ACNR ADVANCES IN CLINICAL NEUROSCIENCE & REHABILITATION
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ISSN 1473-9348 VOLUME 20 ISSUE 3 > 2021
ACNR
ADVANCES IN CLINICAL NEUROSCIENCE & REHABILITATION
www.acnr.co.uk
In this issue
Cristina Simonet and Alastair Noyce – Mild parkinsonian signs: the interface between ageing and Parkinson’s disease
Kate Lilley, Sudarshini Ramanathan, Russell C Dale, Fabienne Brilot and Simon Broadley
– MOG antibody associated disorder (MOGAD)
Manoj Sivan, Stephen Halpin, Jeremy Gee, Sophie Makower, Amy Parkin, Denise Ross, Mike Horton
and Rory O’Connor – The self-report version and digital format of the COVID-19 Yorkshire Rehabilitation Scale (C19-YRS)
for Long COVID or Post-COVID syndrome assessment and monitoring
Ann Williamson – Hypnotic interventions in the management of chronic pain
Richard Sylvester, Richard Greenwood, Camille Julien and Brent Eliot – The Queen Square Brain Injury Clinic
ACNR > VOLUME 20 NUMBER 3 > 2021 > 1
BOOK REVIEWS > INDUSTRY NEWS > CONFERENCE PREVIEWS AND REPORTS > EVENTS DIARY
Sialanar
(400mcg/ml glycopyrronium bromide
®
equivalent to 320mcg/ml glycopyrronium)
Symptomatic treatment of severe
sialorrhoea in children aged 3 years and
older, with chronic neurological disorders
Designed for Children
Sialanar® is +25% more bioavailable than
glycopyrronium bromide 1mg/5mL oral solution1,3
Benefits of dispensing Sialanar® Other glycopyrronium
for patients under your care: bromide solutions:
TESTED AND LICENSED FOR NOT LICENSED FOR TESTED AND LICENSED FOR NOT LICENSED FOR
CONCENTRATED SOLUTION NON–CONCENTRATED SOLUTION CONCENTRATED SOLUTION USENON–CONCENTRATED
WITH FEEDING TUBES SOLUTION USE WITH FEEDING TUBES USE WITH FEEDING TUBES USE WITH FEEDING TUBES
Concentrated solution
May result in greater volume
(2mg/5ml glycopyrronium
of liquid for equivalent dose
bromide) therefore relatively
of Sialanar®
TESTED AND LICENSED FOR NOT LICENSED FOR TESTED AND LICENSED FOR NOT LICENSED FOR
LUTION USE WITH FEEDING TUBESSOLUTION
NON–CONCENTRATED USE WITH FEEDING TUBES USE WITH FEEDING TUBES USE WITH FEEDING TUBES
small volume to swallow
SYRINGE FOR TITRATION AND CORRECT USE CUP OR SPOON SYRINGE FOR TITRATION AND CORRECT USE IN USE SHELF LIFE
CUP=OR
60SPOON
DAYS IN USE SHELF LIFE VARIES = 14–28 DAYS
IN USE SHELF LIFE = 60 DAYS IN USE SHELF LIFE VARIES = 14–28 DAYS
Minimal excipients –
Some glycopyrronium
sugar free, alcohol free
solutions
14 contain sorbitol 14
D CORRECT USE IN USE SHELFCUP
LIFEOR SPOON
= 60 DAYS
and sorbitol free IN USE SHELF LIFE = 60 DAYS
IN USE SHELF LIFE VARIES = 14–28 DAYS
60
IN USE SHELF LIFE VARIES = 14–28 DAYS
DAYS
28
DAYS
60
DAYS
28
DAYS
14 14 In use shelf life
60 28 life 6060
In use shelf days 28 varies 14 to 28 days
STORED BELOW 25ºC AND IN THE STORED BELOW 25ºC AND IN THE
NO SPECIAL STORAGE CONDITIONS ORIGINAL CARTON TO PROTECTNO SPECIAL STORAGE CONDITIONS ORIGINAL CARTON TO PROTECT
PALATABLE TASTE
DAYS
SOME HAVE A PALATABLE TASTE
DAYS DAYS
PALATABLE TASTE SOME HAVE A PALATABLE TASTE
DAYS
STORED BELOW 25ºC AND IN THE STORED BELOW 25ºC AND IN THE
NO SPECIAL STORAGE CONDITIONS NO SPECIAL STORAGE CONDITIONS ORIGINAL CARTON TO PROTECT
TE SOME HAVE A PALATABLE TASTE ORIGINAL CARTON TO PROTECT
New BNFc Oral solutions are not interchangeable on a microgram-for-
update microgram basis due to differences in bioavailability2
www.proveca.com
Prescribing Information UK
Sialanar® 320 micrograms /ml oral solution Sialanar® contains 2.3 mg sodium benzoate (E211) in each ml. Patients require daily dental
hygiene and regular dental checks. Thicker secretions may increase risk of respiratory
Please refer to the full Summary of Product Characteristics (SmPC) before prescribing. infection and pneumonia. Moderate influence on ability to drive/use machines.
Presentation: Glycopyrronium oral solution in 250 ml or 60 ml bottle. 1 ml solution contains Fertility, pregnancy and lactation: Use effective contraception. Contraindicated in
400 micrograms glycopyrronium bromide, (equivalent to 320 micrograms of the active pregnancy and breast feeding.
ingredient, glycopyrronium).
Undesirable effects: Adverse reactions more common with higher doses and prolonged
Indication: Symptomatic treatment of severe sialorrhoea (chronic pathological drooling) use. In placebo-controlled studies (≥15%) dry mouth, constipation, diarrhoea and vomiting,
in children and adolescents aged 3 years and older with chronic neurological disorders. urinary retention, flushing and nasal congestion. In paediatric literature; very common:
irritability, reduced bronchial secretions; common: upper respiratory tract infection,
Dosage: Start with approximately 12.8 micrograms/kg body weight of glycopyrronium pneumonia, urinary tract infection, agitation, drowsiness, epistaxis, rash, pyrexia. The
per dose, three times per day. Increase dose weekly until efficacy is balanced with side Summary of Product Characteristics should be consulted for a full list of side effects.
effects. Titrate to maximum individual dose of 64 mcg/kg body weight glycopyrronium or
6 ml three times a day, whichever is less. Monitor at least 3 monthly for changes in efficacy Shelf life: 2 years unopened. 2 months after first opening.
and/or tolerability and adjust dose if needed. Not for patients less than 3 or over 17 years
old as Sialanar® is indicated for the paediatric population only. Reduce dose by 30%, in MA number: References:
mild/moderate renal failure. Dose at least one hour before or two hours after meals or at Sialanar® 250 ml bottle – EU/1/16/1135/001 1. Data on file, 2020
consistent times with respect to food intake. Avoid high fat food. Flush nasogastric tubes Sialanar® 60ml bottle – EU/1/16/1135/002 2. BNFc – Last updated: 29 October 2020
with 10 ml water. 3. PAR Glycopyrronium bromide 1mg/5ml Oral solution
Legal Category: POM
Contraindications: Hypersensitivity to active substance or excipients; pregnancy and Basic NHS Price:
breast-feeding; glaucoma; urinary retention; severe renal impairment/dialysis; history of Sialanar® 250 ml bottle £320 Adverse events should be reported.
intestinal obstruction, ulcerative colitis, paralytic ileus, pyloric stenosis; myasthenia gravis; Sialanar® 60ml bottle £76.80
concomitant treatment with potassium chloride solid oral dose or anticholinergic drugs. Reporting forms and information can be
Marketing Authorisation Holder (MAH): found at: www.mhra.gov.uk/yellowcard
Special warnings and precautions for use: Monitor anticholinergic effects. Carer should Proveca Pharma Ltd. Marine House,
stop treatment and seek advice in the event of constipation, urinary retention, pneumonia, Clanwilliam Place, Dublin 2, Ireland Adverse events should also be reported
allergic reaction, pyrexia, very hot weather or changes in behaviour. For continuous or repeated Further prescribing information can
intermittent treatment, consider benefits and risks on case-by-case basis. Not for mild to be obtained from the MAH. to Proveca Limited. Phone: 0333 200
moderate sialorrhoea. Use with caution in cardiac disorders; gastro-oesophageal reflux disease; Date of last revision of prescribing 1866 E-mail: medinfo@proveca.co.uk
pre-existing constipation or diarrhoea; compromised blood brain barrier; in combination with: information: April 2019
antispasmodics, topiramate, sedating antihistamines, neuroleptics/antipsychotics, skeletal
muscle relaxants, tricyclic antidepressants and MAOIs, opioids or corticosteroids. Date of preparation: March 2021 UK-SIA-2021-029
f r o m t h e c o - e d i t o r ...
Todd Hardy, BSc (Hons), PhD, MBBS, FRACP, is Co-Editor of ACNR and is a Staff
Editorial board and contributors
Specialist Neurologist at Concord Repatriation General Hospital, Clinical Associate
Professor in Neurology at the University of Sydney, and Co-Director of the MS
Clinic at the Brain and Mind Centre. His main interests are multiple sclerosis and
I
t is a hot hot day in July, and other immune-mediated central nervous system disorders.
already 2021 has seemed like
a long year to many of us, as Ann Donnelly, MB, ChB, BSc (Clin Neurosci), MRCP, is Co-Editor of ACNR and
we face a possible third wave, a Consultant in Neurology at the Royal Free London Neurological Rehabilitation
and also try to find some green Centre. She completed undergraduate training at University of Glasgow Medical
School, with Neurology postgraduate training at Kings College Hospital, National
zones we can travel to for much Hospital for Neurology and Neurosurgery, and Guys and St Thomas’ Hospital. She is
needed holidays. interested in neurorehabilitation with a focus on patients with multiple sclerosis.
Despite the fatigue indu-
cing heat, this issue is exciting, Kirstie Anderson, BMedSci, MBBS, MRCP, DPhil (Oxon), is Editor of our Sleep Section and runs the
enlivening and full of clinic- Regional Neurology Sleep Service with a clinical and research interest in all the sleep disorders. She is an
Honorary Senior Lecturer at Newcastle University with an interest in the link between sleep and mental
ally eloquent articles which Ann Donnelly, Co-Editor. health.
can help us to improve clinical
practice across the board of Anish Bahra, MB, ChB, FRCP, MD, is Editor for our Headache Series and Consultant Neurologist at
neurology and neuro-rehabilitation, from an international group Barts Health and the National Hospital for Neurology and Neurosurgery (NHNN), UK. Her specialist
interest is in primary and secondary headache disorders having completed her original research in
of authors. Cluster headache. She runs a tertiary Headache service at the NHNN and a neurostimulation MDT at
Simonet and Noyce from the Wolfson Institute of Preventive Barts Health.
Medicine, Queen Mary University of London, look at what we
know about patients with mild Parkinsonian signs. They methodic- Roger Barker, MRCP, PhD, F.Med.Sci., is Consulting Editor of ACNR, Professor of Clinical Neuroscience
at the University of Cambridge and an Honorary Consultant in Neurology at The Cambridge Centre for
ally help us to consider how we might differentiate between nigros- Brain Repair. His main area of research is into neurodegenerative and movement disorders, in particular
triatal degeneration and normal ageing, reviewing evidence about Parkinson’s and Huntington’s disease.
early signs, and looking at areas where we need further research.
From Sydney and the Gold Coast, Lilley et al provide a clear and Alasdair Coles, PhD, is Consulting Editor of ACNR. He is a Professor in Neuroimmunology at
Cambridge University. He works on experimental immunological therapies in multiple sclerosis.
clinically important review of MOG antibody associated disorders,
evaluating current treatment options, and again shining a light on
Rhys Davies, MA, BMBCh, PhD, MRCP, is Editor of our Book Review Section. He was accredited as a
where we may need to look in future. Consultant Neurologist on the specialist register in 2009 and is currently a Consultant Neurologist at
The CNR group at the National Hospital for Neurology and the Walton Centre for Neurology and Neurosurgery in Liverpool and at Yssbyty Gwynedd in Bangor,
Neurosurgery once again have set the standard for neurorehabili- North Wales. He has a clinical and research interest in cognitive neurology.
tation, this time outlining how the Queen Square Brain Injury clinic
Ellie Edlmann, MRCS, PhD, is ACNR’s Assistant Neurosurgery Editor and is a Clinical Lecturer in
for traumatic brain injury can offer specialist input, and excellence Neurosurgery at University of Plymouth. She has a keen research interest in head injury, clinical trials
of care to a complex group of patients and their families. and neurosurgery in older patients. She completed her PhD at the University of Cambridge, and has
The ABN trainees have updated an article written many years been active in national and international research collaboratives.
ago by myself, on how to prepare for the SCE examination. It is full
Rosemary Fricker, PhD, FHEA, is our Nutrition and Stem Cells Editor. She is currently Visiting Professor
of great tips and useful links. Wishing this year’s group the best of
of Neurobiology at Keele University, and the former Director of Medical Science at Keele Medical
luck for the exams ahead, this article will definitely help you. School. She graduated with a PhD in Neuroscience from Cambridge University and her areas of research
Dr Ann Williamson looks back on her decades of experience are in developing cell replacement therapies for neurodegenerative disease, stem cells, and the role of
vitamins in neuronal development and neural repair.
with Hypnosis and its utility in the management of chronic pain.
This area can be resistant to most available clinical approaches
Manoj Sivan, MD, FRCP, is the Editor of our Pain and Rehabilitation Section and is an Associate Clinical
and her article provides us with a few more potential tools for Professor and Honorary Consultant in Rehabilitation Medicine (RM) with University of Leeds and Leeds
management. Teaching Hospitals and a Honorary Senior Lecturer in the Human Pain Research Group with University of
Once again JMS Pearce places a common symptom, vertigo, into Manchester. His research interests are pain medicine, rehabilitation technology, chronic conditions and
outcome measurement.
its historical context. His articles usually delve into the brilliantly
detailed observations of Neurologists of the past, who, without our Marco Mula, MD, PhD,FRCP, FEAN, is Editor of our Epilepsy Section. He is a Consultant in Neurology
current imaging tools, were able to describe and define syndromes and Epileptology at St George’s University Hospital and Reader in Neurology at St George’s University of
using clinical skill alone. They succeeded in their work against all London. He is a Fellow of the Royal College of Physicians and the European Academy of Neurology as
well as a member of the Royal College of Psychiatrists. He has authored more than 200 publications and
odds. Memorably, Robert Bárány received the Nobel Prize for his three books in the field of epilepsy.
semicircular canal research whilst in a prisoner of war camp in
1914. Ed Newman, BSc(MedSci), MD, FRCP, is ACNR's Movement Disorders Editor. He is a Consultant
The book reviews of two relevant Oxford Handbooks Neurologist at Queen Elizabeth University Hospital and Glasgow Royal Infirmary. He has a specialist
interest in movement disorders and Parkinson’s disease. He is part of the national DBS service in
(Neurorehabilitation and Neuropsychiatry) provide excellent Scotland and runs a Parkinson’s disease telemedicine service to Western Isles. He also runs the clinical
insight with practical opinions. neurosciences teaching programme for University of Glasgow’s Medical School.
As we look ahead, with recent relaxation of COVID regulations,
wondering what lies ahead for our patients, Sivan et al and the team Emily Thomas, BmBCh, MRCP, PhD, is the Editor of our Rehabilitation Section.She is a Consultant in
Rehabilitation working for Solent NHS Trust, Southampton. Her main interests are holistic brain injury,
from University of Leeds have produced a much lauded COVID 19
rehabilitation and spasticity management.
Yorkshire Rehabilitation Scale (Covid-19 YRS) questionnaire. This
helps us to assess long COVID and post COVID syndrome patients David Werring, FRCP, PhD, FESO, is ACNR’s Stroke Editor. He is Professor of Clinical Neurology at
comprehensively and monitor the effects of intervention. The ques- UCL Institute of Neurology, Queen Square, and Honorary Consultant Neurologist at University College
tionnaire, which can be downloaded from our site is now recom- Hospital and The National Hospital, Queen Square.
mended by NICE. From a more personal view, Dr Larner writes
Peter Whitfield, BM (Distinction in Clin Med), PhD, FRCS Eng., FRCS, SN, FHEA, is ACNR’s Neurosurgery
about his first hand post COVID experience and muses about the Editor. He is a Consultant Neurosurgeon at the South West Neurosurgery Centre, Plymouth. His clinical
possible relationship between Post COVID lassitude, or other forms interests are wide including neurovascular conditions, head injury, stereotactic radiosurgery, image
of apathy and a failure of the Bereitschaftspotential. It is a thought guided tumour surgery and lumbar microdiscectomy. He is an examiner for the MRCS and is a member
of the SAC in neurosurgery.
provoking hypothesis.
I hope you enjoy this issue, and wishing you a safe and relaxing
Michael Zandi, MA, MB, BChir, PhD, FRCP, is a Consulting and former Editor of ACNR. He is Consultant
summer ahead. Neurologist at the National Hospital for Neurology and Neurosurgery, Queen Square and UCLH,
London. He is Honorary Associate Professor in the University College London Queen Square Institute of
Neurology Department of Neuromuscular Diseases.
Ann Donnelly, Co-Editor
E. Rachael@acnr.co.uk
Angelika Zarkali, MBBS, PGDip, MRCP, is the Editor of our Conference News section. She is a
Research Fellow in the Dementia Research Centre, UCL and a Specialist Registrar in Neurology in St
George's hospital. She has an interest in neurodegeneration and cognitive disorders.
ACNR > VOLUME 20 NUMBER 3 > 2021 > 3
CONTENTS VOLUME 20 ISSUE 3
New Editorial Team
Members
ACNR is delighted to have welcomed several new
CLINICAL REVIEW ARTICLES members to our editorial team over recent months.
07 Mild parkinsonian signs: the interface between ageing and Parkinson’s If you have an article you would like considered for
disease – Cristina Simonet and Alastair Noyce these sections, please contact us in the first instance
12 MOG antibody associated disorder (MOGAD) – Kate Lilley, Sudarshini Ramanathan, via Rachael@acnr.co.uk
Russell C Dale, Fabienne Brilot and Simon Broadley
CLINICAL VIEWPOINT Anish Bahra, MB, ChB,
16 The self-report version and digital format of the COVID-19 Yorkshire FRCP, MD,
Rehabilitation Scale (C19-YRS) for Long COVID or Post-COVID syndrome will be co-ordinating our Headache series.
assessment and monitoring – Manoj Sivan, Stephen Halpin, Jeremy Gee, Sophie Makower, She is Consultant Neurologist at Barts Health
Amy Parkin, Denise Ross, Mike Horton and Rory O’Connor and the National Hospital for Neurology and
Neurosurgery (NHNN), UK. Her specialist
PAIN SERIES ARTICLE interest is in primary and secondary headache
disorders having completed her original
20 Hypnotic interventions in the management of chronic pain – Ann Williamson
research in Cluster headache. Anish runs a
REHABILITATION ARTICLE tertiary Headache service at the NHNN and a
neurostimulation MDT at Barts Health.
23 The Queen Square Brain Injury Clinic – Richard Sylvester, Richard Greenwood,
Camille Julien and Brent Eliot
Ellie Edlmann, MRCS, PhD,
SPECIAL FEATURES is ACNR’s Assistant Neurosurgery Editor and a
26 ABNT – How to prepare for the SCE in Neurology – Harriet Ball, Mahjabin Islam Clinical Lecturer in Neurosurgery at University
of Plymouth. Ellie has a keen research interest
and Angelika Zarkali
in head injury, clinical trials and neurosurgery
28 ABNT – Navigating the labyrinth of integrated academic training in in older patients. She completed her PhD at
neurology: a guide for the uninitiated – Mahjabin Islam and Gargi Banerjee the University of Cambridge, and has been
active in national and international research
33 Personal Perspectives – COVID-19, lassitude, and the Bereitschaftspotential
collaboratives.
– Andrew Larner
34 History of Neurology – Origins of Vertigo – JMS Pearce
Rosemary Fricker, PhD,
REGULARS FHEA,
11 & 32 Industry News is ACNR’s Nutrition and Stem Cells Series
Editor. She is currently Visiting Professor of
15 Awards and Appointments
Neurobiology at Keele University, and the
35 Book Reviews former Director of Medical Science at Keele
38 Conference News Medical School. She graduated with a PhD in
Neuroscience from Cambridge University and
46 Events Diary her areas of research are in developing cell
replacement therapies for neurodegenerative
Cover image: Our cover image this issue is from Taylor P Kuhn, PhD, Adjunct Assistant Professor, UCLA disease, stem cells, and the role of vitamins in
Semel Institute for Neuroscience and Human Behavior, USA, and is a still from his animated entry into neuronal development and neural repair.
the OHBM BrainArt competition. The animation can be viewed on our online cover at www.acnr.co.uk
For more information see page 32. Marco Mula, MD, PhD,
FRCP, FEAN,
is Editor of our Epilepsy series. He is
Consultant in Neurology and Epileptology at
St George’s University Hospital and Reader
ACNR in Neurology at St George’s University of
London. He is a Fellow of the Royal College
Published by Whitehouse Publishing, 1 The Lynch, Mere, Wiltshire, BA12 6DQ. of Physicians and the European Academy of
Publisher. Rachael Hansford E. rachael@acnr.co.uk Neurology as well as a member of the Royal
PUBLISHER AND ADVERTISING College of Psychiatrists. He has authored
Rachael Hansford, T. 01747 860168, M. 07989 470278, E. rachael@acnr.co.uk more than 200 publications and three books
COURSE ADVERTISING Rachael Hansford E. Rachael@acnr.co.uk in the field of epilepsy championing an
holistic approach to patients with epilepsy.
EDITORIAL Anna Phelps E. anna@acnr.co.uk
DESIGN Donna Earl E. production@acnr.co.uk
Printed by Stephens & George Ed Newman, BSc(MedSci),
Disclaimer: The publisher, the authors and editors accept no responsibility for loss incurred by any person acting or
MD, FRCP,
refraining from action as a result of material in or omitted from this magazine. Any new methods and techniques described is Editor of our Movement Disorders section.
involving drug usage should be followed only in conjunction with drug manufacturers’ own published literature. This is an He is Consultant Neurologist at Queen
independent publication - none of those contributing are in any way supported or remunerated by any of the companies Elizabeth University Hospital and Glasgow
advertising in it, unless otherwise clearly stated. Comments expressed in editorial are those of the author(s) and are not Royal Infirmary. He has a specialist interest
necessarily endorsed by the editor, editorial board or publisher. The editor’s decision is final and no correspondence will be in movement disorders and Parkinson’s
entered into. disease. He is part of the national DBS service
ACNR's paper copy is published quarterly,with Online First content and additional email updates. in Scotland and runs a Parkinson’s disease
Sign up at www.acnr.co.uk/subscribe-to-acnrs-e-newsletter telemedicine service to the Western Isles.
Ed is also interested in medical education
@ACNRjournal /ACNRjournal/ and runs the clinical neurosciences teaching
programme for University of Glasgow’s
Medical School.
4 > ACNR > VOLUME 20 NUMBER 3 > 2021
▼
KESIMPTA IS NOW LICENSED FOR THE TREATMENT OF ADULT
Not representative
of an actual patient -
PATIENTS WITH RELAPSING FORMS OF MULTIPLE SCLEROSIS (RMS)
this image is intended WITH ACTIVE DISEASE DEFINED BY CLINICAL OR IMAGING FEATURES1
to depict the brand.
EFFICACY PRECISION FLEXIBILITY
SUPERIOR, SUSTAINED EFFICACY
in clinical studies vs teriflunomide1,2
• Significant reduction in ARR of up to 59% vs teriflunomide (PReferences: 1. Novartis Pharmaceuticals UK Ltd. Kesimpta® (ofatumumab): Summary of Product Characteristics, Great Britain; April 2021; 2. Hauser SL,
et al. New Engl J Med. 2020;383(6):546–557; 3. Data on file. OMB157 (ofatumumab). Novartis Pharmaceuticals Corp; East Hanover, NJ. December 2019; 4.
Hauser SL, et al. Ofatumumab vs Teriflunomide in Relapsing Multiple Sclerosis: Analysis of No Evidence of Disease Activity (NEDA-3) from ASCLEPIOS I
and II Trials. Presented at the 6th European Association of Neurology Congress as Virtual Congress; 23–26 May 2020. Poster LB62; 5. Migotto M-A, et al.
Neurology. 2018;90(15 Supplement):P3.406; 6. Smith P, et al. Neurology. 2017;88(16 Supplement):P2.359; 7. Perrin Ross A, et al. Patient and Nurse Preferences
for the Sensoready® Autoinjector Pen Versus Other Autoinjectors in Multiple Sclerosis: Results From a Multicenter Survey. Poster presented at the Americas
Committee for Treatment and Research in Multiple Sclerosis Forum 2021; 25–27 February 2021. Poster P210; 8. Data on file. OMB157 (ofatumumab). OMB 157G
5.3.5.3. Statistical overview. Novartis Pharmaceuticals Corp; East Hanover, NJ. December 2019.
Great Britain Prescribing Information: prior to initiation of ofatumumab for live or live-attenuated vaccines and,
whenever possible, at least 2 weeks prior to initiation of ofatumumab for
Kesimpta®▼ (ofatumumab) inactivated vaccines. Ofatumumab may interfere with the effectiveness
of inactivated vaccines. The safety of immunisation with live or live-
Important note: Before prescribing Kesimpta 20 mg solution for injection
attenuated vaccines following ofatumumab therapy has not been studied.
in pre-filled pen consult Summary of Product Characteristics (SmPC).
Vaccination with live or live-attenuated vaccines is not recommended
Presentation: Solution for injection in pre-filled pen. Each pre-filled pen during treatment and after discontinuation until B-cell repletion. In
contains 20 mg ofatumumab in 0.4 ml solution (50 mg/ml). Ofatumumab infants of mothers treated with ofatumumab during pregnancy live or
is a fully human monoclonal antibody produced in a murine cell line (NS0) live-attenuated vaccines should not be administered before the recovery
by recombinant DNA technology. of B-cell counts has been confirmed. Depletion of B cells in these infants
Indication(s): Kesimpta is indicated for the treatment of adult patients may increase the risks from live or live-attenuated vaccines. Inactivated
with relapsing forms of multiple sclerosis (RMS) with active disease vaccines may be administered as indicated prior to recovery from B-cell
defined by clinical or imaging features. depletion.
Dosage and administration: Treatment should be initiated by a physician Interactions: No interaction studies have been performed, as no
experienced in the management of neurological conditions and the first interactions are expected via cytochrome P450 enzymes, other
injection should be performed under the guidance of an appropriately metabolising enzymes or transporters. The response to vaccination could
trained healthcare professional. The product is intended for patient self- be impaired when B cells are depleted. The risk of additive immune system
administration by subcutaneous injection. The recommended dose is effects should be considered when co-administering immunosuppressive
20 mg ofatumumab with initial dosing at weeks 0, 1 and 2, followed by therapies with ofatumumab.
subsequent monthly dosing, starting at week 4. Paediatric population: The Fertility, pregnancy and lactation: Women of childbearing potential
safety and efficacy of ofatumumab in children aged 0 to 18 years have should use effective contraception while receiving ofatumumab and for
not yet been established. 6 months after the last product administration. There is a limited amount
Contraindications: Hypersensitivity to the active substance or to any of of data from the use of ofatumumab in pregnant women. Treatment with
the excipients. Patients in a severely immunocompromised state. Severe ofatumumab should be avoided during pregnancy unless the potential
active infection until resolution. Known active malignancy. benefit to the mother outweighs the potential risk to the foetus. The use
Warnings/Precautions: Injection-related reactions: Patients should be of ofatumumab in women during lactation has not been studied. It is
informed that injection-related reactions (systemic) could occur, generally unknown whether ofatumumab is excreted in human milk. There are no
within 24 hours and predominantly following the first injection. From data on the effect of ofatumumab on human fertility.
clinical studies the most frequently reported symptoms include fever, Undesirable effects: Very common (≥1/10): upper respiratory tract
headache, myalgia, chills and fatigue. Injection-related reactions can infections, urinary tract infections, injection-site reactions (local),
be managed with symptomatic treatment, use of premedication is not Injection-related reactions (systemic). Common (≥1/100 toclinical review article
Mild parkinsonian
signs: the interface
Cristina Simonet, MD,
between ageing and
Parkinson’s disease
is a Consultant in Neurology and Movement
Disorders. She finished her Neurology training
in Spain in 2016. She has had a special interest
in Parkinson’s disease since the beginning of
her training. She joined the PREDICT-PD team
in September 2018, which was a new challenge
for her. She is based at Wolfson Institute of
Preventive Medicine and her research is based on Abstract are known to be present at early stages of PD
studying the early motor features of Parkinson’s Mild Parkinsonian Signs (MPS) describe a (see Figure). We will focus on these domains
Disease.
spectrum that exists between the expected one by one.
motor decline of normal ageing and a more
serious motor deterioration resulting from Bradykinesia
Parkinson’s disease (PD) and neurodegen- Bradykinesia is the only clinical sign that is
eration. Although MPS are a feature of the required to be present in every patient with
prodromal stage of PD, their formal definition PD according to the Queen Square Brain
is unclear and still relies somewhat on conven- Bank Criteria.11 It is described as the ‘slow-
tional clinical criteria for PD. This review will ness of movement initiation with progressive
summarise the early motor features of PD and reduction in speed and amplitude (sequence
methods of assessment, from conventional effect) of repetitive actions’.12 It is interpreted
Alastair Noyce, PhD, MRCP, clinical scales to advances in quantitative by patients as clumsiness or weakness when
is a Reader in Neurology and Neuroepidemiology
at the Preventive Neurology Unit in the Wolfson measures. Finally, the boundaries of motor performing fine and repetitive movements.
Institute of Preventive Medicine, Queen decline as part of normal ageing and patho- Compensatory mechanisms help to maintain
Mary University of London, and a Consultant logical neurodegeneration will be discussed. stable dopaminergic transmission and motor
Neurologist at Barts Health NHS Trust. Alastair function at early stages of PD.13 However,
graduated from Barts and the London School
of Medicine and Dentistry in 2007. He pursued these compensatory mechanisms can fail
integrated training via the Foundation Academic Introduction when more challenging tasks are performed
Programme and an NIHR Academic Clinical Mild Parkinsonian Signs (MPS) describe with associated ‘unmasking’ of subtle motor
Fellowship at UCL. In August 2012, he left clinical the motor spectrum that spans from normal deficits.4
training to pursue a PhD in Neuroscience at UCL.
Between 2014-2016 he undertook an MSc in ageing to the early stages of Parkinson’s Changes in handwriting are thought to be an
Epidemiology at the London School of Hygiene disease (PD).1 A variety of other terms have early sign of PD,14 with micrographia (gradual
and Tropical Medicine. His main research interests been used to describe these features, such as reduction in letter size) being an example of
are Parkinson’s disease and related disorders, subthreshold parkinsonism and subtle motor/ ‘real-world’ bradykinesia.15 In some studies,
particularly early identification and epidemiology,
including environmental, clinical and genetic parkinsonian signs. PD is generally a slowly micrographia has been documented up to
determinants. progressive degenerative disease and because four years before diagnosis.16 Recently, the
it is diagnosed on the basis of established and term ‘dysgraphia’ has been introduced. It goes
Correspondence to: Alastair Noyce, Preventive
Neurology Unit, Wolfson Institute of Preventive typical motor features, subtle motor manifesta- further than micrographia and includes other
Medicine, Barts and the London School of tions may be apparent years before the diag- kinetic variables apart from the script size,
Medicine and Dentistry, Queen Mary University nosis.2 However, many MPS are not specific to such as velocity, fluency, and sentence slope
of London, London, UK.
PD and may not progress in the same manner; which may help to detect even earlier changes
E. a.noyce@qmul.ac.uk
substantial overlap with normal ageing is to in handwriting.14
Conflict of interest statement: None declared be expected.3 Similar to handwriting, speech is an
Provenance and peer review: Submitted and The phase before a diagnosis of PD has often automated task that requires a high level
externally reviewed been referred to as the ‘pre-motor’ phase, but of motor coordination. Abnormalities may
Date first submitted: 15/09/2020 the truth is that motor features in the pre-diag- appear at early stages of PD; hypophonia,
Date submitted after peer review: 4/03/2021 nostic phase have received surprisingly little poor articulation, and hesitation are some of
Acceptance date: 5/03/2021 attention compared to non-motor features.4 the manifestations of vocal hypokinesia.17 The
Published online: 22/6/2021 As such, it is difficult to say whether there is Oxford Discovery Parkinson’s Cohort (OPDC)
To cite: Simonet C, Noyce A. Adv Clin Neurosci a definite ‘pre-motor’ phase, when objective included smartphone-based voice analysis as
Rehabil 2021;20(3):7-11 motor dysfunction has been observed in many part of a motor battery. Speech and tremor
This is an open access article distributed under prodromal settings.5-8 Although several studies were found to be the most discriminatory
the terms & conditions of the Creative Commons have objectively documented motor markers of markers between patients with PD, patients
Attribution license http://creativecommons.org/ neurodegeneration in PD (see Table 1), there is with REM-sleep behaviour disorder (RBD) and
licenses/by/4.0/
https://doi.org/10.47795/KHGP5988
still controversy about when they exactly start controls.18 In a separate case-control study,
and how reliably they can be detected. footage of video recordings from interviews
and press conferences on television were used
Defining MPS to extract acoustic measurements and demon-
MPS in the elderly population without PD strated changes in voice frequency up to five
cluster into four domains: bradykinesia, years prior to diagnosis of PD.19 A reduction in
tremor rigidity, and gait and posture.9,10 They spontaneous (involuntary) eye-blinking and
ACNR > VOLUME 20 NUMBER 3 > 2021 > 7clinical review article
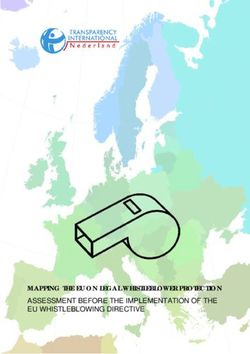
Table 1. Summary of remarkable but non-exhaustive list of epidemiological studies proving the existence of motor prodromes
Study Design Follow-up Sample size Age (years) Motor assessment Findings
Motor progression ( tremor > rigidity > postural
General impression
abnormalities > falls
MPS were associated to
Bruneck cohort 284(MPS+) 66.5±7.8 SN-hyperechogenicity (OR: 2.0),
Longitudinal cohort 5 years UPDRS-III
[57] 109(MPS-) (SD) hyposmia (OR: 1.6), but not with
VRF
Positive relationship between
UPDRS-III
motor score and number of
TREND cohort [58] Cross-sectional NA 698 64 Motor symptoms
non-motor markers (depression,
questionnaire*
anxiety and probable RBD)
HR: significant higher motor
scores than LR
HR:72.2 MDS-UPDRS-III, HR: more likely to fulfil MPS
PREDICT-PD [7] Cross-sectional NA 74(HR) 111(LR)
(69.0- 75.5) Global impression** criteria
Risk estimates predicted motor
scores
Tremor: the most common motor
marker (RR:7.6 at 10 years, RR: 13.7
8166 (PD) at 5 years before diagnosis)
THIN database [25] Longitudinal Case-control 17 years 75(68–81) Medical records
46755 (AMC) Balance impairment and rigidity
appeared 2-5 years before
diagnosis
Higher motor score (2.7 vs 1.3) and
185 rate of phenoconversion to PD in
PARS cohort [59] Longitudinal cohort 8 years 66.6 (SD 5.7) UPDRS-III
(hyposmic) subjects with abnormal dopamine
transporter scan
TREND: Tübinger evaluation of Risk factors for Early detection of NeuroDegeneration, THIN: The UK Health Improvement Network,
PARS: Parkinson Associated Risk Syndrome, NA: not-applicable, AMC: age-matched controls, MPS: mild parkinsonian signs, HR: higher risk (above the 15th
centile of risk estimates), LR: lower risk (below the 85th centile), SD: standard deviation, OR: odds ratio, RR: relative risk, VRF: vascular risk factors,
RBD: REM-sleep behaviour disorder,
* Motor questionnaire: sialorrhea, hypophonia, micrographia, slowing of fine hand movements, arm swing reduction, dysarthria, and rest tremor,
**Global impression scale: 0—normal, 1—unspecific minor abnormality, 2—subtle signs associated with PD, 3—possible early PD, 4—probable PD
with a doubling of the risk of PD.5 In analyses
using data from the UK Health Improvement
Network (THIN) database, 8166 PD patients
were compared with 46455 healthy controls,
and revealed that tremor was the most
common and earliest motor marker reported
in primary care with a subsequent diagnosis
of PD up to ten years later.25 Essential tremor,
which increases in prevalence and severity
with age, might account for some of the
tremor which precedes a diagnosis of PD.
Epidemiological studies support this idea and
find that essential tremor can be associated
with PD, mild cognitive impairment (MCI) and
dementia.26
Rigidity
lack of normal facial responsiveness are char- hands and a short intermission followed by Cogwheel rigidity is a distinctive feature of
acteristic features of hypomimia, which are a re-emergent postural tremor, may also be PD.23 In the study undertaken using the THIN
often described as early motor signs of PD.20 evident at the early stages of PD.23 Numerous database (see above), rigidity and shoulder
Unlike spontaneous blinking, rapid voluntary studies support the idea that tremor in general pain were features that were apparent two
blinking, has been poorly studied in PD, but a is an early feature of PD. For example, a years before PD diagnosis.25 Moreover, rigidity
recent study suggested that it might be an early longitudinal study conducted in central Spain and changes in posture were the most preva-
marker.21 showed that after three-years of follow-up, lent signs in a group of elderly people with
people with ‘essential tremor’ had four times MPS studied by Louis and colleagues, with 24%
Tremor more likelihood of being diagnosed with PD of subjects presenting with isolated rigidity.27
A self-limiting, stress-induced bout of tremor than those without tremor.24 Similar results These results may explain the weighting of
can be the first symptom of PD.22 In the were found in another longitudinal study, with rigidity in MPS criteria defined by the same
absence of tremor at rest, the outstretching of isolated action and rest tremor associated authors, with five out of ten items being related
8 > ACNR > VOLUME 20 NUMBER 3 > 2021clinical review article
to rigidity. However, rigidity is not always easy The motor continuum from natural ageing stage of PD.42 On the other hand, MPS can
to detect. It may manifest through non-specific to neurodegeneration be found in elderly people with SN neuronal
symptoms such as shoulder pain, stiffness, and Parkinsonian signs are common in the elderly. loss and without LB. Ross and collaborators
postural abnormalities when resting or walking. The prevalence of MPS in population-based examined the brains of participants in the
To date there is a lack of tools to objectively studies ranges from 30 to 40% in elderly people Honolulu Heart Program/Honolulu-Asia Ageing
assess rigidity beyond traditional clinical exam- which is much higher than the prevalence of Study (HHP/HAAS). They estimated the density
ination. PD.27 For example, in one study in a community of neurons in the SN in PD cases, individuals
setting, MPS were found in more than one with incidental LB, and elderly people without
Posture and Gait third of individuals over the age of 65 years.28 either condition.43 They found that brains from
The prevalence of gait abnormalities This suggests that MPS cannot be exclusively older individuals without LB but who had MPS
increases with age, but some patterns have considered part of the prodromal spectrum of were associated with lower neuron density in
been shown to be more PD-specific.28 On PD and they may evolve into other conditions the dorsomedial and dorsolateral quadrants of
examination, a classic early parkinsonism with a common denominator of nigrostriatal SN, in contrast to ventrolateral portion of SN
posture when walking includes reduced arm dysfunction. Numerous studies, which were which is seen in PD and incidental LB.
swing, with a flexed elbow and a hand summarised in a review published by Louis et
held in a flexed-adducted position. Kinnier al, have demonstrated that there is an appre- Analogy with ‘Mild Cognitive Impairment’
Wilson was one of the first authors to ciable increase in the incidence of Alzheimer’s The concept of MCI was created to identify
introduce the concept of motor symptoms disease (AD) in people with MPS.3 In one study, individuals who might be in the prodromal
preceding clinical diagnosis. He described a third of patients with AD were found to have stages of AD and other types of dementia. The
that when seated or standing, patients may parkinsonism, which in turn was associated identification of MPS provides similar oppor-
maintain the same position without making with the presence of neurofibrillary tangles tunities for early detection, but also pitfalls. MCI
the normal adjustments which one sees in in the substantia nigra.36 On the other hand, and MPS can occur simultaneously in the same
healthy people (Kinnier Wilson, Neurology; MPS may barely progress over time. This obser- person, increasing the chance of developing a
Volume II, 1940). Using wearable technology vation was made in one longitudinal cohort neurodegenerative disorder. As with MCI, clin-
for objective gait analysis, Mirelman and where one quarter of individuals with MPS ical subtypes of MPS could indicate a variety of
colleagues found that arm swing asymmetry remained stable.37 Based on the multiple trajec- different underlying parkinsonian disorders.44
and loss of limb coordination appeared to be tories that MPS can have, it seems reasonable Unlike MCI, clinical scales including patient’s
less associated with ageing and more likely to to focus our attention on distinguishing which subjective impression about their functional
occur in early PD.29 individuals with MPS will continue to age impairment are more difficult to use in PD due
Postural instability, so long considered normally and which may be in the early stages to lack of awareness of motor disability usually
the fourth cardinal sign in the Queen Square of PD or dementia. seen in PD patients.45 MPS and MCI also share
Brain Bank Criteria, was excluded from the The boundaries between normal ageing, MPS in common associations with chronic cerebro-
Movement Disorders Society Criteria for PD and pathological nigrostriatal degeneration are vascular disease. The role that cardiovascular
that were published in 2015.30 This was mainly difficult to determine. Clinical examination risk factors play in brain health is unques-
because early postural instability should make may reveal clues to define these boundaries; a tionable.46 What is noteworthy, however, is
clinicians consider the possibility of an atypical non-progressive course, symmetric distribution, increasing evidence of a direct relationship
parkinsonian disorder. and slowness with a lack of decrement, are between cardiovascular risk factors and AD.47
It is not surprising that gait patterns, as an all motor features of ageing.3 Axial signs can The study of the interplay between cardio-
automated and rhythmic task, may yield clear predominate in older people with MPS and are vascular disease and the pathology of common
indications of MPS. These include the emer- usually less responsive to L-dopa in patients neurodegenerative diseases is an important
gence of step-to-step variability, arm swing with PD.38 Several studies have specifically area, given that some of these interactions are
asymmetry and reduced truncal rotation.31 At assessed the relative risk of MPS for subsequent potentially modifiable.
the early stages of PD, when compensatory diagnosis of PD and, in one example, MPS at
mechanisms may be present, dual-tasking baseline had a relative risk of 5.5 (2.4–12.6) for Methods of assessing motor dysfunction
during walking is a strategy to make MPS more incident PD over 10 years of follow-up.39 One particular challenge is the development
prominent.32,33 Walking during simple and chal- Minn Aye and colleagues recently evaluated of tests to detect subtle motor abnormalities,
lenging conditions was evaluated in a cohort of the presence of MPS in an elderly community.40 because the heterogeneity of the motor pheno-
696 healthy controls followed up between 2009 They found that one quarter of the group had type makes it difficult to standardise methods of
and 2016. It was found that step-to-step time subtle movement abnormalities and this propor- analysis.4 There is no protocol of motor assess-
variability and gait asymmetry were the best tion increased with age, with three out of ten ment that is well adapted to early stages of
parameters preceding PD diagnosis up to four people older than 75 showing some degree of PD. Standardised approaches, adapting current
years.33 These results were in line with a longi- motor dysfunction. After adjusting for age and clinical scales and creating objective tools,
tudinal study in RBD patients using UPDRS and gender, cognitive dysfunction and symptoms are required to set the boundaries between
the Timed Up and Go test showing that gait of RBD were found to be associated with MPS, prodromal and established PD.48
abnormalities were present between 4-6 years which suggests that in a proportion there may
prior to the diagnosis of an overt parkinsonian be an underlying neurodegenerative process.40 Clinical scales
disorder.34 Although MPS are prevalent in elderly The Movement Disorders Society (MDS)-Unified
The contribution of cerebrovascular disease people, the underlying neuropathology remains Parkinson’s Disease Rating Scale (UPDRS) is a
to MPS in the ageing population has been unclear. The loss of pigmented neurons in the standard means of assessment in PD.49 The
studied. For example, brain autopsies were substantia nigra (SN) pars compacta together motor part (part III) is a semi-quantitative scale
examined from 418 donors in the Religious with the presence of Lewy bodies (LB) are based on integer scoring on simple motor tasks
Order Study cohort who had been evaluated the hallmarks of PD. However, post-mortem addressed to evaluate the cardinal signs of PD.
during life for parkinsonian signs.35 Macroscopic studies have shown that Lewy body pathology Of note, it was designed for established PD, so
infarcts were associated with higher global is not exclusive to PD and have been found it is not expected to be sensitive to detect MPS
parkinsonian scores. In particular, subcortical incidentally in 2-61% of healthy brain donors.41 at the early stages.4
infarcts (macroscopic infarcts and multiple Fearnley and Lees found that individuals with The two most widely accepted criteria for
microinfarcts) were related to gait impair- incidental LB had an intermediate SN neuronal defining subthreshold parkinsonism were
ment. These associations did not change after loss between PD cases and controls, and postu- published by Louis and colleagues, and Berg
adjusting for the presence of dementia. lated that they might represent a preclinical and colleagues on behalf an MDS Task Force.27,49
ACNR > VOLUME 20 NUMBER 3 > 2021 > 9clinical review article
The former was based on binary scoring (present REFERENCES
or absent) of ten items assessing facial expres-
sion, speech, tremor at rest, rigidity, posture and 1. Mahlknecht P, Seppi K, Poewe W. The Concept of 23. Goetz CG. The History of Parkinson’s Disease: Early
axial bradykinesia, but not limb bradykinesia Prodromal Parkinson’s Disease. J Parkinsons Dis. Clinical Descriptions and Neurological Therapies. Cold
(which is necessary for PD diagnosis). MPS were 2015;5:681-97. https://doi.org/10.3233/JPD-150685 Spring Harb Perspect Med. 2011;1:a008862:1-15.
2. Gibb WRG, Lees AJ. The relevance of the Lewy body https://doi.org/10.1101/cshperspect.a008862
defined when any of the following conditions
to the pathogenesis of idiopathic Parkinson’s disease. J 24. Benito-León J, Louis ED, Bermejo-Pareja F. Risk of inci-
were met: rating ≥ 1 for one rigidity item (neck, Neurol Neurosurg Psychiatry. 1988;745-52. https://doi. dent Parkinson’s disease and parkinsonism in essential
right and left arm and leg) AND axial bradykin- org/10.1136/jnnp.51.6.745 tremor: A population based study. J Neurol Neurosurg
esia AND at least 1 of the four remaining 3. Louis ED, Bennett DA. Mild Parkinsonian signs: Psychiatry. 2009;80:423-5. https://doi.org/10.1136/
An overview of an emerging concept. Mov Disord jnnp.2008.147223
items.50 Of note, the Louis definition did not
2007;22:1681-8. https://doi.org/10.1002/mds.21433 25. Schrag A, Horsfall L, Walters K, et al. Prediagnostic
include appendicular bradykinesia. Since limb
4. Maetzler W, Hausdorff JM. Motor signs in the prodromal presentations of Parkinson’s disease in primary care: A
bradykinesia almost certainly belongs to the phase of Parkinson’s disease. Mov Disord. 2012;27:627- case-control study. Lancet Neurol 2015;14:57-64. https://
spectrum of MPS and, in fact may be essen- 33. https://doi.org/10.1002/mds.24973 doi.org/10.1016/S1474-4422(14)70287-X
tial to detect early forms of neurodegenerative 5. Alarcón F, Maldonado JC, Cañizares M, et al. Motor 26. Louis ED. The roles of age and aging in essential tremor:
parkinsonism, several groups have gone back Dysfunction as a Prodrome of Parkinson’s Disease. J An epidemiological perspective. Neuroepidemiology.
Parkinsons Dis. 2020;1-7. 2019;52:111-8. https://doi.org/10.1159/000492831
to integrate the full MDS-UPDRS into the Louis
6. Postuma RB, Iranzo A, Hu M, et al. Risk and predictors of 27. Louis ED, Luchsinger JA, Tang MX, et al. Parkinsonian
criteria for identifying MPS.7,51,52 The MDS Task dementia and parkinsonism in idiopathic REM sleep behav- signs in older people: Prevalence and associations with
Force definition requires exceeding a cut-off of 6 iour disorder: A multicentre study. Brain 2019;142:744- smoking and coffee. Neurology 2003;61:24-8. https://doi.
on the MDS-UPDRS part III, without the inclusion 59. https://doi.org/10.1093/brain/awz030 org/10.1212/01.WNL.0000072330.07328.D6
of kinetic and postural tremor, to be defined as 7. Noyce AJ, Schrag A, Masters JM, et al. Subtle motor 28. Bennett DA, Beckett LA, Murray AM, et al. Prevalence
disturbances in PREDICT-PD participants. J Neurol of Parkinsonian Signs and Associated Mortality in
subthreshold parkinsonism.49 Neurosurg Psychiatry. 2017;88:212-7. https://doi. a Community Population of Older People. N Engl
There exists a modified bradykinesia scale org/10.1136/jnnp-2016-314524 J Med. 1996;334:71-6. https://doi.org/10.1056/
which separately scores three kinetic param- 8. Jennings D, Siderowf A, Stern M, et al. Conversion NEJM199601113340202
to Parkinson Disease in the PARS Hyposmic and 29. Mirelman A, Bernad-Elazari H, Nobel T, et al. Effects of
eters (frequency, rhythm, and amplitude) for
Dopamine Transporter-Deficit Prodromal Cohort. JAMA aging on arm swing during gait: The role of gait speed
each repetitive movement evaluated in the Neurol 2017;74:933. https://doi.org/10.1001/jaman- and dual tasking. PLoS One 2015;10:1-11. https://doi.
MDS-UPDRS-III (finger tapping, prono-supin- eurol.2017.0985 org/10.1371/journal.pone.0136043
ation and opening-closing hand).53 However 9. Louis ED, Tang MX, Mayeux R. Factor structure of 30. Postuma RB, Berg D, Stern M, et al. MDS clinical
Parkinsonian sings in the community-dwelling elderly.
even with these modifications, there are addi- diagnostic criteria for Parkinson’s disease. Mov Disord.
Mov Disord. 2004;19:268-72. https://doi.org/10.1002/ 2015;30:1591-601. https://doi.org/10.1002/mds.26424
tional important features such as manual mds.20013
31. Mirelman A, Bonato P, Camicioli R, et al. Gait impair-
dexterity, posture and gait under challenging 10. Bennett DA, Shannon KM, Beckett LA, et al. ments in Parkinson’s disease. Lancet Neurol 2019;18:697-
conditions that are not captured. Dimensionality of Parkinsonian signs in aging and 708. https://doi.org/10.1016/S1474-4422(19)30044-4
Alzheimer’s disease. Journals Gerontol – Ser A Biol
Sci Med Sci. 1999;54. https://doi.org/10.1093/ 32. Maetzler W, Mancini M, Liepelt-Scarfone I, et al.
Technology-based tools gerona/54.4.M191 Impaired trunk stability in individuals at high risk for
Quantitative motor assessments together Parkinson’s disease. PLoS One 2012;7. https://doi.
11. Hughes AJ, Daniel SE, Blankson S, et al. A
org/10.1371/journal.pone.0032240
with sophisticated software analysis have Clinicopathologic Study of 100 Cases of Parkinson’s
Disease. Arch Neurol 1993;50:140-8. https://doi. 33. Del Din S, Elshehabi M, Galna B, et al. Gait analysis
been created to address the limitations of with wearables predicts conversion to parkinson disease.
org/10.1001/archneur.1993.00540020018011
conventional clinical scales mentioned 12. Bologna M, Paparella G, Fasano A, et al. Evolving
Ann Neurol. 2019;86:357-67. https://doi.org/10.1002/
above. Although technology-based tools allow ana.25548
concepts on bradykinesia. Brain. Published Online First:
objective detection of subtle motor abnor- 2019. https://doi.org/10.1093/brain/awz344 34. Postuma RB, Lang AE, Gagnon JF, et al. How does
parkinsonism start? Prodromal parkinsonism motor
malities, clinical expertise remains equally 13. Nandhagopal R, Kuramoto L, Schulzer M, et al.
Longitudinal evolution of compensatory changes in stri- changes in idiopathic REM sleep behaviour disorder. Brain
important to avoid results misinterpretation.54 atal dopamine processing in Parkinson’s disease. Brain. 2012;135:1860-70. https://doi.org/10.1093/brain/
The range of technology available has 2011;134:3290-8. https://doi.org/10.1093/brain/awr233 aws093
grown exponentially in the last decade. The 14. Letanneux A, Danna J, Velay JL, et al. From micro- 35. Buchman AS, Leurgans SE, Nag S, et al. Cerebrovascular
graphia to Parkinson’s disease dysgraphia. Mov Disord. disease pathology and parkinsonian signs in old age.
kinds of devices range from body sensors to Stroke. 2011;42:3183-9. https://doi.org/10.1161/
2014;29:1467-75. https://doi.org/10.1002/mds.25990
smartphone applications but have also been STROKEAHA.111.623462
15. Rosenblum S, Samuel M, Zlotnik S, et al. Handwriting
expanded from controlled conditions meas- as an objective tool for Parkinson’s disease diagnosis. J 36. Liu Y, Stern Y, Chun MR, et al. Pathological correlates
ured in the laboratory to real life monitoring in Neurol. 2013;260:2357-61. https://doi.org/10.1007/ of extrapyramidal signs in Alzheimer’s disease. Ann
s00415-013-6996-x Neurol. 1997;41:368-74. https://doi.org/10.1002/
the home-environment.
ana.410410312
An important question is whether the 16. Mclennan JE, Nakano K, Tyler HR, et al. Micrographia in
Parkinson’s Disease. J Neurol Sci. 1972;141-52. https:// 37. Wilson RS, Schneider JA, Beckett LA, et al. Progression of
existing scales ought to be the gold standard doi.org/10.1016/0022-510X(72)90002-0 gait disorder and rigidity and risk of death in older persons.
of assessment for MPS or whether there is a 17. Darley FL, Brown JR, Swenson WM. Language
Neurology. 2002;58:1815-9. https://doi.org/10.1212/
need to create new signatures of early motor WNL.58.12.1815
changes after neurosurgery for Parkinsonism. Brain
dysfunction in PD, with an increasing reliance Lang. 1975;2:65-9. https://doi.org/10.1016/S0093- 38. Newman RP, LeWitt PA, Jaffe M, et al. Motor function
934X(75)80054-X in the normal aging population: treatment with levodopa.
on objective measures.55 Neurology. 1985;35:571-3. https://doi.org/10.1212/
18. Arora S, Baig F, Lo C, et al. Smartphone motor testing
to distinguish idiopathic REM sleep behavior disorder, WNL.35.4.571
Conclusions controls, and PD. Neurology 2018;91:E1528-38. https:// 39. Mahlknecht P, Stockner H, Marini K, et al. Midbrain
MPS are an important aspect of the prodromal doi.org/10.1212/WNL.0000000000006366 hyperechogenicity, hyposmia, mild parkinsonian signs
19. Harel B, Cannizzaro M, Snyder PJ. Variability in and risk for incident Parkinson’s disease over 10 years:
phase of PD. There are many unanswered ques- A prospective population-based study. Park Relat
fundamental frequency during speech in prodromal and
tions about where the boundary lies between incipient Parkinson’s disease: A longitudinal case study. Disord. 2020;70:51-4. https://doi.org/10.1016/j.
the ageing process and nigrostriatal degenera- Brain Cogn. 2004;56:24-9. https://doi.org/10.1016/j. parkreldis.2019.12.008
tion, their progression to early PD or dementia, bandc.2004.05.002 40. Aye YM, Liew GM, Ng SYE, et al. Mild Parkinsonian Signs
20. Karson CN. Spontaneous eye-blink rates and dopamin- in a Community Ambulant Population. J Parkinsons Dis.
and the time over which MPS emerge and the 2020;1-7. https://doi.org/10.3233/JPD-191849
ergic systems. Brain. 1983;106:643-53. https://doi.
best means to quantify early motor dysfunction. org/10.1093/brain/106.3.643 41. Zaccai J, Brayne C, McKeith I, et al. Patterns and stages of
The creation of a motor battery that combines 21. Agostino R, Bologna M, Dinapoli L, et al. Voluntary, α-synucleinopathy: Relevance in a population-based cohort.
a variety of motor assessments under chal- spontaneous, and reflex blinking in Parkinson’s disease. Neurology 2008;70:1042-8. https://doi.org/10.1212/01.
Mov Disord. 2008;23:669-75. https://doi.org/10.1002/ wnl.0000306697.48738.b6
lenging conditions, incorporating technology
mds.21887 42. Fearnley JM, Lees AJ. Ageing and Parkinson’s Disease:
and clinical acumen, is needed and should be
22. Djamshidian A, Lees AJ. Can stress trigger Parkinson’s Substantia Nigra Regional Selectvity. Brain, A J Neurol.
evaluated on a large scale in population-based disease? J Neurol Neurosurg Psychiatry. 2014;85:879-82. 1991;114:2283-301. https://doi.org/10.1093/
studies involving elderly people. https://doi.org/10.1136/jnnp-2013-305911 brain/114.5.2283
10 > ACNR > VOLUME 20 NUMBER 3 > 2021You can also read