Update on Liposarcoma - Bone and Soft Tissue Session 2 APIAP 2015 Brisbane Australia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Update on Liposarcoma Bone and Soft Tissue Session 2 APIAP 2015 Brisbane Australia Dr Eric Song Trainee, Healthscope NSW
History 77 year old male, Lung deposit
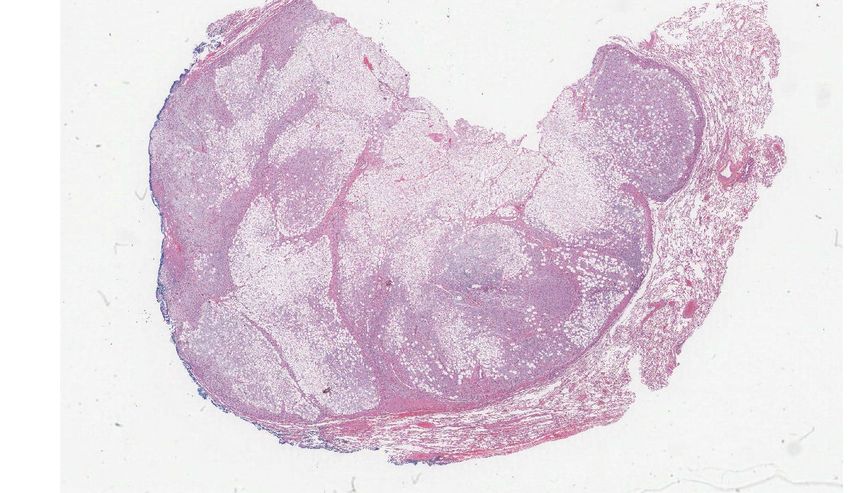
History 77 year old male, Lung deposit

History 77 year old male, Lung deposit

History 77 year old male, Lung deposit

History untold……
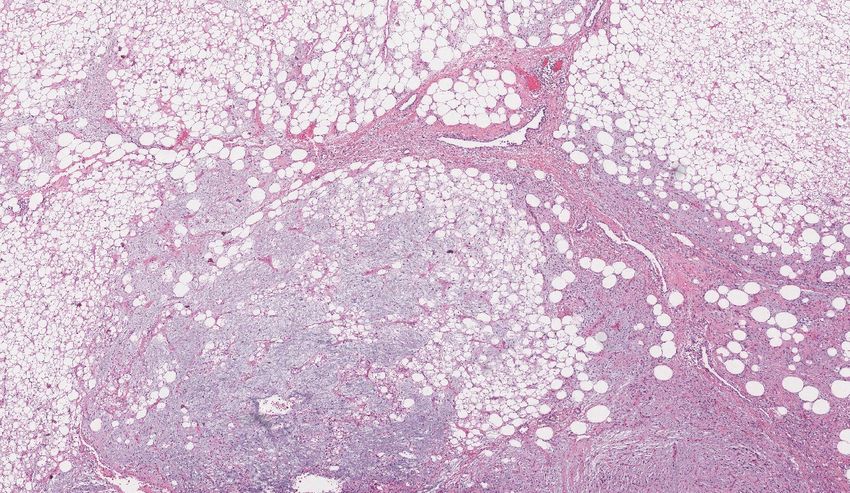
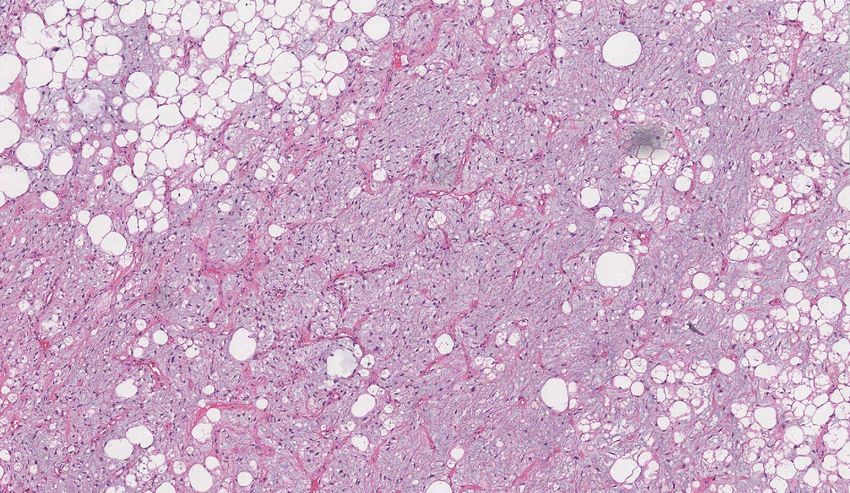
• History of well differentiated liposarcoma with areas of
myxoid dedifferentiation.
• Retroperitoneal in location.
• FISH MDM2 showed amplification.
• Makes myxoid liposarcoma impossible.
• Final diagnosis was…
Dedifferentiated liposarcoma
Features mimicking
myxoid liposarcoma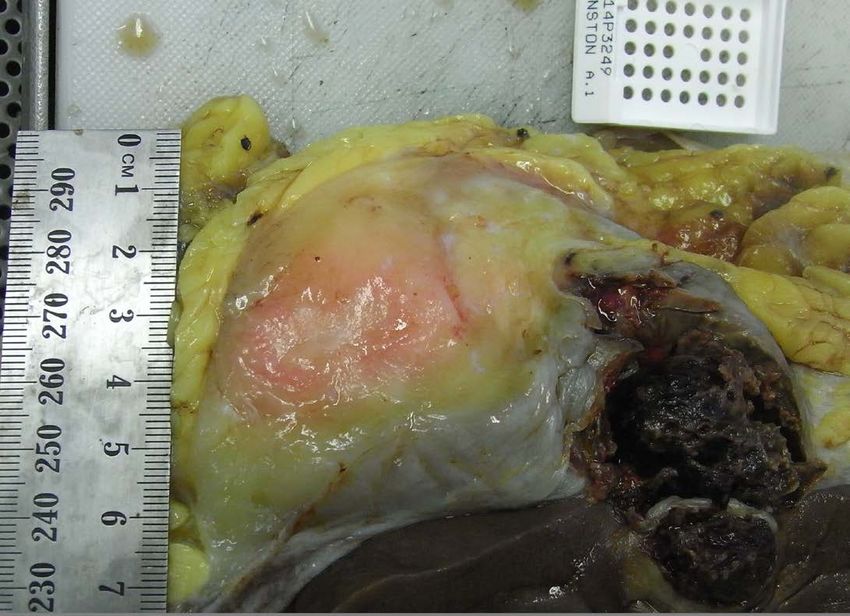
Ancillary testing on retroperitoneal lesion
Fluorescence in-situ hybridization showing high-level
amplification of the MDM2 locus in a dedifferentiated liposarcoma
with prominent myxoid stroma. Chromosome 12 centromeric probe
(CEP12) was used as a control probe (Sioletic 2013).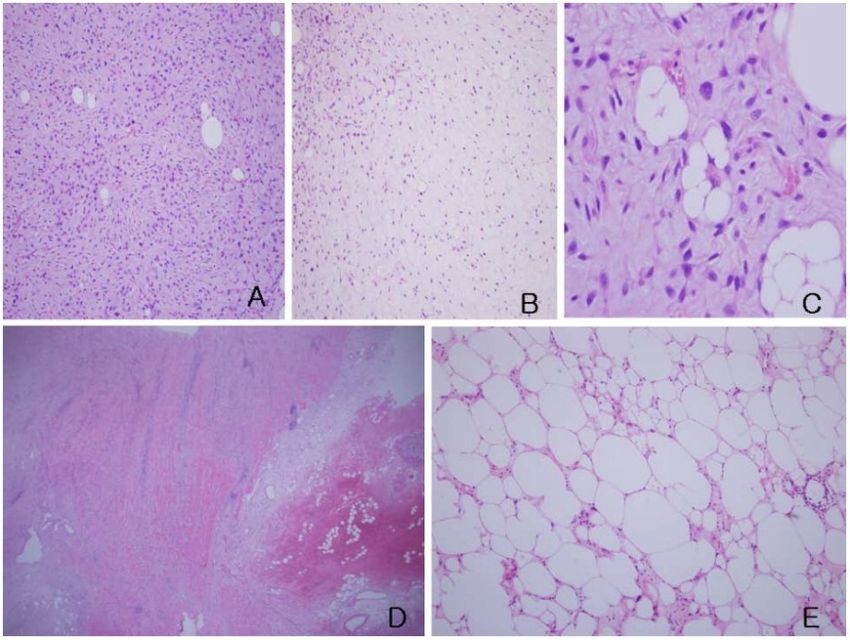
•56 cases of WDLS/DDLS with Myxoid stroma. •95% MDM2, 78% CDK4. •FISH MDM2 positive. •Clinical presentation is important.
Dedifferentiated Liposarcoma
“Magic face changer”Liposarcoma
• The most common soft tissue
malignancy (Hornick 2013).
• First described by Virchow
(Virchow 1865).
• Current WHO – 4 types
(Fletcher 2013).
o Atypical lipomatous
tumour/Well differentiated
liposarcoma
o Dedifferentiated liposarcoma
o Myxoid liposarcoma
o Pleomorphic liposarcoma
“Mammoth Tumor” (Delmaster, 1859)Atypical Lipomatous Tumour /
Well differentiated Liposarcoma
• 40% of all liposarcomas (Fletcher
2013).
• Variable sized atypical adipocytes
in septae and vessels.
• Lipoblasts not essential.
• IHC – MDM2, CDK4.
• FISH – amplification of MDM2.
• Supernumerary ring/giant rod
chromosomes with amplified
segments 12q13-15 (Rosai 1996).
• ALT/WDLS – site dependent with
different prognosis.
Ring chromosomes (black arrows) or
giant marker chromosomes (white
arrows) (Rosai 1996).Recent WHO Changes 2013, ALT/WDLS
• Lipoblasts are not
necessary for
diagnosis.
• ALT – intermediate
prognosis category
due to zero 5 year
mortality.
Well differentiated liposarcoma with variation in adipocyte size,
hyperchromatic nuclei, and scattered lipoblasts (Fletcher 2013).Myxoid Liposarcoma
• 35% of liposarcomas (Fletcher
2013).
• Spindle or ovoid cells with
lipoblasts within myxoid matrix
with chicken wire vessels.
• Specific reciprocal chromosome
translocation t(12;16)(q13;p11)
resulting in rearrangement of
DDIT-3 gene (Crozar 1993).
• IHC – S100 (80%), Tp53 (30%).
• Prognosis - Area of cellularity
(round cells). May be subjective
without clear guidelines.
Myxoid liposarcoma (Fletcher 2013)Recent WHO Changes 2013, MLS
• Round cell liposarcoma
deleted.
• Term “Round cells”
somewhat misleading.
• “Round cells” represent
more poorly differentiated
MLS (Dei Tos, 2000).
Hypercellular area of round undifferentiated cells in myxoid
liposarcoma usually begins around blood vessels (Del Tos 2014).Pleomorphic Liposarcoma
• Rare, 5% of liposarcomas
(Hornick 2013).
• Limbs of older patients, less
likely paratesticular or
retroperitoneal.
• High-grade pleomorphic
morphology with
pleomorphic lipoblasts.
• Molecular or IHC NOT helpful
(Gebhard 2002).
• Prognosis – 50% 5 year
Pleomorphic liposarcoma (Fletcher 2013)
survival.Dedifferentiated Liposarcoma
• First described by Evans (Evans
1979).
• High grade non-lipogenic
sarcoma arising from WDLS.
• Metastatic potential (15-20%).
• Same molecular characteristics
as WDLS (MDM2 amplification).
• Diagnosis usually easy because
of sharp distinction between low
and high grade areas, when
sampled adequately.
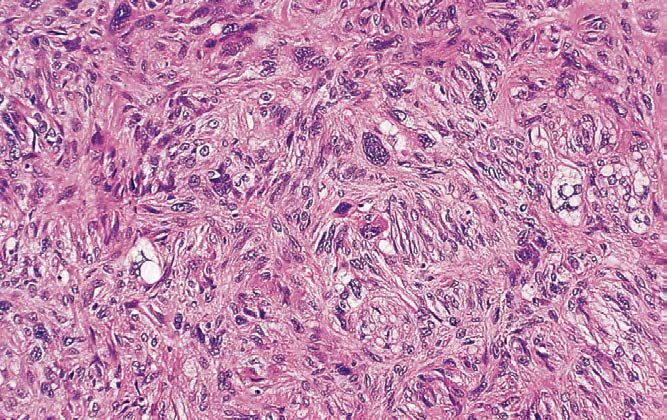
Dedifferentiated liposarcoma with typical
non-lipogenic spindle cell lesion with MFH
like areas and lipoblasts (Mario-Enriquez
2010).Adequate Representative Sampling
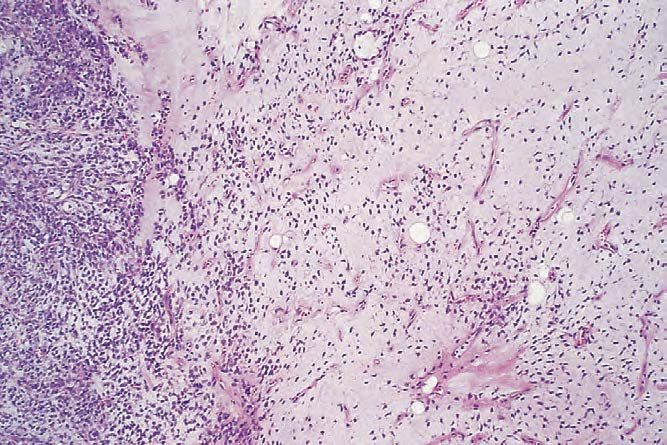
Dedifferentiated Liposarcoma - Difficulties
• Transition may not be clear cut.
– Gradual
– Intermingled
Well delineated DDLS from
WDLS (Fletcher 2014)
Image provided
by Fiona MacleanDedifferentiated Liposarcoma - Difficulties
o Low grade dedifferentiation
(Liau 2015).
o Lipoblastic homologous
differentiation (Mario-
Enriquez 2010).
o Osseus (Chondros 2015).
o Myogenic (Gronchi 2015).
o Chondroid (Longano 2014).
o Meningothelial-like
(Fanburg-Smith 1998;
Nasimento 1998; Li 2005).Image provided by Fiona Maclean
Recent WHO Changes 2013, Mixed type LPS
• Mixed type liposarcoma
deleted.
• Not a true entity
• May represent unusual
morphological patterns
of dedifferentiated
liposarcoma (Fletcher
2014).
Primary mesenteric liposarcoma diagnosed as “mixed-type” (Choi, 2010)Summary • Pathologists should be aware of the new concepts and terminologies. • Advances in cytogenetics have helped delineate LPS categories. • Accurate diagnosis require both morphologic and molecular features. • Treatment and prognosis depend on accurate diagnosis.
Targetted therapy
• Trabectedin (modulates oncogenic
fusion proteins of translocation
related sarcomas) for MLS (Manji
2015).
• CDK4 (VanArsdale 2015).
– Palbociclib (Pfizer)
– Ribociclib (Novartis)
– Abemaciclib (Lilly)
• HGFR (Met) for DDLS (Bill 2015).
• HDACi (MDM2-p53) (Ou 2015).Summary
• ALT is now intermediate prognostic category.
• Dedifferentiation can be low or high grade.
• Heterologous or homologous.
• Delineation may be sharply defined or gradual.
• WDLS only metastasise after dedifferentiation.
• Adequate sampling is crucial.
• MLS doesn’t arise in retroperitoneum.
• Importance of full clinical history including previous
diagnosis, site and molecular results.Acknowledgements • Fiona Maclean (Douglass Hanly Moir) • Carl Bulliard (Healthscope) • Michael Bilous (Healthscope)
References 1. Hornick JL. Practical soft tissue pathology: a diagnostic approach. Philadelphia: Saunders; 2013. 2. Virchow R. Myxoma lipomadotes malignum. Virchow Arch Pathol Anat. 1865;32:545-6. 3. Enzinger FM, Winslow DJ. Liposarcoma. A study of 103 cases. Virchows Arch Pathol Anat Physiol Klin Med. 1962;335:367-88. 4. Fletcher CD, Bridge JA, Hogendoorn PCW, Mertens F. WHO classificaion of tumours of soft tissue and bone. Fourth Edition ed. Lyon: IARC Press.; 2013. 5. Fletcher CD. Soft tissue tumors. Edinburgh, UK: Churchill Livingstone; 2013. 6. Henricks WH, Chu YC, Goldblum JR, Weiss SW. Dedifferentiated liposarcoma: a clinicopathological analysis of 155 cases with a proposal for an expanded definition of dedifferentiation. Am J Surg Pathol. 1997;21(3):271-81. 7. Marino-Enriquez A, Fletcher CD, Dal Cin P, Hornick JL. Dedifferentiated liposarcoma with "homologous" lipoblastic (pleomorphic liposarcoma-like) differentiation: clinicopathologic and molecular analysis of a series suggesting revised diagnostic criteria. Am J Surg Pathol. 2010;34(8):1122-31. 8. Fletcher CD. The evolving classification of soft tissue tumours - an update based on the new 2013 WHO classification. Histopathology. 2014;64(1):2-11. 9. Evans HL. Liposarcoma: a study of 55 cases with a reassessment of its classification. Am J Surg Pathol. 1979;3(6):507-23. 10. Dei Tos AP. Liposarcoma: new entities and evolving concepts. Ann Diagn Pathol. 2000;4(4):252-66. 11. Tajima S, Koda K. Paratesticular dedifferentiated liposarcoma with prominent myxoid stroma: report of a case and review of the literature. Med Mol Morphol. 2015; Accepted 8 May 2015. 12. Sioletic S, Dal Cin P, Fletcher CD, Hornick JL. Well-differentiated and dedifferentiated liposarcomas with prominent myxoid stroma: analysis of 56 cases. Histopathology 2013, 62:287-293. 13. Liau J, Lee J, Wu C, Kuo K, Huang H, Liang C. Dedifferentiated liposarcoma with homologous lipoblastic differentiationL expanding the spectrum to include low-grade tumours. Histopathology. 2013, 652:702-707. 14. Kryvenko ON, Rosenberg AE, Jorda M, Epstein JI. Dedifferentiated liposarcoma of the spermatic cord. A series of 42 cases. Am J Surg Pathol. 2015 March 30.
You can also read

















































