Annals of Emergency Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Supplement to
Annals of Emergency Medicine An International Journal
volume 78 number 2 August 2021
August 2-6, 2021
Online at covidrf.acep.org
2A Schedule of Presentations
S1 Oral Presentations
www.annemergmed.com
YMEM_v78_i2_sS_COVER.indd 1 7/29/2021 11:28:50 AM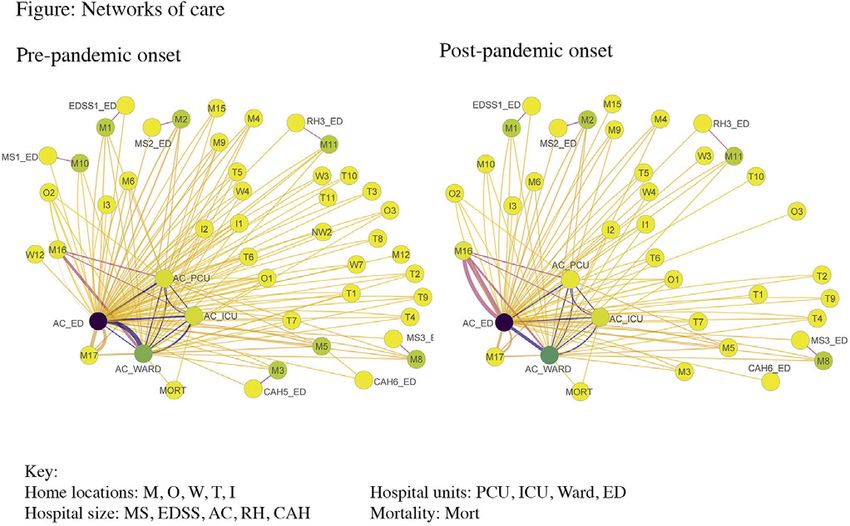
AUGUST 2021
VOLUME 78 NUMBER 2S
Supplement to
ACEP
Annals of Emergency Medicine
Journal of the
American College of
R ESEARCH
Emergency Physicians
F ORUM
Special Edition: COVID
August 2-6, 2021
Annals of Emergency Medicine is owned by Online at covidrf.acep.org
the American College of Emergency Physicians
(www.acep.org). Manuscript submissions and 2021 Research Committee/Research Forum Subcommittee
editorial correspondence should be sent to the Alex Limkakeng, MD, MHSc, FACEP, Research Forum Special Edition: COVID Co-Chair
Editorial Office. Michelle P. Lin, MD, MPH, MS, FACEP, Research Forum Special Edition: COVID Co-Chair
Annals Loren E. Rives, MNA, ACEP Staff
ACEP Marla Payne, ACEP Staff
PO Box 619911
Dallas, TX 75261-9911 2021 Research Forum Special Edition: COVID Abstract Reviewers
John Ashurst, DO, MSc, FACEP
4950 W. Royal Lane Aaron Barksdale, MD, FACEP
Irving, TX 75063-2524 Megan Dougherty, MD
Richard D. Gordon, MD, FACEP
800-803-1403
Matt Gratton, MD, FACEP
Business correspondence (subscriptions, perm- Sarathi Kalra, MD, MPH
ission, and reprint requests, advertising sales Anthony T. Lagina, MD, FACEP
and production) should be sent to Elsevier Patrick Meloy, MD, FACEP
Inc., 1600 John F. Kennedy Boulevard, Suite Joshua J. Oliver, MD
1800, Philadelphia, PA 19103-2888, tele- Brian O’Neil, MD, FACEP, FAHA
phone 800-523-4069. Claire Pearson, MD
Kristine L. Schultz, MD
Copyright © 2021 by the American College of R. Gentry Wilkerson, MD, FACEP
Emergency Physicians. All rights reserved: No Anna Q. Yaffee, MD, MPH
part of this publication may be reproduced,
stored, or transmitted in any form or by any
means, electronic or mechanical, including This Research Forum - Special Edition: COVID was funded in part by a cooperative agreement with the Centers for
photocopy, recording, or any information stor- Disease Control and Prevention (grant number 1 NU50CK000570). The Centers for Disease Control and Prevention is
age and retrieval system, without permission an agency within the Department of Health and Human Services (HHS). The contents of this event and Research Forum
in writing from the Publisher. website do not necessarily represent the policy of CDC or HHS and should not be considered an endorsement by the
Federal Government.
Neither Annals of Emergency Medicine nor
the Publisher accepts responsibility for state-
ments made by contributors or advertisers.
Acceptance of an advertisement for placement
in Annals in no way represents endorsement
of a particular product or service by Annals of
Emergency Medicine, the American College
of Emergency Physicians, or the Publisher.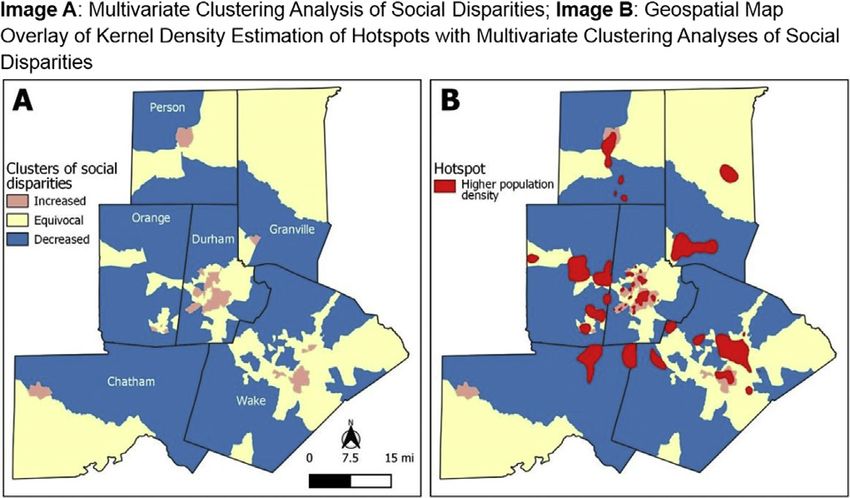
RESEARCH FORUM SPECIAL EDITION: COVID EDUCATIONAL PROGRAM 2021
Monday, August 2, 2021 – On-Demand Access to the Virtual - #10 Facilitated Peer Support Model Offers
Poster Hall available. Promising Mental Health Intervention for
Tuesday, August 3, 2021 - On-Demand Access to the Virtual Emergency Medicine Physicians During the Post-
Poster Hall available. Pandemic Period
WEDNESDAY, AUGUST 4, 2021 – TRACK 1
4:15 – 5:15 pm Central Abstract Session: Clinical Risk Factors
- #11 Impact of BMI on Outcomes in Patients Hospitalized
10:00 – 11:00 am Central Keynote Address for COVID-19
- #12 The Association of Altered Mental Status in the
11:00 – 11:30 am Central COVID-19: A Status Update – Lauren Westafer, Emergency Department With In-Hospital Mortality in
DO, MPH, MS COVID-19 Patients
- #13 Comorbid Conditions With COVID-19 in
11:30 – 12:30 pm Central Plenary I: State-of-the-Art
Hospitalized Pediatric Patients: A Multi-Center Analysis
- #1 Correlation Between New York City Hot Spotting
- #14 External Validation of the Quick COVID-19 Severity
Policy and Mobility to Reduce COVID-19 Spread
Index: A Prognostic Tool for Early Clinical
- #2 Racial Disparities in Patients Hospitalized for
Decompensation
COVID-19: an Observational Cohort Study
- #3 MyCOVIDrisk: User Experience (UX) Study of 4:45 – 5:15 pm Central Abstract Session: Innovations in Telehealth and Care
COVID-19 Risk Assessment and Mitigation Application Delivery
- #4 Association of the Initial Clinical Characteristics With - #15 Long-Term Follow-up of Emergency Department
the Need for the Intensive Care Unit and Hospitalization in Patients Discharged With Moderate Hypoxia and
Patients Presenting to the Emergency Department With COVID-Like Illness in New York City During Height
Acute Symptomatic COVID-19 of the COVID-19 Pandemic
- #5 It’s Time to Rethink How We Screen for - #16 Temporal Associations Between Decreasing Emergency
Communicable Diseases in the Emergency Department: Department and Increasing Emergency Telehealth Volumes
Lessons Learned From COVID-19 During the COVID-19 Pandemic: A Time-Series Analysis
From 2 Academic Medical Centers
12:30 – 1:00 pm Central Pandemic Critical Care Sure Support for Under- - #17 Telemedicine for Veterans in the Setting of the
resourced Communities – Rob Rodriguez, MD
COVID-19 Pandemic: Lessons Learned from Visn 8’S
Clinical Contact Center (A Virtual Urgent Care) in
1:00 – 1:30 pm Central Building the Plane While Flying it –
Alexandra Weissman, MD, MS, MPH; Kusum S. Avoiding Emergency Department Visits
Matthews, MD, MPH, MSCR; Joseph Bledsoe, MD, - #18 The Impact and Efficiency of Medical Screening Exams
FACEP, Peter Hou, MD in Forward Treatment Areas at NYC Public Hospitals
During the Initial COVID-19 Surge
1:30 – 2:00 pm Central COVID-19 – The Year EM Changed –
Mark Rosenberg, DO, MBA, FACEP
5:15 – 5:30 pm Central Closing Remarks –
Alexander T. Limkakeng, Jr., MD MHSc, FACEP; Michelle P. Lin,
2:00 – 2:45 pm Central Sex- or Gender-Specific Differences in the Clinical
MD, MPH, MS, FACEP
Presentation, Outcome, and Treatment of SARS-CoV-2 –
Jeannette Wolfe, MD; Basmah Safdar, MD, MSc; Tracy Madsen,
MD, PhD, FAHCEP, FAHA; Marna Rayl Greenberg, DO, MPH, 7:00 – 9:00 pm Central Theater of War
FACEP
2:45 – 3:15 pm Central An Emergency Physician With Long COVID: WEDNESDAY, AUGUST 4, 2021 – TRACK 2
Understanding the Patient Experience From a Fresh Perspective –
Jeffrey N. Siegelman, MD
11:00 – 11:30 am Central Abstract Session: Bedside Tools
3:15 – 4:15 pm Central Plenary II: Resilience-What Can We Do About it? - #19 Automated Quantification of B-Lines in Lung
- #6 Healthcare Worker Psychological and Physiological Ultrasound on COVID-19 Patients
Health During the COVID-19 Pandemic - #20 Safer Delivery of Aerosolized Medications When
- #7 Shifting Trends in Pediatric Emergency Department Dealing With COVID-19 and Other Contagious Airborne
Psychiatric Visits After the Arrival of COVID-19 Viruses
- #8 Resident Physician Perspectives on the Impact of - #21 Lung Ultrasound Versus Chest X-Ray for the
COVID-19 on Professional Interpersonal Relationships and Radiographic Diagnosis of COVID-19 Pneumonia in a
Workplace Social Capital: A Qualitative Study High Prevalence Population
- #9 Title: Managing Burnout in a Prolonged Crisis: A - #22 Flow and Pressure Differential Results of a Novel
2-Wave Cross-Sectional Analysis of Emergency Department Low-Cost Portable Negative Pressure Patient Enclosure for
Personnel Over 6 Months of the COVID-19 Pandemic COVID-19
2A Annals of Emergency Medicine Volume 78, no. 2s : August 2021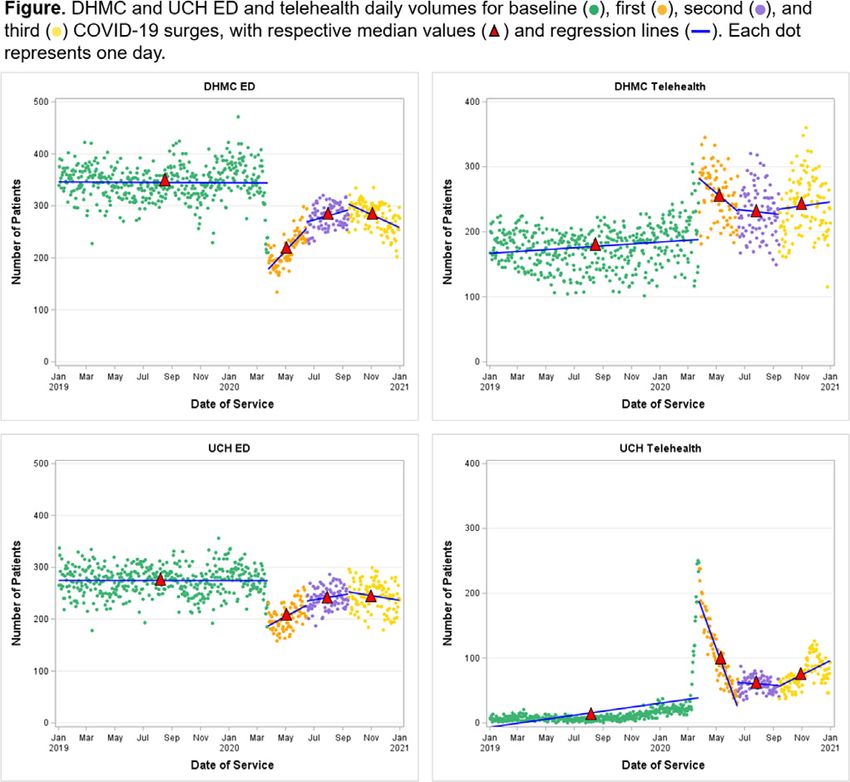
Research Forum Special Edition: COVID Educational Program 2021
WEDNESDAY, AUGUST 4, 2021 – TRACK 2 —cont'd
12:30 – 1:00 pm Central How We Maintained our Clinical Research - #32 Decay of Anti-SARS-CoV-2 Nucleocapsid Igg in
Enterprise During the Pandemic –
Fred Korley, MD, PhD
Seropositive Healthcare Workers Over Time
- #33 Bamlanivimab Reduces COVID-19 Related
1:00 – 1:30 pm Central Abstract Session: Vaccination Emergency Department Return Visits and Hospitalizations
- #23 Degree, Timing and Factors Observed in COVID-19 at a Rural US-Mexican Border Hospital
Post-Vaccination Humoral Antibody Development - #34 Polk COVID-19 and Flu Response Clinical Trial
- #24 COVID-19 Vaccine Hesitancy Among Emergency
4:15 – 5:15 pm Central Abstract Session: Resilience II
Department Patients and Caregivers in New York City
- #25 Correlations Between Community COVID-19 - #35 Prevalence and Predictors of Post-Traumatic Stress
Prevalence, Vaccine Availability and Emergency Disorder Symptoms Among Emergency Physicians in the
Department Non-COVID-19 Utilization United States During the COVID-19 Pandemic
- #26 Implementation of a COVID-19 Vaccine Emergency - #36 Comparison of Mental Health Visits at a Military
Department Education Program for Underserved Treatment Facility Emergency Department Pre- and Post-
Communities: A Pilot Quality Improvement Project COVID-19 Pandemic
- #37 COVID-19 and Medical School Curriculum: Can
1:30 – 2:00 pm Central COVID-19 Research at the Emergency Medicine Successfully Adapt to a Virtual
National Institutes of Health – Format of Teaching?
Jeremy Brown, MD - #38 Posttraumatic Stress in Emergency Department
Healthcare Workers During the COVID-19 Outbreak in
2:00 – 2:45 pm Central EMF Showcase Brooklyn, New York
- #27 Social Determinants of Health and COVID-19
Infection in North Carolina: A Geospatial Analysis 4:45 – 5:15 pm Central Abstract Session: Disparities and Public Health
- #28 The Opioid Epidemic Meets the Coronavirus - #39 Impact of Socioeconomic Status on COVID-19
Pandemic: Rates and Patient Characteristics of Emergency Disease Severity
Department Visits for Opiate Use Disorder During the - #40 Facemasks: Perceptions and Use in an Emergency
COVID-19 Pandemic in the Los Angeles County Public Department Population During COVID-19
Hospital System - #41 Health Insurance and Duration of Symptoms Prior to
- #29 Interpreter Variability of Lung Point-of-Care Ultrasound Emergency Department Visit: An Analysis of 19,850
Rubric in a Population of Non-Critically Ill COVID Patients Patients With Suspected COVID-19
- #30 COVID-19 Infection Experiences and Social - #42 First Year of COVID-19: Stay at Home Decreased
Determinants of Health in North Carolina - A Qualitative Accidents, but Increased Assaults
Analysis
Thursday, August 5, 2021 – On-Demand Access to the Virtual
2:45 – 3:15 pm Central Abstract Session: Antibodies and Monoclonals Poster Hall available.
- #31 Emergency Department-Based Monoclonal Antibody Friday, August 6, 2021 – On-Demand Access to the Virtual
Therapy for Patients With Mild to Moderate COVID-19 Poster Hall available.
Volume 78, no. 2s : August 2021 Annals of Emergency Medicine 3A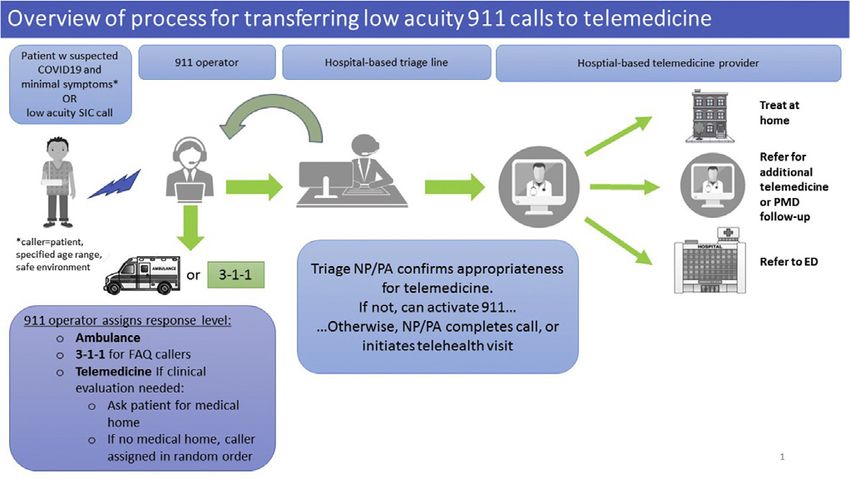
ACEP 2021 DISLOSURE REPORT
In accordance with the Accreditation Council for Continuing Medical Education (ACCME) Standards and the policy of the American College of
Emergency Physicians, presenters must disclose the existence of significant financial interests in or relationships with manufacturers or commercial
products that may have a direct interest in the subject matter of the presentation, and relationships with the commercial supporter of this CME
activity. These presenters do not consider that such relationships will influence their presentation.
Name Company Name Nature of Relationship
M. DiLorenzo Abbvie Owns stock
Ark Genomic Revolution
CVS Health
Edwards Life Sciences
Merck
C. Baloescu Philips
M.F. Young Pfizer
4A Annals of Emergency Medicine Volume 78, no. 2s : August 2021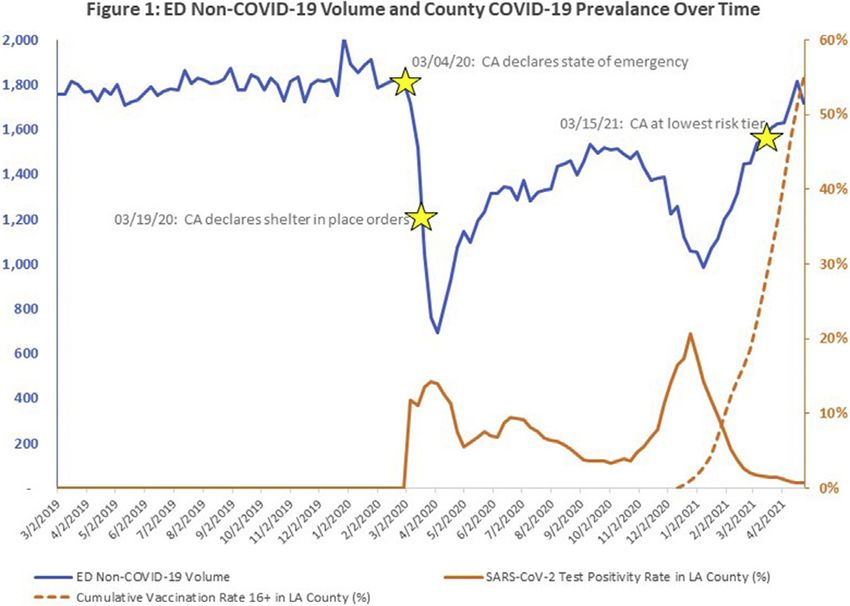
RESEARCH FORUM ABSTRACTS – SPECIAL EDITION: COVID
From the American College of Emergency Physicians
1 Correlation Between New York City Hot Spotting
Policy and Mobility to Reduce COVID-19 Spread
Ngai K, Sheehan D, Tang Y, Hsuan C, Zebrowski A, Carr B/Icahn School of Medicine at
2021 Research Forum – Special Edition: COVID Mount Sinai, New York, New York; Icahn School of Medicine at Mount Sinai, New York,
August 2-6, 2021 New York; Icahn School of Medicine at Mount Sinai, New York, New York; The
Pennsylvania State University, Icahn School of Medicine at Mount Sinai, New York,
New York; Icahn School of Medicine at Mount Sinai, New York, New York
Study Objective: In October 2020, New York State initiated a micro-cluster
strategy (“hot spotting”) that divides into three categories based on COVID-19 cases
and hospital capacity, each with successively more restrictions: Yellow, Orange, and
Red Zones. Our objectives were to evaluate the influence of hot spotting on mobility
and subsequent mortality, and then to identify underlying social determinants of health
associated with the neighborhoods most affected by hot spotting.
Study Design: We combine several data sources in our analysis. Time-dependent
data were obtained from SafeGraph for cellphone mobility at the Census Block Group,
New York State Governor’s Office for hot spotting, school and indoor dining, and NYC
Department of Health and Mental Hygiene (DOHMH) for COVID-19 cases and
mortality. Using the DOHMH’s “Modified Zip Code Tabulation Areas” (MODZCTA),
we matched these to community-level data obtained from 2018 American Community
Survey 5-year estimates for population density. Our main outcomes are Average Median
Percentage Time Home (AMPTH) and Device-Weighted Average Median Percentage
Time Home (DWAMPTH) from SafeGraph Social Distancing Metrics summarized to
MODZCTA boundaries. Home is defined as the common nighttime location of each
mobile device over a 6-week period to a Geohash-7 granularity (w153m x w153m). We
implemented the Wilcoxon rank-sum test with a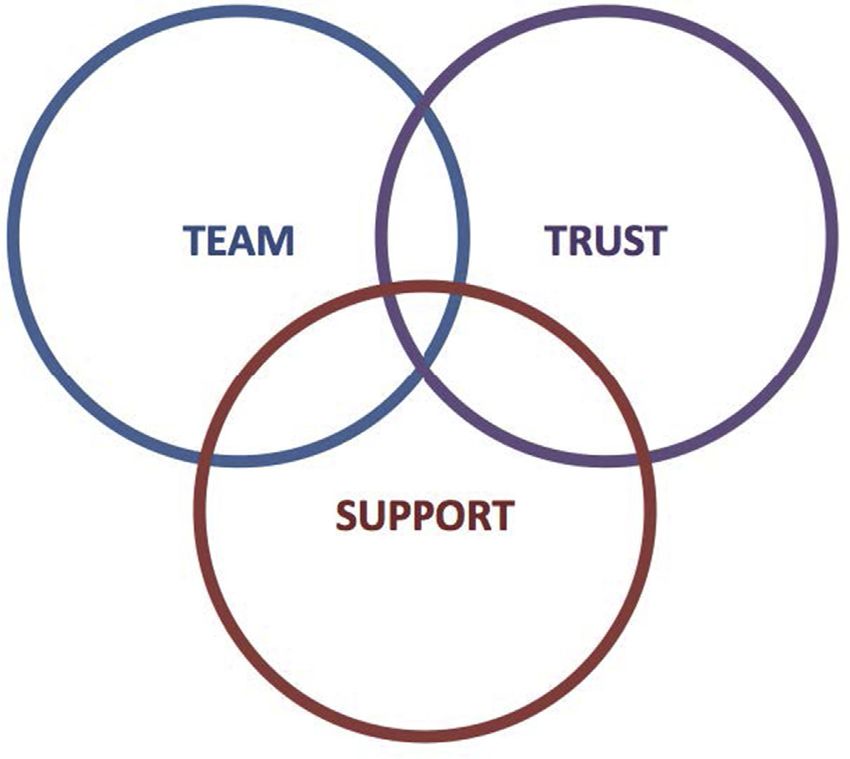
Research Forum Abstracts – Special Edition: COVID
Results: The dataset consisted of 45,360 patients. The cohort was 22% Black, 35% Other common recommendations included more customization options (eg, ability to
Hispanic, 37% White, and 6% Other. The mortality was 15% for all groups. White change font size), having more information when hovering over icons, and options to
patients had the highest mortality rate at 17% compared to 10% in Blacks, 14% in send inputs and risk score results to others or to print them for documentation.
Hispanics, and 15% in Other (ANOVA, p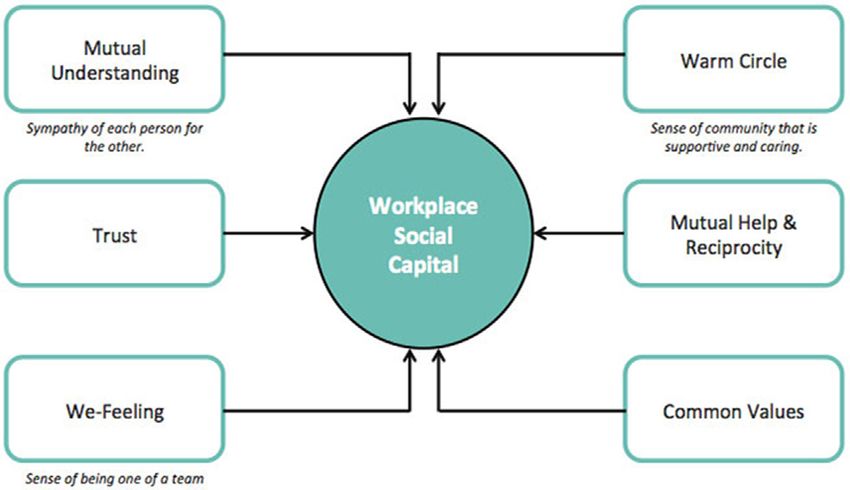
Research Forum Abstracts – Special Edition: COVID
required ICU care or died were more likely to experience altered mental status (aOR attending physician COVID-19 probability assessment – was best at identifying
3.8, 95% CI: 2.1, 6.6), but were less likely to report history of fever (0.5, 95% CI: patients who had COVID-19 (based on subsequent PCR confirmation).
0.3, 0.8). Methods: All 748 patients admitted from the ED between April 27, 2020, and
Conclusions: In ED patients with acute COVID-19, complaints of sore throat, May 17, 2020 were included. Sensitivity, specificity, and positive and negative
myalgias, headache or smell/taste disturbances were associated with discharge and predictive values were calculated for each screening tool. Logistic regression was used to
convalescence at home. Patients who were age 65, Black/African American, assess each tool’s performance. A principal components analysis (PCA) was performed;
experiencing dyspnea, diarrhea, or altered mental status were more likely to undergo the resulting factors were used to model COVID-19 positivity.
hospital admission. Among all admitted patients, altered mental status was positively Results: The emergency physician’s probability assessment yielded higher
associated with ICU care or death, and a history of fever was negatively associated with sensitivity (0.62, 95% confidence interval [CI] 0.53-0.71, Table 1) than the NTS
ICU care or death. COVID-19 presents with a heterogeneous constellation of (0.46, 95% CI 0.37-0.56), and had higher specificity (0.76, 95% CI 0.72-0.80) than
symptoms, and an understanding of the association of the presenting symptoms with the NTS (0.71, 95% CI 0.66-0.75) and the emergency clinician ROS (0.62, 95% CI
the ultimate patient outcome may be useful for allocating resources and targeting 0.58-0.67). Categorization as moderate or high probability on the emergency
management plans. physician’s probability assessment was also associated with the highest odds of having
COVID-19 in regression analyses (adjusted odds ratio¼4.61, 95% CI 3.01-7.06).
Moderate agreement (kappa 0.41-0.60) was observed between the NTS and ED
clinician ROS for fever, cough, shortness of breath, and diarrhea; fair agreement (kappa
0.21-0.40) for sore throat, headache, abdominal pain, and vomiting; and poor
agreement (kappa 0.00-0.20) for myalgias and chills. The 323 patients who had a
response recorded for every symptom were included in the PCA. Only Factor 1 (fever,
chills, fatigue, sore throat, rhinorrhea, and cough) was associated with increased odds of
testing positive for COVID-19.
Conclusion: While the emergency physician’s probability assessment had higher
sensitivity and specificity than the other two tools, none of the tools evaluated in this
study was sufficiently accurate enough to replace a COVID-19 PCR test on a patient
entering a clinical setting where transmission control is crucial. These findings
suggest that hospitals not rely on symptom or probability assessment in determining
infection status but continue to utilize widespread testing. We recommend that
providers in other countries experiencing COVID-19 surges consider the relevance
of these findings and that as the pandemic develops (with the potential for continued
new variant strains), diagnostic testing efforts should supersede the use of clinical
screening tools.
5 It’s Time to Rethink How We Screen for
Communicable Diseases in the Emergency
6 Health Care Worker Psychological and Physiological
Health During the COVID-19 Pandemic
Chang B, Shechter A/Columbia University
Department: Lessons Learned From COVID-19
DiLorenzo MA, Davis MR, Dugas JN, Nelson KP, Grochow Mishuris R, Ingalls RR, Study Objective: Previous work has established that frontline health care workers
Hochberg NS, Schechter-Perkins E/Boston Medical Center, Boston, Massachusetts (HCWs), such as emergency physicians and nurses, are vulnerable to the development
of adverse behavioral, psychological, and physical sequelae, which may persist long after
Study Objectives: COVID-19 symptom severity varies between patients, and some the disaster. We examine the prevalence and predictors of psychological distress in ED
remain asymptomatic. During early April 2020, 70% of patients admitted to the clinicians working during the COVID-19 pandemic. We examined psychological and
emergency department (ED) of a major hospital in New England had COVID-19, physiological (sleep, resting heart rate, blood pressure) of a sample of frontline
many of whom required treatment in the intensive care unit. As the volume of providers during the COVID-19 pandemic
COVID-19 cases presenting to the ED increased, it became essential to develop Methods: This was a sample of 52 clinicians (physicians, residents, nurses, PAs,
accurate triage protocols to separate COVID-positive from COVID-negative patients. NPs) who were frontline HCWs during the COVID-19 pandemic across a diverse
This study assessed which of three different clinical screening tools – a nursing triage (academic, community, urban, and suburban) range of four emergency departments in
screen (NTS), an ED clinician Review of Systems (ROS), and a standardized ED the New York Metropolitan area during July 2020-September 2020. Study design is a
Volume 78, no. 2s : August 2021 Annals of Emergency Medicine S3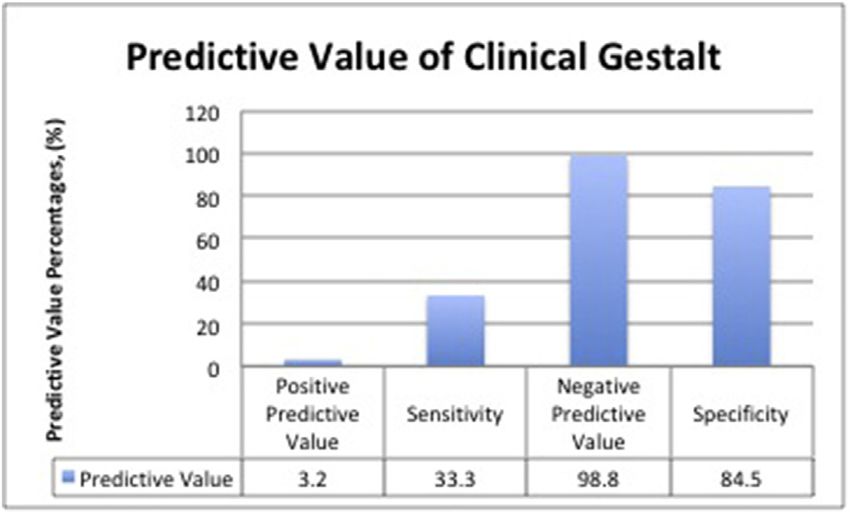
Research Forum Abstracts – Special Edition: COVID
longitudinal prospective cohort design. At baseline, we conducted a psychological test
battery including measures of COVID-19 related stress, PTSD (PCL-5), anxiety
(GAD-5), depression (PHQ-9), and burnout (Maslach Burnout Inventory). We also
assessed home blood pressure at wake/sleep, resting heart rate, and sleep duration using
an accelerometer watch device (Fitbit).
Results: Baseline demographics in our sample had more self-identified women
participants (62%), caucasian (67%), with median age of 42. Sample was diverse,
containing physicians/advanced practice providers (45%) nurses (43%) and residents
(12%) At baseline, positive screens for psychological symptoms were common; 48%
for acute stress, 37% for depressive, and 30% for anxiety symptoms. Overall, housestaff
rates for acute stress and depression did not differ from attendings or nurses. Overall
participants had elevated levels of emotional exhaustion on burnout surveys (median
24, SD 3.5). Average sleep duration was 6.2 hours (SD 1.3), resting heart rate of 86
(SD 18.2), and home blood pressure of 128/76. Increased levels of emotional
exhaustion was positively associated with elevated resting blood pressure (Pearson r¼
.32), and resting heart rate (r¼.38), while negatively associated with sleep duration
(r¼.23).
Conclusion: Our preliminary work and others have highlighted that HCWs are
web 4C=FPO
experiencing significant COVID-19-related psychological and physical distress. Future
work and data will address key questions such as whether such elevated distress
symptoms remain persistent with the evolution of the pandemic. This work and others
emphasize the need for continued mental health support measures for HCWs both
during and in the aftermath of the pandemic.
7
Figure 1. Three primary themes identified as key features of
Withdrawn
strong workplace interpersonal relationships.
8 Resident Physician Perspectives on the Impact Of
COVID-19 on Professional Interpersonal Relationships
and Workplace Social Capital: A Qualitative Study
Querin LB, Allen A, Hamm R, Flynn H/University of North Carolina, Chapel Hill, North
Carolina
Study Objectives: Interpersonal relationships between emergency medicine
resident physicians and their colleagues is key for resident wellness and for optimizing
patient care. Studies have shown that the COVID-19 pandemic has reduced social
connectedness and negatively impacted workplace social capital in many non-medical
professions, yet studies are limited in the medical field, particularly with physicians.
web 4C=FPO
This project sought to uncover resident physician perspectives on the impact of
COVID-19 on professional relationships and to gain ideas on how to optimize
workplace social capital despite and beyond the current limitations of the pandemic.
Methods: This study was conducted at a single academic hospital in the United
States between March-April 2021. Data was collected from emergency medicine
residents via open-ended response online surveys and a semi-structured focus group
discussion. A team of three investigators independently analyzed data from open-ended Figure 2. The 6 core features of workplace social capital.
survey responses and the focus group transcription, using a grounded-theory approach
and consensus of the independent analyses was subsequently generated to identify final
themes and subthemes.
Results: Three main themes regarding resident perspective on professional
interpersonal relationships and social capital were identified: team, trust, and support.
We also report the 6 core factors discussed by residents that have changed secondary to
the COVID-19 pandemic. EM resident physicians feel that the COVID-19 pandemic
has impacted environment, socialization, staff turnover, teaching/debriefing, capacity
limits and approach to education, which have demonstrated an overall negative impact
on interpersonal relationships and social capital. It has also, however, positively
impacted a sense of unity within the emergency department team that residents feel has Figure 3. Factors changed during the COVID-19 pandemic and
enhanced relationships and social capital. experience outcomes/consequences.
Conclusions: The COVID-19 pandemic will have lasting impacts on the way our
hospitals and residencies function. The findings of this study may help to ignite
discussion on how we can build on the positive, while limit the negative impacting
features that have been shaped from the COVID-19 pandemic.
S4 Annals of Emergency Medicine Volume 78, no. 2s : August 2021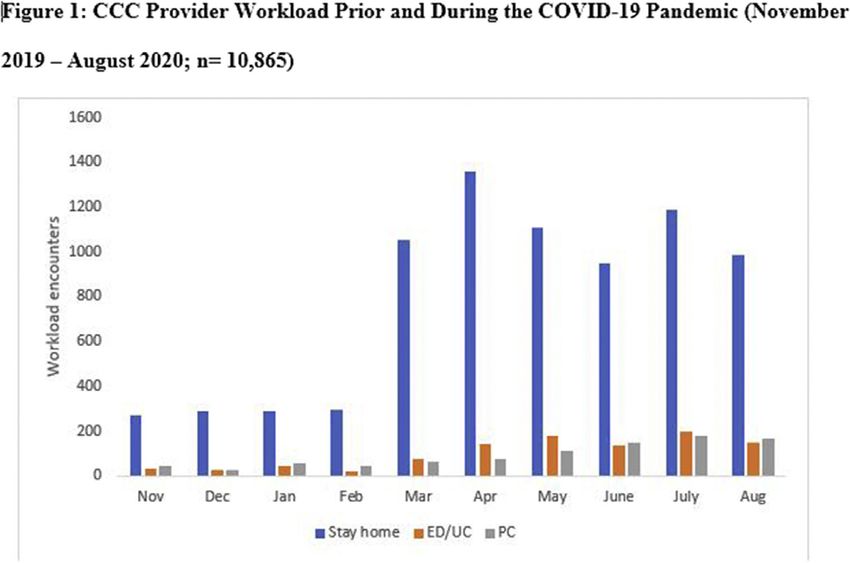
Research Forum Abstracts – Special Edition: COVID
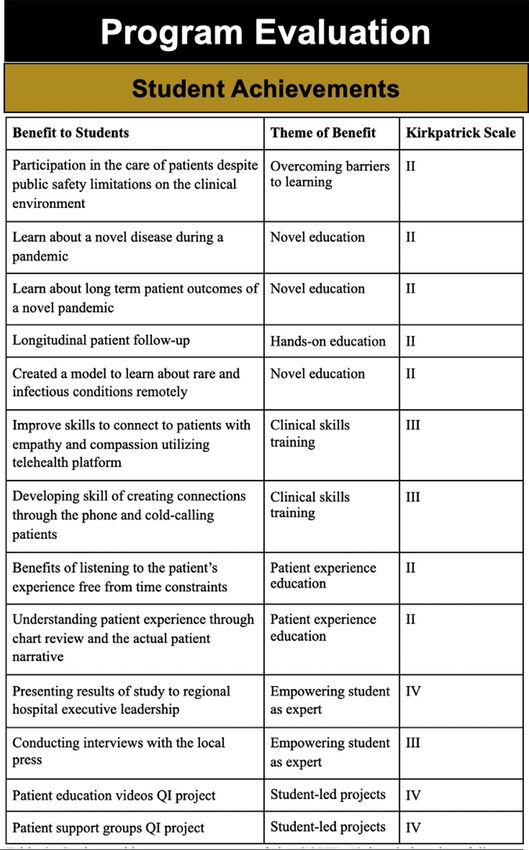
Table 1: Examples of resident physician perspectives supporting the three identified themes important for strong workplace interpersonal relationships & the
paralleled features of workplace social capital.
Theme Examples Paralleled Features of Workplace Social Capital
Team "The ED is a team environment and when shit is hitting the
fan you have to count on the team... "
"... You also need to show that you are a team player so that
when you ask for something out of the ordinary or for
something to get done quickly, people know that you are
willing to help them when they need it, etc."
"We are a beehive and you need all the bees to make the hive
function. It’s the most important aspect of our specialty
and providing good care in a happy environment"
Trust " .. .relationships and trust are paramount to success"
" ...it’s important to build trust."
"You need to have the trust of the people working around you
to trust your clinical decisions... "
"You have to feel comfortable with those you work with to be
on your team, especially with sick patients... "
Support "For a lot of people going to residency they don’t have family
in their new residency spots, therefore the residency
becomes their family and support."
"Residency is a tough time and having a group of people who
you can be close with matters every single day."
"It gives you more of a purpose to come to work when you’re
helping out colleagues and have camaraderie"
9 Managing Burnout in a Prolonged Crisis: A 2-Wave problem-solving (JPS), clear process and leader inclusiveness using logistic regressions.
Cross-Sectional Analysis of Emergency Department Models controlled for age, sex, race, location, tenure and shift, as well as county
Personnel Over 6 Months of the COVID-19 Pandemic COVID-19 case burden using open-access data from John Hopkins University’s
Coronavirus Resource Center.
Bhanja A, Kerrissey MJ, Peabody C, Hardy J, Hayirli TC, Stark N/Harvard T.H.
Results: The sample across both waves consisted of 75 attendings (14.79%), 50
Chan School of Public Health, University of California, San Francisco; University of
California, San Francisco, Harvard Medical School, University of California, San
residents/fellows (9.89%), 38 advance practice providers (5.56%), 254 registered
Francisco nurses (37.13%) and 90 other ED personnel (therapists, social workers, etc.)
(13.16%). Burnout increased over time, where 32.22% reported burnout in wave 1
Study Objective: Management research suggests that inclusive leaders, problem- and 56.51% in wave 2. Worsening burnout also increased over time, 57.32% to
solving teams and clear processes might matter for addressing uncertainty, but how 80.52% respectively. Clear process and leader inclusiveness were significantly
these factors unfold during prolonged crisis and their relationship to burnout is not associated with lower odds of burnout across both time points, 0.28 (p < 0.001) and
well understood. The study objective was to examine associations between teamwork 0.45 (p < 0.05) in wave 1 and 0.30 (pResearch Forum Abstracts – Special Edition: COVID
participants reported feeling better at the end compared to the beginning of each
session. Eighty six percent of physicians reported they would recommend peer support
groups to a friend or colleague. Positive effect sizes showed improvement in 8 of 11
distress symptoms, and marginal significance (pResearch Forum Abstracts – Special Edition: COVID
moderate disease, with 29% having severe disease and 14% have critical diseases. Results: We included 824 visits with 51% male, a mean age was 67.1 (SD 17.0) and
The overall mortality was 15%. The overall hospital median length of stay (LOS) 153 (18.6%) had AMS. There were 132 deaths for an overall mortality rate of 16.1%.
was 5 days (IQR 3-11). Patients with higher BMI were significantly more likely to Patients with AMS had in-hospital mortality of 38.2% (95% CI 30.4%-46.4%),
require mechanical ventilation and require pressor support (PResearch Forum Abstracts – Special Edition: COVID
16 Temporal Associations Between Decreasing
Methods: This was a retrospective observational cohort study of COVID-19 patients
admitted from the emergency department between Feb 29, 2020 to Feb 1, 2021. The Emergency Department and Increasing
health care system is composed of a mix of 2 community and 4 academics EDs in a major Emergency Telehealth Volumes During the COVID-
metropolitan area. Patient demographics, vital signs, laboratory results were extracted 19 Pandemic: A Time-Series Analysis From Two
from our institutional COVID-19 Data Warehouse. Following the convention of qCSI
Academic Medical Centers
variables, respiratory rate (breaths/min), pulse oximetry (%), and oxygen flow rate (L/
Reno E, Eutermoser M, Li B, Davis CB, Shy BD/University of Colorado
min) were used to calculate points between 0 to 12, with higher points associated with
highly likelihood of respiratory decompensation within 24 hours.
Study Objectives: During the initial periods of rising COVID-19 cases and
Results: 35,696 COVID-19 patients were admitted via the emergency department
critically ill patients in 2020, overall ED volumes fell substantially. Our goal was to
during the study period. The mean qCSI was 1.73 (SD 1.82) for non-ICU admissions
compare the contrasting increase in emergency telehealth volume with the
(n¼34,647). The mean qCSI was 2.83 (SD 2.53) for ICU admission (n¼1,049). As of
decreasing ED volumes to identify staffing strategies that can be used in future
the time of submission, ED treat and release patients, as well as decompensation results
epidemics.
are pending.
Methods: We performed interrupted time series analyses to compare the
Conclusions: In this validation study of qCSI using a large system cohort of
associations of COVID-19 surges on daily ED and telehealth volumes at Denver
COVID-19 patients, qCSI appears to correlate strongly with clinical triage for
Health Medical Center (DHMC) in Denver, Colorado, and the University of
admission decision to regular floor vs. ICU level care. Further analysis is needed to
Colorado Hospital (UCH) in Aurora, Colorado. Consecutive adults from January 1,
identify 24-hour respiratory decompensation after regular floor admission.
2019, through December 31, 2020 were included, with time periods corresponding to
baseline volumes (January 1, 2019 to March 24, 2020), and first (March 25, 2020 to
15
June 15, 2020), second (June 16, 2020 to September 12, 2020), and third (September
Long-Term Follow-Up of Emergency Department 13, 2020 to December 31, 2020) COVID-19 surges according to Colorado
Patients Discharged With Moderate Hypoxia and epidemiological data. We performed pairwise comparisons between baseline versus
COVID-Like Illness in New York City During Height each COVID-19 surge for ED and telehealth daily volumes, using linear regression to
of the COVID-19 Pandemic account for secularity and non-parametric statistics to compare median values.
Daniels B, Tanyoue R, Jacobowitz A, Bhandari M, Steel P, Sharma R/Weill Cornell Results: DHMC ED daily volumes differed between baseline (median, 346
Medicine, New York, New York, Weill Cornell Medicine, Weill Cornell Medicine, Weill [interquartile range {IQR}, 325- 367]), and first (219 [196-237]; pResearch Forum Abstracts – Special Edition: COVID
17 Telemedicine For Veterans in the Setting of the
COVID-19 Pandemic: Lessons Learned From VISN
8’S Clinical Contact Center (A Virtual Urgent
18 The Impact And Efficiency Of Medical Screening
Exams In Forward Treatment Areas At NYC Public
Hospitals During The Initial COVID-19 Surge
Care) in Avoiding Emergency Department Visits Dilip M, Tan T, Natsui S, Moskovitz J/SUNY Downstate/Kings County Hospital,
Sikka V, King C, Klinker S, Mont T, Hunt B, Davis S, Fonseca J/Clinical Contact Center, Brooklyn, New York, New York City Health and Hospitals, New York City Health and
VA Sunshine Healthcare Network (VISN 8), St. Petersburg, Florida, University of Hospitals, New York City Health and Hospitals
Central Florida, VA Sunshine Healthcare Network (VISN 8), VA Sunshine Healthcare
Network (VISN 8), Virtual Care, Clinical Contact Center, VA Sunshine Healthcare Background: New York City (NYC) experienced a dramatic surge of infections
Network (VISN 8), St Petersburg, Florida with the novel SARS-CoV-2 virus in March 2020. The rapid increase in patients
presenting to emergency departments (EDs) necessitated a change in intake
Study Objective: The onset of the COVID-19 pandemic forced the health care processes in contrast to prior emergency response protocols outfitted for single day or
industry to consider telemedicine as the primary modality for health care with focus on short-term disasters. To adapt to the increased demands on patient flow, NYC
value and ease for providers and patients alike to achieve outcomes similar to face-to-face Health and Hospitals (NYC H+H) established a rapid medical screening evaluation
primary care (PC), urgent care (UC), and emergency department (ED) visits. It remained (MSE) process in each of its eleven-member public hospitals. Each hospital created
unclear if telemedicine visits actually achieved first contact resolution (FCR), fully its own treatment areas to perform their MSE. Some hospitals created a Forward
meeting the patients’ needs through their virtual care experience. At a time when Florida Treatment Area (FTA) external to the ED to evaluate and disposition patients prior
ranked #3 in its COVID-19 census, Veterans needed access to timely care to answer their to entering the ED.
concerns and questions. This is even more important as Veterans tend to have multiple Methods: Five of the eleven hospitals created external FTAs to perform rapid
comorbidities, translating into increased risk of morbidity and mortality with COVID- MSEs in accordance with EMTALA and make disposition decisions before patients
19. VISN 8, a region of the U.S. Department of Veteran Affairs (VA) that covers most of physically entered the ED. Patients 18 years and older were screened in the FTA and
Florida, South Georgia, Puerto Rico, and the U.S. Virgin Islands, established a Clinical either sent into the main ED for further evaluation or discharged home. Some sites
Contact Center (CCC) in July 2019. The CCC is a 24/7 virtual urgent care organization directed patients to an alternate care site where they could receive COVID-19 testing
providing episodic care via telephone and video with physicians and nurse practitioners (very limited availability) and/or receive further information about COVID-19. Three
who work 7 days a week from 7A to 11:30P. A physician was available overnight for hospitals utilized paper-based MSE, and two used an Electronic Medical Record
COVID-19-related concerns. This study examined the change in CCC workload as a (EMR)-based approach. Paper logs and EMR charts were reviewed using a standardized
result of the COVID-19 pandemic and assessed first contact resolution (FCR) for data extraction template. In addition, patients discharged from the FTA were contacted
patients with COVID-19 related chief complaints. by a follow-up phone call, and a structured interview was used to capture additional
Methods: This was a retrospective study centered around March 11, 2020, when data regarding their subsequent clinical course. Chi-square and Fischer’s exact test were
the World Health Organization (WHO) declared a pandemic. This analysis included a used to compare paper- and EMR-based MSE.
sample size of 6,660 patient episodes between March - August 2020. Our outcome Results: Across the five EDs, a total of 3,335 patients were evaluated in their
variable of interest was FCR. We constructed a binary disposition variable of “stay at respective FTAs. Of these patients, 970 (29.1%) were referred for further evaluation
home” or “other” which included presentation to the ED or PC. Data collected into the ED, of which 203 (20.9% of the subset) were hospitalized and nineteen
included patient age, sex, race/ethnicity, COVID-19-related chief complaints, and visit (2.0%) died. Of 2,302 patients discharged directly from the FTA, 182 (7.9% of the
modality (phone versus video). We used a logistic regression to examine factors subset) returned to the ED within seven days, resulting in 42 (1.8%) hospitalizations
affecting the probability that patients remained at home. A VA IRB determined that and seven (0.3%) deaths. The facilities using an EMR-based approach discharged
the study was exempt from review. proportionally more patients from their FTA (81.9% vs 65.3%, p < 0.001), had
Results: Figure 1 displays the increase in CCC workload during the pandemic similar seven-day return visit rates (9.3% vs 7.1%, p ¼ 0.055) and similar mortality
starting in March 2020 with a sustained ability to achieve FCR. During the pandemic, rates (0.49% vs 0.20%, p ¼ 0.251).
patients with suspected COVID-19 were 2.75 times more likely to stay at home than Conclusion: An MSE in an FTA is a highly effective process to disposition
patients calling with non-COVID-19 related chief complaints. This suggests that patients safely in a high patient volume situation. Differences exist in paper-based vs
telemedicine offers significant public health value to patients who are not presenting to EMR-based approaches, suggesting EMR-based MSEs provide better data and greater
the ED or for PC visits potentially exposing themselves and others to the spread of the effectiveness. This would suggest that prioritizing a standardized EMR-based MSE
virus. The control variables of sex and visit modality were found to not be statistically should be considered in future circumstances.
significant.
19
Conclusion: This study established the value of telemedicine in a pandemic with
FCR and avoidance of public spaces that could potentially lead to a COVID-19 Automated Quantification Of B-Lines in Lung
infection. The service provided by the CCC was invaluable to Veterans as they sought Ultrasound On COVID-19 Patients
out timely care. Baloescu C, Chen A, Raju B, Evans N, Moore CL/Yale University School of Medicine,
Philips Research North America, Philips Research North America, Yale University
School of Medicine, Yale University School of Medicine
Study Objectives: Point-of-care ultrasound (POCUS) has become an important
tool in the global response to COVID-19, supporting screening, diagnosis and
management. Lung features described in COVID-19 include B-lines (ring-down
artifacts appearing in the presence of interstitial lung fluid), thickened and
irregular pleural line, subpleural consolidations and effusions. Computer-aided
interpretation can be incorporated into POCUS platforms to provide objective
data and improve interpretations by novices. We sought to test a commercially
available B-Lines counting feature previously developed using non-COVID data,
on patients suspected of COVID-19. This first step would allow expansion to
automated B-line scoring and further lung feature detection, to create an
web 4C=FPO
intelligent POCUS system with comprehensive set of lung ultrasound features for
COVID-19 pneumonia.
Methods: This was a prospective observational study at a single academic medical
center. Subjects presenting to the emergency department with shortness of breath and
suspected COVID-19 were enrolled. The Philips Lumify TM ultrasound system with
sector or linear transducer was used to obtain 6-second clips of 14 lung zones (upper
and lower, right and left anterior, lateral and posterior). Right and left anterior upper
zone clips were also obtained with a second probe type. Repeat examinations with data
Volume 78, no. 2s : August 2021 Annals of Emergency Medicine S9Research Forum Abstracts – Special Edition: COVID
collection were performed on days 3, 5, 7 or 12+/- 1 day for admitted patients. All clips CM or ACM as described) for 5 min with immediate post-nebulization
with 2 or more B-lines were included (N¼80), as well as a random selection of 70 clips measurements (Post1) and two successive measurements (Post2/Post 3), all five
with 1 or fewer B-lines. B-line count for inclusion was based on visual rating by two minutes apart.
researchers with POCUS training. A POCUS fellowship trained emergency physician Results: Following the 5-min nebulization, mean CM PMs (Post1 cm) were
visually assessed each clip frame and counted the maximum number of B-lines per clip. 152.2-fold larger than mean ACM PMs (Post1 ACM) measurements (p¼0.001)
This was compared to automatic counts by the commercially available Lumify TM and respectively remained 49.6-fold (p¼0.005) and 7.2-fold (p¼0.006) larger at
Lung B-lines Quantification software by intraclass correlation coefficient (ICC) and Post2 and Post3 readings. PM amb and preNeb-PM were all similar (NSD) for
Cohen’s weighted kappa. both ACM and CM approaches when examining all studied particle sizes (0.5, 1.0,
Results: Of the 899 total clips,150 clips from 30 unique subjects and 44 overall and 3.0 m) including 1m preNeb-PMs, measuring 6,977 for ACM approaches and
exams were used for analysis, with 100 clips from patients with confirmed COVID 5,683 for CM use, respectively (NSD). While mean Post1 ACM 1m PMs decreased
by PCR. The average maximum B-line count by algorithm was 1.52 +/- 1.24, and (-31.7%) from pre-Neb-PM readings (6,977 to 4,662; p¼0.002), counterpart Post1
that by expert was 1.60 +/- 1.35 (ns). The ICC between algorithm and expert was CM 1m measurements rose 14,500.09% (from 5,683 to 709,549.93; p¼0.002)
0.87 (95% CI 0.83-0.91), with a weighted kappa of 0.64 (95% CI 0.48-0.81), with corresponding significant elevations for 0.5m (p¼0.001) and 3m (p¼0.002)
indicating substantial agreement. Average of maximum B-line counts, ICC and particle sizes using conventional masks. Of additional note, though applied for just
weighted kappa between algorithm and expert were comparable for COVID+ and five minutes, ACMs were uniformly well tolerated.
COVID- subgroups as well as between transducer types. For COVID + subgroup, Conclusion: Compared to conventional methods, a modified mask system
the average of maximum B-line counts was 1.73 +/- 1.28 for algorithm and 1.78 designed specifically to limit aerosolization of inhaled solutions did provide profound
+/- 1.37 for expert, with weighted kappa 0.67 (95% CI 0.50-0.84), and ICC 0.87 control of fugitive aerosolized particle emissions during nebulizer applications. The
(95% CI 0.83 to 0.91). findings indicate a much safer approach to treating COVID-19 patients and all others
Conclusion: An automated algorithm developed on non-COVID patients can requiring nebulization.
accurately distinguish and quantify B-lines in clips from patients with COVID-19,
with substantial agreement to expert visual rating.
21 Lung Ultrasound Versus Chest X-Ray for the
Radiographic Diagnosis of COVID-19 Pneumonia
in a High Prevalence Population
Gibbons RC, Mendez K, Magee M, Goett H, Murrett J, Genninger J, Tyner N, Tripod M,
Costantino TG/Lewis Katz School of Medicine at Temple University, Philadelphia,
Pennsylvania
Study Objectives: The viral illness severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2), more commonly known as coronavirus 2019 (COVID-19), has
become a global pandemic infecting over 160 million individuals worldwide.
Symptoms are often vague, and physical exam findings have proven unreliable as
20 Safer Delivery of Aerosolized Medications When
Dealing With COVID-19 and Other Contagious
Airborne Viruses
indicators of infection. Therefore, diagnosis typically relies on imaging or
nasopharyngeal swabs. The objective of this study was to compare point-of-care lung
ultrasound (LUS) with chest x-ray (CXR) to determine which is the more accurate
Pepe PE, Rios S, Leal L, Cardona JC, McNally MA, Roach JP, Antevy PM/University of diagnostic imaging modality for diagnosing COVID-19 pneumonia.
Texas Health Sciences Center, Houston, TX (USA), Houston, Texas, City of Coral Methods: This was a single-center, prospective, observational study at an urban
Springs / Parkland Fire Department, Coral Springs, Florida, Memorial Healthcare university hospital with >105,000 patient visits annually. Patients >18 years old, who
System and Joe DiMaggio Children’s Hospital, Hollywood, Florida, Coral Springs / presented to the emergency department with signs and symptoms of COVID-19, were
Parkland Fire Department, Coral Springs / Parkland Fire Department, Coral Springs, eligible for enrollment. Each patient received a LUS, performed by an emergency
Florida, Cleveland Clinic of Florida, Broward Sheriff’s Office, Fort Lauderdale Fire medicine resident or attending physician, using a portable, handheld ultrasound and a
Rescue, Weston, Florida, Coral Springs / Parkland Fire Department, Davie Fire Rescue portable AP CXR after the LUS was completed. High-risk patients or those with an
and Palm Beach County Fire Rescue, Coral Springs, Florida abnormal imaging finding underwent a non-contrast-enhanced computed tomography
(NCCT) as the diagnostic standard. The primary outcome was the sensitivity and
Study Objective: Nebulizer treatments for ill patients with chronic lung disease, specificity of LUS and of CXR at identifying COVID-19 pneumonia against NCCT as
reactive airways and other respiratory emergencies have been implicated in aerosolized the reference standard. Using a power analysis of 80%, our sample size calculation of
spread of highly contagious airborne viruses, including COVID-19. Considering the 98 patients was based on previous data demonstrating a 20% difference in sensitivities
increased risk of aerosolized spread of viruses within confined ambulance between LUS and CXR at diagnosing pneumonia. Data are presented as proportions
compartments, this study specifically evaluated a specially designed nebulizer mask with 95% confidence intervals (CIs). Data analysis included the chi-square and t tests.
modified with expiratory-port filters and sealing faceplates to minimize bio-aerosol Results: 143 consecutive patients with signs and symptoms of COVID-19 were
spread. approached and enrolled. 27 patients were considered low-risk by the attending per
Methods: Recognizing that fugitive aerosol emissions (such as those that would emergency department guidelines, and 6 patients were admitted for alternate
possibly carry COVID-19) typically range from 0.5 to1.5 micron (m), a six-port diagnoses without advanced imaging. 110 patients underwent LUS, CXR, and
(0.3–10m) Kanomax 3889 R particle measurement (PM) counter was placed 78 cm NCCT. 99 LUS and 73 CXRs were interpreted as positive. 81 NCCT were
from each of 15 rotating adult volunteers (non-patient, beardless) including 7 interpreted as positive providing a prevalence of COVID-19 pneumonia of 75%
women and 8 men, ages 18-59 with a mean age of 39 years. The subjects were each (95% CI 66.0-83.2) in our study population. Sensitivity of LUS was 97.6% (95%
sitting upright on a stretcher within a closed standard ambulance compartment. CI 91.6-99.7) vs 69.9% (95% CI 58.8-79.5) for CXR. Specificity was 33.3% (95%
Assigned to one of three rotating fleet ambulances, subjects used the EMS agency’s CI 16.5-54.0) for LUS and 44.4% (95% CI 25.5-64.7) for CXR. LUS positive and
usual jet-nebulizers with a conventional mask (CM) and then returned on another negative likelihood ratios were 1.46 (95% CI 1.12-1.92) and 0.0723 (95% CI 0.01-
day to receive jet-nebulization with the aerosol-controlling mask (ACM) or vice 0.31), respectively vs 1.26 (95% CI 0.87-1.81) and 0.67 (95% CI 0.39-1.16) for
versa (ACM first day, CM next day). After documenting baseline ambient PMs (PM CXR. PPV and NPV for LUS were 81.8% (95% CI 72.8-88.9) and 81.8% (95% CI
amb) within the compartment, the Kanomax operator quickly brought in a subject, 48.2-97.7) compared to 79.5% (95% CI 68.4-88.0) and 32.4% (95% CI 18.0-
closed the door, and waited 5 minutes before making a pre-nebulization PM 49.8) for CXR.
(preNeb-PM). Jet-nebulizers (using H 2 0 solutions) were then applied (either by
S10 Annals of Emergency Medicine Volume 78, no. 2s : August 2021Research Forum Abstracts – Special Edition: COVID
Conclusions: LUS was more sensitive than CXR at identifying COVID-19
pneumonia. LUS using a portable, handheld ultrasound can be a valuable triage
screening modality for patients with suspected COVID-19 pneumonia in diverse
clinical settings.
web 4C=FPO
22 Flow and Pressure Differential Results of a Novel
Low-Cost Portable Negative Pressure Patient
Enclosure For COVID-19
Moschella P, Roth B, LeMatty A, Falconer R, Mousavi ES, Nafchi A, Ashley N,
DesJardins JD/Prisma Health, Greenville, South Carolina, Clemson University,
Clemson, South Carolina
Study Objectives: To overcome the shortage of negative pressure isolation rooms
during the 2019 novel coronavirus pandemic, the novel Covering for Operations
during Viral Emergency Response (COVER) device was developed. The main goal of
the device is to generate a portable negative pressure environment using non-medical
supplies to improve patient and health care worker safety. Several variations of the
device were created and tested for their ability to generate the -2.5 pascal (Pa) pressure
recommended by the Centers for Disease Control [1].
Methods: Device Construction The device utilizes a rigid, polyvinyl chloride
(PVC)-based frame covered in a transparent plastic sheet with a connected sound-
isolated vacuum (Figure 1). Access to the patient can occur from either customizable
user-made perforations along guidelines marked on the top and sides of the transparent
sheet or from along the sheet’s bottom edge. To generate airflow and create a negative
pressure environment, the use of either two 10-inch portable fans or various vacuums
(Dyson® 1.6 hp, Shop-Vac® 2.5 hp, and Shop-Vac® 3.5 hp) were tested. These
airflow-generating fans or vacuums were attached to the device’s two HEPA filter boxes
either directly in the case of the fans or using standard 2.75-inch tubing. Airflow and
Pressure Differential Testing To assess for device efficacy, we tested the airflow
generated by the device using either the fans or the various vacuums. The airflow was
tested using a TSI-ALNOR EBT-731 (TSI Incorporated, Shoreview, Minnesota)
capture hood and reported in cubic feet per minute (cfm). A PPM3-S Abatement
Portable Differential Pressure Monitor (Abatement Technologies, Fort Erie, Canada)
was used to record pressure differentials in pascals in real time within the device using
each of the vacuums. The device’s pressure differential was measured with a simulated
patient present and with and without the maximum 60 cm of functional access cuts
made into the device.
Results: The airflow measurements are displayed in Table 1. The fans as part of the
fully constructed device did not generate any measurable airflow and were dropped
from subsequent testing. The highest measured airflow rates and pressure differentials
were observed with the 3.5 hp vacuum. All the vacuums generated an observable
negative pressure environment even with a simulated patient and 60 cm of access cuts
made into the device as shown in Table 2.
Conclusion: The COVER device uses off-the-shelf, non-medical components to
generate a negative pressure environment using a simulated patient and an aggregate of
60cm of patient care access cuts.
Volume 78, no. 2s : August 2021 Annals of Emergency Medicine S11Research Forum Abstracts – Special Edition: COVID
23 Degree, Timing and Factors Observed in COVID- vaccines, and trust in biomedical science and health care professionals. Recently,
19 Post-Vaccination Humoral Antibody citywide studies have shown the disparities of vaccine uptake among various
Development demographic groups; only 33% of Black adults have taken a vaccine dose while the rate
for Hispanic adults is 4%; 50% for white adults, and 70% for Asian adults. We believe
Pepe PE, Antevy PM, Rosenberg L, Cabral M, Scheppke KA, Jui J, Marty AM/University
the emergency department provides the opportunity to investigate and close these gaps
of Texas Health Sciences Center, Broward Sheriff’s Office and Dallas County
Emergency Medical Services, Houston, Texas, Coral Springs / Parkland, Fire
by addressing hesitancy and offering the vaccine in the emergency department.
Department, Davie Fire Rescue, Palm Beach County Fire Rescue, Coral Springs, Methods: We developed a questionnaire to evaluate patients’ and caregivers’
Florida, Coral Springs / Parkland Fire Department, Coral Springs, Florida, Memorial attitudes and knowledge of COVID-19 vaccine and investigate the reasons for the
Healthcare System and Joe DiMaggio Children’s Hospital, Florida State Department of vaccine hesitancy amongst patients in the emergency department. Adult patients and
Health, Tallahassee, Florida, Oregon Health Sciences University, Portland, Oregon, caregivers of children 0-17 years were asked to complete this survey voluntarily using a
Florida International University, Miami, Florida QR code and a link to the questionnaire.
Results: To date, 66 respondents accessed and completed the survey (34 adults and
Study Objective: The focus of this study was to document the timing of humoral 32 caregivers). Though 64% of adult patients and 81% of caregivers thought that the
antibody (IgM, IgG) development following SARS-CoV-2 mRNA vaccinations and COVID vaccine would be beneficial to their community, many were unsure or
assess factors influencing antibody (Ab) production. reported they would not take the vaccine. 56% of adult patients and 59% of caregivers
Methods: Ranging in age 23-100 years, 77 persons living or working in an assisted were hesitant to receive the vaccine for themselves and 48% of caregivers were hesitant
living facility were tested for IgG and IgM just prior to receiving their 1st dose of the to give the COVID-19 vaccine to their children. The most commonly cited reasons
Pfizer-BioNTech mRNA vaccine on 01/17/2021. Re-retesting occurred on Day 14, being concern about safety of the vaccine and its side effects and poor understanding of
Day 21 (before dose 2), Day 28 and Day 42 (7 days and 21 days after dose 2). Medical the vaccine. 90% of the adult patients and 83% of caregivers stated they would take the
histories, including underlying conditions and medications, were collected vaccine for themselves in the emergency department if offered, and 85% of caregivers
confidentially. Testing involved point-of-care lateral flow chromatography devices would consider giving it to their children. Many respondents belonged to communities
(under emergency use authorization as reported in our previous research on PCR+, of color (Black 16-36%, Hispanic 73-82%), where vaccine uptake was the least.
humoral Ab- persons) using fingerstick samples. The lateral flow assay antigens Conclusion: The emergency department can address patients’ vaccine hesitancy
included a recombinant nucleocapsid protein and a spike protein (S1) conjugated with and alleviate the disparities by making vaccines available in the emergency department.
colloid gold. Readings were recorded 15 min. after obtaining blood samples.
Results: On the day of dose 1, one person had a faint IgM reading (and a known past
history of COVID-19) and 3 others demonstrating detectable Ab were asymptomatic and had
no known prior illness. None of these four persons were PCR + at the time of assay and their
25 Correlations Between Community COVID-19
Prevalence, Vaccine Availability and Emergency
Department Non-COVID-19 Utilization
Ab profiles all further evolved following vaccination. Consistent with the original Pfizer clinical
Gopalsami A, Torbati S/Cedars-Sinai Medical Center, Los Angeles, California
trial, on Day 14, 27 (69%) of the 39 persons 70 had no detectable Ab.
Study Obectives: The coronavirus disease 2019 pandemic has resulted in decreased
However, by Day 21, just prior to receiving the second dose of vaccine, 100% of persons 90 yo, 80% tested Ab negative). Seven days after the second dose, however, 100% of
Methods: This was a retrospective cross-sectional study performed at a single urban
personsResearch Forum Abstracts – Special Edition: COVID
Conclusions: The higher the prevalence of COVID-19 in the community, the Conclusion: The ED often serves vulnerable patient populations. As such, its role
more hesitant patients behaved in seeking ED care for non-COVID-19 reasons. Lower in public health in these communities cannot be underestimated. This pilot quality
disease prevalence and increasing vaccination rates correlate with a return of NC improvement project is a novel method that hospital systems can use to develop and
volumes back to pre-pandemic levels. implement public health education programs to address specific community needs
through the ED. These results show that ED health care providers have the ability to
provide measurable change in attitudes about vaccine safety.
EMF
27 Social Determinants of Health and
COVID-19 Infection in North Carolina:
A Geospatial Analysis
Purakal JD, Silva L, Tupetz A, Seidenfeld J, Limkakeng A, Staton C, Vissoci J/Duke
University School of Medicine, Durham, North Carolina, State University of Maringá,
Duke University School of Medicine, Duke University School of Medicine, Duke
University School of Medicine, Duke University School of Medicine, Duke University
School of Medicine
Study Objectives: The COVID-19 pandemic has demonstrated that social
web 4C=FPO
determinants of health (SDOH) are profoundly linked to the spread and outcomes of
COVID-19. However, the relationships between these SDOH and COVID-19 spatial
outbreaks have yet to be determined. We conducted spatial analyses with geographic
information systems (GIS) mapping of county-level SDOH and regional COVID-19
infection outbreaks to demonstrate the most impactful SDOH and to provide a
pragmatic visual guide to prevent future outbreaks.
Methods: We analyzed the geospatial associations of COVID-19 infections and
SDOH to identify areas of overlap. Our sample comprised all patients in a North Carolina
26
health care system’s registry who tested positive for COVID-19 from March 2020-
Implementation of a COVID-19 Vaccine February 2021. Patients’ addresses were geo-referenced and analyzed by Kernel Density
Emergency Department Education Program for Estimation (KDE) to identify population-dense outbreaks of COVID-19 (hotspots). A set
Underserved Communities: A Pilot Quality of 12 SDOH variables for each county were collected from the American Community
Improvement Project Survey (ACS-5) and the Economic Research Service. Principal Component Analysis was
Bischof JJ, Schoeffler A, Bashian E, Callender N, Fuentes A, Geyer E, More A, Webb T, applied to SDOH variables in order to reduce dimensions down to 3 geographical SDOH
Kman K/The Ohio State Wexner Medical Center, Columbus, Ohio, The Ohio State categories: Protective SDOH, High-Risk SDOH and Increased Vulnerability for Infection
University College of Medicine, The Ohio State University College of Medicine, The (Table 1). Using Multivariate Clustering Analysis (MCA), three clusters of census tracts
Ohio State University College of Medicine, The Ohio State University College of were categorized according to SDOH indicators: decreased social disparities (DSD),
Medicine, The Ohio State University College of Medicine, The Ohio State University equivocal social disparities (ESD) and increased social disparities (ISD) (Image A). Kruskal-
College of Medicine, The Ohio State University College of Medicine, The Ohio State Wallis and Dunn’s Post-Hoc adjusted with Bonferroni were utilized to verify any difference
University Wexner Medical Center in the proportion of patients residing in the different clusters (significance pYou can also read