Transgender Hormone Therapy - April 7th, 2022 Caleb Schmid, MD Assistant Professor
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

OHSU
CPD
Transgender Hormone
Therapy
April 7th, 2022
Caleb Schmid, MD
Assistant Professor
OHSU Endocrinology, Diabetes, and Metabolism
OHSU
Objectives
1. Increase awareness and comfort with gender-affirming care.
2. Learn strategies for initiation of gender-affirming hormone therapy.
CPD
3. Identify misconceptions and considerations when starting hormone therapy.
4. Interactive discussion concerning gender-affirming hormone therapy
2
OHSU
Resources
▪Endocrine Society Guidelines on Treatment of Gender-Dysphoric/Gender-Incongruent Persons
▪UCSF Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender
Nonbinary People
CPD
▪World Professional Association for Transgender Health (WPATH) Standards of Care for the
Health of Transgender and Gender Diverse People, V8
3
OHSU
Definitions
Gender/Gender identity: A person’s internal sense of self-representation as male or female.
Sex: Having attributes that historically characterize “maleness” or “femaleness”, such as gonads,
sex hormones, sex chromosomes, internal/external genitalia, secondary sex characteristics*
CPD
Cisgender: Congruence with sex and gender.
Transgender: Gender identity differs from sex assigned at birth.
Non-binary: transgender or gender non-conforming person who identifies as neither male nor
female.
4
OHSU
Other Terminology
Trans-masculine: gender non-conforming or
non-binary with masculine spectrum gender
identity
Trans-feminine: toward female spectrum
CPD 5
OHSU
Creating a welcoming environment
Transgender patients have faced discrimination
◦ May avoid seeking healthcare
◦ Have led to negative adverse health outcomes
Ask the patient how they would like to be addressed
CPD
◦ Use preferred name
◦ Pronouns - he/him, she/her, they/them
Cultural humility
◦ Patients may have different experiences from yourself or others
Apologize if there is any misunderstanding
6
OHSU
What is “Gender dysphoria”?
American Psychiatric Association DSM-5 definition:
Clinically significant distress or impairment related to gender incongruence, which may include
desire to change primary and/or secondary sex characteristics.
CPD
Outdated terms
◦ Gender identity disorder
◦ Transsexual
ICD-11
◦ Gender incongruence: Gender identity and/or gender expression differs from what is typically
associated with the designated gender.
7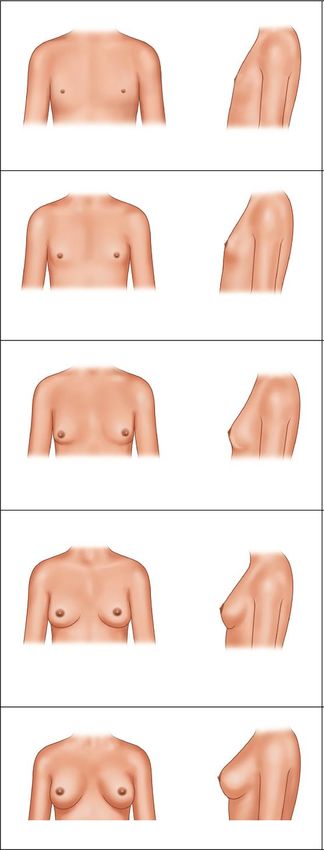
OHSU
Historically a “referral letter” from a mental health
professional was required prior to initiation of hormone
Only mental therapy.
health ◦ Led to a perception of gate-keeping, especially given shortage of
mental health professionals.
professionals can
evaluate for Informed consent model
◦ Discuss risks, benefits, alternatives, limitations.
gender ◦ Be able to distinguish between gender dysphoria and body
dysmorphia.
CPD
dysphoria/ ◦ Minimal risk of regret and no known malpractice cases in a
study performed by 12 major clinics.
gender
incongruence. WPATH Guidelines
“With appropriate training, feminizing/masculinizing
hormone therapy can be managed by a variety of providers,
including nurse practitioners and primary care physicians.”
8
OHSU
Transgender Care and Oregon
Oregon is perceived as more friendly to transgender care
◦ 2015 Oregon Health Plan included informed consent hormone therapy
◦ 2017 policies made legal name change and gender changes on legal documents to
CPD
identify as non-binary
◦ 1 of 14 states with high LGBTQ Policy Tally and Gender Identity Policy tally
Some residents of other states are moving to Oregon for a more inclusive environment
9
OHSU
Case 1
Alexis is a 29 year old transgender female who presents to clinic to discuss
gender dysphoria
◦ First identified as female at age 10, discussed openly with family at age 14
CPD
◦ During puberty, began to feel uncomfortable with changes in voice, increased body hair, etc.
◦ In high school, had significant depression and suicidal ideation associated with gender.
◦ Every time they would look in the mirror, feels like “it does not look like me.”
◦ Has been presenting as female to family, friends, co-workers since after college.
10OHSU
Case #1
Long-standing history (>6 months) of dysphoria
Currently expressing their gender identity
CPD
Desire to change secondary sex characteristics
11OHSU
When to ask for mental health
Inconsistent gender identity
◦ Patient is unsure, or is relatively recent
CPD
Evidence of other mental health condition contributing
◦ E.g. depression, bipolar disorder, recent psychosis
Elements of body dysmorphia
◦ Single or multiple perceived flaws in appearance
12OHSU
At 0.3-0.6% of the population, about 2 million
transgender patients in the USA
Only ◦ About 6,000 endocrinologists in the US
◦ 39% are ≥ 55 years old
endocrinologists
can prescribe ◦ About 300 patients per endocrinologist
hormones for ◦ But not all of these endocrinologists practice gender-affirming
hormone therapy (e.g. Diabetes-only practices)
gender-affirming
CPD
◦ Endocrinologists have a lot of other hormone referrals
hormone
therapy. Most medications used in gender-affirming hormone therapy are
commonly used for other conditions
◦ Contraception
◦ Menopause
◦ Hirsutism/PCOS
◦ Male pattern baldness
◦ Prostate dysfunction
13OHSU
Initial Evaluation
❑History of gender identity
❑Support system
Family, friends, co-workers, mental health providers
CPD
❑Challenges patient has faced or barriers they may see
❑Goals of therapy
❑History of prior medication use
❑Fertility plans
❑Expectations of hormone therapy
14OHSU
Feminizing Hormone Therapy
Goals
◦ Female secondary sex characteristics
◦ Minimization of male secondary sex characteristics
CPD
General Effects
◦ Breast development – typically Tanner stage 2 or 3
◦ Redistribution of subcutaneous fat of the face and body
◦ Reduced body hair
◦ Reduce, potentially reverse androgen-mediated hair loss
15OHSU
Feminizing Hormone Therapy
Sexual and Gonadal Effects
◦ erectile function
◦ ∆ libido
◦ sperm count and ejaculatory fluid
CPD
◦ testicular size
16OHSU
General Feminizing Therapy
Estrogen + Androgen blocker
+/- progesterone
CPD 17OHSU
Estrogens
Primarily 17β estradiol
◦ Bioidentical to ovarian-produced estradiol
◦ Similar to goals in agonadal (e.g. Turner syndrome) or
CPD
menopausal states
Conjugated equine estrogens (Premarin) not
recommended
Ethinyl estradiol not recommended
18OHSU
Estrogen Side effects
oMigraines
oMood swings
CPD
oHot flashes
oWeight gain
19OHSU
Considerations prior to estrogen therapy
• Age
• Tobacco use
• Migraines +/- aura
CPD
• Family History
oBreast, ovarian, uterine cancer
oStroke
oDVT/PE
20OHSU
CPD
Estradiol Formulations
21OHSU
Oral estradiol
oInitial: 2-4 mg/day (Low = 1mg/day)
oMax: 6-8 mg/day
CPD
oIf >2 mg, divided in twice daily dosing
Readily available, cheap, easy to take
22OHSU
Estradiol patches
◦ Initial: 100 mcg
◦ Max: 100-400 mcg/day
CPD
◦ New patch must be placed every 3-5
days
◦ Low risk of VTE
◦ Recommended in patients >45 years old,
high VTE risk
23OHSU
IM Estradiol
Estradiol valerate
◦ Initial: 20 mg every 2 weeks
(10 mg weekly)
◦ Max: 40 mg every 2 weeks
CPD
(30 mg weekly)
Estradiol cypionate
◦ Initial: 2 mg every 2 weeks
◦ Max: 5 mg every 2 weeks
Not used outside of transgender therapy = less availability
24OHSU
CPD
Anti-androgens
25OHSU
Spironolactone
◦ Most commonly used
◦ At higher doses has a direct anti-androgen receptor effect & testosterone
production
CPD
◦ Common side effect = gynecomastia
◦ Initial: 25-50 mg daily
◦ Max: 100-200 mg twice daily
Monitor for hyperkalemia every 3 months for 1st year, yearly following
26OHSU
5α reductase inhibitors
Finasteride
◦ 1 mg daily approved for male-pattern baldness
◦ 5 mg daily for benign prostatic hypertrophy
CPD
Dutasteride
◦ 0.5 mg daily
◦ More effectively blocks type 1 enzyme in hair follicle, may have greater
feminizing effect
Good choice for patients that cannot tolerate spironolactone or partial
feminization.
27OHSU
Other anti-androgens
Cyproterone acetate
◦ Synthetic progestogen, strong anti-androgen activity
◦ Not available in the US – rare fulminant hepatitis
CPD
Bicalutamide
◦ Direct anti-androgen used for prostate cancer
◦ Risk of liver dysfunction, including fulminant hepatitis
◦ Does not outweigh benefits in gender-affirming care
28OHSU
CPD
Progestagens
29OHSU
Progestagens
No well-designed studies of the role of progestogens in feminizing hormone
therapy.
CPD
Anecdotally, patients and providers have noted increased breast development,
improvement in mood, or libido.
◦ Effects on mood are variable, with some patients having negative effects
Theoretical androgenizing effects
30OHSU
Micronized progesterone (Prometrium)
Initial: 100 mg nightly
Max: 200 mg nightly
CPD
May be used in cyclical 12 days a month to mimic cycle, but no clear
evidence of benefit.
31OHSU
Medroxyprogesterone acetate (Provera)
Initial: 5 mg nightly
Max: 10 mg nightly
CPD
Concerns regarding CV disease and breast cancer in Women’s Health
Initiative Study, but may not apply to transgender women.
◦ Population was older, post-menopausal women
◦ Used equine estrogens
◦ Breast cancer risk lower
32OHSU
CPD
Goals and Monitoring
33OHSU
Estradiol
Check every 3-6 months
Make adjustment based on level
CPD
Goal: 100-200 pg/mL
Once stable, continue dose
With injectable formulation, check mid-cycle
Labs may use male reference range, which is not appropriate
34OHSU Testosterone Check every 3-6 months, until stable at goal Goal:
OHSU
Other Labs
Creatinine, BUN, K+
◦ Baseline, every 3-6 months initially on spironolactone
◦ Every 6-12 months following
CPD
Lipids
◦ Based on UPSTF guidelines
Prolactin
◦ If symptoms of prolactinoma – lateral visual field loss, galactorrhea, new HA
36OHSU
Screening
Mammogram
◦ Age >50
◦ After at least 5 years of feminizing therapy
CPD
◦ Every 2 years
DEXA
◦ Start at age 65
◦ s/p orchiectomy and history of at least 5 years without hormone
replacement
37OHSU
Managing Expectations
• Focus on how the patient feels on therapy
• Maximum breast growth can take up to 2 years
CPD
• No change in bone structure or voice from hormone therapy
• Increase in fat, reduced muscle mass
38OHSU
CPD
Endocrine Society Guidelines 2017 39OHSU
CPD
Masculinizing Therapy
40OHSU
Case 2
Andy is a 27 year old transgender male
◦ Reports when he was a child always wanted to play with the boys
◦ Described themselves as a “tom-boy”
CPD
◦ Always felt more comfortable in boy’s and men’s clothing
◦ In puberty, developed depression and self-mutilation after they started
menstruating and breast development started
◦ In high school thought they were lesbian
41OHSU
Testosterone therapy
Goals
◦ Development of male secondary sex characteristics
◦ Reduction in female sex characteristics
CPD
Effects
◦ Increased facial and body hair
◦ Deepening of the voice
◦ Redistribution of facial and body fat
◦ Increased muscle mass
42OHSU
Side effects
•Change in sweat/odor
•Increased acne
•Frontal/temporal hairline recession
CPD
•Male pattern baldness
43OHSU
Sexual/Gonadal Effects
•Increase in libido
•Clitoromegaly
•Vaginal dryness
CPD
•Cessation of menses
44OHSU
CPD
Endocrine Society Guidelines 2017 45OHSU
Testosterone
CPD
Preparations
46OHSU
IM/SubQ Injections
Testosterone cypionate (200 mg/mL)
Testosterone enanthanate
CPD
Initial: 20-50 mg weekly (0.1-0.4 mL)
Max: 100 mg weekly
Recommend 18 g needle for drawing up
22-25 g for injection
47OHSU
Topical
Come in pump or packet form
Applied to upper arms/shoulders in the morning
Remain dry for at least 2 hours
CPD
1% gel
◦ Initial: 25-50 mg
◦ Max: 100 mg
1.62% gel
◦ Initial: 20.25 mg (1 pump
◦ Max: 103.25 mg (5
Avoid contact of the gel with others
48OHSU
Testosterone patches
Have been discontinued by the
manufacturer
◦ Only one manufacturer
CPD 49OHSU
Testosterone levels
Check testosterone every 3-6 months
Consider SHBG
CPD
Goal: middle of male reference range
◦ Typical range = 300-800 ng/dl
Once stable, monitor every 6-12 months
50OHSU
Other labs
Hemoglobin and Hematocrit
◦ Check every 3 months initially
◦ Evaluate for erythrocytosis using male range
CPD
◦ Goal HctOHSU
Cardiovascular risk
Long-term studies from The Netherlands
◦ No increased cardiovascular mortality
Insufficient data to assess risk of MI, stroke,
CPD
death, or VTE in transgender males
52OHSU
Non-binary/Gender non-conforming
•Pronouns can vary. Write down patient preference and refresh your
memory before clinic.
oThey/Them
oZe/Zir
CPD
oXe/Xem, etc.
•Patient’s goals are important.
•Goal for at least low-normal of a specific gender range for bone
health.
53OHSU
Take away points
•Transgender hormone initiation is similar to replacement in
agonadal/hypogonadal state.
CPD
•All medications used are common in the primary care setting for
treatment of other conditions.
•Goals are patient specific, as long as they are within a minimum and
maximum of intended gender range.
54OHSU
Feminizing HRT Quick Tips
STARTING DOSES FOLLOW UP
1. Estradiol oral: 2 mg-4mg po daily Metabolic panel (especially for potassium),
testosterone and estradiol levels q 3 months
Estradiol valerate: 10 mg IM q 2 weeks (Available until labs are stable and at goal
in 10 mg/mL, 20 mg/mL, 40 mg/mL
CPD
concentrations) Estradiol: up to 100-200 pg/mL
Estradiol cypionate: (5 mg/mL): 2.5 mg IM q 1-2 Total testosterone: 50 and after 5-10 years of feminizing
2. Spironolactone: 25-50 mg po BID hormone use
(more options for antiandrogens in Endo Society Prostate cancer screening as appropriate
Guidelines)
Adapted from Quick Sheet courtesy of Dr. Milano of OHSU Transgender Health 55OHSU
Masculinizing HRT Quick Tips
STARTING DOSES FOLLOW UP
*Testosterone cypionate (200 mg/mL) or Consider lipids, CBC and total testosterone
enanthate (200 mg/mL): every 3 months until labs are stable and at
goal:
CPD
• 200 mg IM q 2 weeks
Total testosterone: Normal male reference
• 100 mg IM/SQ q week range (about 400-700 ng/dL)
Hct:OHSU
References
•Wylie C Hembree, Peggy T Cohen-Kettenis, Louis Gooren, Sabine E Hannema, Walter J Meyer, M
Hassan Murad, Stephen M Rosenthal, Joshua D Safer, Vin Tangpricha, Guy G T’Sjoen, Endocrine
Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice
Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 102, Issue 11, 1 November
2017, Pages 3869–3903, https://doi.org/10.1210/jc.2017-01658
CPD
•UCSF Gender Affirming Health Program, Department of Family and Community Medicine, University
of California San Francisco. Guidelines for the Primary and Gender-Affirming Care of Transgender and
Gender Nonbinary People; 2nd edition. Deutsch MB, ed. June 2016. Available at
https://transcare.ucsf.edu/guidelines.
•E. Coleman et al (2022) Standards of Care for the Health of Transgender and Gender Diverse People,
Version 8, International Journal of Transgender Health, 23:sup1, S1
S259, DOI: 10.1080/26895269.2022.2100644
57You can also read

















































