BUT WHY? The MDS, It is a Changing - Objectives Identify the MDS 3.0 changes going into effect on 10/1/18 - Wisconsin Director of Nursing ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
9/25/2018
The MDS,
It is a Changing
BUT WHY?
Cindy Fronning RN-BC, CDONA,
FACDONA, RAC-CT, IP-BC, AS-BC
Director of Education
NADONA
NADONA 1
Objectives
• Identify the MDS 3.0
changes going into effect
on 10/1/18
• Discuss the purpose of
the MDS changes
NADONA 2
1
9/25/2018
MDS Changes
NADONA 3
Section B
• B0700 added “preferred method of
communication, sign language”, cue cards
and consulting with CNAs over all shifts,
(took away “If available”)
– Coding Tips – “
– “This item cannot be coded as Rarely/Never Understood if
the resident completed any of the resident interviews,.
– • While B0700 and the resident interview items are not directly
dependent upon one another, inconsistencies in coding among
these items should be evaluated.”
• B0800 added “preferred method of
communication”
NADONA
4
2
9/25/2018
Section C, D, F
• BIMS Interview: Completion date changed:
“preferably the day before or the day of the
ARD.” (Now the same as pain and PHQ9)
• Assessment Tips for all Interviews
– Interact with the resident using his or her preferred language. Be
sure he or she can hear you and/or has access to his or her
preferred method for communication. If the resident appears
unable to communicate, offer alternatives such as writing,
pointing, sign language, or cue cards.
– Attempt to conduct the interview with ALL residents. This
interview is conducted during the look-back period of the
assessment reference date (ARD) and is not contingent upon
item B0700, Makes Self Understood.
NADONA
5
Section C, D, F cont.
– If the resident interview was not conducted within
the look-back period (preferably the day before or
the day of the ARD), item [C0100, D0100, F0300,
J0200] must be coded 1, Yes, and the standard “no
information” code (a dash [-]) entered in the resident
interview items.
– Do not complete the Staff Assessment for [Mental
Status items (C0700–C1000), Mood items
(D0500), Daily and Activity Preferences items
(F0700–F0800), Pain items (J0800–J0850)] if the
resident interview should have been conducted but
was not.
NADONA
6
3
9/25/2018
Section C, D, F cont.
• Pain, PHQ9 & BIMs Interviews: Coding Tips:
– There is one exception to completing the Staff Assessment of
Resident Mood items (D0500) in place of the resident interview.
This exception is specific to a stand-alone, unscheduled PPS
assessment only and is discussed on page 2-60. For this type of
assessment only, the resident interview may be conducted up to
two calendar days after the ARD.
– When coding a stand-alone Change of Therapy OMRA (COT), a
standalone End of Therapy OMRA (EOT), or a standalone Start
of Therapy OMRA (SOT), the interview items may be coded using
the responses provided by the resident on a previous assessment
only if the DATE of the interview responses from the previous
assessment (as documented in item Z0400) were obtained no
more than 14 days prior to the DATE of completion for the interview
items on the unscheduled assessment (as documented in item
Z0400) for which those responses will be used.
•
NADONA
7
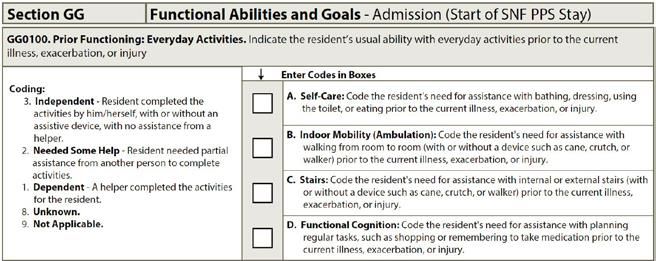
Section GG
• New Item – New coding scale
• Knowledge of the resident’s functioning prior to the current illness,
exacerbation, or injury may inform treatment goals.
• Code based on an assessment of the resident’s function prior to current
illness, exacerbation, or injury. The everyday activities are broken down
into: Self-care; Indoor Mobility ( Ambulation) Stairs & Functional Cognition
•
NADONA
8
4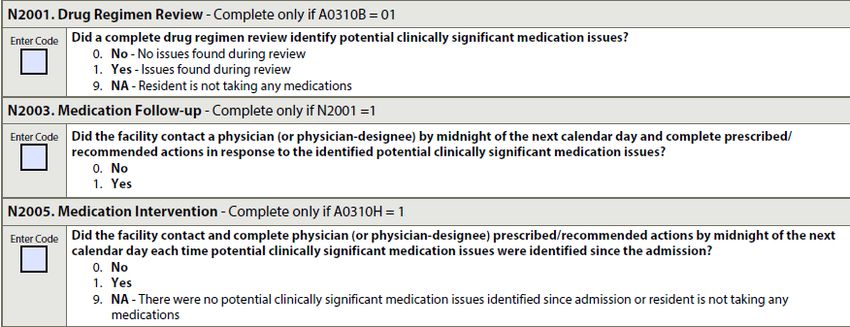
9/25/2018
New Codes
• Independent – Resident completed the
activity per self with /without an assistive
device without assistance from a helper
• Needed some help – Resident needed partial
assistance rom another person to complete
activities
• Dependent – Helper completed the activities
for the resident
• Unknown
• Not Applicable
NADONA
9
Section GG cont.
• Clarifications: Self–Care & Mobility
• “CMS anticipates that an interdisciplinary team of qualified clinicians is
involved in assessing the resident during the three-day assessment
period.”
• Added “Qualified Clinician” to definition box: “Healthcare
professionals practicing within their scope of practice and consistent
with Federal, State, and local law and regulations.”
• The coding options for Column 2, Discharge Goal, changed to allow
coding of “not attempted” codes: “The use of 07, 09, 10, or 88 is
permissible to code end of SNF PPS stay (discharge) goal(s).”
• A change to code 09, “Not applicable,” “Not attempted and the
resident did not perform this activity prior to the current illness,
exacerbation, or injury.”
• There is a new reason code, code 10, Not attempted due to
environmental limitations (e.g., lack of equipment, weather
constraints).
NADONA
10
5
9/25/2018
Section GG cont.
• In “Assessment Period” text on page GG-11, CMS added more
clarification to “Admission”: “The admission function scores are to
reflect the resident’s admission baseline status and are to be based on an
assessment. The scores should reflect the resident’s status prior to any benefit
from interventions.”
• Residents with cognitive impairments/limitations may need physical
and/or verbal assistance when completing an activity. Code based on
the resident’s need for assistance to perform the activity safely.
• An activity can be completed independently with or without devices. If
the resident uses adaptive equipment and uses the device
independently when performing an activity, enter code 06,
Independent.
• When coding the resident’s usual performance, “effort” refers to the
type and amount of assistance a helper provides in order for the
activity to be completed.
• Code based on the resident’s performance. Do not record the
staff’s assessment of the resident’s potential capability to
perform the activity.
NADONA
11
Section GG cont.
• Section GG Clarifications & Coding Tips
• Self-Eating
– The self-care task of eating has been modified to include liquids
as well as food
– For residents with tube feedings or parenteral nutrition. ▪ Tube
feeding and TPN are not considered a part of the eating item.
CMS provided clarifications for whether tube feeding/TPN was of
new onset or was used prior to admission.
• Oral Hygiene
– “If a resident does not perform oral hygiene during therapy,
determine the resident’s abilities based on performance on the
nursing care unit.”
NADONA
12
6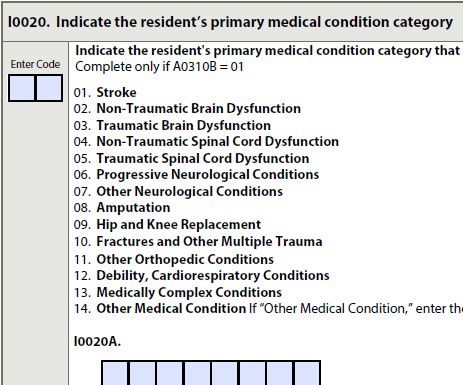
9/25/2018
ADL Scoring
• A resident’s function would be measured using
four late-loss ADL activities & 2 Early Loss ADLs
– (bed mobility, transfer, eating, and toileting)
– (oral hygiene and walking)
• The proposed measure includes:
– GG0130A1—Self-care: Eating - 0–4.
– GG0130B1—Self-care: Oral Hygiene - 0–4.
– GG0130C1—Self-care: Toileting Hygiene - 0–4.
GG0170B1—Mobility: Sit to lying- 0–4 (average of 2
items).
– GG0170C1—Mobility: Lying to sitting on side of bed.
GG0170D1—Mobility: Sit to stand - 0–4 (average of 3
items).
– GG0170E1—Mobility: Chair/bed-to-chair transfer.
GG0170F1—Mobility: Toilet transfer.
– GG0170J1—Mobility: Walk 50 feet with 2 turns - 0–4
(average of 2 items). NADONA
– GG0170K1—Mobility: Walk 150 feet. 13
Section GG Clarifications & Coding Tips cont.
• Toileting Hygiene
– Added “managing undergarments, clothing, and incontinence
products and performing perineal cleansing before and after
voiding or having a bowel movement. If the resident does not
usually wear undergarments, then assess the resident’s need for
assistance to manage lower-body clothing and perineal hygiene.”
– For a resident with an indwelling catheter, base the coding for this
item on the resident’s bowel movements.
NADONA
14
7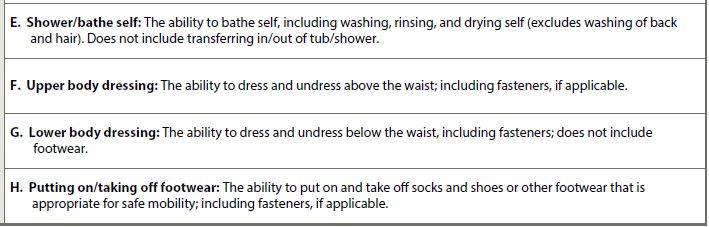
9/25/2018
Section GG Clarifications & Coding Tips cont.
• New Section GG items:
• Coding tips
– Shower/bathe self assessment may take place in a shower, bath, or at a
sink.
– Abdominal binder, back brace, and neck support are coded under upper-
body dressing.
– Ankle or foot orthotics, walking boots, and compression stockings are
coded under footwear.
– CMS provides guidance on coding for residents with single or double lower-
extremity amputations.
– if the helper helps only with buttons or fasteners, this would be considered
touching assistance.
– Knee brace, stump sock on lower extremity, or lower-limb prosthesis would
NADONA
be coded as lower-body dressing. 15
Section GG Clarifications & Coding Tips cont.
• New Mobility Items
A. Roll left and right: The ability to roll from lying on back to left and right side, and return to lying on back on
the bed.
•
NADONA
16
89/25/2018
Section GG Clarifications & Coding Tips cont.
• Clarifications:
– Mobility
• Word safely was removed from several of the
descriptions.
• If bed mobility cannot be assessed because of the degree to
which the head of the bed must be elevated for a medical
condition, then the tasks of Roll left and right, Sit to lying, and
Lying to sitting on side of bed should be coded as 88, Not
attempted due to medical condition or safety concerns.
• The gateway question “Does the resident walk?” has been
removed
– Lying to Sitting on Bed
• Clarification added: “Clinical judgment should be used to
determine what is considered a ‘lying’ position for a particular
resident.” CMS has also added, “If the resident’s feet do
not reach the floor upon lying to sitting, the qualified
clinician will determine if a bed height adjustment is
required.”
NADONA
17
Section GG Clarifications & Coding Tips cont.
• Clarifications cont.
Sit to Stand
• “The ability to come to a standing position from sitting in a
chair, wheelchair, or on the side of the bed.”
– Chair/bed to chair transfer
• Task “begins with the resident sitting in a chair or wheelchair
or sitting upright at the edge of the bed and returning to
sitting in a chair or wheelchair or sitting upright at the edge of
the bed.”
• Mechanical lift coding tip: “If a mechanical lift is used to assist
in transferring a resident for a chair/bed-to-chair transfer and
two helpers are needed to assist with the mechanical lift
transfer, then code as 01, Dependent, even if the resident
assists with any part of the chair/bed-to-chair transfer.”
– “Does the resident use a wheelchair and/or scooter?”
• This item is about the resident who is learning how to self-
mobilize using a wheelchair or who used a wheelchair prior to
admission
• If the resident uses a wheelchair only for transport purposes,
GG0170Q1 and Q3 are to be coded No and the rest of the
NADONA
wheelchair items are skipped.
18
99/25/2018
Section I
• New Item - “Indicate the resident’s primary
medical condition category.”
– Completed only if the MDS is a PPS 5-day assessment.
– The clinical category coded in I0020 must also be included
in items I0100 through I8000 (Active Diagnoses in the Last
7 Days).
– If the hip or knee replacement is secondary to hip fracture,
code as 10, Fractures.
– Additional clarifications for coding “Quadriplegia.”
NADONA
19
Section J
• J2000: Prior Surgery
• Item Rationale
– This item identifies whether the resident has had
major surgery during the 100 days prior to
admission. A recent history of major surgery can
affect a resident’s recovery.
– Meets all of the following criteria for “major” surgery:
1. The resident was an inpatient in an acute care hospital for at
least one day in the 100 days prior to admission to the skilled
nursing facility (SNF),
2. The resident had general anesthesia during the procedure,
and
3. The surgery carried some degree of risk to theNADONA
resident’s life or
the potential for severe disability.
20
109/25/2018
Section K
• For these items:
– K0510C (Mechanically altered diet)
– K0510D (Therapeutic diet)
– K0710A (Proportion of total calories)
– K0710B (Average fluid intake)
• CMS does not require the completion of
column 1, “While NOT a resident,” for the
following items; however, some states
continue to review its completion. If the state
does not require completion, use the standard
“no information” code (a dash [-]):
NADONA
21
Section M
• Change of pressure ulcers/injuries
• The comprehensive care plan should be reevaluated to ensure that
appropriate preventative measures and pressure ulcer/injury
management principles are being adhered to when new pressure
ulcers/injuries develop or when existing pressure ulcers/injuries
worsen.
• Skip Pattern changed
• If two pressure ulcers/injuries occur on the same bony prominence
and are separated, at least superficially, by skin, then count them as
two separate pressure ulcers/injuries. Stage and measure each
pressure ulcer/injury separately.
• If the pressure ulcer/injury was present on admission/entry or reentry
and becomes unstageable due to slough or eschar, during the
resident’s stay, the pressure ulcer/injury is coded at M0300F and
should not be coded as “present on admission.”
• If a pressure ulcer was numerically staged, then became unstageable,
and is subsequently debrided sufficiently to be numerically staged,
compare its numerical stage before and after it was unstageable. If
the numerical stage has increased, code this pressure ulcer as not
present on admission.
NADONA
22
119/25/2018
Section M cont.
• If two pressure ulcers merge, that were both
“present on admission,” continue to code the
merged pressure ulcer as “present on
admission.” Although two merged pressure
ulcers might increase the overall surface area
of the ulcer, there needs to be an increase in
numerical stage or a change to unstageable
due to slough or eschar in order for it to be
considered not “present on admission.”
• Removed M0610-M0900 as of 9/31/18
– Date of Oldest Stage 2 pressure ulcer (M0300B3)
– Dimensions ( M0610A - C)
– Most Severe tissue (M0700)
– Worsening Status (M0800A - F)
– Healed Ulcer (M0900A - D)
NADONA
23
Section M cont.
• Definitions clarified
– M1040D – Lesions / Abrasions
– M1040H – Moisture Associated Skin Damage
– Removed and reworded examples
– M1200G - Application of nonsurgical
dressings
• Added wound-closure strips to examples for “Do not
include adhesive bandages.”
NADONA
24
129/25/2018
Section N
• New Skip Patterns
• N2001 Drug Regimen Review
– Intent: The intent of the drug regimen review items is to
document whether a drug regimen review was conducted upon
the resident’s admission (start of Skilled Nursing Facility [SNF]
Prospective Payment System [PPS] stay) and throughout the
resident’s stay (through Part A PPS discharge) and whether any
clinically significant medication issues identified were addressed
in a timely manner.
NADONA
25
Section N cont.
• Definition of a drug regimen review (DRR) for the MDS is as
follows: ▪ A drug regimen review includes
– medication reconciliation,
– a review of all medications a resident is currently using,
and
– a review of the drug regimen to identify, and
– if possible, prevent potential clinically significant
medication adverse consequences.
• The drug regimen review includes
– all medications, prescribed and over the counter (OTC),
– nutritional supplements,
– vitamins, and
– homeopathic and herbal products,
– administered by any route. It also includes
– total parenteral nutrition (TPN) and oxygen.
NADONA
26
139/25/2018
Section N cont.
• N2001, Drug Regimen Review: Did a
complete drug regimen review identify
potential clinically significant medication
issues?
• Clinically significant medication issues may
include, but are not limited to:
– Medication prescribed despite documented
medication allergy or prior adverse reaction.
– Excessive or inadequate dose.
– Adverse reactions to medication.
– Ineffective drug therapy.
– Drug interactions (serious drug-drug, drug-food, and
drug-disease interactions).
– Duplicate therapy (for example, generic-name and
brand-name equivalent drugs are co-prescribed).
– Wrong resident, drug, dose, route, and time
NADONAerrors.
27
Section N cont.
• Significant Medication Issues cont.
• Medication dose, frequency, route, or duration not
consistent with resident’s condition, manufacturer’s
instructions, or applicable standards of practice.
• Use of a medication without evidence of adequate
indication for use.
• Presence of a medical condition that may warrant
medication therapy (e.g., a resident with primary
hypertension does not have an antihypertensive
medication prescribed).
• Omissions (medications missing from a prescribed
regimen).
• Nonadherence (purposeful or accidental).
•
NADONA
28
149/25/2018
Section N cont.
• N2003: Medication Follow-up
– Integral to the process of safe medication
administration practice is timely communication
with a physician when a potential or actual
clinically significant medication issue has been
identified.
•
– Physician-prescribed/recommended actions in
response to identified potential or actual clinically
significant medication issues must be completed
by the clinician in a time frame that maximizes
the reduction in risk for medication errors and
resident harm.
•
NADONA
29
Section N cont.
• N2005 Medication Intervention – complete
only if Part A Discharge assessment
• Time frame for Notification of Physician with
potential or actual significant medication issue
( Midnight of the next calendar day)
NADONA
30
159/25/2018
Section O
• Medication replaced “drug”.
• Chemotherapy - Hormonal and other agents
administered to prevent the recurrence or slow
the growth of cancer should not be coded in
this item, as they are not considered
chemotherapy for the purpose of coding the
MDS. (Tamoxifen)
• Updated rationale for influenza and
pneumococcal vaccines
• Clarification for Vents (O0100F & O0200G)
– O0100F is now defined as an invasive mechanical
ventilator (ventilator or respirator),
– O0200G is now named a non-invasive mechanical
ventilator (BiPAP/CPAP).
NADONA
31
Appendixes
• Appendix B – Updated State RAI
Coordinators
• Appendix C – Updated Care Areas
Assessments (mostly wording)
– Opioids have been added to the care areas
Delirium, Visual Function, Communication, Activities
of Daily Living, Incontinence, Mood State, Falls,
Dental Care, and Pressure Ulcer/Injury.
– Behavioral Review of Indicators has been updated
significantly with the inclusion of section E items.
– Alarm use has been added as a factor that can
cause or exacerbate behavior
NADONA
32
169/25/2018
Quality
Measures
NADONA 33
Current QMs from the MDS
• The current nursing home quality
measures are:
• Short Stay Quality Measures
• Percent of Residents who Self-Report
Moderate to Severe Pain (Short Stay)
• Percent of Residents with Pressure Ulcers that
are New or Worsened (Short Stay) (9/30/18)
• Percent of Residents Who Were Assessed
and Appropriately Given the Seasonal
Influenza Vaccine (Short Stay)
• Percent of Residents Assessed and
Appropriately Given the Pneumococcal
Vaccine (Short Stay)
• Percent of Short-Stay Residents Who Newly
NADONA
Received an Antipsychotic Medication 34
179/25/2018
Current QMs from the MDS cont.
• Long Stay Quality Measures
• Percent of Residents Experiencing One or
More Falls with Major Injury (Long Stay)
• Percent of Residents who Self-Report
Moderate to Severe Pain (Long Stay)
• Percent of High-Risk Residents with Pressure
Ulcers (Long Stay)
• Percent of Residents Assessed and
Appropriately Given the Seasonal Influenza
Vaccine (Long Stay)
• Percent of Residents Assessed and
Appropriately Given the Pneumococcal
Vaccine (Long Stay)
NADONA
35
Current QMs from the MDS cont.
• Percent of Residents with a Urinary Tract
Infection (Long Stay)
• Percent of Low-Risk Residents Who Lose
Control of Their Bowels or Bladder (Long Stay)
• Percent of Residents Who Have/Had a
Catheter Inserted and Left in Their
Bladder (Long Stay)
• Percent of Residents Who Were Physically
Restrained (Long Stay)
• Percent of Residents Whose Need for Help
with Activities of Daily Living Has
Increased (Long Stay)
NADONA
36
189/25/2018
Current QMs from the MDS cont.
• Percent of Residents Who Lose Too Much
Weight (Long Stay)
• Percent of Residents Who Have Depressive
Symptoms (Long Stay)
• Percent of Long-Stay Residents Who
Received An Antipsychotic Medication
NADONA
37
Claims-Based Short-Stay Measures
• Percentage of residents who were re-hospitalized
after a nursing home admission
– This measure reports the percentage of all new admissions
or readmissions to a nursing home from a hospital where the
resident was re-admitted to a hospital for an inpatient or
observation stay within 30 days of entry or reentry.
• Percentage of short-stay residents who have had an
outpatient emergency department (ED) visit
– This measure reports the percentage of all new admissions
or readmissions to a nursing home from a hospital where the
resident had an outpatient ED visit (i.e., an ED visit not
resulting in an inpatient hospital admission) within 30 days
of entry or reentry.
• Percentage of short-stay residents who were
successfully discharged to the community
– This measure reports the percentage of all new admissions
to a nursing home from a hospital where the resident was
discharged to the community within 100 calendar days of
entry and for 30 subsequent days, did not die, was not
admitted to a hospital for an unplanned inpatient stay, and
was not readmitted to a nursing home NADONA
38
199/25/2018
PDPM Proposed
Changes:
Patient Driven
Payment Method
NADONA 39
MDS & PDPM
• PT Case Mix Group
– Clinical Category (DX) + GG Function Score
• OT Case Mix Group
– Clinical Category (DX)+ GG Function Score
• SLP Case Mix Group
– Presence of Acute Neurological Condition or SLP
– Related Comorbidity + Presence of Swallowing
disorder or Mechanically altered diet
• Nursing Case Mix Group
– Uses Rugs IV (ADLs now based on GG) +
Depression & Nursing rehab end splits
• (NTA)Non-Therapy Ancillary Case Mix Group
– Condition/ Extensive Service (MDS/UB04)
• Non-Case Mix Component
– Set amount for rural & urban
NADONA
40
209/25/2018
Non-Case Set amount
Mix Mix
NADONA
41
MDS Schedule
• Effective 10/1/19
• 5 Day MDS would set the rate for the entire
stay unless IPA completed
• IPA (Interim Payment Assessment) till DC
or next IPA (optional)
– Change in Clinical Condition (Tier 1) to a
different group &
– Would not return to original status within a 14
day period
– ARD would be no more than 14 days after the
change in the tier one classification
– Late and missed guidelines would be followed
• Rates would be adjusted Non-Therapy
Ancillary (NTA) & PT/OT
• Day 3 & Day 20 Rates go down NADONA
42
219/25/2018
Medicare MDS Schedule
Medicare MDS Schedule Assessment reference Applicable standard
date Medicare payment days
5-day Scheduled PPS Days 1–8 All covered Part A days until
Assessment Part A discharge (unless an
IPA is completed).
Interim Payment No later than 14 days after ARD of the assessment
Assessment (IPA) change in resident’s first tier through Part A discharge
classification criteria is (unless another IPA
identified assessment is completed).
PPS Discharge Assessment PPS Discharge: Equal to N/A.
the End Date of the Most
Recent Medicare Stay
(A2400C) or End Date.
NADONA
43
MDS and PDPM
• Interrupted Stay Policy
– If the resident dc to hospital for 4 days the stay
starts over with new 5 day and the payment reverts
to day 1
– If Dc for less than 3 days the stay remains the dame
and the payment continues on to the day of the DC
date.
• Coding of Diagnoses ( I section)
• Therapy
• ADLS (Section GG)
• Swallowing an Mech. Altered Diet (Section K)
• BIMS & CPS ( Section C)
• Services & Diagnoses RUGs
NADONA
44
229/25/2018
Summary
• Need to have experts on coding
• Assessments need to be accurate for 5 day
• 5 day MDS must reflect all services as
might be only chance to set rate
• Need to monitor changes in primary reason
for care
• Monitor length of stay due to decreasing
daily per diems
• Fewer MDS’ - more scrutiny will be needed
• Assessments and documentation created
to obtain information needed for the MDS
NADONA
45
QUESTIONS
Cindy Fronning cindy @ nadona.org
NADONA 46
23You can also read