Updates in Myelodysplastic Syndromes - Michael Keng, MD Assistant Professor of Medicine March 22, 2019 - UVA School of Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Updates in
Myelodysplastic Syndromes
Updates in Hematology and Hematologic Malignancies – 2019
University of Virginia
Charlottesville, VA
Michael Keng, MD
Assistant Professor of Medicine
March 22, 2019
Disclosures Agios – Advisory Board
Question 75F went to her PCP for fatigue x 8 months. CBC reveals Hg 11, MCV 103, Platelets 125K. Blood smear and nutritional studies normal. No inciting medications. BMBX reveals 30% cellularity, rare dysplastic megakaryocytes 6%, no blasts or fibrosis. Normal cytogenetics and NGS panel. What is the next step in treatment: A. Observation B. Repeat BMBX C. TPO agonist D. Lenalidomide E. Azacitidine
Question 75F went to her PCP for fatigue x 8 months. CBC reveals Hg 11, MCV 103, Platelets 125K. Blood smear and nutritional studies normal. No inciting medications. BMBX reveals 30% cellularity, rare dysplastic megakaryocytes 6%, no blasts or fibrosis. Normal cytogenetics and NGS panel reveals DNMT3A R882H mutation at 18% variant allele frequency (VAF). What is the next step in treatment: A. Observation B. Repeat BMBX C. TPO agonist D. Lenalidomide E. Azacitidine
MDS: Diagnosis
Cytopenia(s): MDS “decisive” criteria:
• >10% dysplastic cells in 1 or more lineages,
• Hb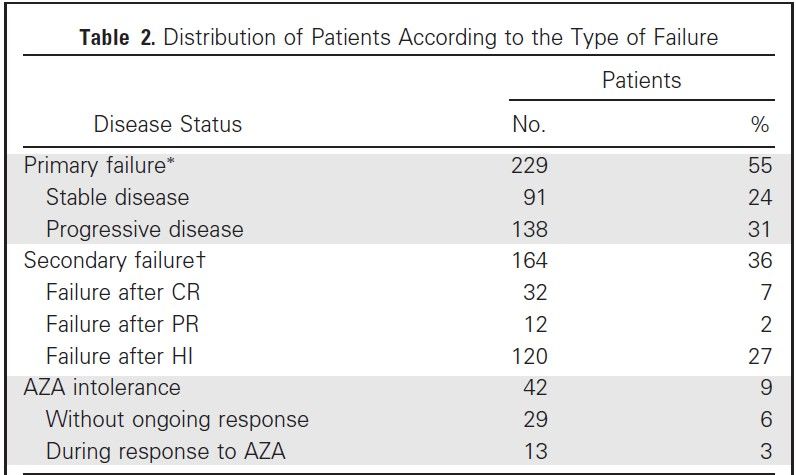
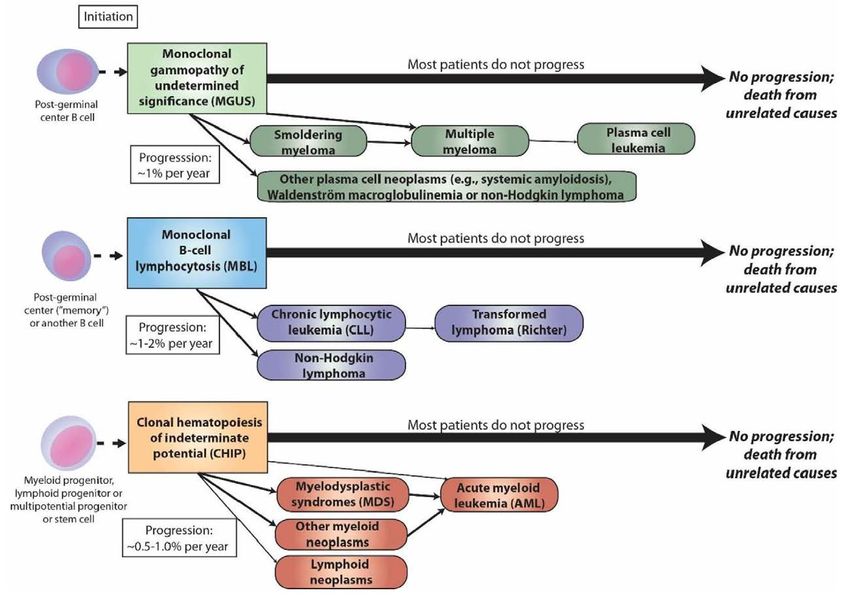
MDS: CHIP
Steensma et al Mayo Clin Proc 2015; 90(7):969-983.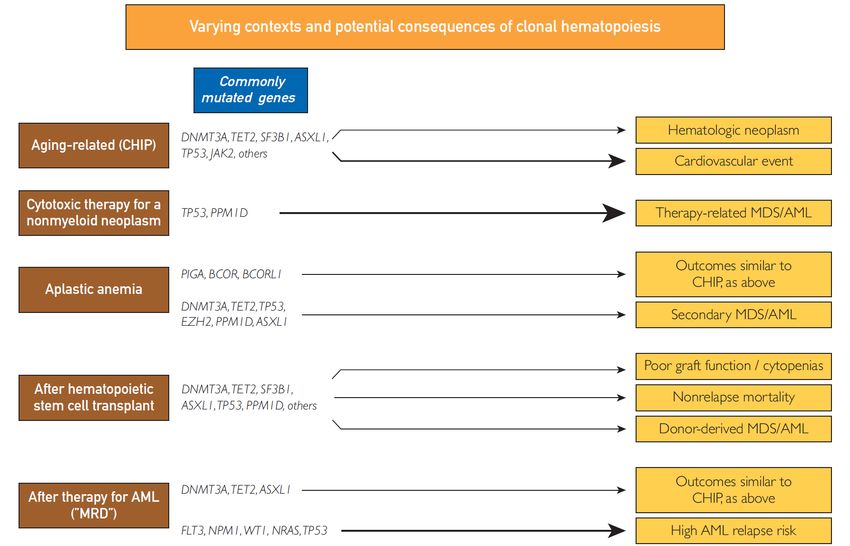
MDS: CHIP
Adapted: NCCN – MDS 2.2019.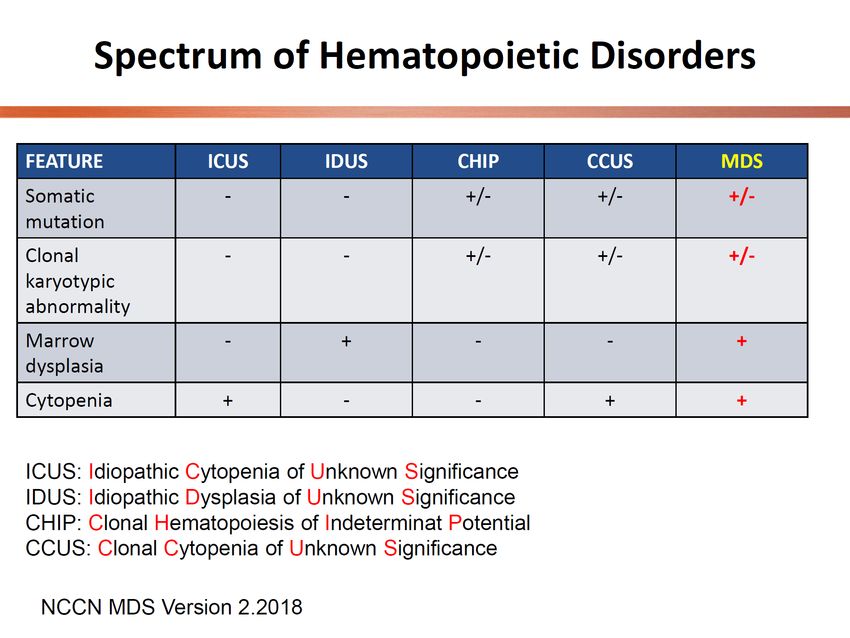
MDS: CHIP
Steensma et al Mayo Clin Proc 2015; 90(7):969-983.
MDS: CHIP
“Watchful” waiting
Do NOT have disease, but a
condition with a risk factor
Reducing the Clone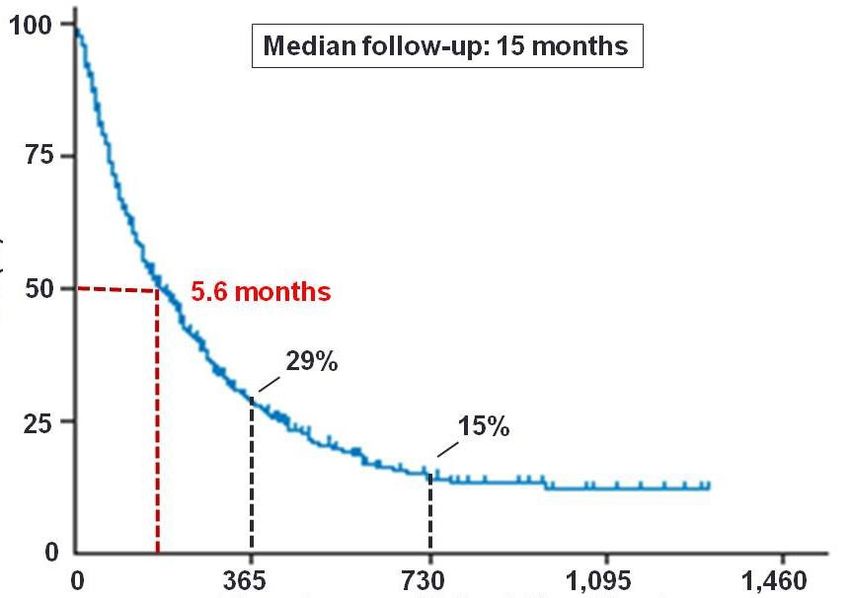
MDS: CHIP
Cardiovascular Risk
Myocardial Infarction
Stroke
Reducing the risk – follow American
Heart Association lifestyle guidelinesMDS: CHIP CHIP Clinic at UVA Heme/Onc Genetics Cardiology
MDS: Lower Risk
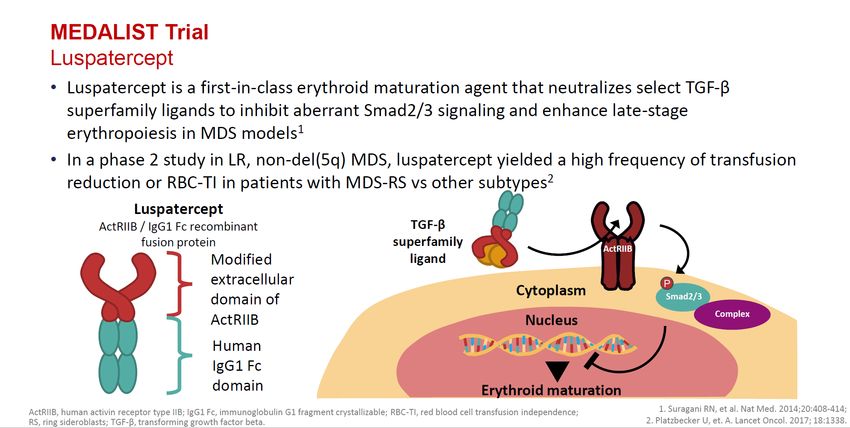
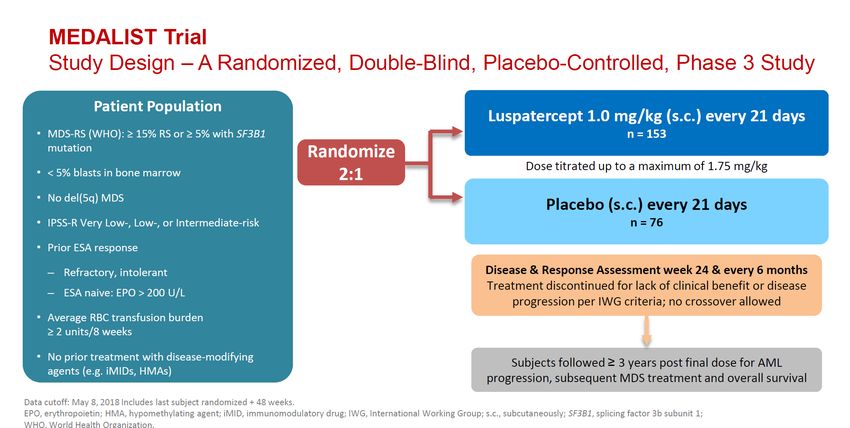
MEDALIST Trial – Phase 3, Randomized, Double-Blind,
Placebo-Controlled Study of Luspatercept to Treat
Patients with Very Low-, Low-, or Intermediate-Risk
MDS Associated Anemia with Ringed Sideroblasts Who
Require RBC Transfusions
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
MEDALIST Trial – Study Endpoints
Primary Endpoint:
RBC Transfusion Independence ≥ 8 weeks
Secondary Endpoint:
RBC Transfusion Independence ≥ 12 weeks
Additional Endpoints:
Duration of Response
Hb Change from Baseline
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
List A, et al. ASH 2018. Abstract 001.MDS: Lower Risk
MEDALIST Trial – Conclusions
In lower-risk, RS-positive MDS, luspatercept
resulted in RBC-TI, major RBC transfusion
reduction, and hemoglobin increase
Erythroid responses are durable
Well tolerated
Potential new therapy
List A, et al. ASH 2018. Abstract 001.Question 70M with MDS-EB2, trisomy 8, and 8% BM blasts. Treatment with azacitidine (75mg/m2 x 5 days) for 3 cycles. Patient complains of fatigue and CBC (WBC 1.5, ANC 0.5, Hg 8, Platelets 50K), all worse than prior to start of treatment. What is the next step: A. Stop therapy and perform BMB B. Continue azacitidine C. Continue azacitidine & increase treatment intervals D. Continue azacitidine & add GCSF E. Continue azacitidine & add TPO agonists F. Continue azacitidine & add GCSF and TPO agonists G. Switch to decitabine H. Switch to another agent
Question 70M with MDS-EB2 and treated with azacitidine for 16 cycles. BMBX after 7 cycles revealed CR. Patient now complains of fatigue and CBC (WBC 2.5, ANC 1.1, Hg 7, Platelets 90K). BMBX now reveals 17% blasts, TP53 and ASXL1 mutations, and complex cytogenetics (trisomy 8, del5q, del 7). He had and continues to decline SCT. What is the next step: A. Hospice B. Continue azacitidine C. Continue azacitidine, but add venetoclax D. Lenalidomide E. CPX-351 F. Switch to decitabine G. Clinical Trial
MDS: Higher Risk
Why Is Time Required?
Consider What is Happening…
ANC (Neutrophil Granulocytes)
3.2 100%
Early toxicities may be 2.7 80%
ANC, 109/L
difficult and/or 2.2 ANC ref. value 60%
discouraging for the 1.7 40%
patient
1.2 20%
0.7 0%
1 6 11 16 21
Treatment, weeks
ANC Mean ± 97.5 CI
Sekeres MA, List AF. Clin Leuk. 2008;2:28-33.MDS: Higher Risk
Timing of Evaluation
Definition of Resistance
Prediction of Response after HMA
FailureMDS: Higher Risk
Median OS 5.6 months
Percent Overall Survival
at HMA failure
for HR MDS
N=435
Time Since Azacitidine Failure (days)
Prebet et al. JCO 2011;29:3322MDS: Higher Risk Performance Status (PS
MDS: Higher Risk
IPSS-R Lower Risk
Rechallenge with ESAs
TPO Mimetics
Lenalidomide
Clinical Trial
Luspatercept
Guadecitabine
Spliceosome InhibitorsMDS: Higher Risk
IPSS-R Higher Risk
SCT
Low Dose Chemotherapy
CPX-351
Clinical Trial
Targeted Therapy (Enasidenib, Ivosidenib)
Non-Targeted Therapy (Rigosertib, Venetoclax)
Combination Therapy (HMA + )
Second Generation HMA
Immunotherapy (Ipilumumab, Nivolumab,
Pembrolizumab)MDS: Higher Risk
ETCTN Trial 10026 - Ipilimumab and Decitabine
- Relapsed MDS patients with 5% blasts or greater
After allogeneic stem cell transplant
OR
After 4 cycles of hypomethylating agentMDS: Higher Risk
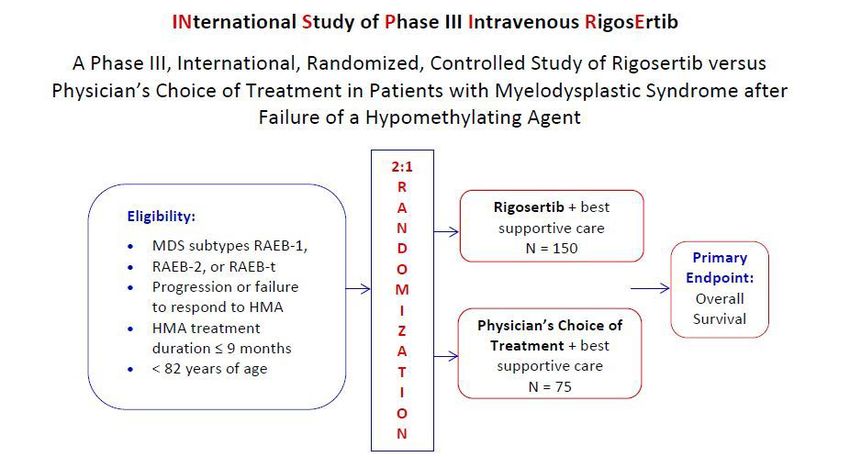
Phase III ONTIME: Rigosertib: PLK and PI3K inhibitor; a novel synthetic
benzyl styryl sulfone that is cytotoxic against a variety of human tumor cell
lines
Wk 16
Stratified by blast %
(5% to 19% vs 20% to 30%)
Patients with higher-risk
MDS (FAB, RAEB/t, Rigosertib (ON 01910.Na) + BSC Continue
CMML), 1800 mg/d x 3 days q2w treatment q4w until
relapsed/refractory after
(n = 180) progression
azacitidine or decitabine
(planned N = 270)
Best Supportive Care
LoDAC, hydrea, GFs
(n = 90)
• Primary endpoint: OS (HR: 0.62)
• Secondary endpoints: IWG response, transformation to AML, infection,
bleeding, QoL
Garcia-Manero et al. Lancet Oncology; 2016;17:496-508MDS: Higher Risk
Garcia-Manero et al. Lancet Oncology; 2016;17:496-508MDS: Higher Risk
INSPIRE - RigosertibMDS: Higher Risk BCL-2 Inhibitor - Venetoclax - Current studies in both treatment naïve and HMA failure settings New Hypomethylating Agents - Guadecitabine (SGI-110, oral) - CC486 (oral form of azacitidine) - Cedazurine (ASTX727, orally fixed-dose combination of decitabine and a cytidine deaminase inhibitor) Imetelstat (telomerase inhibitor) - studied in myeloproliferative neoplasms and transfusion independence rates were ~30%
MDS: Higher Risk
Other Targets
• IDH 1 and 2 – Ivosidenib and Enasidenib
• HIF – Roxadustat
• Need targets for TP53
• Decitabine – 10 day regimen
• APR-246, a TP53 modulatorMDS: Future Direction
We have to do BETTER.MDS and AML: Clinical
Trials at UVA
Upfront – Unfit for Intensive Chemotherapy
Azacitidine and Pracinostat (AML)
BST-236 (conjugate of cytarabine and asparagine)
Azacitidine and Pevonedistat (MDS, CMML, low blast AML)
Upfront – Intensive Chemotherapy
7+3 and Crenolanib (AML)
Relapsed/Refractory
MEC and Lenalidomide (AML)
HAM/Ida-FLAG and Crenolanib (AML)
Ipilimumab and Decitabine (AML/MDS)
Rigosertib (MDS)
Post-SCT
Gilteritinib as maintenance post-SCT
Myelofibrosis
Ictacitinib (Post ruxolitinib failure)Thanks!
University of Virginia Leukemia/MDS Program
Karen Ballen, MD Veronica Brill, MSN, RN, NEA-BC
Kelly Davidson, MD Lisa Huntsinger, MSN, RN, CCRN
John J. Densmore, MD, PhD Elizabeth Daniels, MSN, RN
Katie Ruefer, BSN, RN, PCCN
Michael G. Douvas, MD
Tanya Thomas, BSN, BA, RN, OCN
Laahn Foster, MD Devon Bloxsom, RN
Francine Garrett-Bakelman, MD, PhD Lauren Kramer, RN
Michael K. Keng, MD Holly Mellott, RN
Tamila L Kindwall-Keller, DO Mary Souder, RN
Amy Morris, PharmD
Hillary Maitland, MD
Amelia Hodson, RN
Louise Man, MD Kimberly Underwood, BA
Craig Portell, MD Megan Healy, BA
Indumathy Varadarajan, MD Cory Caldwell, RN
Leonid Volodin, MBBS
Michael E. Williams, MD
Thomas P. Loughran, Jr.,MD
Daniel Reed, MD
Kimberly Leake, FNP, MSN, RN
And Our Patients & Families!!!Contact Information
Appointments or Referrals:
434-924-9333
Office:
434-924-4257
mk2pv@virginia.eduYou can also read