ACRA CORE COMPONENTS OF CVD SECONDARY PREVENTION AND CARDIAC REHABILITATION - STEPHEN WOODRUFFE, ACRA PRESIDENT 2013
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ACRA CORE COMPONENTS OF
CVD SECONDARY PREVENTION
AND CARDIAC REHABILITATION
STEPHEN WOODRUFFE, ACRA PRESIDENT 2013-
2015
AUSTRALIAN GUIDELINES
1999 2004
INTERNATIONAL GUIDELINES 2013 2012 2009

Cardiovascular Disease vs

OUR LEADERS IN THE BATTLE AGAINST THE
DARK MAGIC OF CVD
Tom Briffa Sue Sanderson Jenny Finan
Kim Gray Cate Ferry
Robyn Clark Lis Neubeck Steve Woodruffe
http://geekologie.com/2013/09/harry-potter-character-myers-briggs-pers.php
Steve Woodruffe
AEP
Cate Ferry
NHF
Lis Neubeck
PhD
Kim Gray
Physio
Tom Briffa Robyn Clark Jenny Finan Sue Sanderson
PhD PhD MN NP
TIMELINE OF DOCUMENT DEVELOPMENT November 2013 - Idea conceptualised during ACRA EMC meeting 2 December 2013 - Writing group formed 20 December 2013 - Initial Teleconference Jan – Feb 2014 - Writing group summarised evidence 4 March 2014 - Second teleconference – r/v evidence summary 25 March 2014 - Development of initial table of core components 1 April 2014 - Third teleconference – revision of core components April 2014 - Section leads developed content May 2015 - SW compiled content into working draft June 2014 - Revision by whole writing group

TIMELINE OF DOCUMENT DEVELOPMENT July 2014 - Invitation received to submit paper to HL&C July – August 2014 - Iterative final revisions by LN, SW August 2014 - Meeting of writing group to confirm final draft plans 5 September 2014 - Submitted to HL&C October 2014 - Initial feedback received, revisions required November 2014 - Revisions completed 4 December 2014 - Revised document submitted to HL&C 8 December 2014 - Accepted by HL&C for publication in 2015 19 January 2015 - Published online ahead of print May 2015 - Published in print

DEFINING OUR QUEST
• The coordinated sum of activities required to
influence favourably the underlying cause of
cardiovascular disease, as well as to provide
the best possible physical, mental and social
conditions, so that the patients may, by their
own efforts, preserve or resume optimal
functioning in their community and through
improved health behaviour, slow or reverse
progression of disease
WHO, 1993Referral and access to services
Referral and access to services All eligible patients to be offered referral to a CR service which best suits their individual needs, as soon as possible after diagnosis or discharge from hospital including a referral to a general practitioner for long term care. • Ensure eligibility • Specific considerations in relation to Aboriginal and Torres Strait Islander peoples • Systems of referral and recruitment • Models of service delivery • Expertise and qualifications of the multidisciplinary team
Referral and access to services
Assessment and short-term
monitoringAssessment and short-term
monitoring
All eligible patients to receive an individualised initial
assessment that includes physical, psychological and
social parameters with referral on to appropriate
services based on patient needs; followed by ongoing
review, discharge assessment process and follow-up.
• Detailed initial assessment
• Structured ongoing review, discharge and follow-up
process
• Inclusion of the familyReferral and access to services
Recovery and longer
Assessment and short-term
term
monitoring
maintenanceRecovery and longer
term
maintenance
CR services should facilitate patients to return to, or to
improve on, baseline functioning, including employment-
where applicable, driving, resumption of sexual activity,
and other activities of daily living and maintain life-long.
When the cardiac condition or other co-morbidities
preclude this, the CR service should focus on maximising
potential and providing coping strategies.
• Return to normal functioning
• Exercise programming recommendations
• Long-term managementReferral and access to services
Recovery and longer
Assessment and short-term
term
monitoring
maintenance
Lifestyle/behavioural modification and medication adherenceLifestyle/behavioural modification and medication adherence CR services should be tailored to provide education and skill development to motivate and enable patients to self-care and make changes in their lifestyle, to address multiple cardiovascular risk factors, and to ensure adherence to prescribed medications.
WHAT ARE WE
BATTLING AGAINST?
Poor nutrition
Inactivity OSA
CVD
Depression/
Anxiety
Smoking Obesity
Alcohol/Illicit drugsOUR MAGICAL WEAPONS
• The therapeutic alliance
• Medications
• Smoking cessation strategies including NRT
• Incidental physical activity as well as structured
exercise programs
• Diet and nutritional strategies
• Weight management strategies
• Dyslipidemia/Hypertension/Diabetes management
• Mental health screening and treatment
• CPAP treatment for OSA
• Alcohol consumption reduction/cessation
strategies/support
• Illicit drug use cessation strategies/support
• Action plansReferral and access to services
Recovery and longer
Assessment and short-term
term
monitoring
maintenance
Lifestyle/behavioural modification and medication adherence
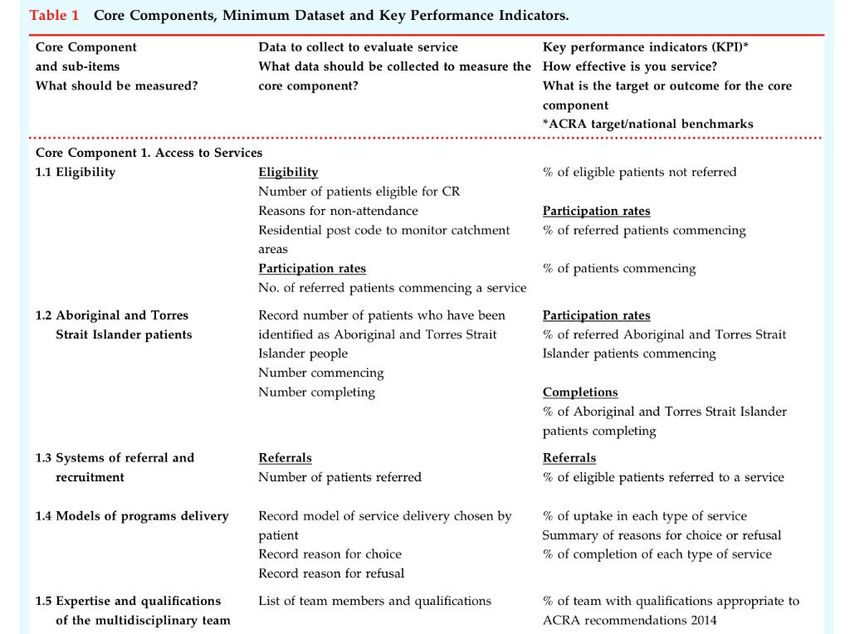
Evaluation and quality improvementEvaluation and quality improvement All CR services must collect a minimum set of data and report on key performance indicators to ensure continuous quality improvement of services and benchmarking. • Minimum data to collect • Key performance indicators • Audit TABLE 1.
WHERE TO NOW FOR OUR HEROES? • Clinicians should use the core components paper to guide effective service delivery and promote high quality evidence based care. • Directors of hospitals and health services should use these core components to aid decision making about the development and maintenance of these services.
THE FUTURE??? • Expanded core components web-based document • Collaboration with like minded groups e.g. CSANZ, NHF, SPA
S T E V E . W O O D R U F F E @ H E A LT H . Q L D . G O V. A U
You can also read