Vanish your varices Exo-laser in varicose veins ablalation - course orientation basics of laser. safety and application of exolaser navigation ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Exo-laser in varicose veins ablalation Vanish your varices - course orientation basics of laser. safety and application of exolaser navigation through varices. cases. hands on.

Exo-laser how can I do it?
Radiofrequency (RF) and Laser (ELT) are
used to heat the vein and give a
permanent intemal and medial changes.
Princible.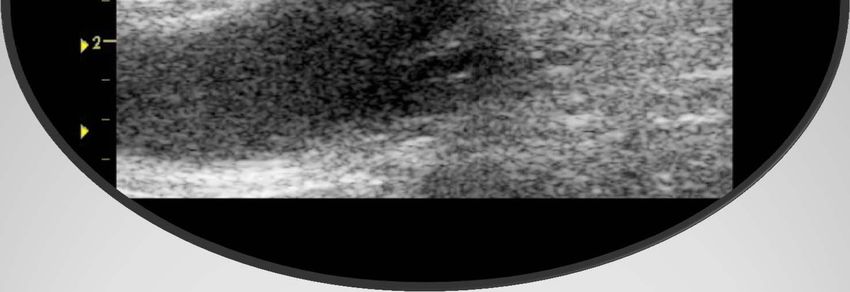
Vein color. Vein type. Vein size Vein navigation.
Color of the vein
Type of the vein

Size of the vein

The hand piece may only be used by
trained and qualified physicians
The general regulations and information
regarding exposure to laser radiation
therapy apply.
safety precautions are the cornerstone
through out the whole procedure.
Laser , sclerotherapy are complementary
processes.
It is a safe procedure: A)-Room requirements. B)-light. C)-skin preparation. D)-set “ . E)-after vanish care. F)-follow up. Precuations:

Before I do it:
1-Examine the patient and tailor your technique.
2-Mapping.
3-Use standard techniques and follow guide lines.
4-Prepare your tumescent anaesthia
(4 components).
5-Avoid:
Skin burn,hematoma and
echomosis,thrombosis
6-Remember complications.
7-prepare your set and fiber.
TIPS&TRICS 1. Remove the hand piece from its case and
inspect it visually to ensure that it is undamaged.
2. Switch on the laser
Warning:
Laser protective eyewear (wavelength-specific)
The parameters are specified in the relevant
laser device.
3. Connect the plug to the laser device.
4. Activate the pilot beam.
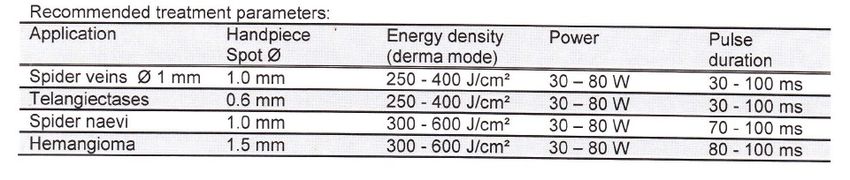
5. Configure the treatment parameters.
6. Set the laser device to "Ready" and depress
the footswitch to emit laser energy.
Prepare your set. The proper functioning of the hand piece must be
tested using the pilot beam.
The pilot beam must produce a red, clearly defined
focal spot.
A)_ pilot beam is irregular shape or a diffuse outline,
the complete derma hand piece must be inspected.
B)- pilot beam loses intensity, the optical fiber cable
must be replaced.
C)-Depending on the laser type, the pilot beam may
need to be reduced to prevent exposing the
vascular structures to excessive radiation.
D)-All of the vessels to be treated must be clearly
visible to the treating physician.
The pilot beam 1-Use the derma hand piece to apply the laser in
short pulses along the vascular tissue that
requires treatment.
2- Adjust the beam diameter in accordance with
the diameter of the vessel being treated.
3-Using light pressure, proceeding from the
distal end.
4-Treatment parameters depend on skin type and
pigmentation.
5-Larger vessels can be compressed by having
glass slides placed over them, and sealed with
pulses of laser light passed through the glass .
TIPS.TIPS.
Configurations.
Configurations.
Risks of laser treatment include :
Swelling
bleeding
infection
nerve damage.
burns to the localized tissue. Possible
complications:
Temporary erythema.
hyperpigmentation, hypopigmentation.
blistering .
scarring
complications: Heavily pigmented or bronzed skin. herpes Contraindications:
Examination &mapping
Skin Burn:
tumescent anaesthesia.
Depth of the vein.
Haematoma and Echymosis.
Nervous Complications:
Transitory par aesthesia is infrequent
(< 5%) and motor nerve problems
can occur .
avoid Step 1: puncture the veins. Step 2:pass the guide wire. Step 3:insert your catheter. Step 4:put your fiber or matrix. Step 5:locate your position. Step 6:injec tumescent anaseathia. Step 6: Endovenous ablation of varicose veins step by step
Puncture the vein
Pass the wire
Insert the catheter
Put the fiber
Locate the position
tumescent anaesthesia.
Fire…..
complications after endovenous treatment of the Saphenous Vein are infrequent and mostly mild • they depend on the technique that is used and on the technical accuracy of the operator • the indication of each technique should be adapted to the individual patient and his pathology Complications
1-Thrombosis.
2-Recurrence:
A) Recanlisation
B) Newvasclursation.
C) Improper technique(vein diamter,energy,
speed and extra axial anatomy).
3-Burn.
4-Nervous complications.
5-Hematoma.
6-Failure.
ComplicationsWho is the Best Candidate For laser Ablation ?
Patent Vein
Reflux
Uniform , non-tortuous Course
Average Diameter
Deep From Skin
Best Candidate5/30/2013
Endovenous laser ablation of varicose
veins:long term results.
by
Prof.Dr.M.Ayman
y Fakhry,Md.
y,
Chairman of vascular surgery dept.
Alexandria armed forces hospital
2013
Incidence of Varicose Veins
40 millions in U.S. have varicose veins
Four times more prevalent than arterial disease
Varicose veins affect 25% of women and 15% of men
Over 1 million people in U.S. seek treatment yearly
Over 150,000 surgical vein strippings yearly
15/30/2013
History of varicose veins surgery
Alexandria.
Elandalos.
EVLT.
Alexandria armed forces hospital.
FIRST PUBLICATION OF ENDOVENOUS LASER
• Title :Endovenous laser : a new minimally
i
invasive
i method
th d off ttreatment
t t ffor varicose
i
veins‐ preliminary observations using an 810
nm diode laser.
• Dermato Surg 2001; 27 : 117‐122
25/30/2013
Simultaneous laser ablation of varicose veins in lower limbs
By
Prof Dr.Shams Eldin Abbas Md,Dr, Fakhry M.Ayman,Md.
2006
127 patients presented to intervension radiology
clinic,Emory university
with grade (2‐6 ceap classification)
varicose veins
veins,
from 1/1/2004‐6/30/2005.
AVC conference
Bib.Alexandria ‐2006
aim
35/30/2013
• Study the efficacy, long term follow up of
patients
ti t undergoing
d i endovenous
d l
laser
ablation of varicose veins.
Patients and method
• 253 outpatients (317 limbs),
From Julyy 2006 to September
p 2009 ((39 months),
),
• were treated with 980 nm diode laser energy delivered
percutaneously using optical fiber under ultrasound
guidance.
• Tumescent anesthesia (50‐150 ml of 0.2% lidocaine)
Power and duration of the pulse were determined by vein
diameter.
D l controll was performed
Duplex f d at:
7 days, 1 month, 3 months, 6 months, 1 year and
yearly thereafter to assess treatment efficacy and adverse
effects.
45/30/2013
RESULTS
GENDER: 91 MALE PATIENTS
162 FEMALE PATIENTS
AGE: 17‐56 YEARS , X = 32.4+1.03 .
55/30/2013
Left l.l. 188
Right l.l. 58
Bilat.l.l 23
Gsv .203 Ssv .98 non axial v. 47
65/30/2013
VEIN DIAMETER :4‐12 MM
DEGREE OF REFLUX :2‐4
Duration of reflux:0.5‐0.7 sec.
Before after
75/30/2013
Before After
85/30/2013
95/30/2013
Results
• Primary great saphenous vein occlusion (97.1%)
• Failure (2.9%)
• Recurrence: one year. (7.5%)
• tributary and collateral veins. (6.3%)
• Great saphenous vein recanalization. (1 2% )
(1.2%
Reccurence
perforators Recanalised s.v.
One year 7.5% 6.3% 1.2%
2 years 14% 8% 6%
3 years 19% 10.5% 8.5%
The three most important factors associated with varicose
vein recurrence included new or recurrent perforating veins,
recanalised great saphenous vein and/or new anterior
accessory great saphenous vein reflux, .
105/30/2013
complications
• Ecchymosis (60.6%).
• moderate
d t pain i during
d i the th procedure
d (16.1%)
(16 1%)
• hematoma (5.5%)
• superficial phlebitis of tributaries (3.4%)
• Hyperpigmentation (2.9%)
• transient paresthesia (3 4%)
(3.4%)
• great saphenousvein thrombophlebitis.(0)
• deep vein thrombosis or pulmonary emboli.(0)
LITRATURES
Why Evlt?
115/30/2013
• Conclusions:
• Extended EVLA (mid‐calf to groin) increased
spontaneous resolution of varicosities.
• Nadarajah S. Theivacumar et al, JVS 2008
125/30/2013
Treatment of varicose veins with endovenous
laser: a prospective follow‐up study
Luiz Marcelo Aiello Viarengo, Guilherme Vieira Meirelles, João
Potério Filho
J Vasc
V B
Bras. 2006 5(3) 184 93
2006;5(3):184‐93
• Varicose vein treatment with endovenous
laser technique was successful in occluding
ggreat saphenous
p vein and its branches,, with
self‐limited adverse effects and recurrence
rate lower than 8% in the follow‐up period.
Laser associated with less pain and faster recovery for small
saphenous varicose veins
• One hundred and six patientwith unilateral, primary
saphenopopliteal incompetence were randomised equally
i
into parallel
ll l groups receiving
i i either
i h conventional
i l surgery or
endovenous laser ablation. Patients were assessed at
baseline and at one, six, 12 and 52 weeks.
• conclusion, Samuel noted that endovenous laser ablation
can be as effective as surgery but with the benefits of less
pain, faster recovery and fewer neural complications.
• The results of the study comparing endovenous laser
ablation
bl i to surgery ffor smallll saphenous
h varicose
i veins
i were
presented at the last Annual General Meeting of the
Vascular Society of Great Britain and Ireland (VSGBI) in
Edinburgh, UK.
135/30/2013
Satisfactory results with endovenous laser
ablation 6.5 years after treatment
• Michael Gough, Leeds General Infirmary, Leeds, UK,
presented long‐term follow‐up after endovenous
laser ablation for great saphenous varicose veins at
the 34th Charing Cross International Symposium in
London, UK. The study reviewed a group of 63
patients (79 limbs) 6.5 years after above‐knee laser
treatment.
• “Persistent below‐knee reflux we now treat it ,reduces
the risk of residual varicose veins after the initial
treatment. As far as the it is tempting to suggest that a
1470nm radial fibre may reduce the risk of this
happening but of course we have to await further
data.
REVATA study
• Future investigations with a properly designed
study should determine the frequency of
recurrences after thermal ablation, however,
based on the REVATA study, the percentage
should be reduced by 25–30% using thermal
ablative techniques compared to surgery,”
• REVATA study The investigation involved 164
varicose vein patients who were treated with
endovenous laser ablation.
145/30/2013
Endovenous therapies of lower extremity varicosities:
A meta‐analysis
Journal of Vascular Surgery
Volume 49, Issue 1, January 2009, Pages 230‐239
• Renate van den Bos MDa, Lidia Arends PhDb, c, Michael Kockaert MDa, Martino
Neumann MD, PhDa and Tamar Nijsten MD, PhDMethods
• A systematic review of Medline, Cochrane Library, and Cinahl was performed to
identify studies on the effectiveness of the four therapies up to February 2007. All
clinical studies (open, noncomparative, and randomized clinical trials) that used
ultrasound examination as an outcome measure were included
• 119 retrieved studies, 64 (53.8%) were eligible and assessed 12,320 limbs.
• Average follow
follow‐up
up was 32
32.2
2 month
month.
• ssuccess rates for stripping, foam sclerotherapy, radiofrequency ablation, and
laser therapy were about 78% ,77%, 84% and 94% respectively.
• Endovenous laser therapy was significantly more effective compared with other
modalities.
conclusion
155/30/2013
Endovenous laser ablation is at least as effective
as surgery in the treatment of saphenous vein
incompetence, but associated with less
periprocedural pain, faster recovery and fewer
neural complications, according to our new trial
and also laser therapy may provide a more
secure closure over the long term when
compared with surgery.
16You can also read