WELCOME Managing Dyspnea in Patients with - COVID-19 - Pallium Canada
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
WELCOME Managing Dyspnea in Patients with COVID-19 Host: José Pereira, MBChB, CCFP(PC), MSc, FCFP Presenters: Doris Barwich, MD, CCFP(PC) Shalini Nayar, MD, FRCPC The webinar will begin soon (please note your microphone is muted). Please use the Q&A function to submit questions.
Housekeeping
• Your microphones are muted.
• Use the Q&A function at the bottom of your screen to submit questions.
Please do not use the chat function for questions.
• This session is being recorded and will be emailed to webinar registrants
tomorrow.
2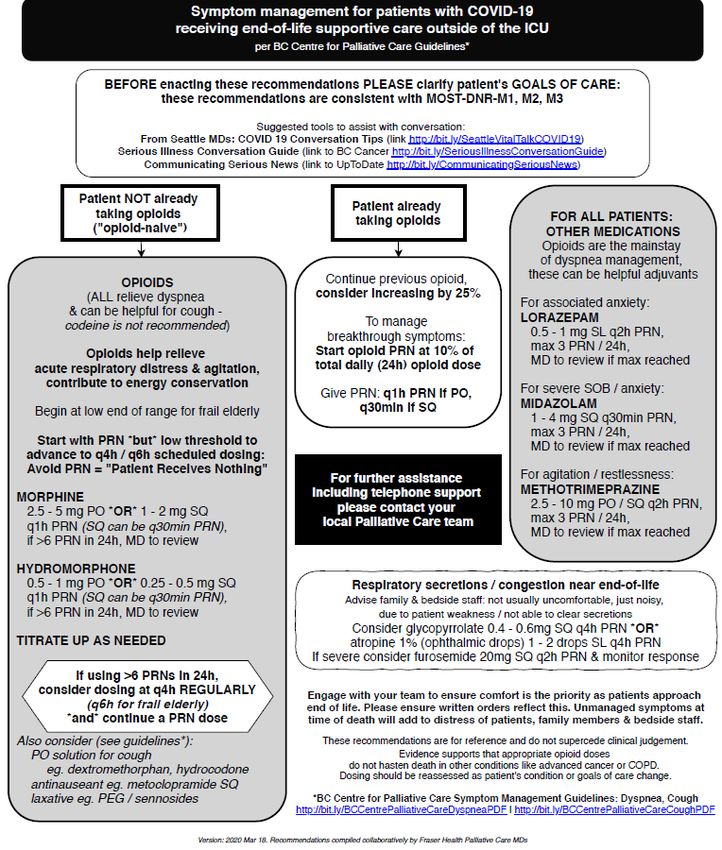
Presenters
Host Panelists
Dr. José Pereira MBChB, CFPC(PC), MSc, Dr. Doris Barwich MD, CCFP(PC)
FCFP Medical Director Fraser Health Palliative
Professor and Director, Division of Palliative Care Network & BC Centre for Palliative
Care, Department of Family Medicine, Care
McMaster University, Hamilton, Canada
Scientific Officer, Pallium Canada Dr. Shalini Nayar MD, FRCPC
Palliative Care & Respirology Fraser Health
3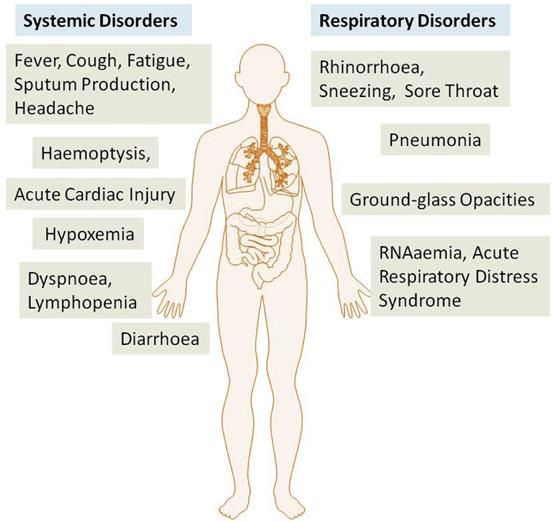
Declaration of conflicts
Pallium Canada
• Non-profit
• Funded mainly by Health Canada over the years in the form of a contribution program
• Recently received funding from CMA, which it is using to address COVID response
(e.g. making LEAP modules available online and webinars)
• Generates funds to support operations and R&D from course registration fees and
sales of the Pallium Palliative Pocketbook
Presenters
• Dr. Jose Pereira – Paid by Pallium Canada as Scientific Officer
• Dr. Doris Barwich
• Dr. Shalini Nayar
4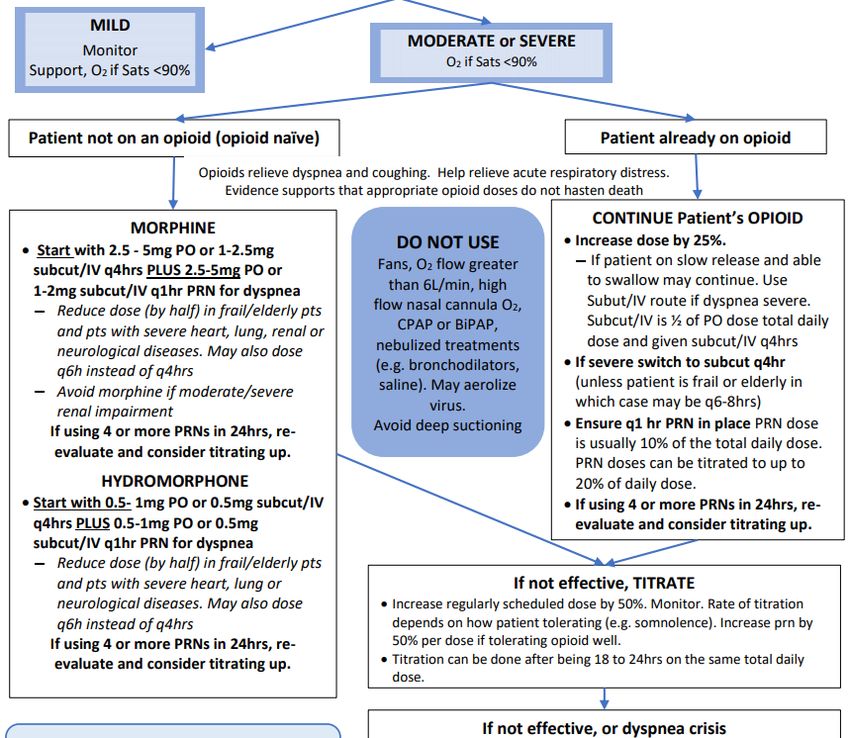
Learning objectives
Upon completing this webinar, you should be able to:
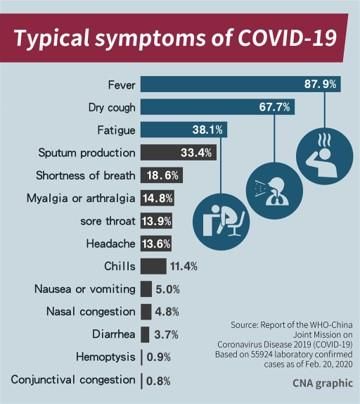
• Describe the prevalence of dyspnea (breathlessness) in patients with COVID-19
disease, and its frequency relative to other symptoms;
• Describe some pathophysiological processes of the virus that relate to
breathlessness, including ARDS;
• Describe the role of some treatments like fluid therapy and steroids relative to COVID-
19 disease;
• Apply a protocol to manage dyspnea in these patients, highlighting the central role of
opioids; and,
• Compare usual palliative care approaches versus COVID-specific palliative care
approaches.
5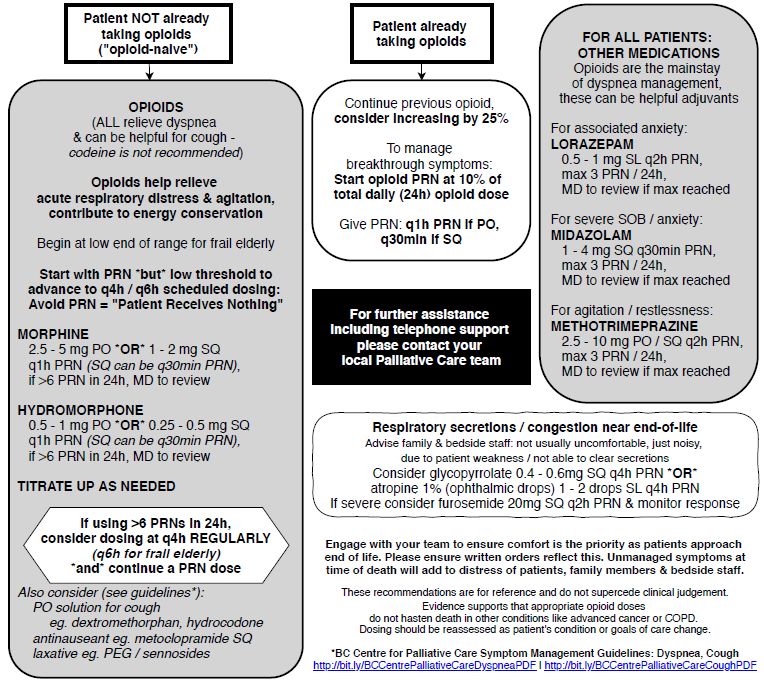
Outline
• Part 1: Background information
• Part 2: Unique aspects of caring for patients with COVID-19 disease
• Part 3: Management of dyspnea (breathlessness)
6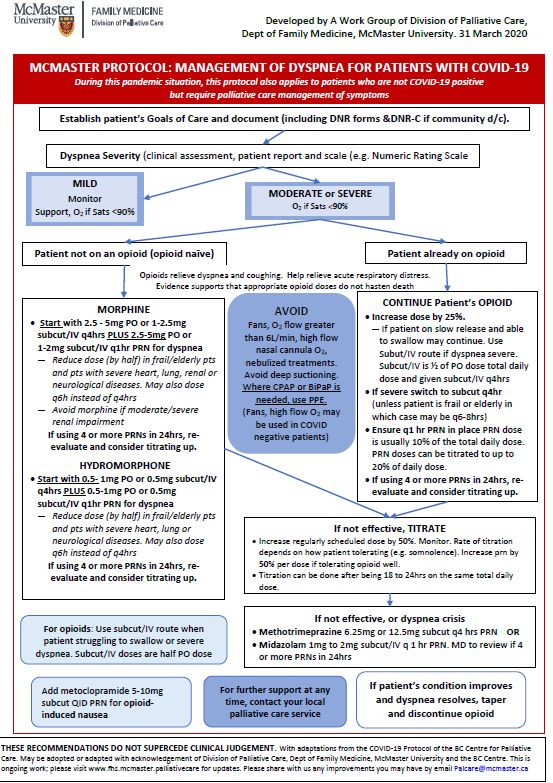
Part 1: Background information
COVID-19
• Incubation period 1 – 14 days
• Highly contagious – symptoms do NOT need to be present
• Transmission
o Between people who are in close contact with one another (within about 6 feet).
o Respiratory droplets produced when infected person coughs, sneezes or talks.
o Droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into
the lungs.
o Aerosol-generating procedures are a caution
• COVID-19 may have unique ability to target lower airways
• From Wuhan data, infection appears most commonly after 5.2 days
• Onset of symptoms to death ranged from 6-41 days (median 14 days)
o Older the patient, shorter the time
8
Presentation, symptoms, and course of COVID-19
• Common presentations:
o Fever, dry cough, fatigue, shortness of
breath
o Viral pneumonia
• If progresses
o Initially mild can progress over a week
(+dyspnea)
o Cases of rapid progression have been
noted, going within hours from
mild/moderate symptoms to severe
respiratory problems
o Severe Complications: ARDS,
arrhythmias, acute cardiac injury, shock
• Recovery: ~2 wks if mild, 3-6 wks if
severe
9
Pathophysiology COVID-19
Four broad categories
• Subclinical
o Asymptomatic; infectious
• Upper respiratory tract
o Dry cough, headache, sinus symptoms
• Systemic flu-like symptoms
o Fever, myalgia, cough
• Lower respiratory tract/diffuse
o Viral pneumonia
o Wuhan data: ~6% severe illness
o ARDS
1011
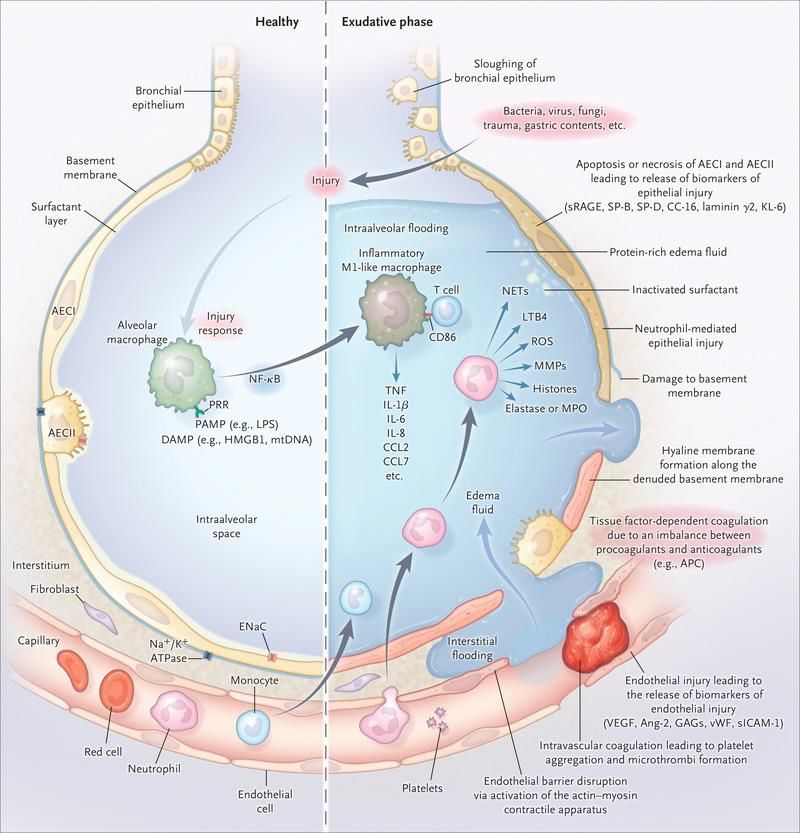
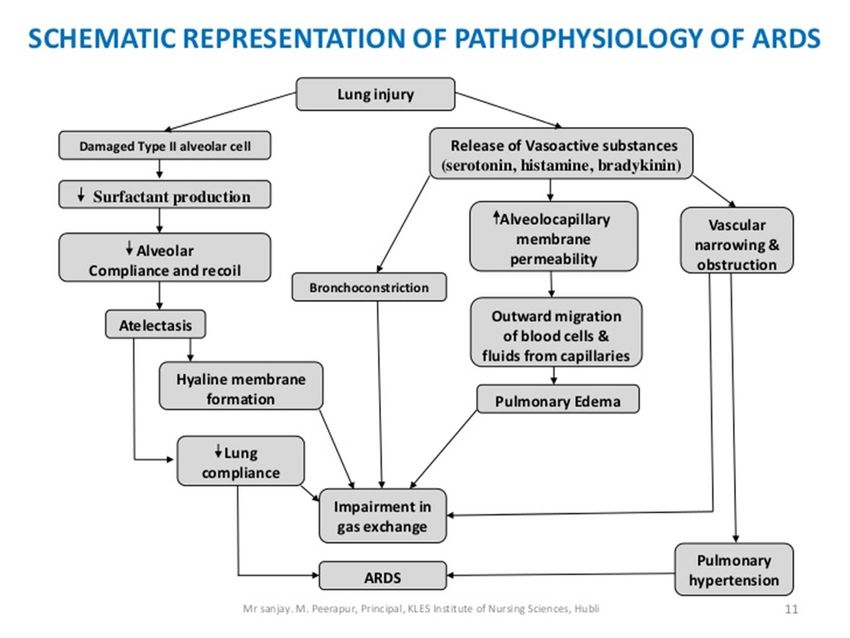
ARDS
12Part 2: Unique aspects of caring for patients with COVID-19 disease
Fluid management
• Aggressive fluid resuscitation should generally be avoided
o COVID-19 patients are seemingly sensitive to fluid overload
o Use of vasopressors is appropriate
o Patients that are volume deplete should get small volume bolus of IVF
o Excessive fluids to clear the lactate in patients who appear euvolemic should be
avoided
14Use of steroids: Specific disease states
• Corticosteroid use
o Mixed results, but overall not convincing, RCT or fully peer reviewed evidence for tx
COVID alone
• COPD
o Regular treatments, including steroids if needed for reactive airways
• Asthma
o Treat with regular asthma tx, including steroids for reactive airways
• Septic shock/concomitant infection
o Follow antimicrobial guidelines
o May opt to use steroids for the indication of septic shock
15Aerosol generating procedures: Treating Hypoxemia
h ttps://emergencymedicinecases.com/faq - items /covid -update -april - 5th-2020/ 16Fraser Health policy RE: CPAP and BiPAP
1. Any patient suspected or confirmed COVID-19 should not receive NIV
or CPAP without careful consideration.
o Early endotracheal intubation may be advised with respiratory failure.
o Full PPE for staff.
2. For other in-patients who are on BiPAP or CPAP at home: Consult
Respirology.
o Patients on nocturnal CPAP for obstructive sleep apnea should be trialed off CPAP.
▪ Clinical judgement in the case of patients at high risk of desaturation (e.g. post operative cases) may
lead to a decision to order the CPAP be continued.
o Patients on nocturnal BiPAP for obesity hypoventilation syndrome are at increased
risk of death compared to patients with OSA therefore continue with BiPAP.
o Caregivers should wear goggles and N95 masks when caring for patients on CPAP &
BiPAP.
17Part 3: Management of dyspnea (breathlessness)
BC Centre for Palliative
Care & Fraser Health
Guidelines 2020
19Dyspnea management guidelines
• Appropriate Goals of Care conversations essential to clarify treatment
goals and realistic options for care.
o E.g. Adaptation of the Serious Illness Conversation Guide: www.fraserhealth.ca/-
/media/Project/FraserHealth/FraserHealth/Health-Professionals/Clinical-
resources/Advance-Care-Planning---Serious-Illness/Serious-Illness_Mini-
Reference_COVID19-Guide.pdf
o HPCO resources: www.speakupontario.ca
o Vital Talk resources: www.vitaltalk.org/guides/covid-19-communication-skills
o Speak Up resources: www.advancecareplanning.ca/covid19
20BC Centre for Palliative
Care & Fraser Health
Guidelines 2020
21BC Centre for Palliative
Care & Fraser Health
Guidelines 2020
22Dyspnea management guidelines: Fraser Health process
1. General guidelines: Fraser Health; McMaster etc.
2. Pre-printed orders (PPOs):
o Crisis order set to complement Actively Dying PPO in Acute Care and Long-Term
Care
o Palliative Sedation Guideline
o Med kits and discharge checklist for COVID positive patients going home
3. Developing a “COVID code” and Emergency med kit for COVID units
4. Facilitating improved access to Palliative Care Physician expertise
23Dyspnea
Palliative care for COVID-19 +ve
“Usual” Palliative Care
patients
Fans are sometimes recommended Fans are not to be used as they
Fans: aerosolize the virus
In some cases, high flow oxygen may High flow O2 aerosolizes virus; use
High flow oxygen: be required, titrated to clinical effect. PPE
E.g. ≥ 60% O2, or as per
CAEP > 6 lpm
BiPAP or CPAP is used in select cases; Use PPE when NIV used
Non-invasive ventilation: e.g. end-stage ALS or COPD; OSA
24Dyspnea
“Usual” Palliative Care Palliative care for COVID-19 +ve patient
Secretions are usually from the upper In severe COVID disease, ARDS and
Airway secretion airway. pulmonary edema is more common. Need
management In severe cases, scopolamine or furosemide and ARDS approaches for that
glycopyrrolate PRN
Opioids are useful in the management of Opioids are very useful in the management
severe dyspnea. of severe dyspnea.
They are safe and effective They are safe and effective
Opioids
(see LEAP online module on Dyspnea for In COVID, they may need to be initiated
guidelines on doses). sooner for their physiological and symptom-
relief benefits
Morphine remains a useful first-line opioid.
Hydromorphone is preferred if a patient has moderate to severe renal impairment.
Fentanyl is preferred over morphine or hydromorphone in severe renal impairment
25Palliative sedation
“Usual” Palliative Care Palliative care for COVID-19 +ve patient
• Methotrimeprazine or midazolam Potential drug shortages.
continuous infusion first choice. • If shortages of midazolam occur,
• Phenobarbital is second or third methotrimeprazine becomes a first choice.
line, added to midazolam if • If infusion pumps are not available, may have
midazolam alone is ineffective. to use intermittent injections of midazolam (or
First-line options
methotrimeprazine).
• If methotrimeprazine or midazolam are not
available, may use lorazepam or phenobarbital
as first choice.
26Emergency kits
“Usual” Palliative Care Palliative care for COVID-19 +ve patient
• Emergency kits in the home often promoted for EOL care at In the pandemic, there is a great risk of significant
home. wastage of precious medications such as
• Generic kits with medications such as opioid, midazolam if generic kits are prescribed and
haloperidol, methotrimeprazine, scopolamine. cannot be reused
• But once dispensed, the medications cannot be reused
for anyone else and have to be disposed of, resulting in
wastage.
• Some recommend instead a just-in-time, tailored-to-specific-
patient approach;
• Requires a system in place with 24/7 access to
pharmacy services (difficult in rural regions or small
communities).
27Opioids and dyspnea
• Multiple studies have shown that opioids are effective for treating dyspnea,
and are recommended even in patients with advanced lung disease.
• Opioids treat dyspnea through many mechanisms
o Reducing respiratory drive
o Reducing anxiety
o Altering central responses to exertion
o Cough suppression
Ma h ler a nd O ’D o nnell, C H EST 2 015; 1 47( 1):232 -241.
H a yen e t a l. N e uroimage 2 017;150:383 -94. 28Opioids and dyspnea
• Symptom-titrated opioids do not hasten death
• In severe COPD, opioids…
o Reduce dynamic hyperinflation and work of breathing
o Allow the patient to take slower, deeper breaths
o Have been used in large studies with no reports of clinically-important respiratory
depression
• In cancer, ALS and severe COPD, opioids…
o Improve dyspnea and reduce respiratory rate without increasing CO2
Breathing is necessary for life. Shortness of breath is not.
Ab dallah e t a l. Eu r R e sp J 2 017;50:1701235.
C u r r ow e t a l. J PSM 2 011;42:388 -99. 29McMaster Dyspnea in
COVID-19 Protocol
Adapted from BC Centre for
Palliative Care and Fraser
Health Protocol
30Dyspnea in COVID-19
See next slide for each of these treatment arms 31Dyspnea in COVID-19
32
See next slide for next treatment arm and more informationDyspnea in COVID-19
See next slide for next treatment arm and more information
33UPPER AIRWAY SECRETIONS
• If mild, no drugs needed. No suctioning or meds.
• If moderate to severe. No suctioning. Start pharmacological treatment:
• Scopolamine: 0.4-0.6mg subcut q 4hrs PRN (more sedating than
glycopyrrolate, which may be useful if patient is also agitated)
OR
Airway • Glycopyrrolate: 0.4mg subcut q 4hrs PRN
Secretions
Timely management is important.
Select according to availability of medications.
LOWER AIRWAY SECRETIONS
Likely ARDS/pulmonary edema. Administer furosemide 20mg - 40 subcut/IV
q2hrs PRN and monitor
34• If on opioid already, titrate (see Dyspnea protocol)
• If not on opioid:
o If moderate, select one of the following:
▪ Dextromethorphan 10mg-20mg PO q 4-6 hrs PRN
▪ Hydrocodone 5mg q 4-6hrs PRN
▪ Normethadone antitussive (Cophylac) 15 drops po QHS or BID
(Not covered by some provincial plans)
Cough o If severe:
Start opioid
▪ Morphine 2.5 - 5 mg PO q4hrs (SC dose is ½ of oral dose)
Or
▪ Hydromorphone 0.5 - 1 mg PO Q4H (SC dose is ½ of oral dose)
▪ For any opioid, reduce the dose by half and consider q6hrly
dosing if patient is frail, elderly or has advanced comorbid illness.
▪ If moderate to severe renal impairment, use hydromorphone
instead of morphine.
35Useful resources
Several useful resources are available to help you manage symptoms:
• BC Centre for Palliative Care bc-cpc.ca/cpc/all-resources/hcp-resources
• Fraser Health; Island Health
o “Actively Dying Protocol”, with new CRISIS orders for COVID-19 patients. Actively
Dying Protocol Part 1, Actively Dying Protocol Part 2, FH Actively Dying Protocol
COVID-19 Addendum 3-4-20.
o Island Health: PPOs for dyspnea management; Palliative Sedation
• Arya et al. Pandemic Palliative Care: Beyond Ventilators and Saving Lives. CMAJ
31 March 2020 https://www.cmaj.ca/content/early/2020/03/31/cmaj.200465
• Canadian Association of Emergency Physicians Protocol: End-of-life care in the
Emergency Department for the patient imminently dying of a highly transmissible
acute respiratory infection (such as COVID-19)
36Conclusions
• Breathlessness is a common presentation in moderate to severe COVID-
19 disease.
• It can take a fulminant course in some cases.
• Opioids offer a very useful and safe symptom management option.
• Become acquainted with protocols in your region, or where these are
absent, use protocols such as the ones from Fraser Health and McMaster.
37Wrap up
• We would appreciate your feedback. You will receive a link to evaluate
the webinar.
• This session is being recorded and will be emailed to webinar registrants
tomorrow or available here: www.pallium.ca/pallium-canadas-covid-19-
response-resources
38THANK YOU
You can also read