STRATEGIES FOR PREVENTION OF CERVICAL CANCER IN NEW ZEALAND - COLLETTE BROMHEAD PHD SENIOR LECTURER MASSEY UNIVERSITY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Strategies for Prevention of
Cervical Cancer in New Zealand
Collette Bromhead PhD
Senior Lecturer
Massey University
Green sea turtle (Chelonia mydas) with Papilloma www.naturescapes.net
ABSTRACT Cervical cancer is now almost completely preventable through HPV vaccination and screening. Despite the huge gains in scientific and medical knowledge in this field, there remain persistent inequities in cervical screening coverage in New Zealand, particularly for Maori women. Our National Cervical Screening Programme (NCSP) has announced it will be transitioning from cytology to primary oncogenic HPV screening by 2021. This allows the potential for self collected samples via a low vaginal swab, a strategy that is increasingly being incorporated into cervical screening programmes internationally. In this talk I will give an update on the role of oncogenic HPV in cervical cancer and the proposed HPV primary screening algorithm for NZ. Additionally I will give a brief overview of our research to establish whether self-sampling for HPV will increase the uptake of screening in Maori, Pacific and Asian women in NZ.
4.9 Million
Humans
27.6 Million Sheep
Centre of
government…and a bit
windy
Papillomaviruses Throughout
History
1842: Rigoni Stern observes the nuns have lower incidence of cervical cancer than
prostitutes……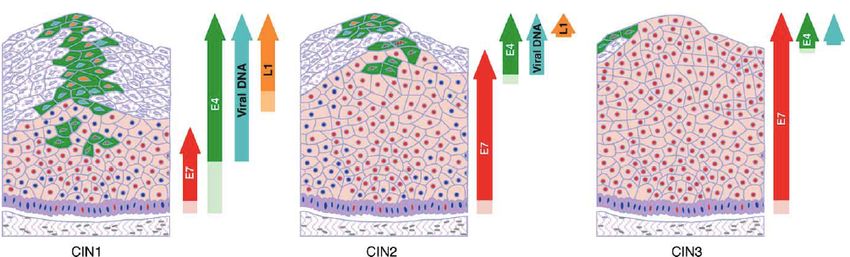
1983: Harald zur Hausen finds HPV types 16 and 18 lurking in HeLa cells and other cervical cancer cells. 2008: Wins the Nobel Prize.
The HPV Genome
•One coding strand.
Genome is divided into
Late and Early regions E6 E7
Transforming
Major capsid protein 7904/1
7000 1000
L1
6000 2000
E1
5000 3000 Replication
4000
E4
L2
E5 E2
Minor capsid protein
Replication and
transcription
Progression to Cancer is Accompanied by
Deregulation of Viral Gene Expression
CIN 1 CIN 2 CIN 3
Common molecular events:
•Viral genome integration into cellular DNA
•Loss of E2 leads to increased E6/E7 expression
•Loss of L1, L2 expression. Therefore, current vaccine
can’t clear pre-cancerous lesions.
Doorbar, J Clin Virol 32:7-15, 2005
HPV AND CERVICAL CANCER IN NEW ZEALAND

Type specific prevalence of oncogenic HPV infection in NZ women
with ASC-H/HSIL cytology, histologically-confirmed grade CIN 2 and
≥ CIN 3
100,0
90,0
80,0
70,0
Prevalence (%)
60,0
50,0
40,0 ASC-H/HSIL cytology
CIN2
30,0
CIN3
20,0
10,0
0,0
16 52 β 31 33 18 58 51 39 45 59 35 56 68 16 16 OHR Single Any
and/or and/or HR HR
18 HPV HPV
18
HPV Genotype (alone)
Simonella et al.: Type-specific oncogenic human papillomavirus infection in high grade cervical disease in New Zealand. BMC Infectious Diseases 2013 13:114.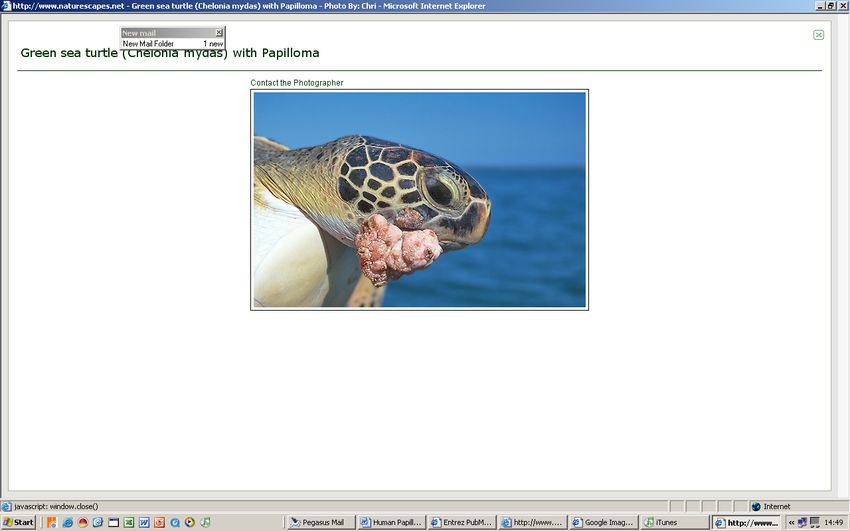
What About Māori Women?
¡ The overall prevalence of vaccine-included types in
CIN2/3 was similar in Māori and non-Māori women,
¡ Implies that the long-term effects of vaccination will
be similar in the two groups.
¡ Age- specific patterns of infection for HPV16/18 in
confirmed CIN2/3 differed between the two groups:
Ø lower prevalence in younger vs. older Māori women (57%
in 20-29 years vs 75% in 40-69 years)
Ø higher prevalence in younger vs. older non-Māori women
(70% in 20-29 years vs 49% in 40-69 years).• Incidence rate of 6.9/100,000 women • Only 13% of women with confirmed cancer had engaged with regular screening
CURRENT NZ CXCA SCREENING
PROGRAMME
• For asymptomatic women aged 20 - 69
• 3 year normal screening interval
• Since 2008 – 100% LBC
• HrHPV qualitative for
– triage of ASC-US and LSIL and
– TOC following treatment of HGSILNZ Screening Pathway for
Asymptomatic Women
(2021)
https://www.nsu.govt.nz/health-professionals/national-cervical-screening-
programme/hpv-primary-screening/frequently-askedKEY POINTS: HPV PRIMARY SCREENING • 5 year interval instead of 3 year • HPV will be primary test but LBC is still primary sample type • Recommended age for commencement has already risen to 25 years • Same screening pathway for unvaccinated and vaccinated women • NCSP register needs significant change • Self sampling acceptability being assessed
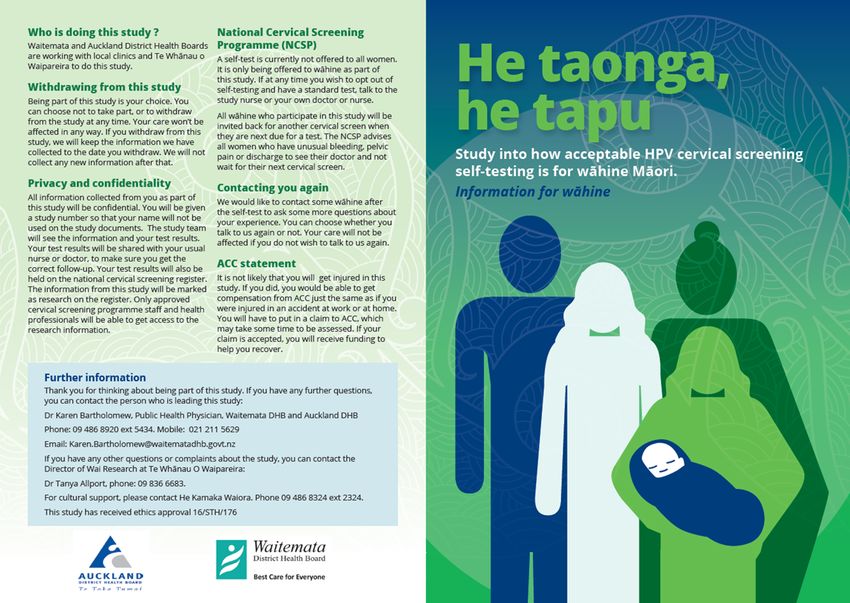
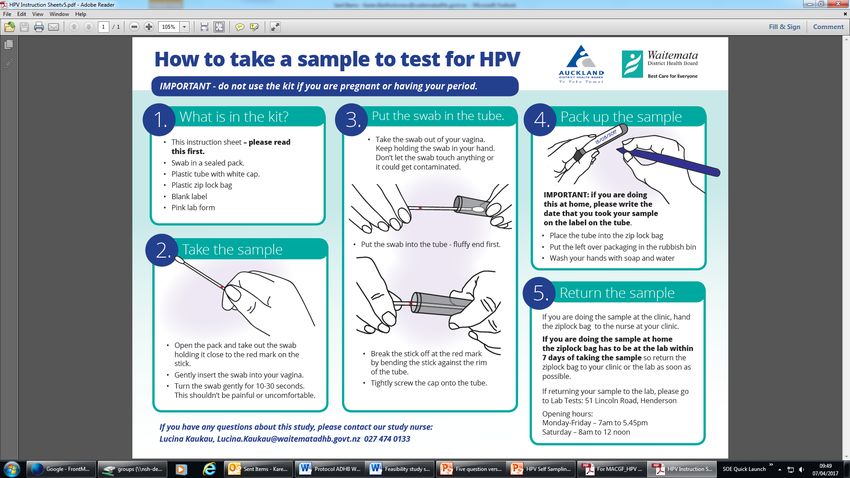
Self Sampling for HPV: To reduce
inequity in coverage and outcomes
Ethnicity Auckland DHB Waitemata DHB
Coverage Addition Coverage Addition
al al
screens screens
to reach to reach
80% 80%
target target
Māori 55.3% 2,539 59.3% 2,744
Pacific 71.4% 1,126 72.6% 722
Asian 56.0% 11,998 68.6% 4,380
NZ 78.5% 1,128 78.7% 1,285
European/Other
Source: National Cervical Screening Programme, Ministry of Health, DHB Quarterly report
3 year coverage for women aged 25-69, by ethnicity, to June 2017Women-centred implementation
research informed by international
evidenceFindings: Women’s experience of current
screening
Reason for not recently or never having had a smear (ranked)
1. Embarrassment Exposing my private parts for someone to look at
(Pacific woman)
2. Prior negative Pain, discomfort, negative clinician interactions
experience They tell us to relax and it’s so painful and uncomfortable
(Pacific woman)
3. Lack of information or Uncertain if they need a test, not comfortable to ask or
knowledge ‘not having sex’
You don’t get a good explanation of the procedure and
purpose (Chinese woman)
GP just texts, no information (Māori woman)
4. Inconvenience Time, travel constraints
Clinic is only open when I’m at work (Indian woman)
5. Cost Contributory but not the main reason (free or low cost for
most)Focus Groups
Quantitative Māori Pacific Asian
Findings Attended
Completed self-test
20
18
10
9
11
11
Percent 90% 90% 100%
84 women
participated
in self-testing Feasibility Study Māori women
Number of
HPV prevalence of Percent
women
5%
Eligible women identified 366
(fits with similar
studies overseas) Able to be contacted (5
114 31% eligible
*1 woman with attempts)
HPV18 had 22%
Declined 25
adenocarcinoma contacted
on colposcopy DNA clinic appointments 31
41%
contacted
Completed the self-test 46
12% eligibleWhat about…
HPV VACCINATION?• Since 2008 Gardasil 4 funded for girls aged 11-13 via school and GP with catchup vaccination funded up to 20 years of age
… a retrospective analysis of 50,984 pregnancies in NZ between 2008 and 2014 found that HPV vaccination with > 1 dose of quadrivalent vax prior to pregnancy was associated with a 13% reduced likelihood of a pre-term birth, but no decrease in pre-eclamplsia or perinatal death.
Effect of vaccination on HSIL rates Smith M, Rumlee L, Canfell K. National Cervical Screening Programme Monitoring Report Number 47 (1 January – 30 June 2017). National Screening Unit: Wellington, 2018.
Changes to HPV Immunisation in
NZ 2017
• HPV Immunisation is now funded for everyone
aged 9-26 years inclusive, including boys and
young men
• Gardasil 9 replases Gardasil 4 and given as
either 2 doses (15
years)
• Vaccinations are provided as part of the
School Based Vaccination Programmed to
children aged 11-12 yearsOngoing Challenges • Getting vaccinated women (particularly those vaccinated with G4) to participate in screening • Evidence of declining participation in NCSP – #Bullet proof • Self sampling a tool to reach this group? • Between the HPV Vaccine and PREP plus condom fatigue, are we on the verge of an epidemic of preventable STI’s such as Syphillis?
The HPV Self-Sampling Feasibility Study
Investigators and Partners
Primary Investigator: Dr Karen Bartholomew
Co-Investigators: Dr Collette Bromhead, Dr Helen Wihongi, Georgina
McPherson, Dr Mee-Ling Yeong, Dr Tanya Allport,
Dr Marion Saville (advisor)
Research team: Jane Grant, Lucina KauKau, Anna Maxwell
Māori Advisors: Dr Sue Crengle, Dr Nina Scott
Pacific Advisors: Dr ‘Aivi Puloka, Leani Sandford,
Asian advisors: Gloria Ya Ping Gao, Samuel Cho, Samantha Bennett
Partners: East Tamaki Health Care PHO, National Hauora
Coalition PHO,
ProCare PHO, Susan Reid (Health Literacy NZ),
Georgina Martin and Hector Kaiwai (WaiResearch)
Laboratory: Anatomic Pathology Service; Dr Mee-Ling Yeong, Amy
Tan, Liz Pringle, Krish Pillay
Clinical Reference : Dr Kristy Gendall, Anna Wang, Dr Collette BromheadMerci!
Email : c.bromhead@massey.ac.nz
Linkedin: https://www.linkedin.com/in/collette-bromhead-0154a972You can also read