Recurrent Penile Swelling in a Healthy Adolescent - NYU Langone Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Department of Urology
Case of the Month
Recurrent Penile Swelling
in a Healthy Adolescent
EVALUATION AT NYU LANGONE HEALTH
This 15 y.o. presented for evaluation of recurrent penile swelling. Three years ago, he had
significant penile swelling attributed to insect bites. Keflex was administered with resolution of
the swelling. One year ago, he re-developed penile swelling, which was treated with Keflex and
steroids with eventual resolution. Allergy testing was positive for common allergens, including
pollen and cats. Endocrinology evaluation revealed no etiology for the swelling, which reoccurred
about 1 month before his visit to NYU Langone. He was given Amoxicillin, Keflex, a Medrol pack,
and Atarax without resolution of the swelling. There was no discomfort or erythema associated
with the swelling. No history of other abnormal areas of swelling, i.e., mouth or lips.
PMH and family history: Constipation, age 9 years; normal colonoscopy; no current GI
symptoms; short stature treated with growth hormone therapy Dad: irritable bowel syndrome;
Hashimoto’s disease Mom: Sjogren’s syndrome; Hashimoto’s disease
Pertinent findings on physical examination: Circumcised phallus; entire penile shaft edematous,
non-pitting with chronic skin thickening/induration; dorsal skin foreshortening with saxophone-
like shape to shaft and glans; glans normal; normal meatus; bilaterally descended testes normal
on palpation; in supine, + left varicocele difficult to palpate due to upper half of scrotum involved
with skin thickening/induration; no erythema (Figure 1)
Sonographic evaluation: A scrotal sonogram showed normal-appearing testes, bilaterally. The
right testis has a volume of 12.6 cc and the left, 10.4 cc. A large left varicocele was present; no
varicocele on the right in standing. Thick (1.2 cm) edematous scrotal wall (upper 1/3) extending
to the penile shaft without hyperemia. No abscess or focal lesion.
The working diagnosis was lymphedema of the penile shaft. The left varicocele with the
significant size discrepancy was discussed with the recommendation for delayed left
varicocelectomy. The patient was advised to consult a pediatric dermatologist for examination
and punch biopsy for a definitive diagnosis. Physical examination by the pediatric dermatologist
confirmed the findings of penile edema and revealed no other areas of swelling or skin
abnormalities. A presumptive diagnosis of cutaneous Crohn’s disease (CD) involving the penis
was confirmed on penile shaft punch biopsy, which showed granulomatous inflammation.
DC 2/9/2021
CASE OF THE MONTH
Figure 1. “Saxophone” Penis
Pediatric Dermatology, Vol 33, Issue: 1, 14-15 ; 2016.
MANAGEMENT
The patient was started on prednisone 60 mg QD with very minimal improvement. While
tapering the prednisone, Tacrolimus 0.1% ointment BID (an immunosuppressant that is a topical
calcineurin inhibitor that blocks T cells’ activation) was started pending approval for adalimumab
(Humira®), a biologic medication. The prior pediatric GI was consulted. Since the inflammatory
markers were WNL, and there were no GI symptoms, a colonoscopy was not performed. The
Crohn’s IBDX prognostic panel and a fecal calprotectin level were WNL. (Calprotectin is a protein
found in neutrophils that has strong antibacterial and antifungal properties. Calprotectin is
activated when inflammation occurs and can be used as a diagnostic indicator. The concentration
of calprotectin relates directly to the severity of the inflammation. Calprotectin assesses disease
activity but also flares in both symptomatic and asymptomatic patients. Regular follow-up with
pediatric GI is planned.
DISCUSSION
This case represents the second patient I have managed in 30 years with cutaneous CD. The
lessons learned from our very knowledgeable pediatric dermatologist, Dr. Vikash Oza, were
instructive, and in the future, CD will be included in my differential of penile swelling. The first
patient with this condition presented at 10 years of age with oral/facial swelling as well as chronic
penile lymphedema for 2 years. He had been seen by a variety of specialists without a diagnosis.
The patient was referred to Dr. Oza, who noted uniform swelling of the lips; upper gingival
overgrowth; mild erythema of the cheeks and upper arms; uniform swelling of the penile shaft;
and indurated, erythematous plaques in the perianal region. Dr. Oza made the presumptive
diagnosis of cutaneous CD in a “split-second.” He has not developed CD 3 years later.
I think about how many swollen penises I have seen over the years and attributed the swelling
to an allergic reaction due to; possibly an insect bite or contact dermatitis. Being unfamiliar
with cutaneous CD years ago, I would not have recognized this cutaneous marker in a child or
adolescent, which would aid in their timely diagnosis and management of CD since approximately
30% of individuals with CD present in childhood.
DC 2/9/2021
CASE OF THE MONTH
HISTORICAL NOTES AND INTRODUCTION
In 1932, Dr. Burrill B. Crohn and his colleagues reported on a subacute or chronic necrotizing
inflammation of the terminal ileum, termed regional ileitis. Later, it was found that this disorder
could involve any area of the GI tract. It was soon recognized that up to 44% of patients with CD
have a cutaneous manifestation at some point in their disease course, making the skin the most
common site of extra-intestinal involvement. In 1965, the first description of non-caseating or
non-necrotizing granulomas at sites noncontiguous to the GI tract was reported by Parks et al.,
and 5 years later, Mountain coined the term MCD—metastatic Crohn’s disease. In children, the
skin findings more frequently precede the GI symptoms by months to years. Skin lesions often
complicate CD.
The GI tract and skin lesions have been divided into 3 broad categories based on pathologic
mechanism. (Table 1)
1. CD-specific manifestations: oral CD, fissures and fistulas, and MCD; mechanism identical to
that of the GI tract; majority of lesions with the exception of MCD, which is rare but critical
to recognize since it often precedes the diagnosis of GI CD.
2. Reactive: erythema nodosum and oral aphthae are most common; mechanism distinct from
GI tract; development may be related to cross-antigenicity between the skin and GI tract.
3. Associated: vitiligo, palmar erythema, clubbing, hidradenitis suppurativa; no well-defined
Table 1 Cutaneous Manifestations of Metastatic Crohn's Disease
mechanism
Table 1. Cutaneous Manifestations of Metastatic Crohn’s Disease (Pediatric Dermatology, Volume: 35, Issue: 5, 566-574)
DC 2/9/2021
Pediatric Dermatology, Volume: 35, Issue: 5, 566-574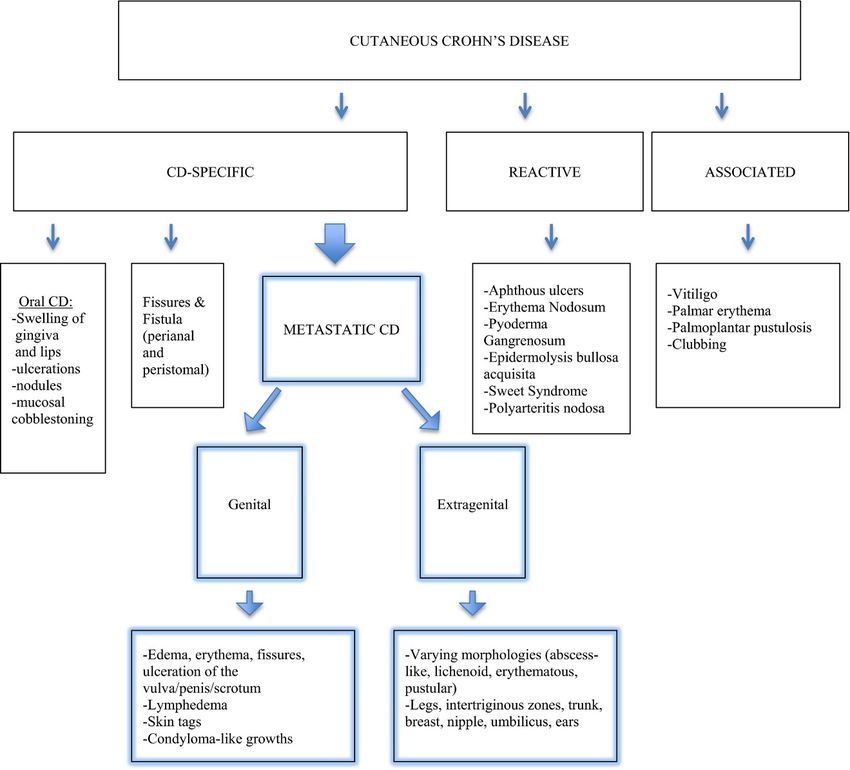
CASE OF THE MONTH
Pathogenesis of MCD
In a susceptible host, CD is thought to develop genetic predisposition, environmental factors,
epithelial barrier dysfunction, and abnormal immune responses to pathogenic and commensal
bacteria. Although there are several theories on the pathogenesis of MCD, the exact etiology
remains unknown. MCD lesions are thought to be related to a granulomatous response to
unidentified antigens from the GI tract. The antigens are deposited into the skin leading to a
perivascular inflammatory response. Another theory invokes a granulomatous vasculitis as
seen in type IV hypersensitivity via sensitized T lymphocytes reacting to circulating antigens,
causing granulomatous injury to the vessel wall and inflammation.
Epidemiology
As many as 30% of patients present with CD at < 20 years, and ~2% are diagnosed at < 10 years.
Cutaneous CD occurs in almost half of patients who ultimately develop CD. Cutaneous CD affects
males and females of all ages equally (mean age of presentation ~9 years for both sexes). At least
7-24% of children have MCD, but this lower occurrence rate is thought to be an underestimation
of reporting or diagnosis.
Clinical Presentation
MCD can occur before, concurrently, or after GI symptoms manifest. About 86% of pediatric
MCD occur in patients with no known intestinal CD, but in those patients, intestinal disease was
diagnosed within 6 years of the MCD diagnosis. Another study reported children with MCD
diagnosed with intestinal CD 9 months to 14 years of age with a mean age of onset of pediatric CD
being 10-14 years. There has been no correlation between MCD and GI disease, but cutaneous
findings tend to be associated more frequently with colonic vs. ileal involvement.
Genital swelling is the most common presentation of MCD. This can involve edema; erythema;
fissures; and ulceration of the vulva, penis, and scrotum, as well as lymphedema; skin tags; and
condyloma-like growths. About 2/3 of children had genital involvement at presentation, while only
1/2 of adults have affected genital sites; 82% of the children had had GI symptoms at presentation.
Extra-genital MCD may involve the extremities, trunk, breast, and intertriginous zones.
Diagnosis Management
MCD is a rare cutaneous manifestation of CD and is often difficult to recognize since it appears
similar to other dermatoses, both granulomatous and non-granulomatous, as listed in Table 2.
Diagnosis starts with a detailed history and physical examination. Once the possibility of MCD or
other cutaneous manifestations of CD have been entertained, a referral to dermatology for a
thorough skin examination and biopsy is warranted for definitive diagnosis.
Table 2. Differential Diagnosis of Metastatic Crohn’s Disease (BioMed Research International 2017 p 3)
Granulomatous Disorders Nongranulomatous Disorders
Cutaneous sarcoidosis Hidradenitis suppurative
Tuberculosis Pyoderma gangrenosum
Syphilis Impetigo
Mycobacterial infections Erythema nodosum
Actinomycosis Factitial dermatitis from factitial injection of foreign substances
Deep fungal infections Schistosomiasis
Lymphogranuloma venereum Chronic lymphedema resulting from obstruction Erysipelas
Granuloma inguinale Chronic cellulitis
Foreign body reaction
DC 2/9/2021CASE OF THE MONTH
The histology of the MCD is similar to the dominant histology of the CD bowel lesions, as
previously mentioned. (Figure 2) On biopsy of genital lesions, the finding of sterile, non-caseating
granulomas with foreign body or Langerhans giant cells, epithelioid histocytes, lymphocytic
infiltrate, and plasma cells, similar to CD or granulomatous lymphangitis, are seen on histological
examination. The inflammatory infiltrate can surround dermal blood vessels and is termed
“granulomatous perivasculitis.”
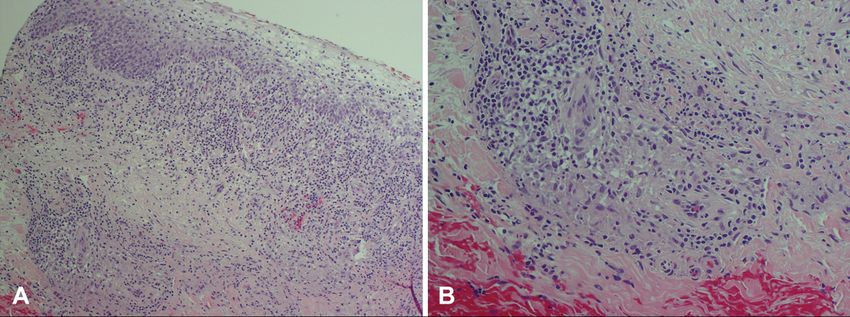
Figure 2. Pathology of Metastatic Crohn’s Disease-9
Metastatic Crohn’s disease. A, Microscopic examination demonstrates noncaseating granuloma formation with brisk lymphocytic
infiltration involving the papillary and mid dermis. B, Higher magnification highlights a well-formed granuloma consisting of epithelioid
histiocytes and lymphocytes. Some histiocytes are angiocentric. (A and B, Hematoxylin-eosin stain; original magnifications: A, ×20; B, ×40.)
J Am Acad Dermatol, Vol 71, Issue 4, 2014, 807,
The finding of granulomas makes it difficult to differentiate from sarcoidosis. Epidermal ulceration,
eosinophilic infiltrate, and marked dermal edema are useful in determining the diagnosis. Since the
infectious granulomatous disorders listed in Table 3 can show similar pathologic features, additional
studies are performed, including periodic acid-Schiff tissue cultures and acid-fast bacilli testing.
Management
Despite MCD causing significant morbidity, treatment has not been standardized in the past. In
2014, The American Academy of Dermatology published MCD treatment guidelines. (Table 3)
Current management approach should initially follow an algorithm but remain individualized
according to disease severity and clinical response. Topical treatments, both steroidal and
nonsteroidal, have been used. Systemic forms of glucocorticosteroids have been the mainstay of
therapy. Sulfasalazine, both topical and oral, has been promising in the healing of MCD lesions.
Metronidazole has been efficacious in cases when steroid therapy was unsuccessful. In addition,
antibiotics and immunosuppressive drugs have been used, including methotrexate, azathioprine,
and cyclosporine. Biologic therapy using adalimumab from living cells and belongs to a class of
medications known as tumor necrosis factor (TNF-alpha) inhibitors has been observed to reduce
the inflammation associated with CD.
DC 2/9/2021CASE OF THE MONTH
Table 3. Therapeutic Approach to Metastatic Crohn’s Disease
Table 3
Surgery
When MCD remains refractory to these various medical interventions, surgical excision and
debridement may be indicated. Excision of GI segments have not been effective for the prevention of
or the treatment of MCD since the skin and GI lesions often have different clinical courses and severity.
CONCLUSION
Cutaneous CD occurs in about 50% of individuals with CD, and MCD is a rare subset of the
cutaneous manifestations of CD. Since the genitalia are the more common site of MCD, urologists,
both pediatric and adult, need to be aware of this entity due to its non-specific clinical presentation,
which is similar to other inflammatory skin disorders that are more common to our specialty. It is
important to recognize this rare dermatosis since it can serve as a marker of significant risk for the
development of Crohn’s disease that needs to be monitored by gastroenterologists.
DC 2/9/2021CASE OF THE MONTH
REFERENCES
1. Kumaran, M, Gupta, Somesh, Ajith, C, Kalra, Navin, Sethi, Sunil, Kumar, Bhushan, et al. (2006). Saxophone penis revisited.
Int J STD AIDS. 2006 Jan;17(1):65-66.
2. Drew J.B. Kurtzman, Trevor Jones, Fangru Lian, Lisan S. Peng. Metastatic Crohn’s disease: A review and approach to therapy.
J Am Acad Dermatol. 2014 Oct;71(4):804-13.
3. Aberumand B, Howard J, Howard J. Metastatic Crohn’s Disease: An Approach to an Uncommon but Important Cutaneous Disorder.
Biomed Res Int. 2017;2017:8192150.
4. Schneider SL, Foster K, Patel D, Shwayder T. Cutaneous manifestations of metastatic Crohn’s disease.
Pediatr Dermatol. 2018 Sep;35(5):566-574.
ELLEN SHAPIRO, MD
Ellen Shapiro, MD, is professor of urology at the NYU Grossman
School of Medicine. She has been director of Pediatric Urology at NYU
School of Medicine, now NYU Grossman School of Medicine, since
1993. Dr. Shapiro brings more than 30 years of expertise in all areas of
pediatric urology, including treatment and management of congenital
anomalies of the kidneys and urinary tract (e.g., ureteropelvic junction
obstruction, vesicoureteral reflux, and ureterocele/ectopic ureter),
hypospadias, undescended testes, hernias, varicocele and kidney
stones as well as complex reconstruction for neurogenic bladder and
bladder exstrophy. Dr. Shapiro completed her urology residency at the
Johns Hopkins Hospital and a fellowship in pediatric urology at the
Children’s Hospital of Michigan. Dr. Shapiro has served on the
executive committee of the American Academy of Pediatrics Section
on Urology and has been chair of the section’s Pediatric Urology
Workforce Study. She has served as a member of the Examination
Committee of the American Board of Urology and the Vesicoureteral
Reflux Guidelines Committee of the American Urological Association.
In addition, Dr. Shapiro has been on the NYU Grossman School of
Medicine Faculty Promotion and Tenure Committee and is currently a
member of the executive committee of the Admissions Committee.
DC 2/9/2021Department of Urology
Our renowned urologic specialists have pioneered numerous advances in the surgical and pharmacological
treatment of urologic disease.
For questions and/or patient referrals, please contact us by phone or by e-mail.
Faculty Specialty Phone Number/Email
Kidney stones, Kidney Cancer, Ureteral Stricture, UPJ obstruction, Endourology, Robotic Renal Surgery, 646-825-6387
James Borin, MD
Partial Nephrectomy, Ablation of Renal Tumors, PCNL james.borin@nyulangone.org
Female Pelvic Medicine and Reconstructive Surgery, Pelvic Organ Prolapse-Vaginal and Robotic 646-754-2404
Benjamin Brucker, MD
Surgery, Voiding Dysfunction, Male and Female Incontinence, Benign Prostate Surgery, Neurourology benjamin.brucker@nyulangone.org
Female Sexual Dysfunction, Male Sexual Dysfunction, General Urology, Benign Disease Prostate, 646-825-6318
Seth Cohen, MD
Post-Prostatectomy Incontinence, Erectile Dysfunction, Hypogonadism seth.cohen@nyulangone.org
Robotic and Minimally Invasive Urology, BPH and Prostatic Diseases, Male and Female Voiding 718-630-8600
Frederick Gulmi, MD*
Dysfunction, Kidney Stone Disease, Lasers in Urologic Surgery, and Male Sexual Dysfunction frederick.gulmi@nyulangone.org
Urologic Oncology, Open, Laparoscopic, or Robot-Assisted Approaches to Surgery, Surgical
646-825-6325
Mohit Gupta, MD† Management of Genitourinary Malignancies including Kidney, Bladder, Prostate, Adrenal, Penile,
Mohit.Gupta2@nyulangone.org
and Testis Cancers
Urologic Oncology (Open and Robotic) – for Kidney Cancer (Partial and Complex Radical), Urothelial 646-744-1503
William Huang, MD
Cancers (Bladder and Upper Tract), Prostate and Testicular Cancer william.huang@nyulangone.org
Pediatric Urology including Hydronephrosis, Hypospadias, Varicoceles, Undescended Testicles,
212-263-6420
Grace Hyun, MD Hernias, Vesicoureteral Reflux, Urinary Obstruction, Kidney Stones, Minimally Invasive Procedures,
grace.hyun@nyulangone.org
Congenital Anomalies
646-825-6322
Christopher Kelly, MD Male and Female Voiding Dysfunction, Neurourology, Incontinence, Pelvic Pain, Benign Prostate Disease
chris.kelly@nyulangone.org
Prostate Cancer: Elevated PSA, 3D MRI/Ultrasound Co-registration Prostate Biopsy, Focal (Ablation) 646-825-6327
Herbert Lepor, MD
of Prostate Cancer, Open Radical Retropubic Prostatectomy herbert.lepor@nyulangone.org
718-261-9100
Stacy Loeb, MD, MSc** Urologic Oncology, Prostate Cancer, Benign Prostatic Disease, Men’s Health, General Urology
stacy.loeb@nyulangone.org
Benign Prostatic Hyperplasia, Erectile Dysfunction, Urinary Tract Infection, Elevated Prostate-specific 718-376-1004
Danil Makarov, MD, MHS***
Antigen, Testicular Cancer, Bladder Cancer, Prostate Cancer danil.makarov@nyulangone.org
Urethral Strictures, Robotic and Open Reconstructive Surgery for Ureteral Obstruction/Stricture, Fistulas, 646-754-2419
Nnenaya Mmonu, MD, MS
Bladder Neck Obstruction, Penile Prosthesis, Post Prostatectomy and Radiation Urinary Incontinence nnenaya.mmonu@nyulangone.org
Male Infertility, Vasectomy Reversal, Varicocele, Post-Prostatectomy, Erectile Dysfunction, 646-825-6348
Bobby Najari, MD
Male Sexual Health, Hypogonadism, Oncofertility bobby.najari@nyulangone.org
Female Pelvic Medicine and Reconstructive Surgery, Voiding Dysfunction, Neurourology, Incontinence, 646-825-6311
Nirit Rosenblum, MD
Female Sexual Dysfunction, Pelvic Organ Prolapse and Robotic Surgery nirit.rosenblum@nyulangone.org
Pediatric Urology including: Urinary Tract Obstruction (ureteropelvic junction obstruction),
646-825-6326
Ellen Shapiro, MD Vesicoureteral Reflux, Hypospadias, Undescended Testis, Hernia, Varicocele, and Complex
ellen.shapiro@nyulangone.org
Genitourinary Reconstruction.
Kidney stones, PCNL, Kidney Cancer, UPJ obstruction, Endourology, Robotic Renal Surgery, 718-630-8600
Mark Silva, MD*
Ablation of Renal Tumors mark.silva@nyulangone.org
Muscle-Invasive Bladder Cancer, Non-Invasive Bladder Cancer, Radical Cystectomy, 646-825-6327
Gary D. Steinberg, MD
Urinary Tract Reconstruction After Bladder Removal Surgery gary.steinberg@nyulangone.org
Female Pelvic Medicine and Reconstructive Surgery, Pelvic Organ Prolapse, Incontinence in Women, 646-825-6324
Lauren Stewart, MD
Female Voiding Dysfunction lauren.stewart@nyulangone.org
Urologic Oncology – Prostate Cancer (MRI-Guided Biopsy, Robotic Prostatectomy, Focal Therapy, 646-825-6321
Samir Taneja, MD
Surveillance), Kidney Cancer (Robotic Partial Nephrectomy, Complex Open Surgery), Urothelial Cancers samir.taneja@nyulangone.org
Urologic Oncology – Prostate Cancer, MRI-Guided Biopsy, Kidney and Prostate Cancer Surgery,
646-754-2470
James Wysock, MD, MS Robotic Urological Cancer Surgery, Prostate Cancer Image-guided Focal Therapy (Ablation, HIFU),
james.wysock@nyulangone.org
and Testicular Cancer
Robotic and Open Reconstructive Surgery for Ureteral Obstruction, Fistulas, Urinary Diversions, 646-754-2419
Lee Zhao, MD
Urethral Strictures, Peyronie’s Disease, Penile Prosthesis, and Transgender Surgery lee.zhao@nyulangone.org
Kidney Stone Disease, Upper Tract Urothelial Carcinoma, Ureteral Stricture Disease, and BPH/Benign 646-754-2434
Philip Zhao, MD
Prostate Disease philip.zhao@nyulangone.org
*at NYU Langone Hospital – Brooklyn ** NYU Langone Ambulatory Care Rego Park NYU Langone Levit Medical †222 East 41st street; NYU Langone Ambulatory Care Bay Ridge, and NYU Langone Levit Medical
***
nyulangone.org 222 East 41st Street New DC
York,2/9/2021
NY 10017
U1020You can also read