SYMPOSIUM 3RD MYVET HOSPITAL GROUP - MAKARANGA LODGE 09 FEBRUARY 2020 - INANDA VETS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

VETERINARY SYMPOSIUM 2020
3rd MyVet Hospital Group
Symposium
Makaranga Lodge
09 February 2020
Editors: Dr Anthony Zambelli & Ms Amanda Shaw
Master of Ceremonies: Dr Kenneth Joubert
1
VETERINARY SYMPOSIUM 2020
Dear Colleagues,
Welcome to our third annual veterinary symposium. My team of dedicated staff, led by Ms
Amanda Shaw, has assembled a useful, coherent and I am sure you will find, enjoyable series
of “upskills” for all attendees. Every year we analyse the feedback you give us, to select topics
that you want to learn about. There’s obviously more than we can cover in one day, so the
choices are very difficult. This year we have chosen to focus on the head, neck, skin and
endocrinology – both medical and surgical.
Dr Kenneth Joubert will be our MC this year, guiding us through the topics of the day, and
welcoming a new speaker – Dr Sara Boyd, a specialist surgeon with over two decades of
experience – who has joined our group. We remain, as ever, dedicated as a group, and with
our visiting consultants, to assisting your practice to extend your service and veterinary
capabilities. Any practice in KZN should be able offer its clients and patients some hope, help
or treatment, that is already available to humans – even without hiring new staff or investing
in expensive equipment. We are here to be an extension of your practice, and we strive to
constantly improve our service offering to you, and with you.
The veterinary healthcare industry in SA is under enormous stress at the moment, as well as
having increasingly demanding clients presenting us with a progressively first-world (aging)
pet population with more chronic illnesses, as well as some local combinations such as
infectious diseases and skin cancer. We must rise to these challenges using the skills and
tools available to us. Our corporate sponsors make this sort of learning opportunity possible,
provide aftercare and tech support, and the products we use, to achieve our goals – they make
us more versatile, flexible and responsive to our pets’ needs. Please thank the representatives
of Royal Canin, Virbac, Zoetis and IDEXX when you see them, and interact with their staff on
the day, to understand how vets and our support industries can work together.
I particularly want to thank Ms Shaw for months of planning and effort, without which this would
not be possible; Dr Joubert for chairing the sessions; Drs Greenberg, Pimosenco, Ruiz and
Boyd, for their time spent on developing lectures and notes; my staff for assisting on the day;
Makaranga Lodge for hosting us yet again; and all of you for supporting us, working with us,
telling us what you need, and helping us grow from a small practice of 6, to a group of over 50
staff. We look forward to many years collaboration for the betterment of all our mutual clients,
our profession and the pet healthcare industry.
Welcome, with sincere thanks
Anthony Zambelli
Director, MyVet Hospital Group
Inanda Veterinary Specialist Centre
2
VETERINARY SYMPOSIUM 2020
Agenda
09.00 - 9.30am - Arrival and Registration
“Practical Tips and Techniques for Surgery of the Head: Ear, Nose and Throat” – pg 9
Dr Sara Boyd
“Oral Tumours: From diagnosis to Treatment. What to Expect.” – pg 17
Dr Jose Ruiz
~Tea~
“Secrets to Success in Dermatology”– pg 33
Dr Anthony Zambelli
“Case Based Approach to Endocrine Conditions” – pg 51
Dr Arina Pimosenco
Royal Canin’s Gastrointestinal Range: What to Use and When
Dr Michelle Harman
~Lunch~
“Canine Behaviour Disorders Influenced by Owners & Environment” – pg 63
Dr Melvyn Greenberg
“How Do We Become the Best Vet/Vet Nurse We Can be?” – pg 67
Dr Kenneth Joubert
16.05pm – Closing
3
VETERINARY SYMPOSIUM 2020
4
VETERINARY SYMPOSIUM 2020
Speakers
Dr. Sara Boyd
BVsc MMedVet (Surgery)
Sara was born and grew up in Johannesburg, South Africa. She
graduated in 1997 from Onderstepoort Veterinary Faculty with a
BVSc. After working in the UK for 2 years, she returned to
Onderstepoort as a surgical resident and later, a senior lecturer. She
completed her MMVedVet degree in April 2004. She has been an
owner and partner in Johannesburg Specialist Veterinary Centre for
the past 20 years, prior to going on her own as a consulting Specialist
Small Animal Surgeon. Sara is involved in presenting CPD courses
both in South Africa and abroad. Her special interests lie in the field of
soft tissue and neurosurgery.
She remains proficient in the field of Orthopaedics and is one of the
few South African surgeons regularly performing TPLO and Canine Cementless Total Hip
Replacement. She is married to Mark Boyd and has 3 children.
Dr. José Carlos Almansa Ruiz
DVM (Hons) MSc (Vet), Resident, Veterinary Dentistry
Member of the Royal College of Veterinary Surgeons
José is originally from Spain. He qualified from the
Universidad Complutense de Madrid in 2008. Thereafter
he completed his honours degree in dentistry and
maxillofacial surgery while working in a busy afterhours
hospital in Madrid. In 2009, he relocated to Pretoria
where he undertook an internship in dentistry and
maxillofacial surgery under Prof. Gerhard Steenkamp for
18 months, while concurrently undertaking an MSc
degree.
In 2011, he relocated to the UK where he worked in the
greater London area working as a general practitioner
and getting referrals in dentistry and maxillofacial surgery from Kent and Surrey areas. In
2012, he started his European Diploma in Veterinary dentistry through the alternative pathway
under the supervision of Dr. Lisa Milella, for which he is hoping to submit his credentials in this
year.
In 2014 he completed the AOVET Course-Masters in Operative Treatment of
Craniomaxillofacial Trauma and Reconstruction. In 2015, he moved back to South Africa, this
time to Cape Town, where he joined Tygerberg Animal Hospital as a veterinarian with a special
interest in Dentistry and Maxillofacial surgery. At the beginning of 2017 he moved back to
Pretoria where he joined VetDentSA. He is a consultant for Inanda Veterinary Hospital in
Durban and Tygerberg Animal Hospital in Cape Town. José has a special interest in Wildlife
Dentistry and Maxillofacial surgery where he is an active researcher. He has presented in
national and international congresses.
5
VETERINARY SYMPOSIUM 2020
Dr. Kenneth Joubert
BVSc MMed Vet (Anaes)
Kenneth graduated with a BVSc from The University of Pretoria in
1995. After graduating he joined small animal practice in
Johannesburg for 2 years before returning to the University of
Pretoria. In 2000 he obtained a MMedVet (Anaes) and held the
position of senior lecturer in anaesthesiology at the university. In
2004 he left the university to re-join private practice before starting
his own referral practice in anaesthesiology, pain management
and critical care. Kenneth has published 37 scientific publications,
delivered 80 scientific presentations, delivered 142 continuing
education talks, done 14 multimedia presentations, published 39
non-scientific articles, presented 7 course, written one book
chapter and attended 66 congress of continuing education.
Kenneth currently holds an extra-ordinary lecturing post in
Pharmacology in the department of Paraclinical Sciences at the University of Pretoria and runs
a private practice dedicated to anaesthesia, analgesia and intensive care. He has regularly
examined students in pharmacology, anaesthesiology and clinical studies. Kenneth has and
is currently involved in the supervision of 4 students. Kenneth has a keen interest in total
intravenous anaesthesia, intensive care, ventilation and cardiology. His research interests
included non-steroidal anti-inflammatory agents, anaesthetic depth monitoring and total intra-
venous anaesthesia.
Kenneth chaired the Faculty Ethics Committee (Animal Use and Care Committee) until it was
dissolved to form a University based Animal Use and Care Committee. I was then a member
of the Senate committee for Research Ethics and Integrity and the Animal Use and Care
Committee of the University of Pretoria. Kenneth currently serves on the AUCC (RECA)
Nelson Mandela Metropolitan University and the Ethical Review Group of the AVA. He is also
a member of the Education Committee and the Standard Committee of the South African
Veterinary Council. In 2019 he joined Inanda Veterinary Hospital.
Dr. Arina Pimosenco
DVM cum laude BVSc(Hons)
Arina qualified as a veterinary surgeon cum laude in 2007 in Eastern
Europe. She has worked in Johannesburg suburbs mostly with
small animals from 2009 to 2016. She also completed her Honours
Degree in Veterinary Medicine, Clinical Pathology and Radiology in
2014 from Onderstepoort. Arina likes challenging diagnostics and
endless opportunities of veterinary medicine to help our furry family
members. She joined Inanda Veterinary team in May 2016 and has
been privileged to work for Veterinary Medicine Specialist
Dr Anthony Zambelli, where she continues professional development in the veterinary field of
choice. Arina is currently doing Advanced Practitioner course in Small Animal Medicine with
European School of Veterinary Postgraduate Studies (ESVPS) and Harper Adams University
in UK.
6
VETERINARY SYMPOSIUM 2020
Dr. Melvyn Greenberg
BVSc
Melvyn Qualified with B.V.Sc. at Onderstepoort in1973,
receiving the Pfizer Clinics Prize in final year. He has been a
Small animal private practitioner since January 1974 with a
special interest in animal behaviour from the outset. He
received the Boswell Award from the SAVA in 1995 and the
Rick Massey Trophy from the Witwatersrand Branch of the
SAVA in 1999 for outstanding service to the veterinary
profession, and he co-founded the Animal Behaviour
Consultants Group in 1994 due to the plethora of behaviour
disorders amongst pets, hoping that all qualifying consultants “talk the same language”.
He also hosted a Pet Care line, initially as Capitol Vet on Capitol Radio, then as Dr Platzhund
on Radio 702 (and later Cape talk) over a period of 22 years – borne, initially, out of the need
to advise the public on how to prevent dogs from biting people. He was the first veterinarian
to conduct puppy socialisation classes at the veterinary practice level, and then helped
promote it nationwide. He is the author of Dr Platzhund’s Pet Pointers, published in 1998
containing close to two dozen common pet-related problems but has also written thousands
of articles in hundreds of local and national printed media, on behaviour issues, over 33 years
He has been an invited guest on animal related issues on many television programmes
throughout the country which included a personal 13 -episode series The Creature Feature.
He was an expert witness in 18 serious court cases involving canine aggression causing
human injury, mutilation or death, and was initially a resident advisor to Mutual & Federal and
then to the legal fraternity at large.
Dr. Anthony Zambelli
BSc(Hons) BVSc DiplSnrMgmt MMedVet(Med) (cum laude)
Anthony qualified as a vet in 1998, concurrently completing
the intercalated honours degree in Zoology from Wits in
1995. After 5 years in private practice in the UK, during
which time he completed the fast-track MBA certificate and
diploma courses in senior management through the Open
University, he returned to SA to undertake specialist training
and a lectureship at OP. He completed his MMedVet(Med)
in 2006, graduating cum laude in 2008. He started in private
practice in 2006, before branching out to start up Inanda
Vets in 2011. With Dan Ohad and Remo Lobetti he
completed a long term study in Boerboel Cardiomyopathy,
as well as a study on hypertriglyceridaemia in Miniature
Schnauzers. He is currently a student of UNISA, in his 4th
year of a degree in Chemistry and Archaeology.
7
VETERINARY SYMPOSIUM 2020
(notes)
8
VETERINARY SYMPOSIUM 2020
Practical Tips and Techniques for
Surgery of the Head: Ear, Nose and
Throat
Dr Sara Boyd BVSc MMed Vet (Surgery)
INTRODUCTION
Surgery of the “head” is a very wide based topic, however it encompasses commonly
presenting conditions, many of which can be adequately addressed in a general
practice type set-up. The aim of this talk is to try and provide some practical treatment
tips for these cases; it will cover the principles of surgical ear techniques that are
available, surgery of the external nasal passages and surgery of the oral cavity and
soft tissues of throat. Oral tumours and their treatment does not fall within the scope
of this talk and is addressed as a separate topic in this symposium.
Ear
A large number of conditions that affect the ear do not require surgical intervention;
however, surgery may be required in the presence of severe recurrent ear disease
that is refractory to medical treatment, if condition involves neoplasia or if owner
compliance is lacking. End stage ear canals often require surgical intervention and
three surgical procedures have been well described in the definitive treatment of Otitis
Externa (OE) in both dogs and cats. The aim of all of them is similar: to remove the
source of the infection and to improve ventilation and drainage of the ear canal.
Surgical anatomy: The
external ear canal is a
cartilage tube that
extends from the
external auditory
meatus on the skull to
the external pinnae. It
consists of a short
vertical canal and a
slightly longer horizontal
canal which ends at the
tympanic membrane. It
is lined by epithelium
that is continuous with FIGURE 1. SCHEMATIC DIAGRAM OF THE SKULL ANATOMY AND
the skin and therefore TYMPANIC BULLA OF THE DOG
9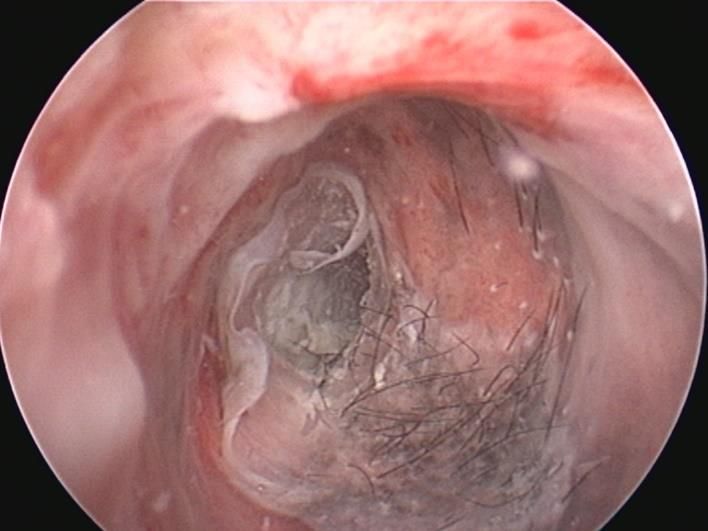
VETERINARY SYMPOSIUM 2020
prone to the same conditions and allergies that the skin suffers from. The tympanic
bulla or middle ear lies on the medial aspect of the ear drum and contains the auditory
ossicles. It also has the sympathetic nerve running through it and the hypoglossal
nerve and external carotid artery running directly ventral to it. The facial nerve runs
just caudal and ventral to the external auditory meatus and is very prone to injury
during surgery, especially with chronic ear disease. The last structure that may be
damaged during surgery is the Retroglenoid vein which lies rostral to the tympanic
bulla. This causes significant haemorrhage at the time of surgery but has no long term
ill-effects. In cats the tympanic bulla has two distinct compartments, a larger ventro-
medial one and a smaller dorso-lateral one. The medial portion of the ear canal is the
inner ear which lies in the petrous part of the temporal bone. When this is affected
more serious clinical and vestibular neurological signs may be present.
The most commonly executed surgical procedures for the treatment of chronic Otitis
Externa and media include: a lateral ear canal ablation, vertical ear canal ablation,
ventral bulla osteotomy (VBO) and lastly a total ear canal ablation (TECA) together
with a lateral bulla osteotomy (LBO). This is fondly known as a TECABO!
Lateral Ear Canal Resection: This is the resection of the lateral wall of the vertical ear
canal in order to facilitate air flow and drainage and allow better access to the rest of
the ear canal for topical treatment applications. The modified version where a cartilage
drainage plate is created to prevent hair growth around the opening is known as the
Zepp’s procedure. The procedure, although popular is rarely successful as it often fails
to remove the underlying cause. One exception to this is in the presence of an isolated
lesion on the lateral wall of the vertical canal.
Vertical Ear Canal Ablation: This is similar to the above procedure but requires
dissection and resection of the entire vertical canal. Again, its indications are limited
to those conditions that only affect the vertical canal. It does create a much better
cosmetic appearance than that of a lateral wall resection.
Ventral Bulla Osteotomy: This procedure is designed to provide drainage at the most
ventral portion of the tympanic bulla. The indications are for primary conditions of the
middle ear where an intact ear drum and a normal external ear canal exist and for
failed TECA procedures. It requires technically difficult dissection, especially in the
dog. In cats is the procedure of choice for removing inflammatory polyps and the entire
lining of the tympanic bulla.
Total Ear Canal Ablation and Lateral Bulla Osteotomy: This is a salvage procedure,
but is by far the most effective surgical treatment for end-stage ear canal disease. End
stage ear canals have the following characteristics: hyperplasia of the epithelium,
hypertrophy of the glands, collapse and/or stenosis of the horizontal part of the ear
canal, calcification of the peri-auricular soft tissue. Many of these cases also have a
ruptured tympanic membrane and concurrent otitis media. By removing the entire
lining of both the external ear canal and the tympanic bulla, TECA/LBO provides a
definitive cure for these animals. It is however a complicated procedure with serious
10VETERINARY SYMPOSIUM 2020
potential complications if it is performed by someone who is not totally familiar with the
anatomy of this area. Described complications of this surgical procedure include:
fascial nerve palsy, vestibular syndrome, Horner’s syndrome (in cats), chronic
recurrent draining sinus tracts and poor carriage of the external pinnae.
Nose
Many of the nasal and oral issues mentioned above: fall under the category of Upper
Airway Obstruction Syndrome (UAOS) or Brachycephalic Airway Syndrome (BAS)
and refers to a combination of problems causing partial or complete obstruction to the
upper airway. Breeds commonly affected include: English and French Bulldogs,
Boxers, Boston Terriers, Pug and Staffordshire Bull Terriers. These breeds all have
the typically compressed face characterised by an inherited developmental defect
where facial bones grow to normal width, but reduced length. The soft tissues of the
head are not proportionately reduced and are often even redundant. The components
of BAS include: stenotic nares, elongated soft palate, everted laryngeal saccules and
tracheal hypoplasia.
Stenotic nares are visually apparent and easy to diagnose. Observing the external
openings during inspiration, we can clearly see whether there is paradoxical closure
as the animal inspires. Sneezing, inspiratory stridors or mucopurulent discharges are
further clues to stenotic nares. Other causes of nasal obstruction include traumatic,
neoplastic, foreign body inhalation or infectious causes of nasal disease.
Stenotic nares are found frequently in Brachycephalic breeds. Although a minor
component of the syndrome, having insufficient external passage for air causes
animals to open-mouth breathe and increases respiratory flow rates through the rest
of the airway. The surgical repair is not technically demanding, it consists of performing
bilateral wedge naroplasties. It is important that these wedges are sufficiently deep to
open the nares at least 7-10mm into the nasal passages. Fine absorbable suture
material is used to close the defects and haemorrhage is usually easily controlled.
Mouth and Lip Surgery
Many simple reconstructive techniques are available to repair (sometimes substantial)
defects to the nasal and lip region. Resection of tumours is another prime indication
for these types of procedures. Techniques used may be as simple as accurate
anatomical reconstruction or as complicated as lip to lid transposition flaps. During the
presentation, a variety of clinical cases will be used to demonstrate the techniques. At
all times it must be remembered that the lips and mouth are a highly mobile structures
and adequate tension relieving techniques are essential to their success. On the
upside: these oral cavity of blessed with a prolific blood supply, so healing is fast and
patient morbidity low.
11VETERINARY SYMPOSIUM 2020
Throat
Staphylectomy is the resection of an elongated soft palate. This is performed via an
oral approach and aims to remove excessive tissue so that the obstruction to the
dorsal glottis is removed. The excessive tissue is clamped and sharply resected. A
monofilament absorbable suture material in a continuous pattern is used to close the
defect. Intraoperative haemorrhage and oedema, as well as the post-operative risks
of dog developing obstruction from the surgery are further causes for concern. More
advanced techniques for resection using laser excision has been performed
successfully, however the equipment needed is expensive and not readily available.
Further upper airway obstruction can be caused by eversion of the laryngeal ventricles
into the opening of the glottis. These ventricles are mucosal diverticulae that are
situated rostal and lateral to the vocal folds. When excessive negative pressure is
experienced within the upper airway, these ventricles tend to evert towards the midline
and become extremely oedematous. They then block the lower half of the airway at
the level of the laryngeal glottis. Many affected animals have a combination of the
above conditions which can lead to a decrease in glottis aperture of as much as 80 to
90%. Surgical correction is straight forward resection of the distal saccules, which is
only hindered by difficulty with visualisation due to caudal position and presence of an
ET tube.
Stabilising the patient in respiratory distress
The classic signs of acute respiratory distress include open mouth, laboured breathing,
cyanosis, abducted forelimbs, restlessness and even collapse. Animals exhibiting
these signs should be handled with care so as not to compromise them any further.
Removing them from their distressed owners and taking them to a cool, quiet
environment where oxygen supplementation can be administered, is the first important
step. Supplementary oxygen can be started immediately. Concurrent hyperthermia is
common and cooling techniques including icepacks in the axilla, inguinal area or on
the extremities or surrounding the IV line should be employed. Wetting the animal and
directing an electric fan on them, may also help to bring the body temperature back to
normal. Before physical examination is possible, the dog may require a sedative like
Buprenorphine and possibly even treatment with a short acting, IV corticosteroid. They
should be allowed to remain unrestrained and, in the position that they find most
comfortable.
In more severe cases, where laryngeal oedema has developed, the veterinarian may
have to consider endotracheal intubation or even an emergency tracheostomy. IV fluid
administration is not usually necessary in the immediate stabilisation and care should
be taken, if administered, not to overhydrate the already compromised lungs.
Establishing the cause of the respiratory distress
By assessing the abnormal respiratory sounds at various levels, we can gain clues as
to the underlying origin of the obstruction. It is important to note at his point that
12VETERINARY SYMPOSIUM 2020
animals should never make a noise when breathing. Even young animals which
present with noisy breathing, must have some form of obstruction. This should be
recognised by veterinarians and corrected as early as possible.
Gentle pressure over the laryngeal area often exacerbates respiratory compromise at
the level of the larynx. Auscultation is useful for localizing the obstruction to this region.
A characteristic inspiratory stertor, is a common finding in laryngeal obstruction cases.
Once the problem has been isolated to the larynx, survey radiographs of the laryngeal
region are useful and should accompany the standard views of the thoracic cavity.
Routinely, radiographs are followed by a full visual examination of the laryngeal region
with the animal lightly anaesthetised. This helps differentiate laryngeal paralysis from
laryngeal collapse, elongated soft palate or everted laryngeal ventricles.
Visual examination of the upper airway
These patients are considered anaesthetic risks and every precaution should be taken
to make sure that they survive the initial diagnostic procedures. Laryngeal function can
be inhibited by certain drugs and these should be avoided if an accurate assessment
of laryngeal function is to be made. Preoxygenation of affected dogs for 3-5 minutes
with 100% oxygen prior to induction can significantly decrease risks. Propofol is
generally used as the author’s induction agent of choice, as it has the advantage of
having a very short half-life. The animal should only be anaesthetised to the level
where the tongue can be retracted, but the swallowing mechanism is not affected.
Tongue should not be pulled too forcefully, as this can give a false under-estimation
of the length of the soft palate. Endotracheal tubes and oxygen supplementation are
always on hand and in case blood oxygen saturation levels cannot be maintained.
An accurate light source and a long tongue depressor or laryngoscope is required in
order to assess the length of the soft palate in relation to the tip of the epiglottis. The
normal guideline is that a 1-3 mm overlap is acceptable. In the case of an elongated
soft palate, there may be as much as a 12-20mm overlap. In English Bulldogs, this
redundant soft palate tissue may also be exceedingly thick.
The soft palate should then be elevated to visualise the entrance to the glottis. This
allows the relationship between the corniculate and cuneiform processes of the
arytenoid cartilages to be assessed. Any contact or overlap between them, may
indicate a degree of concurrent laryngeal collapse.
During inspiration, it is important to establish whether the vocal cords are abducting
appropriately. In the case of laryngeal paralysis, the vocal folds cannot be adequately
abducted and so they obstruct the laryngeal glottis. This exacerbates the negative
pressure within the airway and leads to a vicious cycle of respiratory obstruction and
eventually upper airway collapse. A useful aid in confirming whether paralysis is
present or not, is to inject the animal with Doxapram (Dopram) at a dose of 0.5-2 mg/kg
IV whilst observing the vocal folds for movement. The increased respiratory effort that
occurs when Dopram is given, makes it easier to see whether there is adequate
abduction and exacerbates paradoxical movement.
13VETERINARY SYMPOSIUM 2020
If all of the above structures appear within normal limits and no obvious cause for the
respiratory obstruction can be identified, then endoscopy of the trachea and bronchi
is indicated.
CONCLUSION
Surgery of the head is one of the few places where simple techniques and
unsophisticated equipment can be used in first opinion practices to significantly
improve outcomes. The golden rules are that surgeons make a correct diagnosis,
understand the aim of the technique and follow sound surgical principles in the
correction of the initial condition.
REFERENCES
1. Fossum TW. Surgery of the upper respiratory system. In: Fossum TW. Small
Animal Surgery (4th). Missouri: Elsevier Mosby:2013: 906-957.
2. Fasanella FJ, Shivley JM, Wardlaw JL et al. Brachycephalic airway obstructive
syndrome in dogs: 90 cases (1991-2008). J Am Vet Med Assoc 2010;237:1048.
3. Hedlund CS. Surgical management of brachycephalic syndrome. In: Bojrab MJ.
Current Techniques in Small Animal Surgery (4th): Pennsylvania: Williams and
Wilkens: 1998: 357-376.
4. Poncet CM, Dupre GP, Freiche VG, et al. Long term results of upper respiratory
syndrome: surgery and gastrointestinal tract medical therapy in 51
brachycephalic dogs. J Small Anim Pract 2006;47:137.
5. Riecks TW, Birchard SJ, Stephens JA. Surgical correction of brachycephalic
syndrome in dogs: 62 cases (1991-2004). J Am Vet Med Assoc 2007;230:1324.
6. Torrez CV, Hunt GB. Results of surgical correction of abnormalities associated
with brachycephalic airway obstruction syndrome in dogs in Australia, J Small
Anim Pract 2006:47: 150.
14VETERINARY SYMPOSIUM 2020
15VETERINARY SYMPOSIUM 2020
(notes)
16VETERINARY SYMPOSIUM 2020
Oral Tumours: From Diagnosis to
Treatment. What to Expect.
Dr. José C. Almansa Ruiz DVM (Hons) MSc (Vet)
EVDC Resident, Board Ready
Malignant Oral tumours represent 6-7% of all the tumours diagnosed in canine
patients; the incidence is lower in cats. Oral neoplasms should be differentiated from
inflammatory processes, infection, and developmental or congenital lesions. A variety
of odontogenic and non-odontogenic tumours occur in the oral cavity. These
neoplasms may appear as ulcerated, non-healing lesions or a more conventional
mass-like structure. The pet owner more readily notices lesions when they occur in
the rostral aspects of the maxilla or mandible. Encouraging clients to brush their pets
teeth will also help for them to “keep an eye” in their pets oral health. Unfortunately,
pet owners only generally notice these neoplasms when they are in an advance stage
of development. Hence, the important to act quickly when is first presented to the
general practitioner.
Staging the oral neoplasia:
On the initial presentation, a conscious examination of the mass is performed if the
patient allows it, although an examination under general anaesthesia is still required
as part of the clinical staging of the tumour. Part of this initial assessment of the patient
must always include a CBC, biochemistry panel and in older patients a urine analysis.
The TNM system is used to stage these lesions (See addendum). During the clinical
assessment of the lesion, features like ulceration, mobility, size, location, consistency,
are important for the pathologist to give us a more accurate diagnosis. Part of the
staging involves evaluation the regional lymph nodes bilaterally. The mandibular
lymph nodes are the only regional lymph nodes superficial enough to be palpated,
during this process size and mobility must be recorded. Enlargement of the lymph
node does not necessarily mean local metastasis, but also could be a reactive lymph
node. The absence of mobility may be an indicator of the invasion of the lymph node
capsule by the tumour. A study performed by Williams et al (2003) reported on 100
cancer patients undergoing clinical examination of the lymph nodes and
lymphadenectomies, reported that 70% of cases with Lymphadenomegaly had
metastatic disease and 40% of cases without lymphadenomegaly had metastatic
disease (Williams / Packer 2003).
17VETERINARY SYMPOSIUM 2020
Lymph nodes can also be evaluated using contrast-enhanced CT imaging, one study
looked at the diagnostic accuracy of CT for determining metastatic mandibular and
medial retropharyngeal lymph nodes in dogs with either nasal or oral cancers reporting
a sensitivity of 12.5 and 10.5%, and the specificity was 91.1 and 96.7%, for mandibular
and medial retropharyngeal lymph nodes, respectively. Due to the low sensitivity,
contrast-enhanced CT imaging is not a reliable tool to predict lymphnode metastasis.
Guided ultrasound fine needle aspiration permits sampling of the mandibular,
retropharyngeal and parotid lymphocentres; the withdraw of this practice is the
possibility of missing microscopic metastatic disease if no gross lesions are present in
the sampled lymph nodes. More recent studies have confirmed the lesser reliability of
FNA assessing metastasis, with one study reporting 77.2% accuracy in dogs and cats
and another reporting an incidence of 72.8% and 85.9% diagnostic samples in dogs
and cats, respectively (Ku/Kass 2017 and Amore-Fuster/Cripps 2015). Furthermore,
things get a little bit complicated when evaluating metastatic disease in melanocytic
tumours due to the difficulty to differentiate melanocytophages from melanocytes in
the regional lymphnodes.
Billateral lymphadenectomy of the medial retropharyngeal and mandibular
lymphocentrums reported an incidence of metastatic disease in 48 canine patients
suffering from oral melanoma and oral squamous cell carcinoma of 33% in at least
once lymphocentrum (Grimes/Mestrinho 2019). Odenweller et al evaluated metastatic
disease in 98 dogs and 10 cats presented with oral and maxillofacial neoplasms;
unilateral excisional biopsies were performed, including the parotid lymphocentrum,
reporting an overall metastatic rate of 14%. Of the cases with metastatic disease,
26.7% did not involve the mandibular lymphocentrum. Hence, the importance of not
to rely only on the palpation, aspiration or biopsy of the mandibular lymphocentrum.
To date no clinical studies have reported a correlation between performing unilateral
or bilateral lymphadenectomies and the survival times. It is the author’s opinion that a
more aggressive treatment can be instated based on a more accurate staging.
Imaging can be used to assess the extent of local disease and response to treatment,
identify lymph nodes that may have metastatic disease, screen distant organs for
possible metastasis, and allow image-guided sampling of suspected neoplastic
lesions. Choosing the best imaging technique for a patient depends on several factors
including where and what is being imaged, what information is needed, and also
sometimes cost of the imaging procedure to decide on a best course of action for an
individual patient. Computed tomography is routinely used in maxillofacial surgery to
evaluate the invasion of bone and extension into adjacent structures; it also helps
determine if a tumour is resectable and helps the surgeon to map the osteotomy sites.
These reconstructions are also a great education tool for clients, this way they can
“see” what has been planned surgically for their pet and they feel more confident about
the procedure. If the mass is not resectable, and radiation therapy is indicated, i.e
nasal adenocarcinomas, the CT is extremely important to plan it. The CT scan /
radiographs of the thorax should be done using positive pressure ventilation. CT has
been found to be significantly more sensitive than thoracic radiographs for detecting
18VETERINARY SYMPOSIUM 2020
soft tissue nodules. Only 9% of CT-detected pulmonary nodules are identified on
thoracic radiographs The lower size threshold is approximately 1 mm to detect
pulmonary nodules on CT images and 7–9 mm to reliably detect nodules on
radiographs.
Some authors recommend abdominal ultrasound as part of the initial work up; the
reasoning behind it is that in 3% of oncology patients additional synchronous tumours
may be present (Rebhun JAAHA 2010 / Bigio Vet Comp Oncol 2017/ Magestro Vet
Comp Oncol. 2017).
Obtaining a good biopsy sample is extremely important for the surgical and medical
planning of the patient. The mainstay of planning the biopsy sites relies on diagnostic
imaging, being the gold standard advanced CT imaging (CT or MRI). A good biopsy
must have a representative sample of the most severe, showing more changes area/s
of the lesion. To achieve this, the clinician must select the best biopsy technique, the
correct sample site and submit the sample correctly. The biopsy sample should always
represent the worst part of the mass; this may mean collection of more than one
sample. Biopsying healthy tissue next to the lesion for comparison as in skin biopsies
is contraindicated. The biopsy tract should not transect a healthy tissue plane as
during this procedure neoplastic cells may seed along this tract. It is also advisable to
obtain microbiological samples in case the changes seen were related to infection and
not to neoplasia.
There are two types of biopsy, closed or open, the gold standard in oral and
maxillofacial oncology is open biopsies. The decision to perform an excisional biopsy
is a complex one. This type of biopsy should be reserved to small pedunculated
masses, that their removal would not affect the treatment plan. Incisional biopsies
using a 4-6 mm punch biopsies at a minimum depth of 2 mm are recommended to
biopsy a soft tissue mass. Once the punch is at the desire depth the punch is tilted in
order to “scoop” the sample. These samples should be placed on a clear paper for
1min with the connective tissue facing down on the paper to prevent the sample from
curling during fixation and to help orientate the sample. The sample will then be
transfer to a container with a volume of fixative 20 times more than the size of the
sample to prevent degeneration of the sample. It is the opinion of the author to include
bone when possible into the sample to help the pathologist get a more accurate
diagnosis. Sometimes the mass to biopsy has a mineralized consistency, in those
occasions the use of a chisel and mallet or a michele trephine is indicated to collect a
representative sample.
Epidemiology of common oral neoplasms:
DOGS
Oral tumours in dogs represent approximately 5.4 % of all canine tumours. The
distribution in South Africa based on a study performed between 2000-2008 reported
Osteosarcoma to be the most commonly diagnosed malignant oral neoplasia, followed
by malignant melanoma and squamous cell carcinoma. The incidence of
19VETERINARY SYMPOSIUM 2020
osteosarcoma in the literature is much less, with melanomas, fibrosarcomas and
squamous cell carcinomas being the three most common malignant tumours in the
oral cavity of dogs.
There are several reported risk factors associated to some of these neoplasms. Dogs
living in urban industrialised regions are more predisposed to develop tonsillar SCC
as opposed to rural environments; this may be due to increased exposure to
environmental carcinogens. Canine oral papillomavirus is known to be involved in the
development of oral papillomas in dogs. Furthermore, it is thought that there can be
progression of viral papillomas to carcinomas in dogs. Lastly, oral osteosarcomas
have been reported to develop secondary to exposure to ionizing radiation, a known
carcinogen.
CATS
The proportion of oral tumours is slightly higher with 7.4% - 10.6% of all feline
neoplasms. The most common neoplasia is SCC, comprising 68 - 98% of all oral
malignant tumours. There are several reported risk factors associated with this
neoplasia:
• Flea collars had five times increased risk of developing oral SCC
• Canned food diet (3.6 times increased risk),
• Canned tuna fish diet (> 4-fold increase),
• Exposure to household environmental tobacco smoke (2x increase, not
significant). Bertone JVIM 2003
• Relationship between oral SCC and exposure to household environmental
tobacco smoke, and furthermore implicated p53 as a potential site for
carcinogen-related mutation, with cats exposed to smoke 4.5 times more likely
to overexpress p53 based on evaluation of tumour biopsy samples, and those
exposed for 5 years or longer were 7 times more likely to overexpress p53
(Snyder Vet Path 2004).
CANINE ACANTHOMATOUS AMELOBLASTOMA (CAA)
CAA is a subtype of ameloblastoma that is very specific of dogs. Although considered
a benign lesion that does not metastasize, it has tropism for bone, medular, cortical or
alveolar bone, causing osteolysis and mobility of teeth. The term acanthomatous
means “thorn like”, referring to an internal sheet of interlocking polygonal epithelial
cells reminiscent of the epithelial cells of the stratum spinosum of the skin or oral
mucosa. This feature is unique to CAA.
En-bloc resection is the gold standard of treatment, and is generally curative. It
manifests grossly as a gray to pink, irregular, exophytic, verrucous mucosal mass that
arises immediately adjacent to teeth. It is indistinguishable from peripheral
odontogenic fibroma (POF) / fibromatous epulis of periodontal ligament origin
(FEPLO), squamous cell carcinoma, pyogenic granuloma and gingival hyperplasia;
hence when dealing with a patient with gingival enlargement, it is extremely important
to send for histopathology all the excised tissue. Approximately 50% of CAA occur in
20VETERINARY SYMPOSIUM 2020 the rostral mandible, but they can be found anywhere in the jaws. Golden retrievers are over represented in the biggest study to date in CAA (Goldschmitdt et al JVD 2017). The treatment options are en-bloc resection with 1 cm margins, intra-lesional bleomycin injections and radiation therapy. The author discourages radiating these lesions due to the possibility of transforming them into SCC. SCC DOG It is the 2nd most common oral tumour in dogs 24.5%. Can be found in different sites of of the oral cavity, involving the gingiva, tonsil, oral mucosa, lip and palate. There are two different types with very different prognosis: non-tonsillar and tonsillar categories. At histological level in dogs, OSCC can be divided into histologic subtypes that are in many but not all aspects similar to OSCC in humans. These subtypes include well-, moderately, and poorly differentiated conventional SCCs as well as more rare subtypes such as papillary and basaloid SCCs and adenosquamous and spindle cell carcinomas. They generally show a “moth eaten” appearance on intra-oral radiographs. The 1-year survival rate ranges from 84% to 91% and the metastatic rate ranges from 3% to 36% in dogs following surgical resection of OSCCs. The prognosis for dogs with OSCC is generally excellent following radical surgical excision of the tumour via mandibulectomy, maxillectomy, or glossectomy. Mandibular/maxillary SCC: The prognosis reported when aggressive surgical resection (at least 1cm – (2cm better!)) is excellent. These margins must always be evaluated based upon pre-op CT imaging (remains the standard of care – with adjunctive therapy in specific cases). In non-tonsillar OSCC, fewer than 15% of dogs have detectable nodal metastases and fewer than 5% of dogs have radiographic evidence of pulmonary metastasis at the time of diagnosis. The outcomes reported following mandibulectomy or maxillectomy for SCC included MSTs of 3.5 to 19.2 months, a disease-free interval of 26 months, and 1-year survival rates of 57% to 91% (Kosovsky Vet Surg 1991, Schwarz JAAHA 1991, White JSAP 1991, Wallace Vet Surg 1992). However, more recent results for SCC treatment outcomes have been reported and include more optimistic rates, such as a 1-year survival rate of 93.5% for 21 dogs that had undergone curative-intent surgery and an MST of 365 days for dogs > 10 years old (Fulton, J Am Vet Med Assoc 2013). The 1- year survival rate for all dogs that were surgically treated was 93.5%; the 1-year survival rate was 100% for dogs
VETERINARY SYMPOSIUM 2020
Radiation therapy alone has a median survival time of 16-36 months. It is better for
smaller lesions – showing longer survival times. (Burk 1996). One year survival in 70%
of patients and 30% of recurrence rate. Radiation therapy used post-op after
incomplete surgical excision of oral SCC had longer median survival time (2051 days)
compared to those with incomplete excision and no radiotherapy (181 days). (Riggs,
J Am Vet Med Assoc 2018). Radiation therapy has been considered as an adjunctive
therapy to reduce tumour size prior to surgery (Mestrinho, Aust Vet J 2012). Maxillary
SCC in 1 dog non-resectable at presentation. Radiotherapy and chemotherapy
(carboplatin and doxorubicin) decreased tumour size to allow for surgical resection –
free from local disease for 421 days. The use of piroxicam has reported the following
results:
• Piroxicam alone (0.3mg/kg PO SID) (Schmidt, J Am Vet Med Assoc 2001) –
Response rate 17.6%. MST 180d.
• Piroxicam and cisplatin (Boria, J Am Vet Med Assoc 2004) 5/ dogs responding
to tx –However renal toxicity in 41%! So limited clinical usefulness.
• Piroxicam and carboplatin (de Vos, Vet Comp Oncol 2005) – 7 dogs with T3
oral SCC (tumour >4cm) had complete response in 57% with median follow-up
time of 534 days.
There is a novel treatment published in the literature: Intralesional bleomycin and feline
IL-12 DNA combined with translesional electroporation (Reed, Cancer Gene Ther
2010) - 2 dogs with mandibular/maxillary SCC. Both had complete response and
tumour free 3 and 5 years later. The second report of this treatment with a slight
variation (electroporation and IV bleomycin) in a bigger population (11 dogs) reported
complete remission in 8 dogs and partial remission in 2. The recurrence rate was
27.3%. All dogs with tumours less than 1-2cm had complete remission without
recurrence. (Simcic, Vet Comp Oncol 2019).
Lingual/sublingual SCC:
With a metastatic rate of 37.5% (Carpenter JAAHA 1993), it is the second most
common lingual tumour in dogs after MM (Dennis, J Am Vet Med Assoc 2006).
Females are more at risk in all breeds, with poodles, labs and samoyeds
overrepresented. The typical presentation is bilateral symmetrical involvement
(61.9%), infiltrating the full thickness of the tongue (52.4%) and involving the rostral
two-thirds (85.7%). A very good functional outcome has been reported associated with
radical glossectomy in 5 dogs – Subtotal (50% resection) or total glossectomy (100%
resection) (Dvorak, J Am Anim Hosp Assoc 2004). Hypersalivation is the most
common reported complaint following aggressive resection.
Tonsillar SCC:
It has a high rate of metastasis, with 98% metastasizing to the regional lymph nodes
(via lymphatics) and 63% to more distant anatomic sites (presumably
hematogenously). The high rate of metastasis is related to a rich blood supply and
22VETERINARY SYMPOSIUM 2020
lymphatics draining to ipsilateral and contralateral lymphocentres. There are ten times
more common in urban vs rural areas with a median age of 10 years. They range from
microscopic primary tumours with advanced metastatic disease to bulky exophytic
tumours.
Surgical resection followed by radiotherapy (9 Gy once a week for 4 weeks) and
carboplatin treatment (300mg/m2) in 5 dogs reported a median survival time of 211
days, with 2 dogs been alive and disease free at 826 and 1628 (Murphy, JSAP 2006).
In a multi-centre study of 44 dogs treated with surgery, radiotherapy and/or
chemotherapy reported an overall median survival time of 179 days (Mas, JSAP
2011). They concluded that no matter what treatment modality was used the survival
time was short, although there were a small number of long-term survivors.
Papillary SCC:
It is a lesser aggressive variant reported in young dogs, but also can be seen in adult
dogs (Nemec, J Comp Pathol 2014). It is a distinct histopathological sub-type of SCC.
A Retrospective study of 12 dogs – median age 9 years. They presented as a
verrucous pink mass arising from the gingiva of rostral maxilla or mandible. May be
associated with papillomavirus? – Although no strong evidence. They are locally
aggressive with underlying bone lysis. Respond well to aggressive local surgery and
radiotherapy. No reports of metastasis. Often curative.
SCC CATS
SCC represents 61-64% of all oral tumours in cats. Cats with advanced OSCC
presented with metastasis of the mandibular lymphnodes or lung metastasis did not
have a shorter MST (Soltero-Rivera JFMS 2014). FOSCC exhibit overexpression of
COX-1 and COX-2. A study performed in the UK on feline patients treated by their
general practitioners reported an overall median survival time was 44 days (Hayes
JSAP 2007).
Mandibular/maxillary
The maxilla and mandible can equally be affected. Most cats are referred for a non-
healing surgical site or “abscess”. There is generally bone enlargement with facial
asymmetry, ulceration and difficulty eating. 73.1% had marked osteolysis on
radiographs. Cats with oral SCC are typically diagnosed late and the response to
therapy is poor. Cats with mandibular swellings in 50% of cases will have a tumour.
Sometimes there is no difference on rads between tumour and osteomyelitis.
(Kapatkin JAAHA 1991). The MST of any treatment method is 60 days (Gendler
JAVMA 2010 and Postorino JAHA 1993). When performing a mandibulectomy
combined with radiation or chemo in SCC affecting the mandible, there is a 1 yr
survival rate of 51%, 2 yr survival rate of 34%. (Northrup JAAHA 2006). If radiation
therapy is used on its own the MST is only 36-97 days (Bregazzi 2001 Vet radio
ultrasound).
23VETERINARY SYMPOSIUM 2020
Lingual/Sublingual and Tonsillar
Lingual SCC is locally very aggressive and difficult to treat. There are two growth
patterns recognised, a destructive or an irregular proliferative pattern.
Fidel et al reported a combined protocol using chemotherapy and radiation therapy
comprising 14 fractions of 3.5 Gy given within a 9-day period with the addition of
carboplatin given at 90–100 mg/m2 on day 1 and day 4.5. Treatments were twice daily
with a 6-hour delay between treatments. Cats with tumours of tonsil origin or cheek
responded best to therapy and were long-term survivors with a mean survival of 724
days and the median had not been reached because of continued survival of 4 cats
(Fidel JVIM 2011).
Oral Malignant Melanoma (OMM) DOGS
It is the most common malignant neoplasia in the oral cavity of dogs. The term
melanoma is a misnomer, as this lesion is a sarcoma; a synonym will be
melanosarcoma. Occurs most frequently in aged patients over 11 years of age. Breeds
with highly pigmented oral mucosa (Chow-Chow and Scottish Terrier) seem to be
over-represented. The gross appearance of oral melanoma varies from coal black,
patchy black and white, pink/red (tumour associated granulation tissue), purple, or
white (amelanotic). Melanomas readily invade soft tissues and bone and may be
associated with extensive local tissue destruction. Disruption of the dental arcade or
pathologic fractures can occur if the melanoma invades the jaw. Mostly gingival but
can be labial mucosa, palate, buccal mucosa and tongue.
Can metastasise to brain, meninges, pituitary gland, striated muscle, pleura,
pericardium, heart, prostate, pancreas, adrenal glands, liver, kidney, spleen, ileum,
omentum, mediastinal lymph nodes, thyroid, prostate, salivary gland, stomach, testis
and eyes, tonsils.
HISTOLOGY
There are three main categories based on microscopic features of the predominant
cell type including polygonal (epithelioid), spindle and mixed (epithelioid and spindle)
cells. Different studies disagree re distribution of types.
Dx: A variety of useful antibodies for IHC assays are now available for the diagnosis
of canine oral melanoma: S100, Melan A, PNL2 and tyrosinase-related proteins 1 and
2. S100 may be the most sensitive, but it is the least specific of this antibody stains.
TREATMENT OPTIONS:
Curative Intent Surgery
Cornerstone combined with vaccine/chemotherapy or radiation therapy. The case
series published by Tuohy et al (JAVMA 2014) analysing 70 patients undergoing
curative intent surgery described a median progression-free interval and ST of 508
and 723 days, respectively. Thirty-two (45.7%) dogs had disease progression.
Significant associations with PFI or ST were found for administration of adjuvant
24VETERINARY SYMPOSIUM 2020
therapy, presence of metastatic disease at the time of diagnosis, higher tumor stage
(III or IV), and increased tumor size (> 3 cm). Co-adjuvant treatment was associated
with a 130% increased hazard of disease progression; the presence of metastasis at
the time of diagnosis was associated with a 281% increased hazard of death. A second
paper (Boston JAVMA 2014) evaluating the efficacy of systemic therapies after
surgical excision of oral melanomas indicated that surgical treatment of oral malignant
melanoma in dogs can result in an MST of 346 days, with long-term survival in 29%
of cases. Dogs that were treated with surgery alone had an MST of 352 days, and we
were not able to detect a survival advantage with any form of postoperative adjuvant
therapy. Interestingly this paper reported no difference on MST between marginal
resections and wide or radical resections.
Xenogeneic DNA vaccination
Vaccine (Oncept in the UK) contains plasmid DNA-targeting tyrosinase, a glycoprotein
essential for melanin synthesis and demonstrated to be overexpressed in melanomas
(Bergman & Wolchok 2008), conflicting results so far but is potentially therapeutic in
stage II/III locoregionally controlled disease.
Results of Grosenbaug (2011) documented a statistically significant improvement in
survival for vaccinates (more than 1075 days) compared to historic controls. Verganti
(2017) reported only a disease free interval of 477 days in vaccinated dogs vs 491 for
non-vaccinates and a MST of 455 days. In Ottnod’s (2013) study, disease free interval
for vaccinates was 171d, and for non vaccinates it was 258 days.
In the Verganti (2017) study, effects of vaccine were seen early on (in loading period)
but 50% of patients with stages I to III disease died due to local recurrence (with or
without regional lymph node involvement; 17·9%) or due to metastatic disease
(29·6%) to the lymph nodes, lungs, liver, brain, tonsil and skin which means melanoma
vaccine may not be effective in all the patients treated or works only for a limited time.
Patients with macroscopic disease had a 44·4% response rate to the vaccine and the
MST for dogs with stage IV disease was 178 days.
a) Carboplatin: Response rate 28%
b) Cisplatin and piroxicam: response rate 18% both drugs nephrotoxic!
c) Palliative radiation: MST 7.9 months (prognosis not dependent on stage- they
all respond the same)
d) Definitive-intent radiation therapy (Proulx 2003) MST 7 months
e) Hypofractionated radiation + low-dose cisplatin or carboplatin as a radiation
sensitizer- mst 363 days.
FIBROSARCOMA DOG
It is one of the three most common tumours reported in the oral cavity of dogs. It is
locally aggressive with a low rate of metastasis (VETERINARY SYMPOSIUM 2020
Frazier et al. Vet and Comp. Oncology 2011:
A total of 29 dogs were included in this study. The overall survival time (from surgery
to tumour related death) reported here was 24.8 months. Seven dogs (24.1%)
developed metastasis: three to regional (mandibular) lymph node only, three to lung
only and one to both regional lymph node and lung. The median survival time of the
seven dogs that developed metastasis was 391 days. Golden Retriever or Golden
Retriever mixed breed dogs were more likely to experience local recurrence than other
breeds (P = 0.03).
The median survival time (MST) of all dogs was 743 days (95% CI 569–1598 days).
The 1-and 2-year survival times were 87.7% (95% CI66.5–95.9) and 57.8% (95% CI
31.6–77), respectively. The median survival times of dogs treated with surgery alone
or with surgery and radiation therapy were not statistically different (1024 days and
576 days, respectively; P = 0.40). The MST for dogs with complete excision was not
statistically different from those with incomplete excision (1598 days versus 576 days,
respectively; P = 0.09);
Gardner et al VCO 2015. 65 Dogs receiving different therapies:
Approach Median survival Notes
time (d)
Conservative surgery 301
Aggressive surgery (removal of bone), 526 some of these had radiation
Palliative intent radiation therapy – 24- 204
30gy
Definitive radiation therapy (no sx) – 54- 825 these were all T3
60Gy
Chemotherapy (Doxorubicin or Use of chemo didn’t stat sig affect MST
Lomustine)
No Tx 205
RADIATION AND SURGERY 505
RADIATION (CURATIVE INTENT) AND 575 not stat sig vs palliative and
SURGERY surgery
Soft tissue sarcomas have been historically considered resistant to radiation therapy,
requiring doses above 50 Gy to markedly affect the neoplastic tissue. Although
radiation therapy can be used to treat macroscopic disease, it is most efficacious when
employed against microscopic disease.
26VETERINARY SYMPOSIUM 2020
Hi-lo fibrosarcomas:
Median age 8yo and 52% were golden retrievers (Ciekot et al JAVMA 1994).
Histopath: fibroblasts with abundant collagenous tissue. Recognised as ‘Low grade’
due to
• low numbers of fibrocytes,
• low mitotic index (0-1 mitotic figues per HPF),
• minimal cellular anaplasia,
• minimal pleomorphism,
• abundant collagenous matrix.
• Poor demarkation from surrounding tissue
Innocuous histo appearance but these are invasive: invade ST and bone and met to
local LN. 72.7% of dogs evaluated found to have underlying bone lysis
‘Fibrosarcoma’ doesn’t distinguish between low grade and high grade.
OSTEOSARCOMA DOG
It is the most common bone tumor in dogs. Osteosarcomas are divided into
appendicular and axial, with 49% of axial osteosarcomas occurring in the mandible or
maxilla. Osteosarcomas of the maxillofacial region most often arise from the bone
medullary region. Although can also be juxtacortical OSA (Periosteal and parosteal
OSA) (Murphy Veterinary Oral and Maxillofacial Pathology 2019). The mean age at
diagnosis of canine oral and maxillofacial osteosarcoma is 9–10 years. Seventy three
per cent of dogs with maxillary osteosarcoma, and 100% of mandibular osteosarcoma
have been reported to weigh more than 20 kg. Mixed-breed dogs, German shepherds,
golden retrievers and Labrador retrievers were most commonly presented. Factors
such as ionizing radiation, genetics, bone tumour viruses, chemicals, chronic irritation
due to fractures repaired by metallic implants, bone infarcts, skeletal diseases or
disorders as well as body size and sex are believed to be involved in pathogenesis.
While osteosarcoma in general is known to be a disease with rapid local progression
and mortality due to early lung metastasis, comparatively, oral and maxillofacial
osteosarcoma have been found to progress slower and show lower tendency to
metastasize than other axial subtypes. As with osteosarcomas at other locations,
clinical signs are caused by the expansive mass and tissue destruction.
There are six histologic subtypes of OSA – osteoblastic (osteoblasts predominate),
fibroblastic (fibroblast-like spindle cells arranged in patterns reminiscent of
fibrosarcoma), chondroblastic (extensive regions of chondroblastic differentiation with
chondroid matrix deposition), giant cell (large numbers of intermixed multinucleate
cells), telangiectatic (endothelium like sarcoma cells form blood-filled cavities and
sinuses reminiscent of hemangiosarcoma), and poorly differentiated OSA (neoplastic
cells are anaplastic). Osteoblastic OSA is further subdivided into productive (abundant
tumor associated osteoid matrix (TAOM)) or nonproductive (minimal TAOM) (Murphy
Veterinary Oral and Maxillofacial Pathology 2019).
27You can also read

















































