Strategic Framework 2015-2019 - SDC Global Programme Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Strategic Framework 2015–2019 SDC Global Programme Health


Introduction
Countries worldwide are increasingly facing global ment in health at a bilateral and global level. Hence,
risks that threaten their development prospects. the global dimension of the SDC’s engagement in
Poor populations in low and middle-income coun- health is not a recent development but has, in fact,
tries are particularly vulnerable to these risks al- been strengthened through the establishment of
though they have hardly contributed to creating the GPH.
them. Traditional modalities of international coop-
eration such as bilateral and multilateral instruments The strategic framework defines the Programme’s
are no longer sufficient for dealing with global chal- goals and mission as well as its core components
lenges that transcend national borders. For this rea- and working modalities. It also informs resource al-
son, the SDC was mandated through the Federal location and monitoring as well as reporting and
Council’s 2013-16 dispatch to parliament to set up communication.
programmes to address major global development
challenges. These programmes are considered com- Consequently, the target audiences of the present
plementary to bilateral and multilateral assistance. strategic document are bilateral and global SDC
Since then, five programmes have been established, programmes with health components, Swiss federal
each addressing one major global development risk: departments and agencies implementing the Swiss
climate change, water, migration, food security and Health Foreign Policy, Swiss non-state actors active
health. The aim is to reduce poverty and social in- in international health cooperation as well as global
equalities in low and lower middle-income countries health players such as international NGOs, multilat-
by strengthening their capacities to cope with these eral, philanthropic or private sector organisations.
global development challenges and by promoting
an enabling environment at the global policy level. This strategic framework is the product of an it-
erative process and of broad consultation with the
This medium-term framework provides strategic aforementioned parties, to whom the Global Health
direction for the Global Programme Health (GPH) Team owes a debt of gratitude for their valuable
and builds on the SDC’s long-standing engage- comments and suggestions.
3
4

Table of Contents
Introduction 3
1. Global health challenges at a glance 6
2. Switzerland’s and the SDC’s response to global health challenges 8
3. Programme goals and mission 10
4. Programme components 12
4.1 Component 1: Reducing the burden of communicable diseases through innovative
research and development of medical resources 14
4.1.1 Sub area 1: Improving access to medical resources for neglected tropical diseases 15
4.1.2 Sub-area 2: Accelerating malaria elimination 16
4.2 Component 2: Advancing universal health coverage through sustainable health financing
and targeted health systems strengthening 17
4.3 Component 3: Promoting sexual and reproductive health and rights of young people
through an enabling policy environment 18
4.4 Component 4: Addressing determinants of health through multisectoral collaboration 19
4.5 Component 5: Strengthening global health governance through efficient coordination
between multilateral organisations 20
5. Working modalities 21
6. Human resources, budget, M&E and communication 23
7. Appendices 21
Appendix 1: References 24
Appendix 2: List of acronyms 24
Appendix 3: SDC Health Policy 25
Appendix 4: The 20 objectives of the Swiss Health Foreign Policy 25
Appendix 5: Monitoring matrix of the Global Programme Health –
example from one priority area 26
Appendix 6: Results framework for each programme component 27
1. Global health challenges at a glance
Worldwide, countries and people are becoming in- •• Globally, an estimated 1.8 to 3 billion people still
creasingly interdependent due to diverse globalisa- have no access to sustainable safe drinking
tion processes. Events in one part of the world can water, causing a high number of deaths due to
spread rapidly across the globe. This is most obvious water-borne diseases.
with health issues that transcend national borders. •• 1 billion disabled people worldwide, 80% of
The most recent examples are the resurgence of po- them living in low and middle-income countries,
lio, the spread of antimicrobial resistance and the remain neglected.
Ebola outbreak. •• Every year, 100 million people are pushed into po-
verty due to out-of-pocket payments necessi-
A first attempt to respond to these increasingly tated by ill health.
“global” challenges was the formulation of the Mil-
lennium Development Goals (MDGs). The MDGs
mobilized resources in an unprecedented manner, Several shortcomings in the MDG framework
especially for health. This boost resulted in consid- have contributed to the failure in meeting some
erable progress in improving the health status of MDG targets:
many people in low and middle-income countries.
For instance, •• The MDGs’ focus on specific diseases and popu-
lation groups resulted in vertical strategies and
•• global child mortality dropped from 12.6 to 6.6 eventually in a fragmentation of the health
million deaths annually, system, with emphasis on services specifically for
•• 3.3 million deaths due to malaria were averted malaria, TB and HIV/AIDS as well as for child and
worldwide (2000-2012), maternal health.
•• maternal mortality globally was reduced by •• A comprehensive approach to health systems
45% (1990-2013), strengthening, including social health protec-
•• TB-related mortality decreased by 41% bet- tion, quality management of health services and
ween 1990 and 2010.1 social accountability mechanisms was neglected.
•• The MDGs were directed only towards low
and lower middle-income countries.
Despite this progress in health-related issues, which
to a large extent is the result of substantial external
support, major challenges remain: In the post-2015 era these shortcomings need to be
addressed, new health issues tackled and alter-
•• In many countries maternal mortality rates con- native approaches applied. Following an improve-
tinue to be high. Among young women, birth and ment in economic and social standards of living for
pregnancy-related complications are the second at least parts of the population in many middle but
leading cause of death.2 also low-income countries, the coming decades will
•• Social inequalities related to gender, age, disa- be marked by a massive demographic transition:
bility or geographical location are becoming even
more pronounced, especially in middle-income •• The world’s population is not only growing, but
countries that today have the highest number of also ageing.
poor people. •• Changing lifestyle patterns and an altered diet
•• The only age group showing a rise in the number foster the spread of non-communicable disea-
of AIDS-related deaths is that of 10-19 year-olds.3 ses (NCDs), e.g. cardiovascular diseases, cancer
•• 200 million cases of malaria and 600,000 deaths and diabetes.
still occur every year.4
•• Neglected tropical diseases affect more than 1
billion people worldwide. Moreover,
•• Increasing mobility is leading to a growing num-
ber of accidents and injuries.
1 United Nations 2014 •• Climate change as well as water, air and soil
2 UNFPA 2014
3 UNAIDS GAP Report 2014 pollution due to industrialization entail global
4 WHO 2014 health risks.
6
•• Violence (through war-like conflicts, crime and The broadly defined health-related Sustainable
domestic violence) is widespread, especially due Development Goal (SDG) – “ensure healthy lives
to the increasing number of fragile contexts. In and promote well-being for all at all ages” – and its
turn, violence produces trauma and impairs men- targets will address most remaining and new health
tal health. challenges. In order to achieve this ambitious set of
•• The growing number of fragile contexts as well goals, it is critical to mobilize additional funding
as the control of pandemics will increasingly re- as well as allocate and use resources more cost-
quire a global response that combines effective effectively.
emergency responses and more long-term invest-
ments to build resilient health systems. “New” global players – emerging economies,
philanthropic organisations, private companies
and social businesses – that have emerged during
Health systems strengthening will also be key the MDG era must assume more shared respon-
to managing the dual disease burden, i.e. commu- sibility on global health. The increasing number of
nicable and non-communicable diseases, as well global health challenges and actors necessitate a
as complex combinations of different conditions in further strengthening of global health govern-
one patient. A qualified and motivated health work- ance structures to develop, effectively implement
force is the backbone of solid health systems. Yet, and coordinate globally agreed responses.
competition for qualified healthcare personnel
has become a global phenomenon and the “brain These different players will need to form multi-
drain” of health workers, especially from low and stakeholder coalitions to address increasing
middle-income to high income countries needs to complexity and to implement the broad post-2015
be curbed. agenda. The role of non-state actors (private sec-
tor, NGOs and philanthropic organisations) in global
Moreover, a strategic shift away from purely a health governance and with regard to new partner-
disease focus to a broader conceptualization ship models has to be more clearly defined in terms
of health to include its determinants such as in- of consultative versus proper membership status,
come, education or gender is crucial. Such a com- selection of representatives etc.
prehensive approach to address health issues re-
quires intersectoral collaboration or what is called
the “health in all policies” approach.
7
2. Switzerland’s and the SDC’s
response to global health challenges
In light of this changing context, Switzerland needs •• A constitutional mandate and correspon-
to redefine its role in global health. Accordingly, ding laws on international cooperation (1976,
the country has sought to develop a coherent set of 2006) as well as dispatches to parliament (2013-
policies that guide its responses to the global health 2016, 2017-2020) that stipulate a commitment to
challenges and health related-SDG agenda outlined addressing global development risks;5
above. By doing so it hopes to make relevant contri- •• Switzerland’s Foreign Policy Strategy (2012-
butions to effective and sustainable solutions. The 2015 and beyond);6
medium-term strategic direction of the GPH for •• the SDC‘s Health Policy7 and
the period 2015-2019 is defined by: •• the Swiss Health Foreign Policy.8
5 Schweizerische Eidgenossenschaft (2013)
6 Eidgenössisches Departement für auswärtige
Angelegenheiten (2012)
7 Federal Department of Foreign Affairs and Federal
Department of Home Affairs (2012)
8 Swiss Agency for Development and Cooperation (2013a)
SDC GLOBAL PROGRAMME HEALTH
EXISTING POST-2015 AND SDC HEALTH POLICY SWISS NEW
SUSTAINABLE
GLOBAL HEALTH DEVELOPMENT Improve populations’ HEALTH GLOBAL HEALTH
CHALLENGES GOALS health through: FOREIGN CHALLENGES
`` Health systems
e.g.
`` Maternal &
strengthening POLICY e.g.
`` Ageing societies
`` Reduction of communicable
newborn mortality `` Non-communicable
and non-communicable
`` Tropical diseases diseases
diseases
`` Social inequalities SWISS KNOW-HOW, SWISS FOREIGN `` Health determinants
`` Maternal, newborn & child,
`` Weak health `` Pandemics
RESOURCES AND sexual & reproductive health POLICY STRATEGY
systems `` Sustainable
PARTNERS funding
DISPATCH TO PARLIAMENT ON INTERNATIONAL COOPERATION (2013–2016; 2017–2020)
MANDATE OF SDC: REDUCE POVERTY AND SOCIAL INEQUALITIES
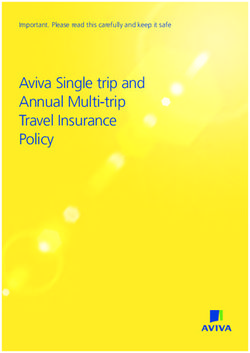
Figure 1: Swiss policies and
SWISS LAWS ON COOPERATION WITH DEVELOPING AND TRANSITION COUNTRIES (1976, 2006) frameworks guiding the
Global Programme Health
8
Under the two laws on international cooperation, Both policies and their respective objectives
the SDC’s mandate is to reduce poverty and so- build on Switzerland’s comparative advantages
cial inequalities. The SDC thus aims to contribute in the health sector. The country hosts some of the
to greater equity worldwide and to the gradual ful- world’s leading clinical and public health research
filment of human rights for all, including the right entities (University Hospitals of Geneva and Laus-
to health. anne, Swiss Tropical and Public Health Institute etc.),
research-based pharmaceutical and biotech compa-
The SDC’s Health Policy (see appendix 3) is nies (e.g. Roche, Novartis, Actelion) as well as major
aligned with the Swiss Health Foreign Policy non-governmental organisations active in health
(SHFP), which stipulates 20 objectives (see appen- (International Committee of the Red Cross, Doctors
dix 4 for the complete list of policy objectives). The Without Borders, the Global Fund, the Global Alli-
SHFP addresses all of the country’s international ance for Vaccination and Immunization, Medicines
concerns related to health. The rationale for such a for Malaria Venture, Drugs for Neglected Diseases
policy is to make Swiss health policy more coherent initiative etc.). Moreover, it has a long list of private
and effective, thereby safeguarding Swiss health-re- health insurance schemes as well as re-insurance
lated and economic interests in a globalised world, companies such as Swiss Re. Last but not least, Swit-
improving its contributions to global health and zerland is home to the World Health Organization.
ultimately strengthening its reputation as a cred-
ible and reliable partner. Hence the SHFP promotes
inter-departmental strategic alignment and regular
consultations. An example of such a coordinated ap-
proach is the coherent support across departments
to consolidate Geneva’s position as global health
capital. Switzerland was one of the first countries
worldwide to adopt an interministerial agreement
on health foreign policy objectives9.
9 Norwegian Ministry of Foreign Affairs (2012); Bundesministeri-
um für Gesundheit der Bundesrepublik Deutschland (2013)
9
3. Programme goals and mission
The overall goal of the SDC’s Global Programme Specifically, the SDC aims to foster initiatives that
Health is to improve the health status of poor develop innovative solutions for the health needs
and vulnerable people in low and lower middle- of vulnerable and poor people in low and lower
income countries by addressing specific global middle-income countries without adopting any spe-
health risks. This is done by engaging in policy cific geographical focus. Through both avenues
dialogue as well as by supporting global ini- – policy work and programme support – the
tiatives within the core components. By global Programme strives to fulfil its mission, namely
initiatives we mean operational activities of a group to influence agenda setting and shape policy
of partners that go beyond policy work and also formulation at the global level and to advocate
include technical advice and support, advocacy, re- the Swiss perspective.
search or product/service provision for the benefit of
several low and middle-income countries.
10The Global Programme Health complements SDC- The selection of Programme components and re-
supported bilateral programmes by: lated priorities is based on the following crite-
ria:
•• engaging with health risks and challenges that re-
quire action at a global policy level, •• A global response is required.
•• supporting innovative initiatives and partnerships •• Innovative partnerships with existing or new part-
that are organized at a global level and benefit a ners can be built, especially in the context of “In-
larger number of low and lower middle-income ternational Geneva”.
countries, •• The SDC’s Health Policy goals and the objectives
•• drawing on experiences and results from SDC of the Swiss Health Foreign Policy are advanced.
country programmes to nurture global policy •• The SDC exhibits a comparative advantage
work. In turn, the latter informs SDC’s national through its humanitarian, bilateral or multilateral
policy dialogue and programme work in partner programmes and/or it can leverage Swiss know-
countries. how in order to make a significant difference.
•• Relevance for at least two geographical regions
where the SDC maintains programmes in health.
As a relatively small donor agency, the SDC re-
lies on strategic partnerships with other donors,
international NGOs, the private sector and multilat-
eral agencies for influencing policy and provid-
ing effective support to initiatives at the global
level. By strategic partners we mean organisations
with resources – financial, technical, political or oth-
er – that are critical for creating meaningful impact.
`` Information about the latest
developments in the global
health debate
`` Provision of technical
support/products
SDC GLOBAL SDC BILATERAL
PROGRAMME HEALTH PROGRAMMES
`` Influence global agenda setting with health components
and shape policy formulation
`` Support global initiatives
and partnerships
Use of evidence from
country-specific policy and
programme work:
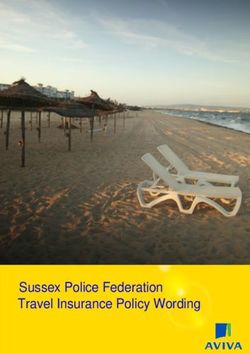
Figure 2:
Goals and mission of the `` Results
Global Programme Health `` Operational experiences
`` Lessons learnt
114. Programme components
The Global Programme Health focuses on five core While components 1, 2, 3 and 5 seek to strengthen
components: health systems, component 4 addresses determi-
nants of people’s health. Only by addressing both
Addressing communicable diseases through
1. aspects, i.e. the determinants of health and health
research and development of medical resources systems, can poor people’s health be improved and
poverty reduced (see Figure 3).
2. Advancing universal health coverage through
health financing and health systems strengthen- Under the component “determinants of health”,
ing the GPH will concentrate on global challenges to be
addressed through multisectoral approaches, espe-
Promoting the sexual and reproductive
3. cially on nutrition and water. The other components
health and rights of young people through an focus on strengthening primarily four of the six
enabling policy environment. building blocks of health systems: service delivery,
medical products, health financing and leadership/
4. Addressing determinants of health through governance.
multisectoral collaboration
Strengthening global health governance
5.
through efficient coordination between multilat-
eral organisations.
12Cross-cutting approaches comprise both health Moreover, each of the five components matches
systems strengthening as well as multisectoral one or several objectives of the SDC Health Policy
initiatives to address determinants of health and the Swiss Health Foreign Policy respectively (see
outside of health systems. The focus is on vulner- appendices 3 and 4). Malaria, neglected tropical
able groups, i.e. people who are more likely to be diseases, R&D for diseases that primarily affect
exposed to major health risks. These include preg- low and middle-income countries, universal
nant women, children, young people, disabled health coverage as well as sexual and repro-
persons and the elderly. ductive health are all explicit targets under the
health-related SDG 3. “Global health governance”
The different components are linked both conceptu- corresponds to SDG 17 on global partnership for
ally and operationally. Many activities at the poli- sustainable development. “Determinants of health”
cy level as well as at the level of the supported are incorporated in basically all SDGs.
initiatives address more than one component.
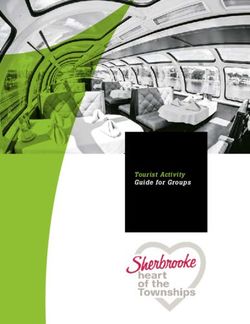
Figure 3:
Core components of the
Global Programme Health
1 COMMUNICABLE
DISEASES 2 UNIVERSAL
HEALTH COVERAGE
SDC GOALS:
DETERMINANTS REDUCE POVERTY AND HEALTH
OF HEALTH AND PEOPLE’S SOCIAL INEQUALITIES SYSTEMS
LIVELIHOODS
IMPROVE POOR AND VULNERABLE
PEOPLE’S HEALTH
4 NUTRITION,
WATER, CLIMATE,
MIGRATION, EDUCATION
3 SEXUAL AND
REPRODUCTIVE
HEALTH AND RIGHTS
5 GLOBAL HEALTH
GOVERNANCE
etc. OF YOUNG PEOPLE
GLOBAL HEALTH POLICIES, PARTNERSHIPS AND INITIATIVES
134.1 Component 1: Reducing the burden of communicable diseases through innovative research and development of medical resources The Programme’s engagement in reducing the bur- for new products is the greatest. Without sufficient den of communicable diseases and especially ma- investment in R&D for these diseases, achieving laria is the logical continuation of a long-standing the SDGs may prove to be difficult. For most non- commitment at the bilateral and global level through communicable diseases, products are globally avail- which the SDC has built a track record and reputa- able. However, product pricing and the provision of tion. Reducing communicable diseases enhances health services for these diseases are critical. Ad- health gains for the affected people and fosters dressing gaps in research and development (R&D) of socio-economic development in low and middle- medical resources is a good entry point for a global income countries. It also frees resources for health programme as this field is organized globally and fo- systems, for instance to deal with the rising burden cuses on patients who are spread across the world. of non-communicable diseases. This component focuses on research and development of medical This component is divided into two sub areas since resources for communicable diseases of the poor the policy and intervention strategies for neglected and access to them because this is where the need tropical diseases differ from those for malaria. 14
4.1.1 Sub area 1:
Improving access to medical resources
for neglected tropical diseases
Neglected tropical diseases (NTDs) are a group of •• Advance demonstration health R&D initiati-
chronic and disabling infections affecting more than ves and related policy formulation for the es-
1 billion people. No efficacious medicines are availa- tablishment of a global voluntary health R&D
ble for many of these diseases, or they are toxic and financing mechanism
difficult to administer. Because neglected tropical •• Accelerate pre-qualification listing by WHO
diseases mainly affect the world’s poorest people, and subsequent country registration of glo-
commercial markets that traditionally drive phar- bal health/medical products that address ne-
maceutical company investment in new product re- glected tropical diseases.
search and development are lacking. Market failure
is even more apparent with regard to much needed
diagnostics, and current funding levels are wholly The policy impact hypothesis is that creating
inadequate to address neglected tropical diseases as a global framework for R&D and access to global
only few donors support this area of research and health products against diseases disproportionately
development. affecting poor people in low and lower middle-in-
come countries will ultimately result in the establish-
Switzerland’s position as a leader in innovation as ment of a global financing and coordination mecha-
well as the presence of a research-based pharma nism for health R&D. This in turn leads to research
industry and other research organisations has facili- and development of new global health products
tated the exploitation of synergies for international that are introduced in low and lower middle-income
research collaboration. It also hosts major Product countries and accessed by poor and vulnerable pa-
Development Partnerships (PDPs), such as the Drugs tients.
for Neglected Diseases initiative (DNDi), that have
R&D expertise in NTDs. This area is closely linked to other components of
the GPH, i.e. strengthening global health govern-
Against this background, the SDC’s policy goal is ance, addressing determinants of health and health
to advance the global framework for the re- systems strengthening. Improving medicines regu-
search and development of and access to global latory systems, for instance, not only accelerates
health products for diseases disproportionately access to products that address neglected tropical
affecting people in low and lower middle-in- diseases but also strengthens health systems.
come countries, with a focus on neglected trop-
ical diseases. Three specific objectives have been
defined to achieve this policy goal:
•• Strengthen global research and development
capacities addressing specific neglected tro-
pical diseases in endemic countries through
public-private product development partner-
ships
Voluntary
R&D financing
mechanism
advanced
POLICY GOAL:
R&D capacities
strengthened ADVANCE GLOBAL R&D
through PDPs
AND ACCESS FRAMEWORK
FOR NEGLECTED DISEASES
WHO pre-qualification
listing and country
Figure 4a: registration of products
Policy goal and specific
objectives of sub-area 1
accelerated
154.1.2 Sub-area 2:
Accelerating malaria elimination
Despite enormous progress in malaria control, the •• Develop new medicines, diagnostics and vec-
disease remains a major global public health prob- tor control tools through innovative research
lem. Worldwide, an estimated 3.4 billion people in and development mechanisms and enhance
97 countries are still at risk of malaria. The successes access to these resources in endemic countries
achieved in the past decade are fragile. For instance, •• Strengthen technical capacities at global, re-
mosquito resistance to insecticides and parasite gional and country levels for accelerating ma-
resistance to antimalarial medicines continue to laria control and (pre-) elimination
spread. These are major challenges transcending •• Foster a comprehensive development ap-
country-level capacities and requiring a global re- proach in the fight against malaria through
sponse. Hence maintaining investment for malaria- promoting multisectoral policies (e.g. water,
related research and development and strengthen- agriculture, nutrition).
ing public-private partnerships’ capacity to pursue
elimination objectives are essential.
The policy impact hypothesis is that the advance-
Although malaria elimination is relatively well fund- ment of a global R&D and access framework that
ed, the SDC can make an important difference due fosters innovative financing and multisectoral ap-
to the availability of competitive Swiss scientific and proaches to malaria control and elimination leads to
technical resources in this field. The SDC’s strategic the expansion of malaria-free zones and ultimately
partners in PDPs, academia and industry are among to reduced malaria-related morbidity and mortality
the leading organisations active in malaria control. among populations in currently endemic countries.
Most of these partners are members of the Swiss
Malaria Group, a network supported by the SDC. For instance, the SDC’s support to WHO’s Global
Malaria Programme and the Global Fund (GFATM)
Therefore, the policy goal is to advance a global and the resulting opportunities to influence agenda
R&D and access framework that fosters innova- setting and shape policy formulation underline the
tive financing and multisectoral approaches to strategic link to the core area of “strengthening
malaria control and elimination. The Programme global health governance”.
seeks to achieve three specific objectives to ensure
accomplishment of this policy goal:
New medicines,
diagnostics and
vector control tools
developed
POLICY GOAL: Technical capacities
at the global, regional
ADVANCE GLOBAL R&D and country levels
AND ACCESS FRAMEWORK strengthened
FOR MALARIA CONTROL
AND ELIMINATION
Figure 4b:
Multisectoral
Policy goal and specific
objectives of sub-area 2 approaches
fostered
164.2 Component 2:
Advancing universal health coverage through sustainable
health financing and targeted health systems strengthening
Globally, 400 million people have no access to •• Social health protection mechanisms are ex-
healthcare. Therefore many countries have stipulat- panded to include poorer populations
ed the gradual achievement of universal health cov- •• Additional domestic and global resources for
erage (UHC) as one of their central goals in health. sustainable health financing are mobilized
This means that essential promotional, preventive, •• Quality of service delivery is improved
curative, rehabilitative and palliative services of good through targeted health systems strengthe-
quality are accessible to the entire population with- ning.
out exposing people to financial hardship. The main
challenges are to finance an expanded range of ser-
vices of a certain quality for more people while at The policy impact hypothesis is that the gradual
the same time protecting them from high costs. Al- expansion of universal health coverage through ef-
though NCDs are not a core component of the GPH, fective policies and initiatives fostering sustainable
they are addressed through this core component as health financing and a targeted strengthening of
UHC is also about offering a broader range of af- health systems leads to an increasing part of the
fordable services at a certain quality in an integrated poor population in low and lower middle-income
way. This can be achieved through health services countries having access to quality health services
that are more robust in terms of funding, manage- and products without facing financial hardship.
ment and organisation.
The SDC, through its strategic partnerships, seeks to
The SDC’s comparative advantage is based on its promote equity by extending coverage of necessary
long track record of supporting health financing health services to groups such as pregnant women,
strategies and social health protection mechanisms children, disabled people and poor population seg-
in a number of bilateral programmes. Furthermore, ments and facilitate their stepwise inclusion in social
Switzerland has one of the best health systems, for health protection mechanisms. The SDC does so in
instance in terms of quality and health systems man- the framework of its support to WHO and its board
agement. It also possesses extensive private sector membership at the GFATM and other multilateral
expertise in health insurance as well as technical, players. Therefore, this component is closely linked
academic and research capacities for strengthening to that of “global health governance”.
health systems.
The Programme’s policy goal in this component
is to gradually advance universal health cover-
age in low and lower middle-income countries
through policies and initiatives fostering sus-
tainable health financing and targeted health
systems strengthening. Three specific objectives
have been formulated to achieve this policy goal:
Additional
resources for
sustainable health
financing
mobilized
POLICY GOAL:
ADVANCE UNIVERSAL
HEALTH COVERAGE IN LOW
Quality of AND LOWER MIDDLE-
Figure 5:
Policy goal and specific
service delivery
improved
INCOME COUNTRIES Social health
objectives of component 2
through targeted protection
health systems mechanisms expanded
strengthening to include poorer
populations
174.3 Component 3:
Promoting sexual and reproductive health and rights of
young people through an enabling policy environment
Progress with regard to sexual and reproductive Since national policy dialogue on this topic is diffi-
health and rights (SRHR) is limited worldwide be- cult in many countries, influencing global policy is a
cause it is still inadequately addressed at the level more useful means of impacting on national policies
of research, policies and action. The fact that it is and action. The SDC’s and Switzerland’s engage-
closely linked to cultural and societal values impedes ment in this area is appropriate because the country
the development of favourable national and global pursues liberal domestic policies and therefore has
policies, such as the integration of services related credibility to engage in policy dialogue on favour-
to sexual and reproductive health in primary health able SRHR for young people. Moreover, the SDC
care. Adequate information, education and services can build on experiences gained from bilateral pro-
for young people remain particularly limited. Yet grammes active in sexual and reproductive health.
they represent a large section of the population in
low and middle-income countries and their health The global policy goal is to ensure access to com-
is the basis for future societal and economic devel- prehensive and integrated quality sexual and
opment. Interventions with and for young people reproductive health information, education and
can thus have a positive effect on reducing early and services for young people through the promo-
unwanted pregnancies, maternal deaths or sexually tion of an enabling global policy environment.
transmitted infections including HIV/AIDS. Thus, in This is to be achieved through three specific objec-
the area of SRHR, the GPH will focus mainly − al- tives:
though not exclusively − on young people.
•• Research in sexual and reproductive health
Globally, funding priorities have been focused on of young people is strengthened to serve as
maternal, newborn and child health as well as spe- a foundation for evidence-based global, regional
cific diseases such as HIV/AIDS rather than SRHR. and national policies, guidelines and programmes
Slow progress in some areas of SRHR is due to the •• Access to comprehensive, culturally sensiti-
fact that SRHR is directly or indirectly influenced by ve and age-appropriate quality sexual and
factors outside the health system, such as educa- reproductive health and rights services for
tion, gender equality and more broadly poverty. young people is improved
The core area of SRHR is therefore closely linked to •• Health systems are strengthened through
“universal health coverage” and “determinants of linking HIV/AIDS with sexual and reproductive
health”, two other core areas of the GPH. health and rights services, and through integrati-
on into primary health care.
The policy impact hypothesis is that an enabling
global policy environment is informed by evidence,
including field experiences and the active participa-
tion of young people, fosters access to comprehen-
sive and integrated quality sexual and reproductive
Research in sexual
and reproductive health information, education and services for young
health strengthened people, which in turn leads to an improvement in
their sexual and reproductive health and rights.
POLICY GOAL:
ENSURE ACCESS
TO QUALITY SEXUAL
AND REPRODUCTIVE
HEALTH SERVICES FOR
Access to YOUNG PEOPLE Health systems
comprehensive, strengthened through
culturally sensitive and linking HIV/AIDS with
age-appropriate quality Figure 6:
sexual and reproductive
Policy goal and specific
services improved health and rights objectives of component 3
services
184.4 Component 4:
Addressing determinants of health through
multisectoral collaboration
The place where people are born, grow and live, the as well as with other strategic partners outside the
state of their environment, income and education health sector who are willing to work on these pri-
levels, family and social networks are key determi- orities. The specific objectives are:
nants of their health. This interdependency between
health and its underlying determinants calls for 1. R
educe the dual burden of malnutrition
cross-sectoral responses and “health in all policies” and/or the burden of water-borne diseases
approaches. It is important that awareness of these on poor people in low and lower middle in-
determinants is raised in other sectors as well, both come countries through the generation of
at the national and international level. Therefore evidence, the formulation of multisectoral
the SDC’s Health Policy stipulates that it promotes policies and innovative collaborative inter-
multisectoral approaches to address both systemic ventions at the global, regional and national
and social determinants impeding access to quality level
health services.
2. Whenever relevant and possible, consider health
The policy goal is to address determinants of in other SDC Global Programme interven-
health through the formulation and imple- tions (by adding a component, encouraging co-
mentation of specific “health in all policies” ordinated approaches, measuring health effects)
approaches for priority areas and related multi-
sectoral approaches. The priority is to address mal- Whenever relevant and possible, ensure that
3.
nutrition in its different forms, including obesity, to food security and/or “water-sanitation-hy-
promote health and prevent NCDs. Moreover, qual- giene” are taken into consideration in the
ity of (drinking) water is another priority to prevent work of the Global Programme Health.
water-borne diseases. The GPH will aim to develop
joint interventions with SDC Global Programmes10 The policy impact hypothesis is that specific
“health in all policies” and multisectoral strategies
addressing major determinants of health are imple-
mented in such way that health risks are reduced for
10 Swiss Agency for Development and Cooperation an increasing number of poor and vulnerable groups
(2014, 2013b, 2013c) in low and lower middle-income countries.
Food security and
water-sanitation-
hygiene considered
in SDC Global
Programme Health
POLICY GOAL: Health aspects
considered in
ADDRESS DETERMINANTS other SDC Global
Programmes
OF HEALTH
Burden of
Figure 7: malnutrition and
Policy goal and specific water-borne diseases
objectives of component 4 reduced
194.5 Component 5:
Strengthening global health governance through efficient
coordination between multilateral organisations
Global health governance has gained in importance hance the credibility of WHO, the Global Fund
during the last decade. This development is due to and other multilateral organisations through
the impact of globalisation and the awareness that effective and tangible development results
many health challenges can no longer be solved •• Strengthen multisectoral approaches and col-
through domestic actions alone but need to be laboration in health with multilateral partners
tackled jointly by the global health community and •• Strengthen Switzerland’s shareholder role in
its various actors through a coherent system of gov- multilateral organisations through coherent
ernance. The growing number of actors has led to a policy messaging across Swiss departments.
complex landscape in global health governance. The
situation becomes more complex as the actors and
the governance system also have to address new The policy impact hypothesis is that a stronger
challenges (e.g. NCDs related to obesity, tobacco normative and coordinating role of WHO, multisec-
and alcohol). toral collaborations for health between multilateral
organisations based in Geneva as well as coherent
Hence, the policy goal is to strengthen global Swiss policy messaging will foster the efficient co-
health governance by leveraging Geneva’s posi- ordination between these organisations. This in turn
tion as host to many health organisations and will contribute to strengthening global health gov-
consolidating the role of WHO as the leading glob- ernance and ultimately to increased effectiveness of
al coordinating authority on health. WHO defines global health interventions for the benefit of poor
rules and processes and facilitates collective action people in low and lower middle-income countries.
against health threats. The SDC shares this policy
goal with other Swiss federal departments and of-
fices, who together implement the Swiss Health
Foreign Policy. Three specific objectives have been
outlined to achieve this policy goal:
•• Strengthen WHO’s coordinating and norma-
tive role in global health governance and en-
WHO‘s coordinating
and normative role
strengthened and credibility
of multilateral partner
organisations enhanced
Figure 8:
Policy goal and specific
objectives of component 5
Switzerland‘s
POLICY GOAL: shareholder role
in multilateral
STRENGTHEN GLOBAL organisations
Multi-sectoral HEALTH GOVERNANCE strengthened
approaches and
collaborations
in health
strengthened
205. Working modalities
The Programme seeks to influence agenda setting innovative global partnerships and initiatives it
and shape policy formulation through a three- supports, such as the WHO, Global Fund or UN-
fold approach: AIDS. Depending on the component, the GPH
works directly with strategic operational and
1. Engaging in health policy dialogue: institutional partners, which include multilateral
The Programme engages in policy dialogue at the agencies, international NGOs, private sector or-
United Nations and WHO level with focus on its ganisations, research institutes and other donors.
core components. The Programme pursues the Research-based pharmaceutical companies as
objective of influencing policy within the frame- well as research institutes, for instance, are of-
work of the Swiss Health Foreign Policy by align- ten collaborators in PDPs supported by the SDC
ing its positions with other federal departments, in the core component “innovative research and
such as the Federal Office of Public Health, the development of medical resources”. They provide
Division for Sectoral Foreign Policy and the Swiss access to compound libraries and know-how.
missions in Geneva and New York. Its policy work
is underpinned by evidence and experiences from
Wherever possible, the Programme seeks to make
SDC-supported global initiatives as well as multi- SDC bilateral programmes benefit directly from
lateral and bilateral programmes that are of rel- these global initiatives. An example is the P4H
evance to the GPH components. (“Providing for Health”) initiative that provides coor-
dinated technical and strategic support to countries
2.
Supporting innovative global partnerships that want to develop social health protection strate-
and initiatives: gies. Several SDC bilateral programmes supporting
The Programme endeavours to shape policies national health financing reforms (e.g. Tanzania,
related to its core components through board Mozambique, Chad and Benin) have facilitated P4H
memberships and other steering functions in the technical assistance to their bilateral partners.
213. Fostering knowledge building and exchange
The prerequisites for such synergies are that both
of experiences through continuous network- SDC country programmes and the GPH focus on
ing: similar priorities and that continuous exchange is
The credibility of the Programme’s policy work facilitated in a systematic way. The SDC’s Health
depends not only on the supported global initia- Network has a pivotal role in fostering knowledge
tives, but also on a continuous exchange with the exchange, capacity building and institutional
SDC’s bilateral and humanitarian programmes learning as well as collaboration within the SDC.
active in health with regard to their country level Important instruments to promote such activities
policy and programme evidence. The GPH aims are the SDC face-to-face Health Network meet-
to nurture its global policy work in an informed ings, e-discussions and news/literature notifica-
way by making use of the results, operational tions on topics relevant to both sides. Hosted and
experiences and lessons learnt from the SDC’s facilitated by the GPH, the Network also provides
country-based cooperation activities. At the health policy and programme-related advice and
same time, the Programme supports the SDC’s strategic orientation.
policy dialogue at the national level by informing
bilateral programmes about the latest develop-
ments in global health policies relevant to their
work.
226. Human resources, budget,
M&E and communication
The team of the Global Programme Health is com- 2. Second, progress and effectiveness are assessed at
posed of 6 full time equivalents, including two the level of each of the supported global partner-
health policy advisors who are also jointly respon- ships/initiatives that fall under the respective core
sible for the SDC Health Network. Given its limited component. The performance of each supported
human resource base, the Programme strives to global initiative is measured according to the re-
leverage “external” capacities, for instance of SDC spective objectives and expected outcomes stipu-
bilateral and other global programmes as well as lated in the contract agreements (see appendix 5).
of Swiss federal departments involved in the SHFP,
to advance policy goals and the supported global Reporting on progress and results is done through
initiatives. Resources (funds, competencies, skills, in- different channels: the Programme’s annual report,
fluence) can be combined in a synergistic and cost- the SDC Health Network share web as well as policy
effective way to pursue mutual objectives. briefs on topics, positions and supported initiatives
related to the five core components. Finally, the
For the period 2015-2019, the Programme’s indica- Programme also participates in and (co-)organizes
tive budget amounts to approximately CHF 250 events (conferences, symposia, workshops etc.) to
million of which approximately CHF 170 million are disseminate results and lessons learnt both within
dedicated to multilateral support. the SDC and outside. At the same time, such events
are opportunities to engage in stakeholder dialogue
Monitoring & evaluation are ensured at two lev- and relationship building with parties who work on
els: the GPH’s core components but who are not strate-
gic partners in SDC-supported global initiatives.
1. First, for each core component a results frame-
work was developed that stipulates the global The Programme will define core elements for its
policy goal, the policy impact hypothesis, the medium-term SDC internal (e.g. decision makers
specific objectives and expected results neces- at division and country office levels) and external
sary to achieve that impact as well as the key per- communication. Accordingly communication ob-
formance indicators (see Appendix 6 of the full jectives will be specified annually in the framework
document). of the Programme’s annual planning exercise.
237. Appendices
Appendix 1: References
Bundesministerium für Gesundheit der Bun- Swiss Agency for Development and Coopera-
desrepublik Deutschland (2013): Globale Gesund- tion (2013a): SDC Health Policy.
heitspolitik gestalten – gemeinsam handeln – Verant-
wortung wahrnehmen. Konzept der Bundesregierung. Swiss Agency for Development and Coop-
eration (2013b): Strategic Framework 2013-2017.
Eidgenössisches Departement für auswärtige Global Programme Food Security.
Angelegenheiten (2012): Aussenpolitische Strat-
egie 2012-2015. Swiss Agency for Development and Coopera-
tion (2013c): Strategic Framework 2013-2017. Glob-
Federal Department of Foreign Affairs and Fed- al Programme Migration and Development.
eral Department of Home Affairs (2012): Swiss
Health Foreign Policy. United Nations (2014): Millennium Development
Goals Report 2014. New York
Norwegian Ministry of Foreign Affairs (2012):
Global health in foreign and development policy. UNAIDS (2014): GAP Report.
Report to the Storting (white paper).
United Nations Population Fund (UNFP) (2014):
Schweizerische Eidgenossenschaft (2013): Botschaft State of World Population.
zur Internationalen Zusammenarbeit 2013-2016.
World Health Organization (2014): World Malaria
Swiss Agency for Development and Coopera- Report. Geneva.
tion (2014): Strategic Framework 2013-2017. Global
Programme Water Initiatives.
Appendix 2: List of acronyms
AIDS = Acquired Immune Deficiency Syndrome RBM = Roll Back Malaria Partnership
CCM = Core Contribution Management R&D = Research and Development
GF(ATM) = Global Fund for AIDS, TB and Malaria (of medical products)
GMP = Global Malaria Programme SDC = Swiss Agency for Development and Cooperation
GHG = Global Health Governance SDGs = Sustainable Development Goals
GPH = SDC Global Programme Health SHFP = Swiss Health Foreign Policy
MDGs = Millennium Development Goals SRHR = Sexual and Reproductive Health and Rights
M&E = Monitoring and Evaluation STI = Sexually Transmitted Infections
NCDs = Non-Communicable Diseases TDR = Special Programme for Research and
NGO = Non-Governmental Organisation Training in Tropical Diseases
NMRA = National Medicines Regulatory Authorities TB = Tuberculosis
NTDs = Neglected Tropical Diseases UHC = Universal Health Coverage
OECD = Organisation for Economic Co-operation UNAIDS = United Nations AIDS Programme
and Development WHO = World Health Organization
PDPs = Product Development Partnerships WoG = Whole of Government
P4H = Provinding for Health Global Network
24Appendix 3: SDC Health Policy
The overall goal of the SDC’s Health Policy is to of this overall goal, three main objectives have
improve population health with a special focus been formulated:
on poor and vulnerable groups. By vulnerable
groups, we mean people who are more likely to be •• Strengthen health systems to extend universal coverage
exposed to major health risks and in need of health •• Reduce the burden of communicable and non-
services. These include pregnant women, children, communicable diseases
young people, disabled persons or the elderly. In •• Improve maternal, newborn and child, as well as
order to effectively contribute to the achievement sexual and reproductive health.
Appendix 4: The 20 objectives of the Swiss Health Foreign Policy
Those objectives to which the Global Programme 12. Further strengthen the international system
Health responds are marked in bold: for communicable disease surveillance and
control
1. Establish a legal framework for collaboration
with the European Union on health and con- 13. Protect the public from health risks in the ar-
sumer protection matters eas of food safety, radiological protection and
chemicals
2. Strengthen WHO as the leading, coordinat-
ing global health authority 14. Combat the global shortage and unequal distri-
bution of health personnel
3. Improve the effectiveness, efficiency and
coherence of the global health architecture 15. Improve access to essential (established and
newly developed), good-quality, affordable
4. Place at the centre of Swiss Health Foreign medicines and medical devices
Policy, the promotion of effective, high-
quality, affordable and equitable systems 16. Promote the prevention, diagnosis and
treatment of non-communicable diseases
5. Integrate health as a key element of foreign policy
17. Establish internationally the fourfold policy (pre-
6. Consolidate and strengthen Geneva’s posi- vention, therapy and rehabilitation, harm reduc-
tion as the “health capital of the world” tion, and law enforcement and control)
7. Establish conditions for the strengthening 18. Make available Switzerland’s capacities and skills
of global health research for saving lives and restoring health in humani-
tarian crises
8. Position the strengths of Switzerland’s health
sector economy internationally 19. Promote and secure the right of everyone
to the enjoyment of the highest attainable
9. Provide appropriate protection for intellectual standard of physical and mental health
property (IP) as an incentive for research
20. Promote maternal and child health, and sex-
10. Sustainably improve the economic, social ual and reproductive health
and environmental determinants of health
11. Fully exploit the potential of technological develop-
ments and social media in the area of global health
25Appendix 5: Monitoring matrix of the Global Programme
Health – example from one priority area
Addressing communicable diseases through innovative research and
development of medical resources
NTDs: Improving access to medical resources for neglected tropical diseases
Overall policy goal Specific policy goals Annual policy Overall policy
results results
Advance global R&D and access • Strengthen global R&D capacities and efforts for • To be completed • To be completed
framework for global health NTDs and other diseases that disproportionately at the end of the at the end of the
products against NTDs and other affect people in low and lower middle-income year project (phase)
diseases that disproportionately countries
affect people in low and middle- • Establish a sustainable and voluntary financing and
income countries. coordination mechanism for innovative health R&D
at the global level
• Accelerate and increase efficiency of regulatory
review and registration processes of global health
products
Initiatives Objectives of initiatives Annual opera- Overall opera-
(with average annual SDC dis- tional results for tional results for
bursements in CHF and contract each initiative each initiative
period)
Special Programme for Research • Foster an effective global research effort on infec- • To be completed • To be completed
and Training in Tropical Diseases tious diseases of poverty and promote the translation at the end of the at the end of the
(TDR) of innovation to health impact in disease endemic year project (phase)
countries
1,650,000 CHF (2013-2015)
Drugs for Neglected Diseases • Develop and provide access to treatments for • To be completed • To be completed
initiative (DNDi) neglected tropical diseases that primarily affect the at the end of the at the end of the
poor and marginalised populations worldwide year project (phase)
2,000,000 CHF (2013-2016) • Deliver 11 to 13 new treatments by 2018 for leish-
maniasis, human African trypanosomiasis (sleeping
sickness), Chagas disease, malaria, paediatric HIV,
and specific helminth infections
Foundation for Innovative New • Drive the development and early implementation of • To be completed • To be completed
Diagnostics (FIND) innovative diagnostic tests that have a high impact at the end of the at the end of the
on patient care and disease control in low-resource year project (phase)
800,000 CHF (2013-2016) settings
WHO-FIND Ebola Diagnostic Ac- • Research, develop and provide access to new Ebola • To be completed • To be completed
cess Coalition diagnostic tests at the end of the at the end of the
year project (phase)
1,000,000 CHF (2014-2015)
Innovative R&D Demonstration • Through innovative approaches to coordination and • To be completed • To be completed
Projects financing of R&D: develop a series of cost-effective at the end of the at the end of the
novel therapeutic products against different forms year project (phase)
2,000,000 CHF (2014-2016) of leishmaniasis as well as diagnostic kits for malaria,
schistosomiasis and trypanosomiasis (sleeping sick-
ness)
TOTAL: 7,450,000
26Appendix 6: Results framework for each programme component
Component 1: Reducing the burden of communicable diseases through innovative research and
development of medical resources
Sub area 1: Improving access to medical resources for Neglected Tropical Diseases
Policy impact hypothesis: The creation of a global framework for R&D and access to global health products against diseases dispro-
portionately affecting poor people in low and lower middle-income countries will ultimately result in the establishment of a global
financing and coordination mechanism for health R&D. This in turn leads to research and development of new global health products
that are introduced in low and lower middle-income countries and accessed by poor and vulnerable patients.
Policy goal, impact hypothesis and specific objectives Key performance indicators
Global health New global health products are developed, registered and intro- • Number of health technology products devel-
impact duced in low and lower middle-income countries and accessed by oped through financing from the R&D fund
patients • Number of newly developed health tech-
nology products pre-qualified by WHO and
registered by National Medicines Regula-
tory Authorities (NMRAs) of endemic
countries
• Number of deliveries to endemic countries
(categorised by developed health technol-
ogy product)
Global policy Global framework for R&D of and access to global health products • Amount of non-earmarked, pooled fund-
goal for diseases disproportionately affecting people in low and lower ing paid into the global voluntary health
middle-income countries, with a focus on NTDs, is advanced R&D financing mechanism
• Number of projects funded through global
voluntary health R&D financing mechanism
Specific Strengthen global R&D capacities addressing specific neglected • Number of products developed through
objective 1 tropical diseases in endemic countries through public-private product R&D at different stages of the pipeline
development partnerships (discovery, pre-clinical, clinical and imple-
mentation) for specific NTDs and poverty-
related diseases
Expected results • New or improved efficacious and safe quality medicines, diagnostics and • Number of collaborations between dif-
vector control products for selected NTDs and poverty-related diseases ferent organisations doing R&D of health
developed technology products
• Complementary approaches to different health technology products ›› for the same disease
collaboratively developed (e.g. diagnostic and medicine for one disease, ›› that can be used for several diseases
diagnostic that can be used for several diseases)
Key activity • Strengthen global R&D capacities through Product Development Partner-
lines ships (PDPs) (medicines, diagnostics, vector control tools)
• Foster collaboration between PDPs in order to advance the development
of integrated solutions to NTDs and poverty-related disease control and
elimination
• Contribute to the development of knowledge regarding access to
medicines and value for financial issues of PDPs
• Align PDPs with WHO-led process by linking them with innovative
financing and coordination mechanism (see specific objective 2)
27You can also read