Tactical Combat Casualty Care Update - Harold Montgomery 17 May 2018 - Special ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Tactical Combat Casualty
Care Update
Harold Montgomery
17 May 2018
Disclaimers
“The opinions or assertions contained herein
are the private views of the author and are not
to be construed as official or as reflecting the
views of the Departments of the Army, Air
Force, Navy or the Department of Defense.”
- No financial interests in items discussed
- Off label uses: TXA, OTFC, Ketamine
1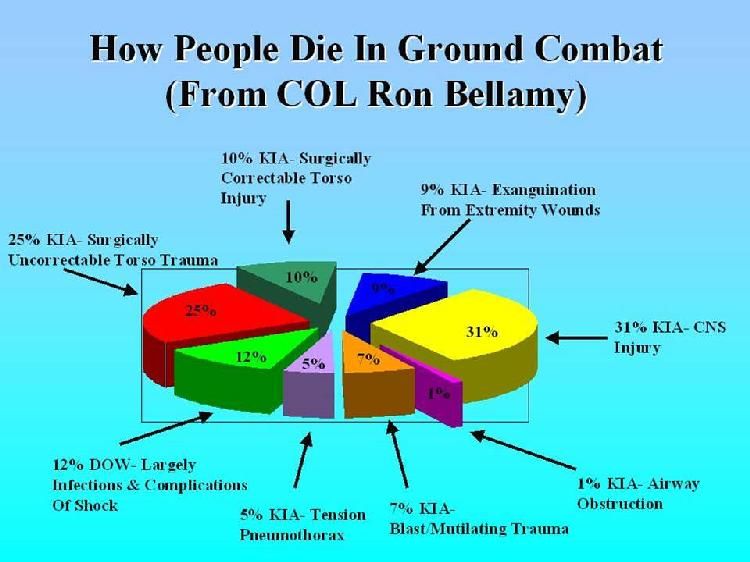
Learning Objectives
At the conclusion of this activity, the participant
will be able to:
- Become familiar with battlefield trauma care
advances pioneered by Tactical Combat Casualty
Care (TCCC)
- Discuss recent advances in TCCC
- Discuss current capability gaps in TCCC
Tactical Combat Casualty Care
The Prehospital Arm of the Joint Trauma System
• Medics, Corpsmen, PJs
TCCC • Combat Lifesavers
• All Service Member Self/Buddy Care
4
2
Intro to TCCC
5
Link to Intro to TCCC Video on Deployed Medicine Link to Intro to TCCC Video on YouTube
TCCC: Beginnings
6
3
7
Tourniquets: The Primary
Driver for TCCC
“The striking feature was to see healthy
young Americans with a single injury of the
distal extremity arrive at the magnificently
equipped field hospital, usually within
hours, but dead on arrival. In fact there were
193 deaths due to wounds of the upper and
lower extremities, …… of the 2600.”
CAPT J.S. Maughon
Mil Med 1970
* Extremity hemorrhage math in Vietnam:
193 of 2600 = 7.4% x 46,233 fatalities = 3,421
preventable US deaths from extremity hemorrhage
8
4
Tourniquets Reconsidered –
The Primary Driver for TCCC
• ATLS 1992: Tourniquets strongly discouraged
• Fear of ischemic damage to limbs - BUT
• Exsanguination from extremity hemorrhage was the
#1 cause of preventable death in Vietnam - AND
• Tourniquets can control extremity hemorrhage
• Used routinely during orthopedic surgery and limbs
are not lost there as a result
• Also – even if you had to choose between death and
losing a leg….
• Bottom line: The “No Tourniquet” rule was NOT
evidence-based and was NOT logic based. 9
Pulling the Thread –
Medical Issues
Other Aspects of Care in 1992 that Needed Review
• Tactical context in battlefield trauma care
• Fluid resuscitation and IV access
• Battlefield analgesia
• Prevention of coagulopathy
• Spinal precautions
• Battlefield CPR
• Treatment of tension pneumothorax
• Battlefield antibiotics
• Undertaken as a Naval Special Warfare Biomedical
R+D project 10
5
Prehospital Trauma Care:
Military vs Civilian
• Hostile fire
• Darkness
• Environmental extremes
• Different wounding
epidemiology
• Limited equipment
• Multiple casualties
• Need for tactical maneuver
• Long delays to hospital care
• Different provider training and experience
• What do we do about this? 11
Tactical Combat Casualty Care
(TCCC) : A Different Approach
• Battlefield trauma care research effort – Special
Operations and USUHS: 1993-1996
• Reviewed most recent trauma care literature
• Combat environment and mission considered
• Combat medic training and equipment considered
• Project included input from combat medics,
corpsmen, and pararescuemen (PJs)
• Evidence-based – INCLUDING requiring evidence
for current practice at that time
• Goal – To prevent ALL preventable deaths 12
6
Tactical Combat Casualty
Care in Special Operations
Military Medicine Supplement
August 1996
Evidence-based trauma
care guidelines customized
for use on the battlefield
TCCC Lessons Learned
3. If What You’re Doing is Not
Working - Do Something Else.
7
Tactical Combat
Casualty Care (TCCC)
• First used by Navy SEALs,
75th Ranger Regiment, and Air
Force Pararescue in 1997
• PHTLS, ACS COT and NAEMT
endorsement 1999
• Most of Special Operations and
most conventional forces were
NOT using TCCC at the start of
the war in Afghanistan.
15
Tourniquets Early in the Iraq
and Afghanistan Conflicts
• Increased use of tourniquets by both Special
Operations and conventional units beginning in 2005
The Drivers:
• Holcomb study: “Causes of SOF Deaths 2001-
2004” – highlighted need for TCCC
• USAISR tourniquet study by Walters et al (2005)
• TCCC Transition Initiative begun in 2005
Butler – ACS Bulletin - 2015
8
Tourniquets Early in the Iraq
and Afghanistan Conflicts
The Drivers:
• USSOCOM TCCC message - March 2005
• USCENTCOM tourniquet and hemostatic agents
(HemCon) message – 2005
After these two events, tourniquet use became
more and more prevalent among US combat forces.
Butler – ACS Bulletin - 2015
Tourniquets – Kragh et al
Annals of Surgery 2009
• Ibn Sina Hospital, Baghdad, 2006
• Tourniquets are saving lives on the battlefield
• 31 lives saved in 6 months period by the use of
prehospital tourniquets
• No loss of limbs from tourniquet ischemia
• Author estimated 1000+ lives saved with TQs 18
9
TCCC: How Do We Know
That It’s Working?
• Near universal DoD acceptance after 17 years of war
• Tarpey 2005: “Overwhelming Success” in 3rd ID
• Kragh 2008: Estimated over 1000 lives saved with tourniquet use –
in 2008
• Kotwal 2011: Lowest incidence of preventable deaths ever
documented by a combat unit
• Savage 2011: Highest casualty survival rate in Canadian Military’s
history
• Butler 2015: 67% reduction in deaths from extremity hemorrhage
from 2006 to 2011
• Acceptance by NAEMT/American College of Surgeons /Hartford
Consensus/WH Stop the Bleed
• USCENTCOM TCCC requirement – November 2017
• DoD Instruction on TCCC 1322.24 – 16 March 2018 19
Individual First Aid Kits
(IFAKs)
At this point in time, the US
Military has more experience
with tourniquets and hemostatic
dressings than any other
organization in history. (14 years
of war and 50,000 + casualties)
Cost: $128
• In 2001 – very few American combatants had
tourniquets - no one had hemostatic dressings
• In 2018 - no American combatant goes onto the
battlefield without an IFAK that contains both
10Battlefield Trauma
Care: Then and Now
21
Battlefield Trauma Care:
1992
• Based on trauma courses NOT developed for combat
• Medics taught NOT to use tourniquets
• No hemostatic agents
• No junctional tourniquets
• Large volume crystalloid fluid resuscitation for shock
• Civil War-vintage technology for battlefield analgesia IM
morphine)
• SOF medics – IV cutdowns for difficult venous access
• No tactical context for care rendered
• 2 large bore IVs on all casualties with significant trauma
• No focus on prevention of trauma-related coagulopathy
• Heavy emphasis on endotracheal intubation 22
11Battlefield Trauma Care:
Now
• Phased care in TCCC
• Aggressive use of tourniquets in CUF
• Combat Gauze as hemostatic agent
• Aggressive needle thoracostomy
• Sit up and lean forward airway positioning
• Extraglottic airways – i-gel
• Surgical airways for maxillofacial trauma
• Hypotensive resuscitation with blood products
• IVs only when needed/IO access if required
• PO meds, OTFC, ketamine as “Triple Option”
for battlefield analgesia
• Hypothermia prevention; avoid NSAIDs
• Battlefield antibiotics
• Tranexamic acid – given ASAP when indicated
• Junctional Tourniquets/XStat 23
TCCC in DoD Policy
24
12ASDHA TCCC Letter
14 February 2014
Called for “…uniform TCCC training throughout the Department.”
CENTCOM Directive
06 November 2017
Mandates TCCC-MP for all medical personnel (medics, physicians, PA, etc…)
Mandates TCCC-AC for all non-medical personnel entering CENTCOM AOR.
26
13DOD Instruction on
Medical Readiness Training
16 March 2018
DOD Instruction on
Medical Readiness Training
Section 2.a.b Policy
“TCCC is the DoD standard of care for first
responders (medical and non-medical) …..All
Service members receive role based TCCC training
and certification in accordance with the skill level
(i.e., All Service Members, Combat Lifesaver,
Combat Medic/Corpsmen, and Combat
Paramedic/Provider) outlined by the Joint Trauma
System, the DoD’s Center of Excellence for trauma
as designated in DoD Instruction (DoDI) 6040.47.
14ASDHA TCCC Implementation
17 April 2018
Services to have standardized role-based TCCC training integrated
no later than 30 April 2020. 29
ASDHA TCCC Implementation
NLT 30 April 2020
• Integration of basic TCCC skills into initial-entry
training (BCT/Boot camp)
• Standardized TCCC Training & certification:
– Service Members
– Combat Lifesaver
– Medics/Corpsman
– Advanced Providers
30
15How Is TCCC Updated?
The Committee
on TCCC and the
TCCC Working
Group
TCCC will always be a work in progress. 31
TCCC Lessons Learned
5. Maintain an Active Search
for Good Ideas – Wherever
They Can Be Found – and
Process Them As Though
Lives Depended on It
Because, indeed – they do.
16Changes to the TCCC
Guidelines
33
TCCC Team 2018
• CoTCCC
• Special Operations Medicine
• Joint Trauma System
• USAISR and other military medical research
facilities
• Service Surgeon General/TMO offices
• Coalition partner nations
• Combatant unit medical officers
• DHA Medical Logistics Office
• Combat Medical Schoolhouses
• Other government agencies 34
17Committee on Tactical Combat
Casualty Care (CoTCCC)
• First funded by USSOCOM in 2001-2002 at the
Naval Operational Medicine Institute (NOMI)
• Later sponsored by Navy and Army Surgeons
General and the U.S. Army Institute of Surgical
Research
• 42 members - all services
• Trauma Surgeons, EM and Critical Care
physicians; operational physicians and PAs;
medical educators; combat medics, corpsmen, and
PJs
• 100% deployed experience in 2016
• Relocated to the Defense Health Board in 2007
at the direction of ASD/HA
• Moved to the Joint Trauma System in 2013
35
TCCC Change Process
2018
• Need for change identified
• Prioritization
• Sponsor and author team designated
• Draft change paper prepared
• Change presented to TCCC Working Group
• Change revised as needed
• CoTCCC vote on change – 2/3 majority required
• Change approved by JTS Director
• Change published in the JSOM
• TCCC Guidelines and curriculum updated 36
18Recent Advances in TCCC 37
TCCC Changes:
2013
• TCCC Casualty Card (DD1380)
– Kotwal
• Vented chest seals
– Butler/CAPT Don Bennett
• Junctional tourniquets
– Kotwal
• Triple-Option Analgesia
– Butler
19TCCC Changes:
2014
• Alternate hemostatic dressings
– Bennett
• Fluid resuscitation
– Butler
• Updated tourniquet use guidelines
– Shackelford
TCCC Changes:
2015
• Zofran in for Phenergan
– Onifer
• CricKey for Surgical Airways
– Mabry
• Abdominal Aortic Junctional TQ
– Not recommended
• XStat
– Sims/Bowling
20TCCC Changes:
2016
• ITClamp
– Not Recommended
• Pelvic Binders
– Shackelford
• Comprehensive Review
– Montgomery
TCCC Changes:
2017
• Extraglottic Airways in TCCC
–Otten – approved 25 August 2017
• Management of Suspected Tension
Pneumothorax in TCCC
– Butler - approved 19 Jan 2018
21Extraglottic Airways in
TCCC
43
Extraglottic Airways in
TCCC
1) Adds extraglottic airways (EGAs) as an option for airway
management in Tactical Field Care.
2) Recommends the i-gel as the preferred EGA because its gel-
filled cuff makes it simpler to use than EGAs with air-filled cuffs
and eliminates the need for cuff pressure monitoring.
3) Notes that should an EGA with an air-filled cuff be used, the
pressure in the cuff must be monitored, especially during and
after changes in altitude.
22Extraglottic Airways in
TCCC
4) Emphasizes that extraglottic airways will not be tolerated by a
casualty unless he or she is deeply unconscious and notes that an
NPA is a better option if there is doubt about whether the casualty will
tolerate an EGA.
5) Adds the use of suction when available and appropriate (eg, when
needed to remove blood and vomitus) as an adjunct to airway
management.
6) Clarifies the wording regarding cervical spine stabilization to
emphasize that it is not needed for casualties who have sustained
only penetrating trauma (without blunt force trauma.)
Extraglottic Airways in
TCCC
7) Reinforces that surgical cricothyroidotomies should not be
performed simply because a casualty is unconscious.
8) Provides a reminder that for casualties with facial trauma or
facial burns with suspected inhalation injury, neither NPAs nor
EGAs may be adequate for airway management, and a surgical
cricothyroidotomy may be required.
23Extraglottic Airways in
TCCC
9) Adds that pulse oximetry monitoring is a useful adjunct to
assess airway patency and that capnography should be also be
used in the TACEVAC phase of care.
10) Reinforces that a casualty’s airway status may change over
time and that he or she should be frequently re-assessed.
Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
48
24Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
1. Continues the aggressive approach to suspecting and
treating tension pneumothorax based on mechanism of
injury and respiratory distress that TCCC has advocated for
in the past, as opposed to waiting until shock develops as a
result of the tension pneumothorax before treating. The
new wording does, however, emphasize that shock and
cardiac arrest may ensue if the tension pneumothorax is
not treated promptly.
49
Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
2. Adds additional emphasis to the importance of the
current TCCC recommendation to perform needle
decompression (NDC) on both sides of the chest on a
combat casualty with torso trauma who suffers a traumatic
cardiac arrest before reaching a medical treatment facility.
3. Adds a 10 gauge, 3.25 inch needle/catheter unit as an
alternative to the previously recommended 14 gauge, 3.25
inch needle/catheter unit as recommended devices for
needle decompression.
50
25Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
4. Designates the location at which NDC should be
performed as either the lateral site (5th intercostal space
{ICS} at the anterior axillary line {AAL}) or the anterior site
(2nd ICS at the midclavicular line {MCL}).
5. Adds two key elements to the description of the NDC
procedure: insert the needle/catheter unit at a
perpendicular angle to the chest wall all the way to the hub,
then hold the needle/catheter unit in place for 5-10 seconds
before removing the needle in order to allow for full
decompression of the pleural space to occur.
51
Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
6. Defines what constitutes a successful NDC, using
specific metrics such as: an observed hiss of air escaping
from the chest during the NDC procedure; a decrease in
respiratory distress; an increase in hemoglobin oxygen
saturation; and/or an improvement in signs of shock that
may be present.
52
26Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
7. Recommends that only two needle decompressions be
attempted before continuing on to the “Circulation” portion
of the TCCC Guidelines. After two NDCs have been
performed, the combat medical provider should proceed to
the fourth element in the “MARCH” algorithm and
evaluate/treat the casualty for shock as outlined in the
Circulation.
Since the manifestations of hemorrhagic shock and shock
from tension pneumothorax may be similar, the TCCC
Guidelines now recommend proceeding to treatment for
hemorrhagic shock (when present) after two NDCs have
been performed.
53
Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
8. Adds a paragraph to the end of the Circulation section of
the TCCC Guidelines that calls for consideration of
untreated tension pneumothorax as a potential cause for
shock that has not responded to fluid resuscitation. This is
an important aspect of treating shock in combat casualties
that was not presently addressed in the TCCC Guidelines.
54
27Management of Suspected
Tension Pneumothorax in TCCC
TCCC Guideline Change 17-02
9. Adds finger thoracostomy (simple thoracostomy) and
chest tubes as additional treatment options to treat
suspected tension pneumothorax when further treatment is
deemed necessary after two unsuccessful NDC attempts –
if the combat medical provider has the skills, experience,
and authorizations to perform these advanced interventions
and the casualty is in shock. These two more invasive
procedures are recommended only when the casualty is in
refractory shock, not as the initial treatment.
55
TCCC Proposed Changes:
Underway in 2018
• Advanced Resuscitative Care
– Butler
• Relook at Tourniquets in TCCC
– Montgomery
28Traditional TCCC Casualty
Flow
Individual Medic/Corpsman Medical Capability
w/IFAK w/ AidBag On Evac Platform
w/ More Equip
57
Operational Casualty Flow
29Advanced Field/Resuscitation
Care Phase
• Beyond a single medic with an aidbag, but still in
prehospital/Role 1 environment
• Inclusion of advanced procedures at CCP / BAS
/ Shock Trauma Plt / FOB Aid Station / SOF
Medic setting by advanced providers or forward
medical teams
• **NOT to be confused with PFC or Role 2**
• Training Requirement and Expanded Capability
for Role 1 Providers/Advanced Medics.
• Multiple Hands
Advanced Field/Resuscitation
Care Phase
• Fresh Whole Blood/Blood Products
• REBOA
• Definitive Junctional Management
• Advanced Airway Management/Suctioning
• UltraSound
• Burn Fluid Resuscitation
• Advanced Monitoring
• Improved Hypothermia Prevention
60
30Tourniquet Review
• Validate / Re-validate currently
recommended tourniquets
• Review additional tourniquets
– Potentially recommend additional TQs
– Identify why some TQs are not recommended
• Define CoTCCC-Recommended TQ
Specifications
• Refine the CoTCCC process for reviewing
previously recommended items. 61
TCCC
Engagement
62
31All TCCC change
papers are
published in the
JSOM
- Searchable in
PUBMED
- Permanent part
of the published
medical literature
TCCC Guidelines:
The What
TCCC Curriculum:
The How
MPHTLS Textbook:
The Why
TCCC Change Papers
The Detailed Why
“Military units that have trained all of their members in
Tactical Combat Casualty Care have documented the
lowest incidence of preventable deaths among their
casualties in the history of modern warfare.”
32TCCC Journal Watch
TCCC Article Abstracts:
Monthly focused PUBMED search
of prehospital trauma literature
Available on Deployed Medicine, JTS Website and through the TCCC Distro
TCCC in Social Media
@CommitteeonTCCC tc3committee
@CoTCCC @JointTraumaSyst
@JointTraumaSystem
Channel Name:
CoTCCC
https://www.linkedin.com/company/jointtraumasystem Committee-on-
TCCC
Join the LinkedIn Discussion Groups:
TCCC (https://www.linkedin.com/groups/12036508)
66
33Social Media
Collaboration
Network
JTS Official Website
http://jts.amedd.army.mil/
68
34CoTCCC on JTS Site
http://jts.amedd.army.mil/
69
Deployed Medicine
70
35Medic Survey 2016
What Medics Want:
• MOBILE Access
• NO CAC
Requirement
• Quick Knowledge
Access
• Teaching Tools
Deployed Medicine
• DM is a Defense Health Agency-sponsored
project to
– trial new innovative learning models.
– improving readiness and performance of deployed
military medical personnel.
– deliver personalized, dynamic learning using the most
current and accessible technology.
– enabling a self-directed and continuous study of
medical best practices and lessons learned.
72
36Website:
www.deployedmedicine.com
Previous www.cotccc.com
is migrating to Deployed Medicine
73
https://itunes.apple.com/us/app/deployed-medicine/id1203051672?mt=8
https://play.google.com/store/apps/details?id=com.allogy.deployedmedicine
74
37TCCC & JTS on DM
75
Synchronized Content
Mobile App Website
76
38TCCC Collections
77
Guidelines
78
39Videos
79
Podcasts
Available on Deployed Medicine
Also Available as Podcast Subscriptions
Subscribe on iTunes: Search for “Combat Casualty Care”
Subscribe on Android at:
http://subscribeonandroid.com/tccc.blubrry.net/feed/podca
st/
RSS Feed for the Combat Casualty Care Podcast:
http://tccc.blubrry.net/feed/podcast/
80
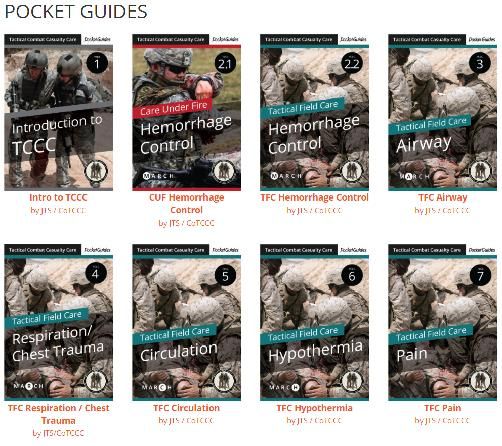
40Pocket Guides
81
Pocket Guide
82
41References
83
Instructor Materials
84
4285
TCCC Curriculum:
DM and NAEMT Websites
• Also direct mailings to DoD combat medical
schoolhouses
• Also Special Operations Medical Association
and JSOM websites 86
43Performance Improvement
Quality Assurance
Lessons Learned
87
Casualty AAR System & DoDTR
• Gather Lessons Learned
directly from medics
involved
• Collect Prehospital Data
to improve training &
equipment
• NOT punitive or
investigative, but is PI
TCCC POI AAR TACEVAC AAR
44Casualty AAR System & DoDTR
Available for download on the JTS Site: http://jts.amedd.army.mil
Send to:
usarmy.jbsa.medcom-aisr.list.jts-prehospital@mail.mil
NIPR: SOF-Casualty-AAR@socom.mil or
SIPR: SOF-Casualty-AAR@socom.smil.mil
89
Quality Assurance
in TCCC Training:
The JTS TCCC
Curriculum
90
45TCCC Training in the DoD: 2018
- Incompletely trained
- Incorrectly trained
- Incompletely executed
- Need a STANDARD
91
Saving Lives on the Battlefield
I (2012) and II (2013)
• Surveys of prehospital care
in Afghanistan
• Combined Joint Trauma
System/USCENTCOM team
• Directed interviews with
hundreds of physicians,
PAs, and combat medical
personnel in combat units
• COL Russ Kotwal (I)
• COL Samual Sauer (II)
46Findings from the Two
CENTCOM/JTS Prehospital
Care Assessments
• TCCC is not being implemented evenly across
the battle space
• These variations are not just SOF versus
conventional forces difference
• Why is this happening?
• “We teach physicians ATLS (maybe) and then
assign them to operational units and expect
that they can effectively supervise medics who
have been taught battlefield trauma care based
on TCCC concepts.”
Non-Standard TCCC
Courses
• Many “TCCC” courses (unit-based, service-
based, and vendor-based) – aren’t!
• Incorrect messaging
– Instructor drift
– “Never take off a tourniquet in the field”
– “Let the tourniquet down every 15 minutes”
• Incorrect messaging has been DIRECTLY
associated with adverse outcomes
• Inappropriate training
94
47RECENT Preventable
Adverse Outcomes
• One Special Operations member suffered a leg
amputation from prolonged tourniquet use – only
amputation from tourniquet use in US forces. Unit
members had been told never to take off a tourniquet in
the field at their “TCCC” course. Tourniquet was left on
for over 8 hours.
• A casualty suffered pulmonary edema at a foreign
medical facility from getting 9 liters of NS during
resuscitation from hemorrhagic shock
• 2 deaths from unrecognized tension pneumothorax
• Respiratory arrest from using midazolam after fentanyl
lozenges
TCCC Training – The
Need for a Standard
• In the absence of a standard high-
quality TCCC course with a
professionally developed curriculum,
"TCCC Training" in the DoD can wind
up being an hour of Powerpoint slides
or 11 days of inappropriate training - or
anything in between.
96
48Variable TCCC
Instructors
• TCCC Instructor # 1
– Up to date on current TCCC Guidelines, Practices,
and Curricula
• TCCC Instructor # 2
– Teaching what they learned “when” they learned it but
not up-to-date.
• TCCC Instructor # 3
– Selectively teaching the parts they agree with or are
comfortable with or understand.
• TCCC Instructor # 4
– Teaching their own “interpretation” of TCCC. 97
Joint Trauma System
White Paper to Service SGs
• Outlined the problem
• Documented the bad outcomes from non-standardized
TCCC training
• Recommended that we use the JTS-developed TCCC
98
curriculum as taught through NAEMT.
49Training Standard
NAEMT
ACLS/BLS – American Heart Assn
ATLS – ACS Committee on Trauma
TCCC – JTS CoTCCC
ACS COT and NAEMT
* NAEMT training sites can be established at military
bases anywhere in the world or with commercial TCCC
training vendors
NAEMT Courses
Advantages
• They use the JTS/CoTCCC curricula.
• They QA their instructors.
• Have a system for establishing training sites
• Certification card at the end of the course.
• NAEMT database of all who complete the course.
• Less expensive than commercial training vendors.
• Cost: $10 per student (medics, physicians, PAs - who
need to be certified)
• Potentially free for non-medical combatants (but no
NAEMT certification cards)
• The course with the “Shock Labs” - cost $2000 per 100
student plus 10 days travel (another $2000)
50Translating TCCC to
the Civilian Sector
101
102
51White House:
“Bystander – Stop the Bleed”
• White House meeting on this topic 6 October 2015
• Emphasis was on BYSTANDERS being able to
use tourniquets and hemostatic dressings 103
104
5243 States and 15 Nations over a 10-day period.
30,000+ Trained
Coming back soon: MARCH 2019 105
Thank You! @CommitteeonTCCC
Harold Montgomery CoTCCC
Committee-
@CoTCCC Operational Medicine Liaison on-TCCC
Joint Trauma System / CoTCCC
Harold.r.montgomery2.ctr@mail.mil
tc3committee
HRMontgomery75@gmail.com
SOMA Related
www.deployedmedicine.com http://jts.amedd.army.mil/
106
53You can also read