Suicidal Patients in Primary Care: What Now? - NPACE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Suicidal Patients in
Primary Care: What
Now?
Dr. Tari Dilks, PMHNP-BC, FNP-BC
Professor and Co-Coordinator Graduate Nursing
McNeese State University
Developed for NPACE – Nashville, 2018
Originally developed with:
Dr. Amanda Eymard, PMHNP-BC
Disclosures
Dr Tari Dilks has been a paid speaker for
Otsuka
1Disclaimer
The material in this presentation has been
put together originally by Drs. Dilks and
Eymard from a variety of sources and every
effort has been made to assure its accuracy.
Changes happen rapidly in this field and
the material may become dated. Material in
this presentation should not be perceived as
a recommendation for patient care for
anyone who is not a patient of Dr Dilks.
Objectives
Discuss laws specific to suicide assessment,
treatment, and management.
Review appropriate suicide assessment,
treatment, and management protocol in primary
care setting.
Discuss legal/ethical issues regarding suicide risk
in primary care setting.
Discuss referral procedures and options for
patients needing involuntary confinement.
Kate Spade – 1962 - 2018
http://www.foxnews.com/entertainment/2018/06/18/kate-spades-funeral-to-be-held-at-her-birthplace.html
2Anthony Bourdain – 1956-2018
https://pagesix.com/2018/06/09/anthony-bourdain-was-regularly-suicidal-after-end-of-first-marriage/
https://youtu.be/4ESz9cefwPQ
https://youtu.be/4ESz9cefwPQ used with permission
National Suicide Prevention
Lifeline at 1-800-273-TALK
(8255)
or
Contact the Crisis Text Line by
texting TALK to 741-741.
3Case Study
59 y/o female presents to clinic with multiple somatic
complaints; much focus on insomnia, pain, low energy,
increased anxiety. Recent financial stressors, new
medications prescribed for co-morbidities, family stress.
Made several passive comments regarding not wanting
to live anymore. Avoids subject when asked directly
about SI; laughs and attempts to change subject.
What do you do? What other information do you need
to move forward?
CDC Report – June, 2018
Between 1999 and 2016 over ½ of the US states
saw an increase in suicide rates of over 30%
All states, with the exception of Nevada saw an
increase of 6% or more
About 90% of suicides did have pre-existing
psych conditions as determined with
psychological autopsies, medical records and
information gathered from clinicians and families.
Among those with no known mental health
condition – 84% were men
54% of suicides had not received a clinical
diagnosis of mental illness at the time of death.
Leading causes of death by suicide in order –
firearms, hanging and poisoning.
Contributing factors are varied – relationship,
heath, housing, job, legal problems, substance
abuse and recent crisis are often identified, but
are not the only factors
Suicide is more than an mental health issue.
4Link between suicide and RLS
A June 4, 2018 presentation at SLEEP 2018 reported
on a strong link between lifetime suicidal behaviors
and Restless Leg Syndrome of 30.7% compared to
controls at 10.1%.
N=198 patients with RLS and 164 controls
RLS is also associated with insomnia and depression
One of the researchers indicated that the findings are
similar to those patients with chronic pain
Koo, B. & Winkelman, J. (2018). Restless Legs Syndrome an independent suicide risk factor? Presented at SLEEP 2018: 32nd Annual Meeting
of the Associated Professional Sleep Societies.
Suicide Stats
Approximately 45,000 US suicides in 2016 – 1 every 12
minutes – has been on the rise in past decade
More people die from suicide than homicide or
automobile accidents – ½ use firearms
Highest suicide rate has changed from people over 65
to mid-life (45-64)
Highest rate for men >75 and women 45-64
Suicide is the second leading cause of death in 15-34
year olds
25 attempts for each successful suicide
Females attempt suicide 3x as often as males, but males
complete suicide 4x as often as females.
Freeman, S. (2010); SAMSHA (2018)
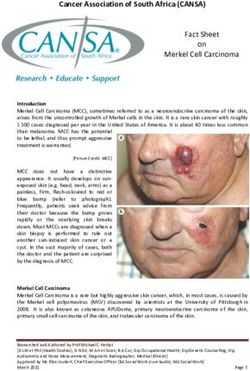
Changes in Suicide Rates – 1999-2016
file://localhost/.file/id
=6571367.15138136
https://www.cdc.gov/mmwr/volumes/67/wr/figures/mm6722a1-F.gif
5 Montana had the highest suicide rate
(29.2/100,00)
Lowest was in DC (6.9/100,000)
While Nevada was the only state who
experienced a decrease in suicide rates, it
remains the 9th highest rate in the country
Rates for 10-14 year old girls have tripled.
June 2018 CDC Report
Key Message
Suicide is preventable
There are evidence based strategies
that can help
Highlights the need for access to
mental health care
Help is available and there is no shame
in seeking help
Older Adults
>8,000 people >60 die each year from
suicide.
White males >75 years old 4x higher rate
of suicide than nation’s overall rate of
suicide (Lowest rate is adult African
American women)
2x more likely to use firearms
More frail, more likely to have a plan,
more isolated, less likely to be rescued,
more likely to die!
Disabled, alone, dependent, medical
issues, lack of access to social support
SAMHSA, (2018); AoA, (2012)
6Depression and Adolescents
What is the role of depression in
adolescent suicide, murder sprees and
teenage mother’s killing their babies.
Some studies indicate that 8.3% of
adolescents will begin to exhibit signs
of major depression compared to 5.3
% for adults.
Adults are more apt to recognize their
depression and get treatment, while
most teenagers will not receive the
help that they need.
The suicide rate in 2015 was 12.5 per 100,000
in adolescents – that is more adolescents than
will die from all other illnesses – cancer to AIDS
– combined. Only traffic accidents will take
more adolescents than suicides.
Even more frightening – there are studies that
suggest every single day, in every single
school, in America, teenagers are thinking
about suicide or making actual attempts:
19% (3 million) of all US high school students have
thought of suicide
Over 2 million have made plans to carry it out
400,000 have made suicide attempts requiring medical
attention
Over 1,000 attempts a day, nationwide, every day of the
year
Suicide rates in girls ages 10-14 have tripled over
the past 15 years from 0.5 to 1.7 per 100,000
A child under the age of 13 commits suicide every
3.4 days according to one study
The CDC has reported (2) five year olds, (4) six
year olds and (8) seven year olds committed suicide
between 1999 and 2015.
7 The cause is unknown – perhaps bullying and
internet? Expectations of coaches, parents and
school?
Suicide in elementary school children not well
studied (10th leading cause in this age group).
Sheftall et al. (2016) reported that young children
are more commonly black, males who use
hanging/suffocation/strangulation at home and
have relationship problems with family members.
Mental health issues have more often been
associated with ADD/ADHD.
What is the lowest age you have seen of someone
who is suicidal?
http://pediatrics.aappublications.org/content/early/2016/09/15/peds.2016-0436
Groups at risk
Incarcerated
US Armed forces and veterans
Youth in foster care
LGBT populations – some data indicate that
suicidal behavior ranges from 40-65% in
transgendered individuals
Bereavement of a loved ones suicide
Medical co-morbidities
A bit more on transgendered rates
Selected Prevalence Other
Trans men (46%) Family lack of support
Trans women (42%) (57%)
Cross dressing (21%) Discrimination/harassme
Ages 18-24 (45%) nt (59%)
Multiracial (54%) Health care professional
Low ed. level (49%) refused to treat (60%)
Disabilities (65%) Victimized by law
enforcement (61%)
Homeless (69%)
https://williamsinstitute.law.ucla.edu/wp-content/uploads/AFSP-Williams-Suicide-Report-Final.pdf
Retrieved 07/19/18
8US Air Force Suicide Prevention
US Air Force Suicide Prevention Program has
11 policy and education initiatives which
increased social support, social skills, and help
seeking. This shifted the focus away from
individuals to community wide concerns. There
was a 33% reduction in suicide and other related
problems since its inception in 2001.
http://dmna.ny.gov/r3sp/suicide/AFPAM44-160.pdf
Retrieved 07/19/18
2012 National Strategy for
Suicide Prevention
Four interconnected strategic sections
Empowering and promoting health in individuals,
families and communities
Preventive services in clinical and community
settings
Treatment and support services
Plans for surveillance, research and evaluation
Priorities –
add suicide prevention strategies into health care reform,
encourage health care systems to aid in suicide reductions,
change the public conversation
CDC – Several Resources
Suicide prevention: A technical package of
policy, programs and practices.
https://www.cdc.gov/violenceprevention/pdf/s
uicideTechnicalPackage.pdf
Strategic direction for the prevention of suicidal
behavior: Promoting individual, family, and
community connectedness to prevent suicidal
behavior.
https://www.cdc.gov/ViolencePrevention/pdf/
Suicide_Strategic_Direction_Full_Version-a.pdf
9Strategies - CDC
Strengthen economic supports
Increase access and delivery of mental health
support
Promote protective environments and
connectedness
Teach coping and problem solving skills
Identify and support people at risk
Lessen harm (safe reporting) and prevent future
risk
Additional Resources
Zerosuicide in health and behavioral health care
– toolkits available
http://zerosuicide.sprc.org/
Suicide Prevention Resource Center – has
multiple links to many different tools
http://www.sprc.org/sites/default/files/migrate/lib
rary/RS_suicide screening_91814 final.pdf
Risk factors
Prior suicide attempts (especially in the previous 5 year
period)
Mood disorders
Alcohol and drug use
Access to lethal means
Unsafe media portrayals of suicide
Lack of supportive relationships – personal and health
care providers
Violence
Life transitions
SAMSHA, (2012)
10Additional risk factors
Family history of suicide
White, older male
Recent loss
Lives alone; minimal support
Medical co-morbidities including depression and
schizophrenia
Psychosis and substance abuse
Protective factors
Availability of supportive health care providers –
medical and mental health
Restrictions on lethal means of suicide
Supportive environments
Connectedness
Moral objection to suicide
Previous coping and problem solving
Reasons to live
Warning signs
Talking about wanting to die and ways to kill
oneself
Giving away belongings
Feelings of hopelessness, entrapment, pain and
feeling as if they are a burden
Drug and alcohol use increases
Anxiety, restlessness, agitation, recklessness and
withdrawal
Sleep disturbance
Rage or mood swings
11Assessment and Prevention
45% - 60% of all people who died from suicide
saw their PCP within one month of their death.
Perform a suicide risk assessment on every
patient at risk, and especially those on
antidepressants!
Barriers and challenges to assessment.
This represents an area of training that bears
more emphasis in preparing PCPs
(York, 2011).
Get talking
Open discussion about suicide can be helpful
and will not give the person ideas or push them
to do it.
Most suicidal people do not want to die.
Relationship with PCP = trust and respect.
Who should be screened?
Anyone being seen for depression or with a
history of depression – (ask at EVERY visit)
Alcohol use problems and/or history
Anyone receiving catastrophic news; recent
diagnosis
Exhibiting significant change in mood; appetite;
sleep; and/or anxiety
12Acute Risk Factors
3 As
Alcohol abuse
Attention (or concentration) impairment
Awake (insomnia)
3 Ps
Panic attacks
Pleasure (diminished)
Psychic anxiety
IS PATH WARM
Ideation Hopelessness
Substance abuse Withdrawal
Purposelessness Anger
Anxiety Recklessness
Trapped Mood changes
https://www.uptodate.com/contents/suicidal-ideation-and-behavior-in-children-and-adolescents-evaluation-and-management
Don’ts as a Provider
Sound shocked or become emotional
Shame them
Give advice
Debate whether suicide is right or wrong
Offer confidentiality
Change the subject
Ask “why” questions
https://www.suicideline.org.au/resource/supporting-someone-you-know-thinking-suicide/
Retrieved 07/19/18
13APNA Suicide Competencies for
Nurses
Understands the phenomenon of suicide
Manages personal reactions, attitudes and beliefs
Collaborative and therapeutic relationship with the patient
Accurately assesses and communicates with team and
appropriate persons
Risk assessment
Adjusts plan of care with continuous assessment
Assesses and modifies environment
Understands legal and ethical issues
Document
A quick note about antidepressants
See patients for follow-up in two weeks if at all possible,
or at least contact by phone personally. This should be
done any time a medication is started or the dose is
adjusted. This is beyond the time we have today.
Give the medications time to work (STAR-D study) – if
there is some response increase the dose. If no response
in 2-4 weeks switch to another anti-depressant in the same
class. If no response to the second medication trial –
switch class. Three failed trials – refer.
Highest risk group – adolescent and young adults – frontal
lobe development
Screening
Patient Health Questionnaire (PHQ9)
https://www.ucare.org/providers/Documents/Patie
ntHealthQuestionnairePHQ9.pdf
Columbia- Suicide Severity Rating Scale
http://cssrs.columbia.edu/
Geriatric Depression Scale (GDS)
Designed for primary care patients 65 and older
15 items
Free apps for iPhone and Android
142018 Suicide Screen
Questionnaire for at risk youth
20 second administration
https://www.nimh.nih.gov/labs-at-nimh/asq-
toolkit-materials/index.shtml
In the past few weeks, have you wished you were dead? Yes No
In the past few weeks, have you felt that you or your family
would be better off if you were dead? Yes No
In the past week, have you been having thoughts about killing
yourself ? Yes No
Have you ever tried to kill yourself ? Yes No
If yes, how? When?
Are you having thoughts of killing yourself right now?
The screen is positive –
Now what?
Praise the patient for telling you
Ask about frequency of thoughts
Is there a plan and what is it?
Have they had past suicide attempts?
Symptoms – depression, anxiety
Support and safety
Tell someone
Suicide Hotline # 800-273- TALK
What about No Suicide Contracts
Not valid or legal documents – does not protect
a provider from malpractice lawsuits
No evidence that they work – 65% of suicide
attempters in one study had signed a no-suicide
contract
Establish safety plan instead – What is that?
How is it different from no-suicide contract?
15Safety Planning
Identify warning signs
Identify internal coping strategies
Identify people and social settings that will
provide distraction
Identify people to ask for help
Identify professionals and agencies to contact
for crisis
Identify ways to make the environment safe
Reasons for living
https://suicidepreventionlifeline.org/wp-content/uploads/2016/08/Brown_StanleySafetyPlanTemplate.pdf
Involuntary Commitment
https://www.pinterest.com/pin/511017888940112470
Definitions
Suicidal Ideation – talking about harming
oneself, looking for ways to harm and
talking/writing about death, dying and suicide –
what is the content and the chronicity of the
thoughts?
Suicidal Plan – is there a plan and do they have
access to the planned method?
Suicidal Intent - how likely are they to commit
suicide? What are the stressors, emotional pain
and social support?
16 Dangerous to self – "means a condition of a person
whose behavior, significant threats or interaction
supports a reasonable expectation that there is
substantial risk that he will inflict physical or severe
emotional harm upon his own person.” (LA
definition in mental health law – each state may have
their own definitions)
What does this mean?
Are you assessing everyone that is prescribed
antidepressants for suicidal thoughts every visit?
When is the most dangerous period after initiation of
antidepressants?
What about the person that is ‘chronically suicidal’?
Dangerous to others - “The condition of a person's
behavior or significant threats support a reasonable
expectation that there is substantial risk that he will
inflict physical harm upon another person in the
near future"
What does that mean to you?
Are you asking about it when assessing a patient?
Anyone that you suspect of suicidal ideation, should also
be asked about wanting to harm others.
Who else might need to be asked with this?
Gravely disabled – "means a condition of a person
who is unable to provide for his own basic physical
needs, such as essential food, clothing, medical
care, and shelter, as a result of serious mental
illness or substance abuse and is unable to survive
safely in freedom or protect himself from serious
harm; the term also includes incapacitation by
alcohol, which means a condition of a person who,
as a result of the use of alcohol, is unconscious or
whose judgment is otherwise impaired that he is
incapable of realizing and making rational decision
with respect to his need for treatment”
17 What does that mean?
Does it include persons who do not take care of
hygiene?
What about homeless people?
Does the fact that someone hallucinates qualify?
What about someone who is delusional? Does
the content of the delusion matter?
Person with mental illness – "any person with a psychiatric
disorder which has substantial adverse effects on his ability to
function and who requires care and treatment. It does not refer
to a person with, solely, an intellectual disability; or one who
suffers solely from epilepsy, alcoholism or drug abuse.”
Treatment facility – "any public or private hospital, retreat,
institution, mental health center, or facility licensed by the state
in which any person who is mentally ill or person who is
suffering from substance abuse is received or detained as a
patient.… Shall be selected with consideration of first, medical
suitability; second least restriction a person's liberty; third,
nearness to the patient's usual residence; and forth, financial or
other status of the patient, except that such consideration shall
not apply to forensic facilities. “
Forced administration of medications – “Medications may
be administered without the patient's consent and against
their wishes in a situation where in the judgment of the
physician who observes the patient during an emergency
which places the patient or others at significant or imminent
risk of damage to life or limb. This may not be done for
longer than 48 hours except on weekends or holidays during
which 24 additional hours may be allowed. There must also
be an effort to consult with a primary care provider at the
early time within 48 hours.”
What is your state law on these concepts?
What about ICU patients?
18How to know when to hospitalize
Suicide attempt – especially with highly lethal
method, steps to avoid detection, disappointment
that the attempt was not successful
Inability to discuss an attempt and precipitating
factors
Not able to participate in safety planning
Agitation, impulsivity and/or severe hopelessness
Lack of social, emotional and even spiritual support
NOTE: no studies show that hospitalization
prevents future suicides
Know your state laws on
involuntary confinement
What does your state do?
How are APRNs involved? Any barriers to their
involvement?
So what I am supposed to do then?
Safety planning is preferred –
Making sure home environment is safe – no firearms, extra
pills, etc
Identifying warning signs
Collaborating with the patient to come up with ways to
cope with suicidal thoughts on their own
Identify potential family and friends that can be contacted
and contact them! (I will do this in front of the patient)
Identifying mental health resources
Collaborate with other health care professionals
19Outpatient Treatments
Best option for lower risk individuals
By all means though, create a safe environment
and involve the family in monitoring the patient
until they are further stabilized. Educate them
about using the ED if needed
Encourage avoidance of alcohol or drugs
Mental health follow-up within 48 hours if
possible
Tarasoff and duty to warn
1974 case in California when P Poddar told a
university psychologist of his intent to kill a woman
identified as T. Tarasoff.
The psychologist did not warn the woman or her
family, but did notify police who interviewed
Poddar. The police warned him to stay away from
Tarasoff.
He later murdered Tarasoff with a knife.
The provider has a duty to warn the individual, as
well as law enforcement according to the decision
Don’t forget
Take care of you!
If a patient does suicide, you need to deal with
your own vicarious trauma
Consult with legal or malpractice attorney if you
are concerned
20Do you commit?
John is 27 years old and voluntarily homeless.
He has been diagnosed in the past with
schizophrenia. He presents to your office
relatively clean, oriented in all spheres, denies SI
or HI, but does report auditory hallucinations.
He reports that these are no different than ones
he has had in the past and denies that they are
telling him to do ’bad things’. His mom, is
concerned.
Do you commit?
Shelly is an 18 year old college freshman who
has been up for 36 hours studying for her final
exams. She reports that she will just have to
‘jump off the bridge’ if she does not pass her
Nursing 200 course. She is jittery and has no
history of depression or suicidal behaviors.
Do you commit?
Pete is angry with his neighbor Paul. He says
that he has come on to his property and taken
his apples for the last time. If he does it again,
he will have to get his shotgun out and fill it
with rock salt to go after him.
Would your decision be different if Pete was just
angry with unknown thieves?
21Do you commit?
59 y/o female presents to clinic with multiple
somatic complaints; much focus on insomnia,
pain, low energy, increased anxiety. Recent
financial stressors, new medications prescribed
for co-morbidities, family stress.
Made several passive comments regarding not
wanting to live anymore. Avoids subject when
asked directly about SI; laughs and attempts to
change subject.
QUESTIONS?
Selected References
Administration on Aging (AoA) (2017)
https://www.usa.gov/federal-agencies/administration-on-
aging
Freeman, S. (2011). Suicide assessment: Targeting acute
risk factors. Current Psychiatry. 11(1), 57.
Kennebeck, S. & Bonin, L. (2017). Suicidal ideation and
behavior in children and adolescents: Evaluation and
management. Uptodate.
https://www.uptodate.com/contents/suicidal-ideatin-and-
behavior-in-children-and-adolescents-evaluation-and-
management
Substance Abuse and Mental Health Services
Administration (SAMSHA) (2017). https://www.samhsa.gov/
U.S. Department of Health and Human Services (HHS)
Office of the Surgeon General and National Action
Alliance for Suicide Prevention. (2012). 2012 National
Strategy for Suicide Prevention: Goals and Objectives
for Action. Washington, DC: HHS, September 2012.
York, J., et al. (2012). A systematic review process to
evaluation suicide prevention programs: A sample case of
22You can also read