The role of cytoreductive nephrectomy for mRCC in 2020 - Maarten Albersen Dept. of Urology UZ Leuven with assistance of
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The role of cytoreductive
nephrectomy for mRCC in 2020
Maarten Albersen
Dept. of Urology
UZ Leuven
with assistance of:
Eduard Roussel
Alessandro Larcher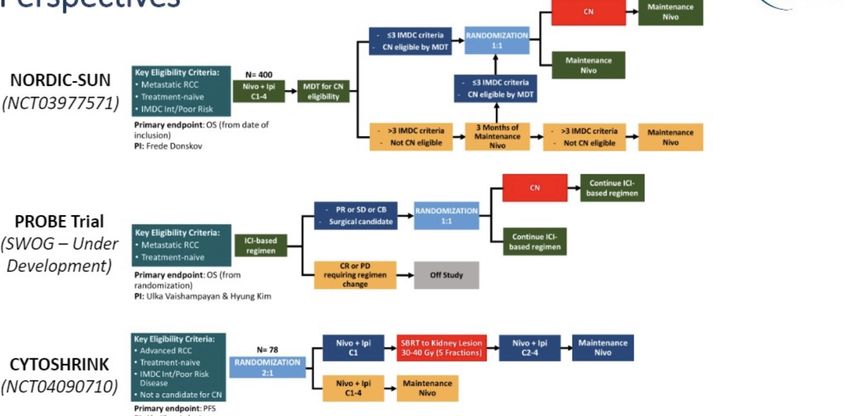
CASE Male, 55 YO Medical history: 2002 pneumonia & TB pleuritis No meds • Presents with macroscopic hematuria / cloth retention in 04/2019 > large tumor Rt kidney with Mayo level 1 thrombus. • Embolisation same night. • Free of symptoms. • CT thorax: multiple pulmonary and pleural mets, bilateral. • IMDC: (before bleeding: 0 risk factors) • What would be your advice on MDT?
CASE 1. AS 2. CN + AS 3. Nivolumab (+- deferred CN) 4. Nivolumab + Ipilimumab (+- deferred CN) 5. Sunitinib (+- deferred CN) 6. Axitinib + Pembrolizumab(+- deferred CN)
What is cytoreductive nephrectomy?
Non-curative nephrectomy in mRCC with the goal of
decreasing total tumorload.
• Often + abdominal metastasectomy/LND
• Upfront or delayed.
• Goals:
• Tumor self-seeding principle: volume reduction
• “abscopal effect” in 2% with metastatic reduction (due to relief of
immune-surpressive effects of primary: immunologic sink)
• Better response with systemic therapy
• Palliation (symptoms/paraneoplastic s)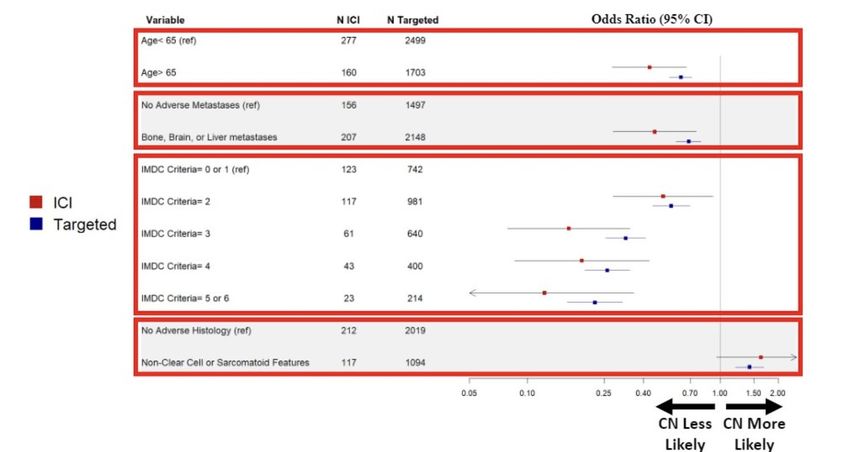
Setting: mRCC
MSKCC-Motzer criteria IMDC-Heng criteria
Diagnosis-systemic therapy < 1 year Diagnosis-systemic therapy < 1 year
PS ULN
LDH > 1.5x ULN Neutrophils > ULN
Platelets > ULN
0 points: favorable OS = 20 months 0 points: favorable OS = 43,2 months
Heng J Clin Oncol 2009 1 or 2 points = intermediate OS = 10 months 1 or 2 points = intermediate OS = 22,5 months
Motzer J Clin Oncol 2002 >2 points = high risk = 4 months >2 points = high risk = 7,8 months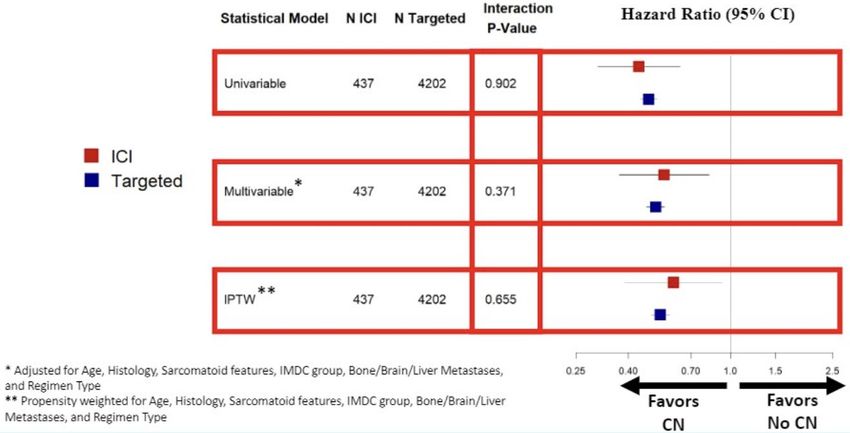
Historical perspective: IFN era
Prospective RCT
Low metastatic load
PS: ECOG 0
Flanigan et al. NEJM 2001
Mickisch et al. Lancet 2001
> Flanigan et al. J Urol 2004
TKI era
Choueiri 2011 Heng 2014 Hanna 2016
Retrospective
Inherent selection bias with CN
Choueiri et al. J Urol 2011
Heng et al. Eur Urol 2014
Hanna et al. JCO 2016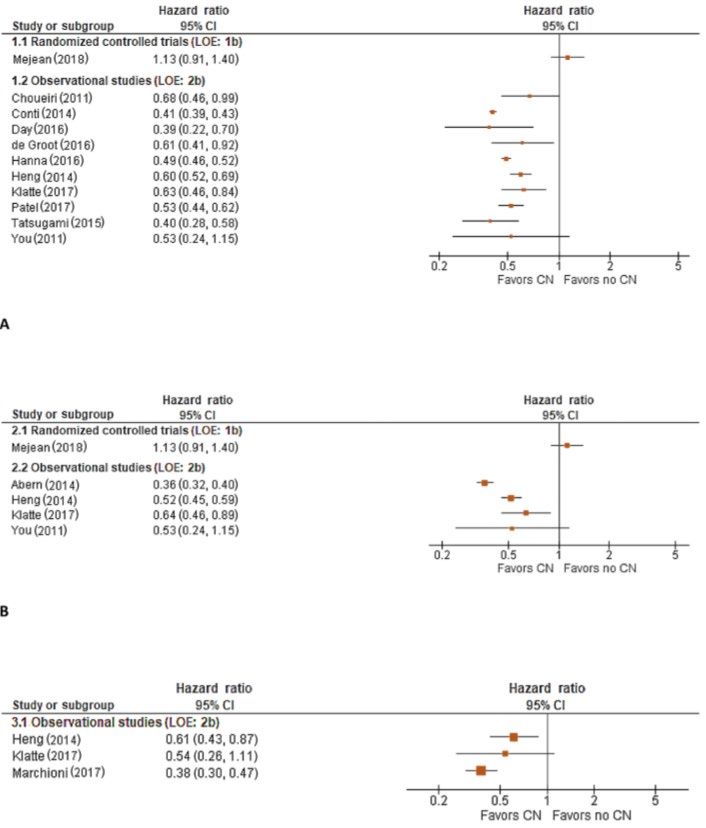
TKI era
Only CN for patients with
life expectancy >12 months
Max 3 IMDC criteria
Heng et al. Eur Urol 2014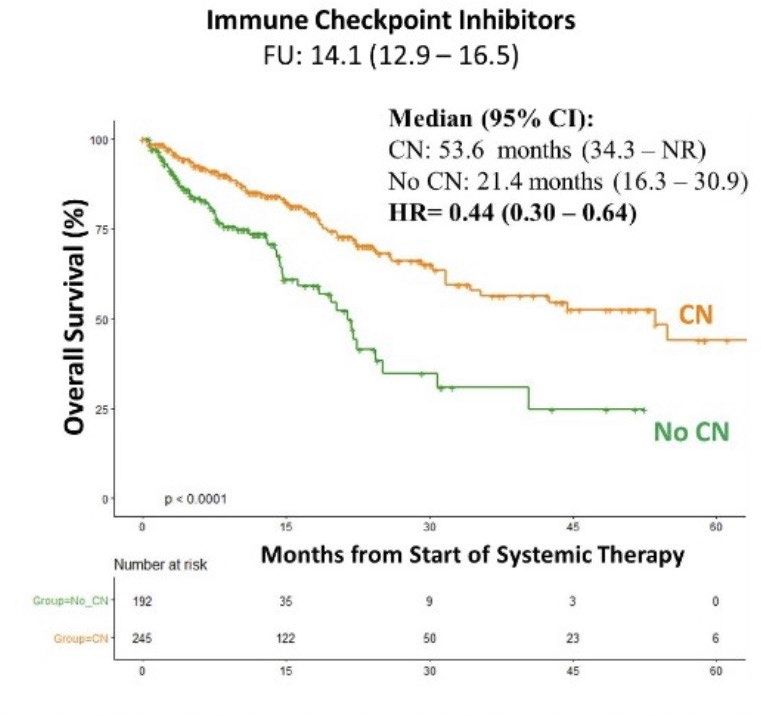
EAU guidelines 2018
CARMENA
3-6
N=226 weeks Subitinib
CN
N=450 50 mg QD 4/2
Key eligibility Criteria
mCCRCC Tx naive Randomization
MSKCC int/poor risk 1:1 Stable disease: 18%
ECOG PS 0-1
Stratification Sunitinib
MSKCC risk groups CN
50 mg QD 4/2
Primary endpoint: OS Centre N=224
Design: non inferiority (HR OSCARMENA Major adverse events in favour of CN + Sunitinib
(net reduction -10%, p=0.04)
Mejean et al - NEJM 2018CARMENA: limitations
Population at high risk:
Survival rates poorer than expected (14-18 mos vs 21.8-
26 mos in Motzer & Chouieri. 43% poor-risk
Slow accrual:
• N= 450/576, accrual 0.7 pts/site/yr
• Need to open UK centres: after accrual open in 26
sites around UK, only 14 patients were enrolled
• Ideal patients for CN did not consent, underwent CN
outside of study, exlucions at investigators discretion
Sunitinib arm:
11/224 (5%) did not recieve Sunitinib
38/213 (18%) underwent CN (median 11 months)
CN+ Sunitinib arm
40/226 (18%) did not receive sunitinib
Mejean et al - NEJM 2018 / Stewart et al. Eur Urol – 2017 / Motzer NEJM 2018 / Chouieri JCO 2017
16/186 (9%) did not receive CNCARMENA: is this the patient we
would typically do CN on?
Arora et al. Eur Urol - 2018CARMENA No survival advantage retrospective 5 - 18 months survival advantage following CN Larcher et al - Eur Urol Oncol 2019
CARMENA in current literature
ccRCC
nccRCC
Bhindi et al - Eur Urol 2019CARMENA: subanalyses: delayed CN (OS)
Response as a Litmus test
SURTIME
15.7 mo 48.5 mo
Mejean et al ASCO 2019SURTIME
N=50
CN Subitinib
N=99 50 mg QD 4/2
Key eligibility Criteria
mCCRCC Tx naive Randomization
ECOG PS 0-1 1:1
Stratification Sunitinib Sunitinib
WHO performance status 50 mg QD 4/2 CN
Primary endpoint: PFS ITT (sec:OS) N=49 3 cycles
50 mg QD 4/2
N (powercalc): 458
PI: Axel Bex
Sponsor: EORTC
Not eligble for CN due to
progression: 29%
Bex et al. Jama Oncology 2018SURTIME
Patients who:
Progress
under TKI
Do not benefit
from CN
Safety: no increase of peri-operative outcomes in deferred CN
Bex et al. Jama Oncology 2018Safety of CN: YAU and Leuven cohorts
Postoperative complications CDC (1-5): 29,5% Postoperative complications CDC (1-5): 42%
• High-grade postoperative complications CDC (3-5): 6,1% • High-grade postoperative complications CDC (3-5): 2,3%
• Surgery-related mortality: 1,4% • Surgery-related mortality: 0%
YAU (n=736) Leuven (n=86)
Cardiopulmonary: 5,3% Neurologic: 3,4%
Neurologic: 1,0% Cardiopulmonary: 4,7%
Vascular/Lymphatic: 9,1% Vascular/Lymphatic: 16,3%
Wound/Skin: 1,8% Wound/Skin: 3,4%
Infectious/Metabolic: 8,8% Infectious/Metabolic: 17,4%
Gastrointestinal: 4,5% Gastrointestinal: 9,3%
Predictors for High-grade postoperative morbidity
• Estimated intraoperative blood loss: HR 2.93 (1.20-7.15)
• CN case load: HR 0.13 (0.03-0.59)CARMENA: subanalyses: 1 IMDC risk factor
Median OS (months) ARM A: CN + Sunitinib ARM B: Sunitinib alone HR (95% CI) P-value
(n=127) (n=139)
IMDC 1 risk factor 31.4 (17.3-45.5) 25.2 (19.6-35.4) 1.29 (0.85-1.98) 0.232
IMDC 2 risk factors 17.6 (13.7-21.5) 31.2 (20.5-40.4) 0.63 (0.44-0.97) 0.033
HR (95% CI) 1.68 (1.10-2.57) 0.88 (0.59-1.30)
P-value 0.015 0.515
Mejean et al ASCO 2019UZ Leuven experience (E. Roussel & A. Verbiest)
CARMENA TKI (26) CARMENA practice changing:
intermediate/poor risk with need for
CARMENA CN-TKI (44)
immediate TKI
TOO GOOD FOR CARMENA There is still a population likely
CN+AS (49) benefitting from CNUZ Leuven experience (E. Roussel & A. Verbiest)
Patients with:
Lung only mets
Single site mets
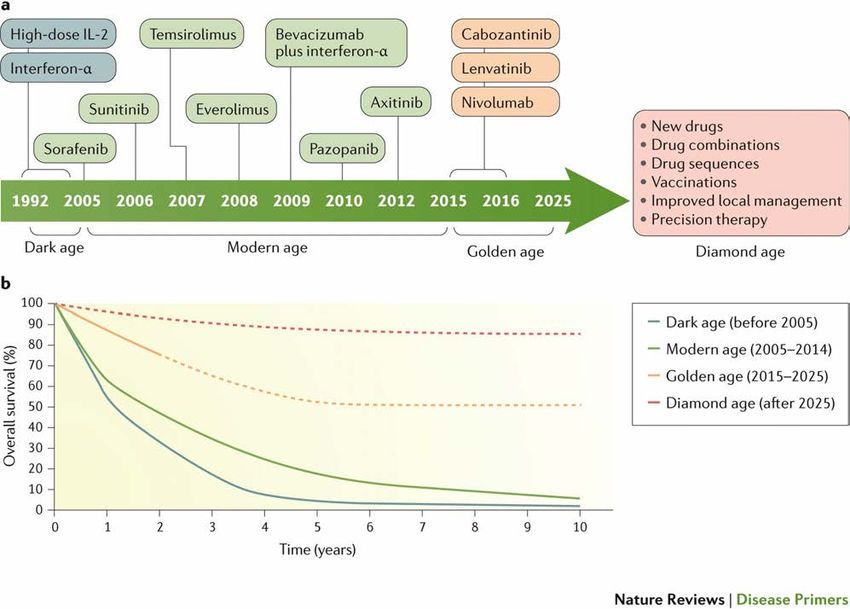
OligometastasisHowever, all these numbers are
OUTDATED (2020)
New backbone in
all risk groups:
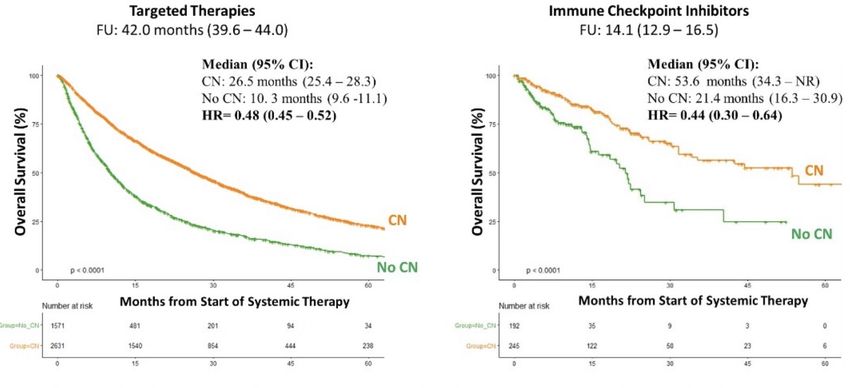
(TKI+) IOIMDC analysis on CN in IO era (ASCO-GU20)
inverse probability treatment weighted propensity scored analysis
Which patients got CN in IO era?IMDC analysis on CN in IO era (ASCO-GU20) inverse probability treatment weighted propensity scored analysis
IMDC analysis on CN in IO era (ASCO-GU20) inverse probability treatment weighted propensity scored analysis
Perspective:
Summary YES, the role of CN has drastically changed after CARMENA • No more upfront CN in intermediate (2 IMDC) and poor risk patients. • Deferred CN has become a valid option with response as litmus test. Upfront CN still is recommended • In symptomatic patients • In IMDC 0-1 favourable/intermediate risk • In oligometastatic patients • In patients in which all tumor can be surgically resected • Probably in the same population combined with IO/IO-TKI
CASE Male, 56 YO Medical history: 2002 pneumonia & TB pleuritis No meds 10 months post-CN: Regression of lung mets (CR)
Primary mCCRCC
Take home: MDT
Requiring and Not immediately requiring
eligible for IO/TKI IO/TKI
IMDC poor IMDC intermediate Oligometastasis
2 factors 1 factor
Ipi-Nivo / Axi-Pembro CN CN
Response
Metastasis
AS
directed Tx
Progressive IMDC
Deferred CN disease favorable
IMDC intermediate / poor Axi-
Pembro
Adapted from: Kuusk et al. Ther Adv Med Oncol 2019You can also read