Sexually Transmitted Infections (STIs) - FAMILY CARE CENTER a medical clinic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sexually Transmitted
Infections (STIs)
Jordan Crawford, PA-C, DIMPH
Family Medicine Physician Assistant
Hope Family Care Center
FAMILY CARE CENTER
a medical clinic
Disclosures • I have no relevant financial interests or relationships to disclose.
About the Speaker • Jordan Crawford, PA-C, DIMPH • In full-time family practice in Kansas City’s east-side at Hope Family Care Center for the last 3 years • Graduate of the University of Kansas (Rock Chalk!), UMKC School of Medicine PA Program (Go Roos!) • Graduate of INMED’s Diploma of International Medicine & Public Health (DIMPH) program

Objectives • Describe the clinical presentation, epidemiology and management of the most common sexually transmitted infections • Recognize the current state of affairs relating to disease burden and public health concerns • Explore the broader implications of STIs **Note, this is a clinical topic with some sensitive images depicting genitourinary anatomy.
Terminology
• STD vs STI
• Sexually transmitted disease (STD): a sexual disease state that is a result of an infection
which may or may not be curable. Moving more away from this terminology, though it
is still accepted and widely used.
• Sexually transmitted infection (STI): refers to an organism acquired via sexual contact.
This is a broader term that is thought to carry less stigma. This implies there may or
may not be active symptomatology in the patient in which they can unknowingly
transmit a bacteria or virus.
Major Viruses Bacteria and Parasitic
HIV/AIDS Human Papillomavirus Chlamydia
Herpes Gonorrhea
Hepatitis Trichomoniasis
SyphilisTransmission
• Blood • Unprotected sex
• Oral
• Semen
• Vaginal
• Vaginal secretions
• Anal
• Infected skin (or lesions)
• Direct skin-to-skin
• Breast milk
• Mother to child• Major public health crisis that is still increasing in incidence, short and long-term health effects, cost burden • On any given day in 2018, 1 in 5 people had an STI
Chlamydia
• Large group of obligate intracellular parasites
§ C. trachomatis (trachoma, inclusion conjunctivitis, pneumonia, and genital infections)
§ The most common bacterial STI
• Incubation period from infection to symptoms: 5 to 14 days
• MANY males and females (perhaps ~40-50%) remain asymptomatic
• Need screening if risk factors or performing routine screening measures (Physical, Well
Woman, Pap)
• Prevalence:
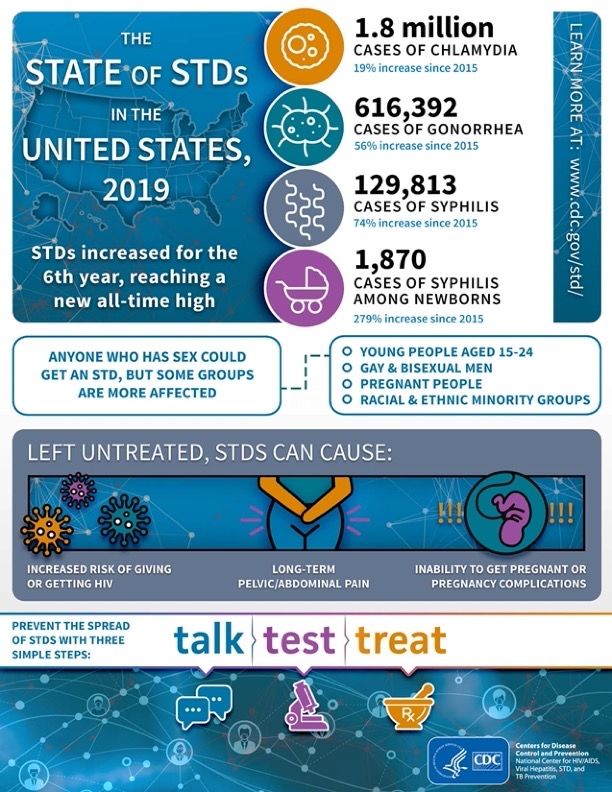
• 1,808,703 cases in 2019; two-thirds of all cases in 15-24 age range; increased across all races,
both men and women and across all regions of the United States
• Missouri (21st) 34,416 total cases in 2019; 561.8 rate per 100,000
• Kansas (25th) 15,286 total cases in 2019; 525.0 rate per 100,000• Signs and Symptoms:
• Urethritis
§ Most common cause of non-gonococcal urethritis
• Cervicitis
• Dysuria, urinary frequency (r/o UTI) , discharge, abdominal/pelvic pain (PID)
• Signs of systemic illness, cervical motion tenderness indicate ascending infection as in Pelvic
Inflammatory Disease
• Complications:
• Lymphogranuloma venereum—ulcerative or vesicular lesion involving
the lymph nodes that can cause buboes and sinus tracts/fistulize
• Oropharyngeal infection (oral sex)
• Conjunctivitis/trachoma
• Pelvic Inflammatory Disease (risk of ectopic)
• Reactive Arthritis (9:1 M to F)• Diagnosis
• Clinical
• Gram stain is negative
• Nucleic Acid Amplification Test (NAAT) is test of choice; Compliment fixation test, ELISA or DNA
probe to confirm (urine or swab)
• Treatment
• Azithromycin 1g in single oral dose
• Doxcycyline 100mg twice daily for 7 days
• Erythromycin is drug of choice in pregnancy (doxy is teratogenic)
• Treat all partners and report!
• Co-infection with GC is common
• Screening
• Pregnant women, sexually active women ages 15-24 (highest risk), women 25+ with risk factors
• Men with risk factors, Men who have sex with men, HIV+Gonorrhea
• Neisseria gonorrhea - gram negative intracellular diplococci
• Highest incidence is 15-29 years of age
• Incubation period is ~2-8 days
• Women continue to have high rates of asymptomatic infection
• Prevalence:
• 616,392 total cases in 2019; like chlamydia, has increased across all races, both men and women
and all regions of the United States
• Missouri (7th) 15,585 total cases in 2019; 254.4 rate per 100,000
• Kansas (25th) 4,948 total cases in 2019; 169.9 rate per 100,000• Signs and Symptoms:
• Urethritis
§ Copious purulent drainage (more obvious in men)
• Cervicitis
• Dysuria, urinary frequency (r/o UTI) , discharge, abdominal/pelvic pain (PID), bleeding after
intercourse
• Complications:
• Conjunctivitis in newborn and adults
• Oropharyngeal infection
• Chronic infection – dissemination, chronic pelvic pain
• Pelvic Inflammatory Disease (risk of ectopic) in females
• Urethritis, epididymitis, prostatitis in males
• Septic Arthritis
• Infertility• Diagnosis • Nucleic acid amplification test (NAAT) is most sensitive and specific (widely used) • Urine specimen – first catch AM (later collections decrease sensitivity by 10%) • Oropharyngeal and rectal site use • Gram Stain – shows gram negative diplococci • Treatment • Ceftriaxone 500mg once IM – this is a new treatment update as of December 2020 • Consider co-treatment for chlamydia with Azithromycin or Doxycycline • Treat all partners and report! • Screening • Pregnant women, sexually active women ages 15-24 (highest risk), women 25+ with risk factors • Men with risk factors, Men who have sex with men, HIV+
Syphilis
• Treponema pallidum is a spirochete that can affect almost any organ or tissue
• Occurs in stages (Primary, Secondary, Latent, Tertiary)
• Increased incidence in urban areas among adolescents and young adults, and injection users
• Prevalence:
• 129,813 of all stages of syphilis in 2019
• Primary and Secondary Syphilis: Missouri (14th) 817 cases in 2019; 13.3 rate per
100,00
• Kansas(35th) 190 cases in 2019; 6.5 rate per 100,000
• Congenital Syphilis: 1,870 total cases in 2019; Missouri (17th) 18 cases, Kansas
(18th) 9 cases in 2019• Signs and Symptoms:
• Painless chancre develops between 10-90 days after exposure
• Generally resolves in 3 – 6 weeks. Bacteria continue to multiply after this time
without symptoms
• +/- painless lymphadenopathy
• At risk groups:
• Women of childbearing age, sexually active teens
• Drug users, Inmates of penal institutions
• Individuals with multiple sexual partners
• Persons who have sex with sex workers
• MSM Infants with infected mothers (congenital: transplacental transmission)• Primary syphilis: exposure to infected tissue or secretion à chancre that is indurated, painless, raised
border
• Resolves without treatment in 3-6 weeks
• Secondary syphilis: following the healing of the chancre, the secondary stage begins
• Typically with the development of a maculopapular rash; sometimes pruritic but usually not
• Described as ‘rough’, red to brown in color; can involve mucous membranes as well as palms of hands
and soles of feet is common
• Tertiary syphilis: Early Latent Stage – this is a serologic evidence without any clinical evidence that may
last 10-20 years
• Late Latent Stage (Tertiary) – reactivation of the latent stage but now with clinical manifestations
• Dermatologic: Gumma (mushy and gummy)
• Cardiovascular: aneurysm, regurgitation, dilation of aorta
• Neurologic: psychosis, dementia, paresthesias, abnormal reflexes
• Approximately 25-40% of untreated patients may progress to tertiary disease (up to 30 years later)• Diagnosis: • VDRL and rapid plasma reagin (RPR) • Enzyme immunoassay (EIA) • Darkfield microscopy, CSF fluid analysis (tertiary) • USPSTF recommend screening for all HIV+, MSM • Treatment: • Benzathine penicillin G 2.4 million units IM in a single dose • Doxycycline 100mg orally twice daily x 14 days • Tetracycline 500mg orally four times daily for 28 days • Ceftriaxone 1 g IM once a day for 8-10 days • High dose Benzathine Pen G at late stages and for neurosyphilis which +/- be efficacious • Treat all partners and report!
Trichomoniasis
• Unicellular Protozoan with flagella, Trichomonas vaginalis
• Typically are not reported infections so incidence is not precisely known in the US
• Thought to be most common nonviral STI worldwide.
• Signs and Symptoms:
• Urethritis in men, vaginitis in women
• Can live in vagina for long periods
o May be asymptomatic, particularly men (up to three quarters)
o Women: yellow-green frothy, malodorous thin discharge, strawberry cervix on exam,
vulvar/vaginal erythema, postcoital bleeding, dyspareunia, pruritis• Complications:
• Premature rupture of the membranes (PROM), preterm delivery, low birth weight in
pregnant women
• Urethritis, cystitis, infertility
• Diagnosis:
• Nucleic acid amplification testing (NAAT)
• Wet mount may yield the ‘motile trichomonads’
• Treatment:
• Metronidazole 2g once orally or Tinidazole 2g once – generally has side effects
• Metronidazole 500mg twice daily for 7 days – better cure rates (compliance issues)
• Treat both partners and abstain from intercourse for about 1 week.
• Note: Metronidazole use, must counsel on di-sulfiram reaction and to abstain from alcohol for 1-3 days after
treatment (nausea, vomiting, headache, etc.)Herpes Simplex Virus (HSV)
• Herpes Simple Virus - Type 1 (not STI)
• 85% of the US population has evidence of infection with HSV type 1 (infected saliva)
• Recurrent, self-limited attacks are common (stress, surgery, fever, viral infections may be trigger)
• Herpes Simplex Virus - Type 2 (STI)
• 25% of US population is infected (sexual contact or at birth)
• Asymptomatic shedding and painful eruptions can occur
• Remains dormant in dorsal root ganglia then reactivates with stress
• HSV 1 – trigeminal; HSV 2 - sacral root ganglia• Transmission:
• Oral, anal, vaginal sex or infected skin to skin contact AND/OR contact with lesions,
mucosal surfaces, genital secretions, or oral secretions.
• Can shed from skin that looks normal
• Believed up to 81% of individuals are unaware of their condition
• 1 million annual new infections
• About 45% ages 15 to 24 years
• 25 million total infections
• About 1 in 6 people aged 14 to 49 have genital herpes
• Cold sore: usually HSV-1; genital lesion: usually HSV-2• Signs and Symptoms:
• 1 or more grouped vesicles on erythematous base appear on genitals, rectum or mouth, break and leave painful ulcers that
crust over and may take 2-4 weeks to heal – burning, stinging, itching
• Prodromal symptoms before recurrences: tingling, itching, sensitivity
• May have systemic symptoms of headache, myalgias, fever, malaise, lymphadenopathy
• 90% of HSV-2 reactivates within 1 year
• Complications:
• Meningitis, Encephalitis, Blindness/Keratitis, Skin infections (pyoderma, herpetic whitlow)
• Mother to child transmission – higher rate of complication to infant
• Diagnosis:
• Clinical
• Tzanck smear done on vesicular fluid may show multinucleated giant cells
• Serologic testing has notorious false-positives, yet commonly used; swab and send for viral culture
• Screening with antibody testing is NOT recommended due to false-positive rate and low specificity
• Treatment:
• Self-limited in orolabial lesions; may use Abreva
• Acyclovir 800mg three times daily for 2-3 days for episodic
• Valacyclovir 500mg two times daily for 3 days for episodicHuman Papillomavirus (HPV)
• Genital HPV – is the most common sexually transmitted infection
• Virus with double-stranded DNA
• More than 77 types (by DNA); ~40 causing genital warts
• Types 6 and 11 are associated with genital condyloma, types 16 and 18 are most
carcinogenic
• When vulvar lesions are present, the entire lower tract is usually involved
• Genital contact most often during vaginal and anal sex, but also oral sex
• Even when infected partner is without symptoms• Most people are unaware they are infected
• ~ 20 million Americans are currently infected; 6 million new infections each year
• Each year ~ 12,000 women get cervical cancer and most are associated with HPV; less
common, penile cancers
• Most people do not develop symptoms – 90% of patient’s own immune system clears ~ 2
years
• Signs and Symptoms:
• ‘Cauliflower-like’ verrucous lesion – condyloma accuminata
• Most are asymptomatic
• May be flat, pedunculated or papular
• Not confined to genitals but also throat, pharynx
• Diagnosis:
• Clinical
• Histologic following biopsy, scrape, or excision
• Pap testing• Treatment: • Typical warts will spontaneously remit (over years) • Cryotherapy, laser excision, blunt dissection • Trichloroacetic acid (TCA) • Commonly recur • Patient applied: podofilox, imiquimod • Vaccine: • Gardasil 9 approved for females and males from age 9 to 45 • 2 or 3 dose vaccine depending on age of initiation
On the Rise
• “The current rise of STIs is a serious public health concern that requires
immediate attention. If left untreated, STIs can lead to severe health
complications, including pelvic inflammatory disease (PID), increased risk of
getting HIV, certain cancers, and even infertility.”
• Statement from the US Department of Health and Human Services on STIs in March
2021Advocacy and Intervention
• Using clear and concise language to get to the point
• Addressing known risks without merely alluding to hypotheticals
• Numbers don’t lie and the statistics are alarming
• They are VERY preventable
• Love them enough to tell them the truth
• A + B = C (hint: the C stands for child)
• The answer does not lie in testing and treatment…this is also centrally behavioral
• Proverbs 10:18 “The one who conceals hatred has lying lips...”• Avoiding language and tone that expresses shame and guilt
• “There’s no love in the blame game.”
• Be a cheerleader, not a buzzkill
• People long for relationships with safety, security and NOT ones where they don’t know where they
stand or fear the partner’s infidelity
• Point to an ideal — there is a better way
• John 10:10 “The thief comes only to steal and kill and destroy. I came that they may have life and have
it abundantly.”
• Give them options
• Monogamy
• Abstinence
• ProtectionQuestions?
References
• UpToDate sections on Chlamydia, Gonorrhea, Syphilis, Trichomoniasis,
HPV, HIV, HSV
• Center for Disease Control – STI/STDs
• MMWR update on Treatment Guidelines
• Current Medical Diagnosis & Treatment
• HHS statement on STIs, HHS.govYou can also read