Vascular Dementia/ Vascular Cognitive Impairment - Alan Thomas Professor of Old Age Psychiatry - HEE NE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Vascular Dementia/
Vascular Cognitive Impairment
Alan Thomas
Professor of Old Age Psychiatry
Newcastle University
Key Paper
O’Brien and Thomas
Vascular Dementia
Lancet 2015: 386: 1698-1706
MCQ 1 The following are characteristic features of vascular dementia: 1. Gradual cognitive decline 2. Persistent complex visual hallucinations 3. Labile mood 4. Prominent executive dysfunction 5. Marked hippocampal atrophy on MR imaging
MCQ 2 In the management of vascular dementia: 1. Antipsychotic drugs have been banned 2. There is good evidence to use statins for secondary prevention 3. NICE recommends AChEI for mild to moderate (MMSE 10-20) vascular dementia 4. Sertraline is appropriate for treating emotional lability 5. There is little evidence for using memantine
Overview 1. Historical background 2. Diagnostic criteria 3. Difficulties with VaD 4. Epidemiology 5. Aetiology 6. Assessment 7. Management
Historical background (I)
• 600 – Term dementia (Latin “de mens”
without mind (Isadore) coined)
• 1642 - Dementia “post apoplexy (stroke)”
described (Willis)
• Up to 1960s dementia seen as consequence of
ageing, due to ‘vascular’ disease
• 1889- A Alzheimer Senile Dementia
(“hardening of arteries”)
Historical background (II) • 1907 Alzheimer described first case AD in 51 y.o. female (“presenile dementia”) • ‘Alzheimer’s disease’ (characteristic pathology) originally thought to be ‘presenile dementia’ • 1968, AD recognised as main cause dementia in late life (Blessed, Tomlinson and Roth)
Historical background (III)
• 1974 – Multi-infarct dementia (MID) coined
(Hachinski). ICD and DSM based on this
• 1980’s/90’s – MID just one of many causes of
Vascular dementia (e.g. subcortical disease)
• 1992/3 – Consensus diagnostic criteria for VaD
(Roman, et al, 1993)
• 2003 – Broader term Vascular Cognitive
Impairment preferred to dementia (the “memory”
issue), includes all subtypes, e.g. “vascular MCI”
and VaD
NINDS-AIREN Criteria
(Roman et al, 1993)
• Dementia (memory and 2 or more
domains)
• Cerebrovascular disease (focal
neurology and CVD on brain imaging)
• Link between the 2 (3 months or
abrupt/fluctuating clinical course)
• Possible VaD if brain imaging negative
or relationship (3/12) not clear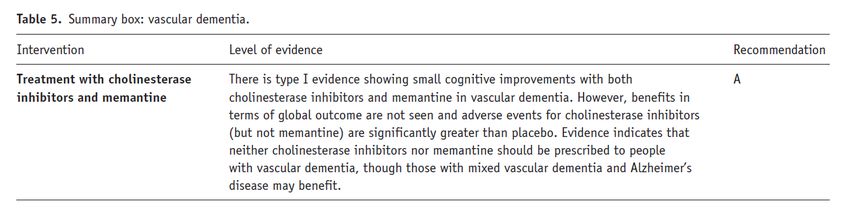
ICD-10 Criteria for VaD 1.Dementia (multiple cognitive deficits including amnesia, clear consciousness, impaired functioning, change) 2.Uneven distribution of cognitive deficits 3.Abrupt onset or stepwise deterioration 4.Presence of focal neurological signs and symptoms of cerebrovascular disease judged to be aetiologically related to dementia NB: No neuroimaging criteria
DSM-IV Criteria for VaD 1.Multiple Cognitive Deficits including amnesia 2.Significant impairment in social or occupational functioning which is a change 3.Presence of focal neurological signs and symptoms or laboratory evidence (=neuroimaging) of cerebrovascular disease judged to be aetiologically related to dementia (stepwise decline dropped) 4.Deficits not only during a delirium
DSM 5: Major Neurocognitive Disorder
A. Evidence of significant cognitive decline from a previous level of
performance in one or more cognitive domains (complex attention,
executive function, learning and memory, language, perceptual-motor, or
social cognition) based on:
1. Concern of the individual, a knowledgeable informant, or the clinician
that there has been a significant decline in cognitive function
and
2. A substantial impairment in cognitive performance, preferably
documented by standardised neuropsychological testing or, in its absence,
another quantified clinical assessment.
B. The cognitive deficits interfere with independence in everyday activities
(i.e. at a minimum, requiring assistance with complex instrumental
activities of daily living such as paying bills or managing medications).
C. The cognitive deficits do not occur exclusively in the context of a
delirium.
D. The cognitive deficits are better explained by another mental disorder
(e.g., Major Depressive Disorder, Schizophrenia).DSM 5: Mild Neurocognitive Disorder
A. Evidence of modest cognitive decline from a previous level of
performance in one or more cognitive domains (complex attention,
executive function, learning and memory, language, perceptual-motor, or
social cognition) based on:
1. Concern of the individual, a knowledgeable informant, or the clinician
that there has been a mild decline in cognitive function
and
2. A modest impairment in cognitive performance, preferably documented
by standardised neuropsychological testing or, in its absence, another
quantified clinical assessment.
B. The cognitive deficits do not interfere with capacity for independence in
everyday activities (i.e. complex instrumental activities of daily living
such as paying bills or managing medications are preserved, but greater
effort, compensatory strategies, or accomodation may be required).
C. The cognitive deficits do not occur exclusively in the context of a
delirium.
D. The cognitive deficits are better explained by another mental disorder
(e.g., Major Depressive Disorder, Schizophrenia).DSM 5: Major or Mild Vascular Neurocognitive Disorder
A. The criteria are met for major or mild neurocognitive disorder
B. The clinical features are consistent with a vascular etiology, as suggested
by either of the following:
Onset of the cognitive deficits is temporally related to one or more
cerebrovascular events.
Evidence for decline is prominent in complex attention (including
processing speed) and frontal-executive function.
C. There is evidence of the presence of cerebrovascular disease from history,
physical examination, and/or neuroimaging considered sufficient to
account for the neurocognitive deficits
D. The symptoms are not better explained by another brain disease or
systemic disorderDSM 5: Major or Mild Vascular Neurocognitive Disorder
Probable vascular neurocognitive disorder is diagnosed if one of the
following is present; otherwise possible vascular neurocognitive
disorder should be diagnosed:
Clinical criteria are supported by neuroimaging evidence of
significant parenchymal injury attributed to cerebrovascular
disease (neuroimaging-supported).
The neurocognitive syndrome is temporally related to one or more
documented cerebrovascular events.
Both clinical and genetic (e.g., cerebral autosomal dominant
arteriopathy with subcortical infarcts and leukoencephalopathy)
evidence of cerebrovascular disease is present.
Possible vascular neurocognitive disorder is diagnosed if the clinical
criteria are met but neuroimaging is not available and the temporal
relationship of the neurocognitive syndrome with one or more
cerebrovascular events is not establishedDifficulties with these diagnostic criteria 1. Problems with criteria 2. Inherent in VaD
Problems with criteria 1.Biased towards AD (not DSM-5) 2.Not validated and unreliable
Biased towards Alzheimer’s disease o Standard dementia criteria have usually made amnesia mandatory o Executive dysfunction is characteristic of CVD o Attentional deficits also more prominent in VaD o Cognitively and functionally impaired may not meet dementia criteria
Comparability and interrater reliability of
clinical criteria for VaD (Chui et al 2000)
‘Sample’: 25 case vignettes of varying types of
cognitive impairment
Diagnosis Interrater
DSM IV 26% 0.6
HIS 25% 0.6
ADDTC 10% 0.4
NINDS-AIREN 5% 0.4Sensitivity and Specificity of NINDS-
AIREN Criteria (Gold et al 2002)
Diagnostic criteria VaD AD Mixed Sens Spec
(neuropathology) (20) (46) (23)
NINDS/AIREN 4 1 4 .20 .93
probable
NINDS/AIREN 11 4 7 .55 .84
Possible
DSM-IV 10 5 6 .5 .84
ICD-10 4 0 4 .2 .94
Gold et al 2002Inherent difficulties with VaD 1.Variety of vascular diseases and anatomical locations for diseases 2. Mixed pathology (AD/DLB/VaD) is common and increasingly so with increasing age 3. But pure VaD is not common
Subtypes of Vascular Dementia
O’Brien and Thomas, 2015TWO MAJOR FORMS OF CVD
Large cortical and
Large-vessel disease
subcortical
Cardiac embolic events
infarcts
Small subcortical
Small-vessel disease infarcts
Diffuse white
matter lesionsDifferent types of
cerebrovascular disease (1)
SIVD -
Ischaemic infarct White matter lacunar
ischaemia stateDifferent types of cerebrovascular disease (2) Multi-infarct SIVD -WMLs Thalamic dementia (MID) CADASIL infarcts
Pure Vascular Dementia is not common
The Myth
Most dementia is AD and/or VaD
AD AD – 60%
+VaD Pure VaD – 20%
Other VaD+AD – 15%
Other - 5%
AD
VaDThe Reality: Brain Bank Studies show
Pure Vascular dementia is rare
Study Sample VaD (%) Pure VaD (%) Setting
size
Galasko et al. 170 9 2 AD Research Centres
(1994)
Drach et al. (1997) 59 27 12 Nursing home
Hulette et al. (1997) 1,929 0.6 0.3 CERAD study
Bowler et al. (1998) 122 6 3 Memory disorders clinic
Holmes et al. 80 29 9 Dementia register
(1999)
Lim et al. (1999) 134 34 3 AD patient registry
Duara et al. (2000) 307 16 4 Dementia brain bank
Barker et al. (2002) 384 18 3 Memory clinics, GPVascular Dementia is Overdiagnosed
Niemantsverdriet et al 2015
27 clinical VaD, only 5 had significant vascular pathology
5 probable VaD (NINDS AIREN) – None had vascular pathology!Big Infarct Case X: Example of Severe Vascular Case which doesn’t cause Dementia 2007 In 2007 (age 66) he suffered a large MCA stroke. Clinically he had hemiparesis and dysphasia, prominently expressive. But no generalised cognitive impairment, remained high functioning (handling money, medication and using computer) for years after this.
Case X
Major Stroke
2007
Urgent CT
BrainCase X
The next day
Large Left
Hemisphere
Evolving
infarctBig Infarct Case X 2015 Referred 8 years later (2015), “possible memory problems”. On examination including detailed neuropsychology he had no dementia, possible MCI (though still dysphasia). He remained independent and able to do high level functions such as handling his medication and doing computer related activities. In 2016 he developed Parkinson’s disease with a highly abnormal FPCIT (grade 3) and begun treatment with co-beneldopa. He remained cognitively fine or just possible MCI.
Several repeat
scans over
the years like
this: Large
Mature
Infarct
(this is 2019)2020 He was re-referred with concerns again about his memory. Repeat scans showed only the chronic large MCA infarct but no change, and no new infarcts. No hippocampal atrophy on coronal views. He had no Visual Hallucinations or REM sleep behaviour disorder. But he did have Cognitive fluctuations as well as Parkinson’s disease. He had progressive impairments in memory from his wife’s report (he no longer could accurately remind her of appointments, visits etc) and difficulties in higher level function (e.g. no longer able to do Sudoku) and worsening of his PD (tremor worse) and excessive salivation. Diagnosis therefore LBD. Not VaD or AD.
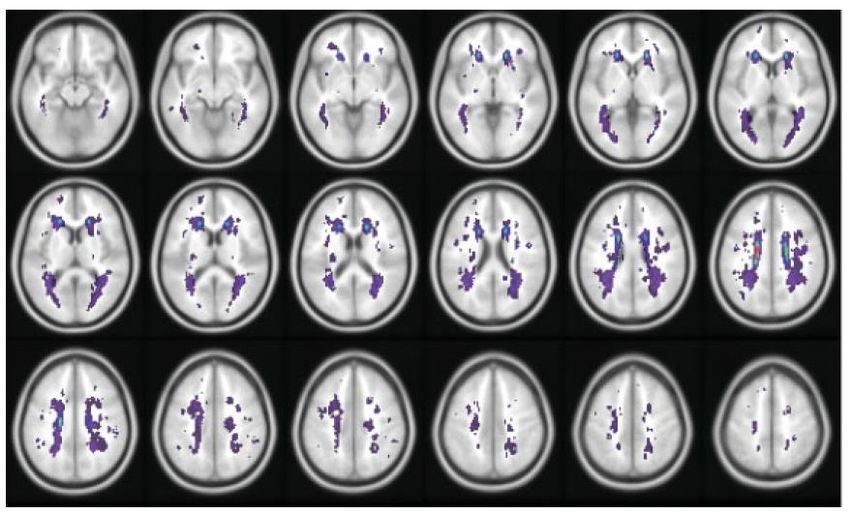
428 healthy adults
>50% had WMH on MRI
42% had DWMH only
33% PVH only
25% had both
Lesson: Presence of WMH should NOT
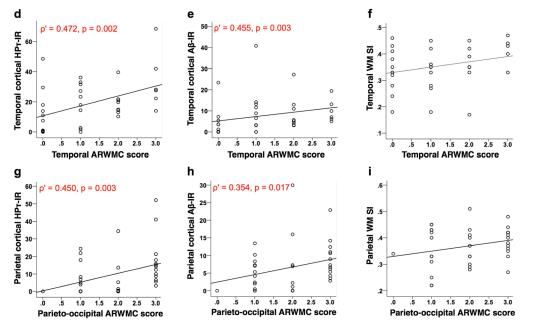
be used to diagnose VaDIt Gets Worse! o AD pathology (specifically tau neuritic load) but NOT vascular pathology correlated with WMH in parietal and temporal lobesin AD dementia (McAleese et al 2015) o WMH associated with markers of hypoxia and microvascular disease in controls but with neurodegeneration (AD pathology) in AD dementia (McAleese et al 2017)
Neuroimaging evidence
Pathological evidence of WML aetiology
Determine the influence of AD-related pathologies and SVD on the severity of WMH
• N = 36 brains (23 AD, 13 controls)
• Post-mortem T2 MRI
• Frontal, temporal, parieto-occipital
and total WMH score
Stepwise linear regression: Tau pathology was a
significant predictor of WMH score (P‘Mixed dementia’ is common o CVD, AD and LBD are all common and age related pathologies o In the ‘old-old’ (80s & 90s) two or more such pathologies are frequently found at autopsy o Clinically, an AD-type presentation with stroke before or after is regularly seen
Snowdon et al, JAMA, 1997, Nun Study
Open circle = no infarcts
Solid circle = 1 or more infarctsEpidemiology • Second most common cause dementia (AD 60%, VaD 20%, DLB 15%) • Rates rise with age (double 5.3y) as for AD (double 4.5y)(Jorm et al, 1987; 2003) • Prevalence higher in Asia (38%) (Fratiglioni et al, 1999) • Males > females, but females “catch up” at older ages (Jorm and Jolley, 1998) • Dementia 3/12 after stroke in 15-30%. A further 20-25% develop delayed dementia.
Aetiology of VaD o Stroke (but no clear link with location) o Hypertension (in mid-life) o Hypotension (in late-life) o Hyperlipidaemia (in some studies) o Diabetes (& ‘metabolic syndrome’) o Smoking (and probably other vrf’s) o Genetic causes (rare) o But age is strongest ‘risk factor’
Studies of VaD Genetics • Six polymorphisms strongly associated with VaD: APOE, ACT, ACE, MTHFR, PON1, and PSEN-1 genes • Only APOE (OR 1.82) and MTHFR (OR 1.32) significant after further analyses • APOE – AD gene, confounded by misdiagnosis? • MTHFR – vascular gene (homocysteine metabolism)
Inheritance of Cerebrovascular disease
Group Specific types Genetics
Stroke(s) CADASIL, CARASIL, Notch 3, other genes
RVCL (HERNS, CRV,HVE) TREX1 gene
Hypertensive Familial Binswanger’s/ unknown
angiopathies Leukoencephalopathies
Amyloid Icelandic, Dutch, Flemish, Cystatin C, APP, PrP,
angiopathies Prion, Finnish, Hungarian, Gelsolin, TTR, BRI
British, Danish, Others APOE
Other angiopathies Moyamoya disease Gene unknown/ Chr 3
Aneurysms Sacular (berry), large Genes unknown (also
aneurysms congenital forms)
Vascular Cavernous angiomas KRIT1 &other genes
malformations Cavernous malformations on Chr 7 and 3 lociAssessment of Vascular Dementia
Clinical features of Vascular dementia • Course: variable, classically abrupt onset of CI, stepwise deterioration but commonly gradual • Symptoms and signs- focal signs, motor/sensory deficits, bulbar, gait; depression, anxiety • Neuropsychometric findings- Executive dysfunction (vs memory and language function); attentional deficits • Depression relatively common; emotional lability common • History of vascular disease: CHD, AF, TIAs, PAD etc • Imaging- CT/MRI- focal infarcts (70-90%); WMLs (70-100%) • SPECT or PET- decreased CBF; patchy • EEG- compared to AD usually normal • Laboratory- changed cardiovascular disease markers
1. Establish presence of dementia 2. Careful history and physical assessment for evidence of CVD (stroke; falls; paresis etc) 3. Physical investigations: high BP or cholesterol; infarct(s) on neuroimaging 4. Determine (as far as possible) relationship between CVD and dementia (by pattern of onset) 5. Prominent executive dysfunction, attentional deficits, slowed information processing suggest VaD more likely 6. Mood changes, emotional lability and disinhibited behaviour are also more characteristic of VaD
Cache County Study Lyketsos et al, 2000 (n=5092)
Prevalence of neuropsychiatric
Features after stroke
(Angelelli et al, 2004)
Healthy Post-stroke patients
Controls 2 months 6 months 12 months
Symptom (n=61) (n=45) (n=45) (n=34)
Delusion 0.0 0.0 0.1 0.1
Hallucination 0.0 0.0 0.0 0.0 NB: Mood
Agitation 0.2 1.5** 1.3 1.2
Depression 0.3 2.9*** 3.4*** 2.7***
lability
Anxiety 0.3 1.6*** 1.1* 1.4*
Euphoria 0.0 0.6**‡ 0.0 0.1
Apathy 0.2 1.0 3.2***†† 2.5***†
Disinhibition 0.0 0.6 0.3 0.3
Irritability 0.3 2.0** 1.8** 2.3***
Aberrant motor 0.0 0.8***§ 0.3 0.3
behaviour
Night-time 0.1 0.7 1.0* 0.9*
disturbances
Appetite/eating 0.2 2.5*** 1.5* 2.1**NICE/SCIE Guidelines for Dementia:
assessment and diagnosis
• Structural imaging should be used to exclude other
cerebral pathologies and to help establish the subtype
diagnosis. MRI is preferred modality to assist with early
diagnosis and detect subcortical vascular changes,
though CT can be used
• HMPAO SPECT should be used to help differentiate
between AD, VaD and FTD if the diagnosis is in doubt
• CSF measurement should not be used as routine
investigationsManagement of Vascular Dementia
Management strategies for VaD • Use drugs developed for Alzheimer’s disease • Antiplatelet agents • BP lowering • Statins • Diet and Exercise • Other target symptoms
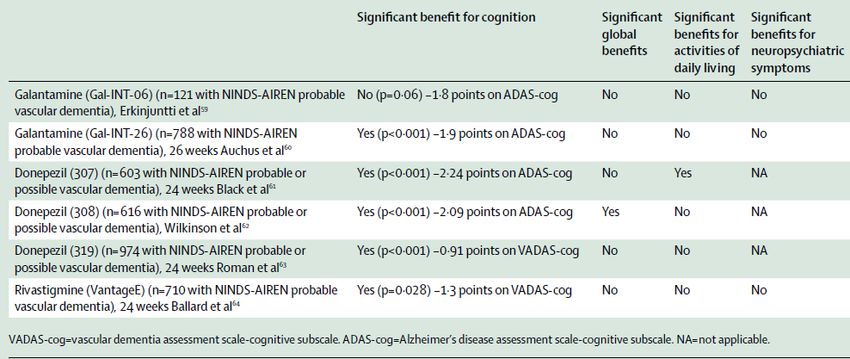
RCTs of CHEI in Vascular dementia
O’Brien and Thomas, 2015Absence of cholinergic deficits in
“pure” VaD (Perry et al 2005)
Sharp et al (2009): Also found ChAT activity only
decreased in VaD with co-existing AD, and may
actually be increased in pure VaDMemantine in VaD:
Two published 6 month studies
• Orgogozo et al, Stroke, 2002. 321 probable
VaD. ADAS-Cog improved 0.6 pts in treated
group, declined 1.6 pts in placebo
• No effect on global outcome (CIBIC+)
• Wilcock et al, ICP, 2002. 579 probable VaD.
Drug treated patients 1.75 pts higher on
ADAS-Cog than placebo at 6 months
• No effect on global outcome (CGI-C)Cochrane review of
memantine (McShane et al 2014)
Published data from two 6 month RCTs
suggest a small beneficial effect of
memantine on cognition and behaviour at
six months in those with mild to moderate
vascular dementia, this effect was not
clinically detectableDementia: assessment, management and support
for people living with dementia and their carers
NICE Guideline NG97, June 2018
Pharmacological management of non-Alzheimer's dementia
1.5.10 Offer donepezil or rivastigmine to people with mild to moderate dementia with
Lewy bodies.[1]
1.5.11 Only consider galantamine[2] for people with mild to moderate dementia with
Lewy bodies if donepezil and rivastigmine[1] are not tolerated.
1.5.12 Consider donepezil or rivastigmine for people with severe dementia with Lewy
bodies[1].
1.5.13 Consider memantine[3] for people with dementia with Lewy bodies if AChE
inhibitors[4] are not tolerated or are contraindicated.
1.5.14 Only consider AChE inhibitors[4] or memantine[3] for people with vascular
dementia if they have suspected comorbid Alzheimer's disease, Parkinson's disease
dementia or dementia with Lewy bodies.
1.5.15 Do not offer AChE inhibitors or memantine to people with frontotemporal
dementiaBAP Dementia Guidelines 2017
Conclusions
• 3020 subjects (mean age 63y) with lacunar infarct
randomised to BP lowering (Hypertension in VaD o Only one study has shown treatment of HTn to reduce dementia incidence (Fourette et al 1998) o >4 RCTs have shown no such benefits on dementia incidence or cognitive decline (Cochrane Review 2014) o May relate to stage at which treatment is given (over-zealous treatment may cause hypotensive damage)
SPRINT Mind (JAMA 2019) • RCT of intensive BP lowering vs standard treatment in 9361 patients >50 years of age with hypertension and no stroke, CV disease • Main outcomes in JAMA and NEJM showed intensive arm had lower fatal and nonfatal CV events and reduced deaths • So study terminated early for cognitive/dementia endpoints (again)
SPRINT Mind (JAMA 2019) No significant effect on dementia Just significant on MCI and composite dementia and MCI
Nimodipine in subcortical VaD
(Pantoni et al, Stroke 2005)
• 242 subjects, subcortical VaD on ICD-10
and CT evidence; Nimodipine 90mg or PBO
• Primary outcome measure NS (Sandoz
Clinical Assessment Geriatric scale)
• Some improvements on secondary
measures (GDS, lexical memory)
• CV adverse events more frequent in
placebo group (RR 2.26 (CI 1.11-4.6))Statins in VaD o 3 RCTs in possible & probable AD (simvastatin and atorvastatin). No difference in cognition, ADL, global, behaviour o No trial in VaD o Cochrane Review (2014): No evidence to support use in dementia o But three large RCTs have found no effect of statins on cognitive decline (Santanello et al 1997; Heart Protection Study 2002; Shepherd et al 2002)
Exercise: The PROMoTE trial
• Single-blind 12 month RCT in 70 subjects (mean age 74)
with subcortical VCI
• Thrice-weekly, progressive aerobic exercise training
program for 6 months c/w usual care plus education
• On primary outcome, exercise group had improved ADAS-
Cog (-1.7 point difference) at 6 months, but no difference at
12 months
• On secondary outcomes, exercise groups had longer timed
walking distance (30 metres) and reduced BP (7mm Hg) at
6 months. Reported to be cost effective at Can $20,000/
QALY
Ambrose et al, Neurology 2016; Davis et al, BMJ Open 2017Exercise: The DAPA study
• 494 people with
dementia
randomised to
exercise or usual
care in 2:1 ratio
• Exercise group 1.4
points worse on
ADAS-Cog
(p=0.03)
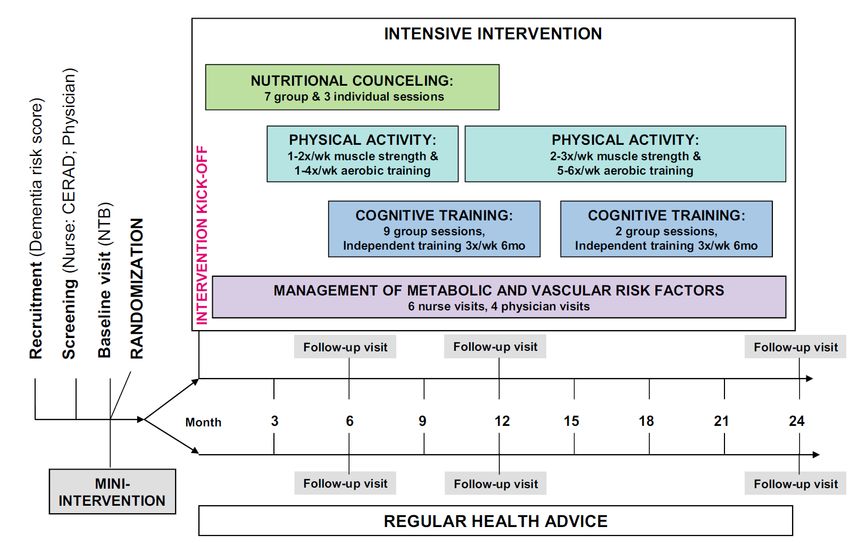
Lamb et al, BMJ 2017FINGER study
Ngandu et al, Lancet 2015
• FINnish Geriatric intervention study to prEvent cognitive
impaiRment and disability (FINGER)
• 1260 people aged 60-77, no dementia but high “risk score” (> 6)FINGER study Ngandu et al, Lancet 2015
Pre-DIVA sudy
Cluster RCT of usual care v 4 monthly
Visits to optimise vascular risk reduction
Sig differences
between
groups in BP
and
Cholesterol
but very small
(1.5mmHg)
Also
Van Charante et 7y
al, outcome
Lancet 2016Mood Disturbance in VaD
• There is evidence demonstrating no benefit from
antidepressants for depression in dementia in
general, including VaD (SADD Study 2011,
DIADS-2, 2010)
• But these trials did not include moderate-severe
MDD
• Emotional lability: small case-control studies
report benefits from low dose TCA and from
SSRIs (typically within two weeks)Psychosis/Aggression in VaD
• RCTs report only modest benefits from APD in
dementia; best evidence is for risperidone
• All APD are associated with cognitive decline &
poorer quality of life, as well as EPSE etc
• APD are associated with a small increased risk of
stroke and death in dementia
• Regulatory authorities caution against their use,
especially in the presence of stroke disease
• APD should only be used in severe cases after
other interventions have failedNICE/SCIE Dementia Guidelines
• For people with vascular dementia, cholinesterase
inhibitors and memantine should not be used for the
treatment of cognitive decline, except as part of properly
constructed clinical studies
• People with vascular dementia who develop non-cognitive
symptoms or behaviour that challenges should not be
prescribed cholinesterase inhibitors, except as part of
properly constructed clinical studies
• Mixed dementia should be managed according to the
condition that is thought to be the predominant cause of
the dementiaMCQ 1 The following are characteristic features of vascular dementia: 1. Gradual cognitive decline 2. Persistent complex visual hallucinations 3. Labile mood 4. Prominent executive dysfunction 5. Marked hippocampal atrophy on MR imaging
MCQ 2 In the management of vascular dementia: 1. Antipsychotic drugs have been banned 2. There is good evidence to use statins for secondary prevention 3. NICE recommends AChEI for mild to moderate (MMSE 10-20) vascular dementia 4. Sertraline is appropriate for treating emotional lability 5. There is little evidence for using memantine
CASC Part 1 You are asked to see a 75 year old man with a severe ‘mixed dementia’ who has become paranoid and aggressive. He lives in an EMI Residential Care Home. You have no access to previous records. ((You will be interviewing his main carer at the home ‘in his best interests’. He is too impaired to be interviewed and he lacks capacity to consent and his wife is unavailable))
CASC Part 2 You conclude he needs antipsychotic medication and you wish to prescribe risperidone. His wife has arrived and you are to discuss this with her.
You can also read