that
(NIVL), is principal investigator (PI) noted Dr Schlager. Of the 106 previously investigated the use
for the Austrian portion of the trial. experts, a third chose life-long of anticoagulants or antiplatelet
The German PIs will be Christian anticoagulation with a vitamin-K agents following venous stenting.
Erbel, Houman Jalaie and Michael antagonist (VKA), 19% chose Today there are still several
Lichtenberg, and Nils Kucher life-long anticoagulation with a single-arm studies that assess
from University Hospital, Zurich, direct oral anticoagulant (DOAC), the use of different venous
Switzerland is the overall PI. anticoagulant in combination with randomised controlled studies on 7% used antiplatelet therapy (APT) stents, and patients within these
ARIVA is an investigator- aspirin,” explained Dr Schlager. antithrombotic or anticoagulant following stent placement alone studies receive anticoagulation
initiated academic trial whose The primary outcome of the treatment in patients after venous and 13% used APT in combination after venous stent placement,
primary aim is to assess different trial is patency at six months, i.e. stenting,” he said. “Therefore, it’s with an anticoagulant. “What was but most are driven by venous
anticoagulation regimes after without the occurrence of either very important to start this study interesting in this publication was stent companies. “None of these
venous stenting in patients with occlusion of at least a part of the as soon as possible.” the variety of different treatment studies specifically address the
chronic post-thrombotic venous stent segment or a re-intervention What’s apparent is that while a regimes after venous stenting,” anticoagulation regime after
lesions. “People who undergo to maintain patency of the range of anticoagulants are used said Dr Schlager. venous stenting,” said Dr Schlager.
endovascular revascularisation treated segment. after venous stenting, there is no “This underlines the need for “Existing single-arm studies focus
and venous stenting will be What’s important about ARIVA, clear evidence on which works a large multicentre prospective on the stents but not on the
randomised to receive either noted Dr Schlager, is that it is better. Indeed, Dr Schlager cited randomised controlled study accompanying medical treatment,
anticoagulation-only therapy the first trial of its kind. “To date an interesting electronic survey which will give us information which is absolutely necessary.”
10 [rivaroxaban] or to receive the we do not have any prospective conducted in the UK several years on which treatment regime is There are three major factorsimpacting on the patency of treatment is a key issue for
“Anticoagulation was no significant difference in on offer. “I think that we need
venous stents, said Dr Schlager. stent patency after venous patency between patients who more prospective randomised
One is the type of lesion – stenting. The interventionalist treatment is a received anticoagulation for a controlled studies after venous
either chronic post-thrombotic, should either be familiar with limited period in comparison stenting, and the ARIVA trial will
acute thrombotic, or non- different anticoagulation
key issue for stent with patients who received help us to get this information,” he
thrombotic, while the second regimes by themselves or should patency after anticoagulation for an said in closing.
lies in haemodynamics. “This is cooperate with angiologists extended period.”
more about the inflow coming and haematologists who venous stenting.” Of course, the study was a References
from the veins below the inguinal are able to take care of the retrospective analysis rather than 1. Milinis K, Thapar A, Shalhoub J, et al.
ligament, which has to be granted anticoagulation regime.“ Oliver Schlager a prospective randomised control Antithrombotic Therapy Following
Venous Stenting: International Delphi
through stent patency after stent During his presentation, Dr study, noted Dr Schlager. “It was Consensus. Eur J Vasc Endovasc
placement,” he said. “But the third Schlager stepped outside of the placement.2 “This is an interesting a nice study, but it shows how Surg. 2018;55:537–544.
2. Sebastian T, Engelberger R, Spirk D, et
most important factor, of course, ARIVA trial to address other new study into patients who received important the ARIVA trial is.”
al. Cessation of anticoagulation therapy
is the anticoagulation treatment, research into anticoagulation. For anticoagulation treatment for a In his concluding remarks, Dr following endovascular thrombus
for which there is no study so far.” example, a study conducted by Tim limited period, and patients who Schlager reiterated that going removal and stent placement for acute
iliofemoral deep vein thrombosis.
That’s why there is a need Sebastian at the University Hospital received anticoagulation for forward there is a clear need Vasa. 2019;48(4):331–339.
for collaboration amongst Zurich, which was published last an extended period after stent for many more randomised
different specialties, Dr Schlager year, looked at the duration of placement,” said Dr Schlager. controlled trials looking at the The ARIVA trial is planned for
went on: “Anticoagulation anticoagulation following stent “What he showed is that there different anticoagulation therapies completion in August 2022.
11Preoperative portal vein embolisation in liver cancer
The three cornerstones of
good patient selection
A
rnaud Hocquelet required. It is not the same if you
(CHUV, Lausanne, are going to treat a large anterior
Switzerland) discussed hepatocholangiocarcinoma of
indications and 7 cm, or several small metastases
patient selection of around 1 cm in the liver. Also,
in preoperative portal vein you have to discuss the complexity
embolisation (PVE). of the surgery. Indeed, a prolonged
Dr Hocquelet told audiences liver ischaemia period from
that surgical resection of vessel clamping is a risk factor of
hepatic tumours is often the postoperative liver failure.”
only curative treatment for large The second cornerstone,
primary tumours or for patients continued Dr Hocquelet, is
with several small secondary the FRL volume percentage of
tumours. However, for many total liver volume. He cited the
patients, their tumours are work of Yiglitler et al. (2003),
considered unresectable because who identified a more difficult
of insufficiency of future remnant postoperative course in those
patients left with a smaller FRL2:
“Now we have a cheap, fast and accurate on CT you can find signs of portal
liver (FRL). hypertension without cirrhosis.
PVE serves as a potential “There is a strong correlation method of assessing liver function – This is an SOS: it should alert you
remedy to this issue. It leads to between the amount of the liver about liver function. Now we
a redistribution of flow and has after surgery and the overall
hepatobiliary scintigraphy.” have a cheap, fast and accurate
been shown to induce local morbidity. Under 30%, your rate method of assessing liver function
hypertrophy of the liver1. “The of morbidity is around 50%. This Arnaud Hocquelet – hepatobiliary scintigraphy. In
indication of PVE is to increase correlation is well-known in our centre, we use the cutoff of
the FRL volume before resection,” several studies.” healthy liver, and 40% for others. contraindication for PVE. Indeed, 2.69 mm/min/kg for the FRL, to
explained Dr Hocquelet, “In Dr Hocquelet also noted more “To accurately assess your FRL, there is a very strong correlation allow surgery.
order to increase surgical margin recent research demonstrating you need a good quality contrast- between a small initial size “‘Volume is not function’ is
and to improve postoperative how combining the albumin- enhanced CT scan with hepatic of the FRL and a high degree true before any intervention.
liver function.” bilirubin score (the ALBI vein visible, in order to perform of hypertrophy4.” In one study, they found very
He outlined the three score) with FLR predicts post- segmentation using automatic, The last cornerstone is the FRL weak correlation between liver
cornerstones of PVE that underpin hepatectomy liver failure3. semi-automatic or hand-free function. “Volume is not function, volume and liver function5. This
good patient selection. The Before major liver resection, the methods – depending on what it is very important to understand is also true after PVE. After PVE,
first is the type of intervention. FRL volume can be calculated software you have available in that,” stressed Dr Hocquelet. you will observe an increase
“You have to talk with your according to the equation: FRL% your centre. “Obviously, for a cirrhotic patient, in volume, but you will have a
surgeons about the amount of = FRL / (whole functional liver “One interesting thing is that everybody thinks about liver bigger increase in function. But
liver to be resected during the volume, excluding tumour), where a very small left lobe (< 10%) function. But for a young patient after ALPPS [Associating Liver
12 intervention, and the margin the usual cutoff is > 30% for the should not be considered a receiving intra-arterial oxaliplatin, Partition and Portal vein Ligationfor Staged hepatectomy] – the
surgical alternative to PVE – at
two weeks you will have a very
strong increase in volume but
no increase in liver function.
If you have the volume but
not the function, you will have
postoperative liver failure.”
He concluded: “PVE is here
to improve surgery quality by
improving margins, to improve
postoperative outcomes by
avoiding liver failure, and to
bring curative treatment to
unresectable patients.
“To do that, you need to talk
with your surgeons, have a good
CT to assess liver volume, and you
have to assess liver function using
hepatobiliary scintigraphy. Of
course, you have to avoid treating
patients with contraindications.”
References
1. Denys A, Bize P, Demartines N et al.
Quality Improvement for Portal Vein
Embolization. Cardiovasc Intervent
Radiol. 2010;33:452–6.
2. Yigitler C, Farges O, Kianmanesh R, et
al. The small remnant liver after major
liver resection: how common and how
relevant? Liver Transpl. 2003;9(9):S18–S25.
3. Zou H, Wen Y, Yuan K, et al. Combining
albumin-bilirubin score with future liver
remnant predicts post-hepatectomy
liver failure in HBV-associated HCC
patients. Liver Int. 2018;38(3):494–502.
4. Hocquelet A, Frulio N, Gallo G, et
al. Point-shear wave elastography
predicts liver hypertrophy after
portal vein embolization and
postoperative liver failure. Diagn Interv
Imaging. 2018;99(6):371–9.
5. Bennink RJ, Dinant S, Erdogan D,
et al. Preoperative assessment of
postoperative remnant liver function
using hepatobiliary scintigraphy. J Nucl
Med. 2004;45(6):965–71. 13Deep vein thrombosis and EKOS™
Interventional treatment to “If you’re treating
minimise post-thrombotic a patient with
syndrome and maximise outcome iliofemoral
M
aximal reduction and freedom from PTS of over
DVT, there
and treatment of 90% at three years, if proper really shouldn’t
post-thrombotic patient selection and procedural/
syndrome (PTS) post-procedural management be anyone with
by optimal are performed.
moderate or
interventional treatment of Referring to data from the
deep vein thrombosis (DVT), past three years from centres severe PTS if it’s
together with the safety and in Bern and Zurich, as collected
efficacy of EKOS™ Acoustic in the Swiss Venous Stent
a first-time DVT
Pulse Thrombolysis™ treatment Registry (SVSR), Professor and they have no
were the first two topics under Kucher shared his experience
discussion at a symposium of the interventional treatment chronic venous
led by BTG, now a part of of acute iliofemoral DVT with insufficiency.”
Boston Scientific. venous stenting. Together the
Nils Kucher (University centres have treated 160 patients,
Nils Kucher
Hospital Zurich, Switzerland) comprising more women than
chaired the event and gave a men, with an overall mean age
presentation addressing how of 48 years old. Most (78%) DVTs
to optimise reduction in PTS were on the left side, and mainly Scientific), and the mean patients had patent stents,” added Professor Kucher then
numbers when treating acute DVT due to May-Thurner syndrome. number of stents deployed was Professor Kucher. addressed the differences
interventionally. He was joined “I want to highlight that 16% had 1.7. “We are shifting towards Villalta scores showed that between the major trials in the
by colleagues Mert Dumantepe varicose veins as a risk factor, single session treatment in the 90% of patients had no PTS at area: the Swiss Registry, ATTRACT
(Acibadem University School and already had chronic venous majority of patients now,” said three years, and 9% had mild and CaVenT. “Why did these trials
of Medicine, Istanbul, Turkey) insufficiency. This is why the Professor Kucher. PTS. Professor Kucher went fail so badly?” he asked.
who discussed the treatment Villalta score is inappropriate Primary patency rate at three on: “Two patients had higher “All of our patients [in the
of femoral PTS with EKOS™, in clinical trials because many years was 79.4% (CI 95% [71.7, scores. These patients had severe Swiss Registry] had descending
and Stefan Stortecky (Swiss patients already have increased 87.1]) with the majority of stent chronic venous insufficiency at iliofemoral DVT, and by
Cardiovascular Centre Bern, Villalta scores,” remarked failures occurring early on. baseline; one had an active ulcer comparison CaVenT and ATTRACT
Switzerland) who reported his Professor Kucher. Assisted primary patency was at the time of DVT. You cannot had 48% and 57%, respectively.
centre’s data on the treatment of Of those treated, 44% 84.9% (CI 95% [78.1, 91.7]), and improve the Villalta score in such The remainder were ascending
high-risk and intermediate high- underwent catheter-directed secondary patency at three years a patient. If you’re treating a femoropopliteal DVTs but these
risk pulmonary embolism (PE). thrombolysis (CDT) – either was 95.6% (CI 95% [91.8, 99.4]). patient with iliofemoral DVT, there should not be touched – they
Professor Kucher emphasised EKOS™ or conventional, “We did not give up if someone really shouldn’t be anyone with need blood thinners.
that interventional treatment of 21% were treated in a single needed a secondary intervention moderate or severe PTS if it’s a “Also, 21% of our patients
acute iliofemoral DVT may lead session (Angiojet ZelanteDVT™ because a stent became first-time DVT and they have no had single session treatment
14 to primary patency of over 95%, thrombectomy catheter, Boston occluded. At three years almost all chronic venous insufficiency.” compared to 0% in CaVenT, andan unknown number if ATTRACT. “Our results is confirmed.” months in May-Thurner syndrome of complaints who had failed on
CDT first was used in 79% of our Regarding his procedural cases; while Duplex surveillance conservative therapy and had a
patients versus 100% and 59% in showed that recommendations, among the and Villalta scores need to be Villalta score greater than eight.
CaVenT and ATTRACT.” 75% of patients key criteria listed by Professor carried out at 2 weeks, 3, 6 and 12 The primary efficacy endpoint
He added that 100% of patients Kucher were: popliteal access months, and then annually. was reduction in Villalta score of
received a stent, compared to 17% reached the with ultrasound guidance, Following Professor Kucher, Dr over six points at day 30 versus
and 30% respectively in CaVenT deciding whether to use CDT first, Dumantepe took to the podium baseline, and increased blood
and ATTRACT, noting: “I wonder
primary or single session thrombectomy; and discussed how endovascular flow in the relevant segment.
how many patients in ATTRACT endpoint.” diagnosing compressed iliac veins intervention using EKOS™ with The primary safety endpoint
had spontaneous flow at the end using venographic criteria; and Acoustic Pulse Thrombolysis™ was major bleeding within 72
of the procedure – not many Mert Dumantepe using intravascular ultrasound treatment is safe and effective hours of starting the procedure
I think.” (IVUS) in cases where venography for patients suffering from and incidence of PE within 30
Professor Kucher summarised technique to identify the distal is equivocal. femoral PTS. days post ultrasound-assisted,
what he felt was key to success thrombus extent,” he said. “If the Post-procedure he He referred to his single- catheter-directed, low-dose
with respect to diagnosis for popliteal cannot be compressed recommended oral anticoagulation centre experience where they thrombolysis (UACDT).
descending DVT. “Colour Duplex then it might not be thrombosed, for at least three months, and included over 200 patients with A total of 202 femoropopliteal
[ultrasound] with calf compression and if it is not thrombosed then no platelet inhibitors; oral symptomatic femoropopliteal PTS patients were included with
is the only reliable imaging a descending iliofemoral DVT anticoagulants stopped at 3–6 DVTs with more than six months Continued on page 16 15Deep vein thrombosis and EKOS™
Continued from page 15 Last on the stand was angiographic obstruction
mean DVT age of 27.1 months, Professor Stortecky who over 48 hours, without any
and with mean dose/duration discussed treatment of high-risk intracranial haemorrhage.
of tissue-type plasminogen and intermediate-risk PE with Moreover, the OPTALYSE Trial
activator (tPA) of 23.3 mg and 22 Acoustic Pulse Thrombolysis™. was able to show that also very
hours, respectively. He familiarised the audience with low doses of tPA over a very
“Our results showed that 75% the EKOS™ system, explaining short treatment period was able
of patients reached the primary that it uses targeted ultrasonic to effectively decrease RV/LV
endpoint [p < 0.001],” reported Dr waves in combination with clot- ratio. Indeed, a tPA rate as low
Dumantepe. “We only saw two dissolving drugs. The system as 1mg/hour/catheter over a 4
major bleeding events, and nine uses a sophisticated catheter and hour treatment period was able
recurrent DVTs. Doppler showed an ultrasonic core to effectively to significantly decrease RV/LV
that patency was around 90% target an entire clot, along with ratio by 0.35 and was as effective
for each segment, and similar at fibrin separation and active as a higher dose regimen.
one year.” drug delivery into the clot by Based on the data, it is likely
He also highlighted the acoustic streaming. that EKOS™ is also effective in
importance of freedom from Professor Stortecky said the PE reducing RV/LV ratio with even
ulceration: “We saw a 91% response team treated three- lower dose tPA regimens and
ulceration healing rate. Washout quarters of patients with EKOS™ . shorter treatment times, Professor
[time to washout of the femoral “Some received medical therapy, Stortecky concluded.
vein] also significantly improved some surgical thrombectomy but Optimising the reduction in PTS
after EKOS™ treatment for second very few received systemic lysis,” numbers when treating acute DVT
day. Villalta score also showed he said. “In fact, the vast majority systolic pressure continuously interventionally, or treating PE
improvement of 10.2 points from of patients received EKOS™ in
“You can rest decreased up to 48 hours. with EKOS™, these results serve
baseline at 360 days, while venous the intermediate- and high-risk assure that No patients had intracranial to further reinforce the benefits
clinical severity score (VCSS) score patient groups.” haemorrhage and there were of using ultrasound-assisted
showed a reduction of 8.1 points He referred to the ULTIMA trial EKOS™ will not very low rates of major bleeding CDT and add to an increasing
from baseline at 360 days. Quality led by Nils Kucher, the primary
interfere with events, added Professor Stortecky. wealth of evidence to support its
of life scores also improved endpoint of which was reduction The protocol for EKOS™ in the growing use.
by 21.3 points on the VEINES in the right-to-left ventricle your procedure.” SEATTLE II study involved patients
scoring system.” diameter (RV/LV) ratio. Results having symptoms less than 14 days References
After presenting a couple of showed that the combination of Stefan Stortecky due to massive or sub-massive 1. Kucher N, Boekstegers P, Müller OJ,
case studies from his centre EKOS™ and heparin led to a ratio PE, and a RV/LV diameter of > et al. Randomized, controlled trial
of ultrasound-assisted catheter-
in Istanbul, he closed his of 0.3, versus 0.03 in those patients bleeding, but you can rest assure 0.9. The PE was confirmed by CT
directed thrombolysis for acute
presentation with a call to action. on heparin alone over 24 hours.1 that EKOS™ will not interfere with scan. UACDT was used with a total intermediate-risk pulmonary embolism.
“The ACCESS PTS treatment “There was also a significant your procedure.” tPA dose of 24 mg. Outcomes Circulation. 2014;129(4):479–486.
protocol reduces PTS scores, difference seen between the The SEATTLE II single-arm included a 25% decrease in CT- 2. Piazza G, Hohlfelder B, Jaff MR, et al.
A Prospective, Single-Arm, Multicenter
that is Villalta and VCSS, improves heparin plus EKOS™ versus study2 in 150 patients (31 massive measured RV/LV diameter ratio Trial of Ultrasound-Facilitated,
quality of life, and these benefits heparin alone at 90 days,” noted PE, 119 sub-massive) showed over 48 hours, a 30% decrease Catheter-Directed, Low-Dose
have persisted for 365 days so far,” Professor Stortecky. “There was the RV/LV ratio was significantly in pulmonary arterial systolic Fibrinolysis for Acute Massive and
Submassive Pulmonary Embolism: The
said Dr Dumantepe. “It’s time to a small and statistically non- decreased over 48 hours, as well pressure by procedure end and SEATTLE II Study. JACC Cardiovascular
16 stop saying nothing can be done.” significant increase in minor as the mean pulmonary artery a 30% decrease in pulmonary Interventions. 2015;8(10):1382–1392.‘Incredible efficacy’ of DES treatment in long BTK lesions
D
uring an update occlusions that are difficult to One of these is a self-expanding
on clinical trials treat with balloon angioplasty.1 polymer-based drug-eluting
and new data in “For those patients who are paclitaxel stent – [studied in]
peripheral vascular failing balloon angioplasty, the Saval trial4. Another is on
disease, including we have yet to realise the the MicroStent [Micro Medical
femoral, below-the-knee (BTK) ideal technology to overcome Solutions, USA] which is a bare
and critical limb ischaemia (CLI), these limitations,” Dr metal, interwoven stent for the
Robert Lookstein (Icahn School Lookstein commented. BTK circulation. Both of these
of Medicine at Mount Sinai, New Exploring BTK treatment trials are currently enrolling and
York City, USA) presented 10-year options to date, he further the preliminary results are not yet
findings of the LONG DES-BTK explained that investigations publicly available5.”
study of the use of drug-eluting of drug-coated balloons (DCB) In the meantime, the body of
stents (DES) in the treatment of have so far been unsuccessful data on the use of short coronary
BTK disease. in improving upon outcomes of balloon-expandable stents for
The study seeks to expand balloon angioplasty. “We have two the treatment of infrapopliteal
on the existing datasets of DES, negative prospective randomised disease has grown. These have
as part of continuing efforts to trials and a third trial where we been summarised in a systematic
determine when and in whom this don’t have 12-month follow review and meta-analysis by
technology is best suited. up yet.” Varcoe et al. (2019), which
“We hope that this LONG-DES The first of these two included data pertaining to seven
dataset will inform practitioners prospective randomised trials, randomised controlled trials with
that even in lesions where IN.PACT DEEP, included 358 mid-term (12-month) follow-up,
you require three overlapping CLI patients randomised to with the conclusion that DES
coronary stents, results are safe receive IN.PACT Amphirion significantly improved rates of
and effective in achieving limb DCB (Medtronic, Ireland) or primary patency, freedom from
salvage with very, very low rates plain balloon angioplasty. reintervention, and freedom from
of reintervention,” Dr Lookstein No statistically significant major amputation compared to
told the LINC Review ahead of differences were detected in control therapy (plain balloon
the session. the primary efficacy outcomes “The only implants to date that have angioplasty, BMS, or DCB).
In infrapopliteal disease, the
use of balloon angioplasty with
of clinically-driven target lesion
revascularisation and late lumen
demonstrated efficacy have been balloon- The investigators also found
that stents coated in sirolimus
bail-out bare metal stenting loss at one year.2 expandable coronary DES.” analogues were more effective
(BMS) in cases of residual stenosis The second prospective than paclitaxel.1
or flow-limiting dissection is randomised trial of BTK DCB was Robert Lookstein These randomised trials
associated with poor long- BIOLUX P-II, which included 72 included relatively short lesions
term patency and the need for patients randomised to receive with mean lesion lengths ranging
reintervention. Patients with BTK either the Passeo-18 Lux DCB balloon. Major amputations were to date that have demonstrated from 15.9 mm to 34 mm.1 The
disease frequently have comorbid (Biotronik, Germany) or plain also similar at 12 months.3 efficacy have been balloon- only included trial with lesions
diabetes, renal insufficiency, and balloon. Here, the primary As such, he continued, expandable coronary DES,” over 100 mm – the IDEAS trial6,
have a history of tobacco smoking endpoint of six-month patency numerous investigators globally he said. which randomised a real-world
– all of which are associated loss was not significantly inferior have looked to scaffolds as a “There are ongoing studies patient cohort with long BTK
18 with long, calcified stenoses and in the DCB group relative to plain viable solution. “The only implants evaluating novel technologies. lesions to DCB or coronaryDES – had multiple issues, as Dr use of stent implantation.
Lookstein described: “There were “For the past 10 years, we have
multiple DES allowed in the study. been using a single coronary
The only published data that has DES platform for infrapopliteal
ever been presented publicly lesions below the knee: the
was of the six-month follow up. Xience everolimus-eluting stent
Lastly, DES was compared to an [Abbott Vascular, USA]. We
arm of heterogeneous DCB. So have placed stents in the BTK
it was much more of a real world circulation for patients with CLI
registry dataset of all-comers, in over 375 individuals now, and
randomising two different we have been following all of our
technologies for long lesions.” patients with a routine clinical and
imaging protocol.”
“We have placed A key aim of the LONG DES-
BTK study at Mount Sinai was to
stents in the BTK ascertain how safety and efficacy
outcomes related to the number
circulation for of stents implanted in a single
patients with case. Like most coronary stents
being applied in the peripheries,
CLI in over 375 the Xience stent has a maximum
individuals now.” length of 38 mm, and as such
even a relatively short lesion
of 45 mm would require the
Robert Lookstein
implantation of two overlapping subset of long infrapopliteal
stents. In the cohort of 75 patients lesions that have failed balloon References Passeo-18 PTA balloon catheter in
subjects requiring revascularization of
in LONG DES-BTK, lesion lengths angioplasty, amputation-free 1. Varcoe RL, Paravastu SC, Thomas
infrapopliteal arteries) JACC Cardiovasc
No DCB or DES are currently ranged from around 50 mm to survival for the entire cohort SD, et al. The use of drug-eluting
Interv. 2015;8:1614–22.
stents in infrapopliteal arteries: an
approved for the BTK circulation 150 mm, requiring the tandem (including Rutherford 4, 5 and 4. The DES BTK Vascular Stent System
updated systematic review and
vs PTA in Subjects With Critical Limb
in the US, Dr Lookstein noted. implantation of two to four stents. 6) was 73% at one year. When meta-analysis of randomized trials. Int
Ischemia (SAVAL). ClinicalTrials.gov.
Turning to his own centre’s “These were all patients that you look at the cohort broken Angiol. 2019;38(2):121–35.
https://clinicaltrials.gov/ct2/show/
2. Zeller T, Baumgartner I, Scheinert D, et
approach, he explained: “Our were treated with this technology down by Rutherford category, al; IN. PACT DEEP Trial Investigators.
NCT03551496 (accessed Jan 2020).
for the Rutherford 4 and 5 5. A Clinical Evaluation of the MicroSTent®
clinical protocol at Mount Sinai not as a primary therapy, but after Drug-eluting balloon versus standard
PeripherAl Vascular SteNt in Subjects
is to cross infrapopliteal lesions, bail-out following suboptimal patients, amputation-free survival balloon angioplasty for infrapopliteal
arterial revascularization in critical limb With Arterial Disease Below the
perform prolonged long balloon angioplasty. So the patient had at one year was over 90%, and ischemia: 12-month results from the Knee (STAND). ClinicalTrials.gov.
angioplasty, and then perform a to undergo revascularisation, for the Rutherford 6 patients IN.PACT DEEP randomized trial. J Am https://clinicaltrials.gov/ct2/show/
Coll Cardiol. 2014;64:1568–76. NCT03477604 (accessed Jan 2020).
subsequent repeat angiographic fail balloon angioplasty (defined this fell down to almost 50%.
3. Zeller T, Beschorner U, Pilger E, et 6. Siablis D, Kitrou PM, Spiliopoulos S, et al.
assessment of the lesion that was as either significant elastic So we are seeing significant al. Paclitaxel-Coated Balloon in Paclitaxel-coated balloon angioplasty
treated. Unfortunately, we find recoil with a > 50% residual benefit for amputation-free Infrapopliteal Arteries: 12-Month Results versus drug-eluting stenting for the
From the BIOLUX P-II Randomized treatment of infrapopliteal long-
that in [up to] 30% of cases, there luminal narrowing, or a flow- survival favouring the use of this
Trial (BIOTRONIK’S-First in Man study segment arterial occlusive disease: the
is significant elastic recoil or flow- limiting dissection). technology in Rutherford 4 and of the Passeo-18 LUX drug releasing IDEAS randomized controlled trial. JACC
limiting dissection requiring the “In this very challenging 5 patients.” PTA Balloon Catheter vs. the uncoated Cardiovasc Interv 2014;7:1048–56. 19Treating traumatic aortic injuries
C
hallenges and
solutions in the
endovascular
management of
traumatic aortic
injuries were laid bare by
Sanjeev Kumar, an interventional
radiologist within the department
of cardiovascular radiology and
endovascular interventions at
the All India Institute of Medical
Sciences (AIIMS), New Delhi, India.
Dr Kumar started by
highlighting the high rates
of mortality for patients with
traumatic aortic injuries: “Seventy
percent of them die on the spot,
and of those patients who reach
a trauma centre, 50% will die
within 24 hours – before they are
treated,” he said. “Hence time is
crucial when you are talking about
traumatic aortic injuries in this
group of patients.”
Dr Kumar stressed that
the treatment paradigm for
traumatic aortic injuries has
changed drastically over the
last two decades. Endovascular haemodynamically unstable.
“Since patients are young with a
“Since time is successful outcome,” he added.
With polytrauma patients there
exposure, he said.
Elaborating on each challenge
repair has largely replaced open
repair, for example, resulting in a small radius of the curvature of life, optimising is also a risk of intra-procedural in turn, Dr Kumar started
major reduction in mortality and the aortic arch, conformity of the haemorrhage, requiring by looking at the effect of
procedure-related paraplegia, device to the arches is an issue,”
the timing for optimum anticoagulation. hypovolaemia on device sizing.
yet conversely it is associated he explained. a repair is very In addition, remodelling and “As we know, hypovolaemia
with increases in early graft- Tears are usually located in ageing of the aorta occurs with decreases aortic diameter,” he
related complications. the vicinity of the isthmus, noted important for time. “And since they are young said. “It’s been studied in unstable
Such rises are indicative of Dr Kumar, thus the coverage
a successful patients, the natural history of patients with a mean arterial
the many challenges in carrying of the subclavian artery (SCA) this ageing is not widely studied,” pressure (MAP) of 75 mmHg and
out endovascular repair, said Dr in emergency situations poses outcome.” added Dr Kumar. Similarly, a heart rate of more than 130
Kumar. The sizing of the grafting a great problem. “Since time is optimal follow-up for such beats per minute.” The aortic
presents a particular challenge life, optimising the timing for Sanjeev Kumar patients should be addressed size in such patients has been
20 because many patients are so a repair is very important for a to limit the cumulative radiation underestimated by as much as13%, he underlined, therefore when you are treating aortic
there may be a mismatch trauma patient, device selection
between the aortic diameter becomes very important,”
and the endograft which could he explained.
theoretically result in an increased Dr Kumar went on to discuss
risk of endoleak or other vessel diameter. “Often at times
endograft-related complications. because young patients have
“In this group of patients, if they inotropic support, you must
are haemodynamically unstable, consider the access vessel in
we should do a 10% over-sizing these patients,” he explained. Such
over and above the normal over- patients may be on the borderline,
sizing,” he explained. said Dr Kumar. “But still you can
Most of these trauma patients consider higher thresholds in this
are young, too – at least patient because of the young
compared to patients typically
experiencing aortic aneurysms. “In higher-
“They have a smaller radius of
aorta curvature compared with grade lesions,
aneurysmal patients,” said Dr endovascular
Kumar. “And, because of the sharp
aortic angulation distal to the left interventions are operative management results in these patients are bleeding from In his concluding remarks, Dr
SCA, the conformity of the device
to the aortic arch – and hence
recommended.” mortality rates as high as 50% in
these patients.”
everywhere, such as liver trauma.”
Indeed, heparinisation with an
Kumar said that minimal aortic
injury, i.e. patients with grade I and
provision of an adequate ceiling – He outlined coverage of anti-clotting time in the range of grade II lesions without external
is always a challenge.” Too much
Sanjeev Kumar the left SCA. “Because of the 200 is recommended, and routine contour abnormality, should
oversizing risks graft corrugations vicinity of the trauma, often in an heparinisation should be provided be managed conservatively.
or collapse, he added. and elastic nature of the vessels,” emergency situation will you need at a lower dose than administered “Endovascular repair is still
Dr Kumar outlined an he added. to cover this left SCA and you are during elective TEVAR. Spinal considered a procedure of choice
older case in which a typical “However, if your access vessel not able to assess the adequacy drainage, on the other hand, is not in suitable morphology patients,”
aortic arch injury – an isthmic is inadequate, you can always go of the Circle of Willis or the routinely recommended in such he said. “In higher-grade lesions,
pseudoaneurysm – was treated to the iliac, for example, which dominance of the left tibial artery,” patients, noted Dr Kumar. endovascular interventions
with a GORE TAG (WL Gore & was done in [one of my] patients he said. Summing up, Dr Kumar said are recommended.
Associates, USA) device. The for a successful aortic repair.” “However, if the left SCA is that the long-term natural history “Urgent repair should be
follow-up CT showed poor But Dr Kumar’s abiding covered, you should check the is still unknown in such young carried out within 24 hours
positioning and nonconformity message is of prompt treatment. dominance of the right vertebral patients. “There are certain or at least before the hospital
of the device. This led to graft “Urgent repair within 24 hours is artery and Circle of Willis and, morphological changes of the discharge. This is the ideal time for
collapse that was ultimately recommended in the guidelines if the anatomy is unfavourable, aorta which take place over time,” the treatment,” he said. “We still
treated by a proximal overlapping if there are no other serious surgical revascularisation should he said. “And also, the follow- need to devise the optimal follow-
stent graft (Valiant, Medronic, concomitant injuries,” he said. be considered in this patient,” up strategy and the cumulation up and understand the natural
Ireland). “Nowadays we have a “But at least the patients should he said. of radiation exposure is a key history of these patients, and see
lot of devices on our shelf which be repaired before hospital Heparinisation is a major component in managing this how they progress over a period
improve conformability, hence discharge because non- challenge, he went on: “You know patient with endovascular repair.” of time.” 21You can also read