ACTIVITY DISCLAIMER - Juvenile Arthritis - Aafp
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Juvenile Arthritis
Sarah Merrill, MD
ACTIVITY DISCLAIMER
The material presented here is being made available by the American Academy of Family
Physicians for educational purposes only. Please note that medical information is constantly
changing; the information contained in this activity was accurate at the time of publication. This
material is not intended to represent the only, nor necessarily best, methods or procedures
appropriate for the medical situations discussed. Rather, it is intended to present an approach,
view, statement, or opinion of the faculty, which may be helpful to others who face similar
situations.
The AAFP disclaims any and all liability for injury or other damages resulting to any individual
using this material and for all claims that might arise out of the use of the techniques
demonstrated therein by such individuals, whether these claims shall be asserted by a
physician or any other person. Physicians may care to check specific details such as drug
doses and contraindications, etc., in standard sources prior to clinical application. This material
might contain recommendations/guidelines developed by other organizations. Please note that
although these guidelines might be included, this does not necessarily imply the endorsement
by the AAFP.
1
DISCLOSURE
It is the policy of the AAFP that all individuals in a position to control content disclose
any relationships with commercial interests upon nomination/invitation of
participation. Disclosure documents are reviewed for potential conflict of interest
(COI), and if identified, conflicts are resolved prior to confirmation of participation.
Only those participants who had no conflict of interest or who agreed to an identified
resolution process prior to their participation were involved in this CME activity.
All individuals in a position to control content for this session have indicated they have
no relevant financial relationships to disclose.
The content of my material/presentation in this CME activity will not include
discussion of unapproved or investigational uses of products or devices.
Sarah Merrill, MD
Assistant Professor, Department of Family Medicine and Public Health, University of California, San Diego
School of Medicine
Dr. Merrill is a board-certified family physician who specializes in sports medicine. In addition to diagnosing
and treating injuries associated with athletics, she provides primary care for patients of all ages, including
preventive care and treatment of acute and chronic diseases. An avid yoga practitioner and certified yoga
instructor, she has a special interest in rehabilitating individuals who have yoga injuries. She also enjoys
performing ultrasound-guided diagnostics and procedures. Recently, she published two chapters in the
clinical reference text The 5-Minute Sports Medicine Consult, 3rd Edition.
Dr. Merrill instructs students, residents, and fellows at UC San Diego School of Medicine, is an assistant
program director for the UCSD Family Medicine Residency Program, and is the medical director of UC San
Diego Health’s Scripps Ranch Family Medicine Center. She also provides care throughout the San Diego
community and for many sporting events, serving as the team physician for the University City High School
and Scripps Ranch High School football teams; medical director for the California State Games; medical team
captain for San Diego Rock ‘n’ Roll Marathon; and event physician for the BMX World Championships. Dr.
Merrill completed a sports medicine fellowship at UC San Diego School of Medicine, where she also
completed a residency in family medicine with an additional certification in integrative medicine. She earned
her medical degree from Loyola University Chicago Stritch School of Medicine in Illinois. She is a member of
numerous professional associations, including the American Medical Society for Sports Medicine (AMSSM),
the American Medical Association (AMA), and the AAFP.
2
Learning Objectives
1. Describe diagnostic principles, appropriate pre-referral
evaluation, and red flags in pediatric rheumatologic
diseases.
2. Discuss treatment options, including side effects of
common medications and what contraindications to
immunizations exist for patients in active treatment.
3. Define the subtypes of Juvenile Idiopathic Arthritis
(formerly Juvenile Rheumatoid Arthritis) and identify
common signs and symptoms of each subtype.
Audience Engagement System
Step 1 Step 2 Step 3
3
Juvenile Arthritis: Definition
• Variety of autoimmune
and inflammatory
diseases that affect the
joints of children 18 years
and younger3
Pathogenesis
• Genetic and environmental
factors3, 4
• Stress
• Trauma
• Gut microbiome
• History of infections4
4
Juvenile Idiopathic Arthritis
• “Group of inflammatory
disorders that begins before
the 18th birthday and persists
for at least 6 weeks with other
known conditions excluded”13
Juvenile Idiopathic Arthritis: Categories
JIA
Enthesitis/spondylitis
Systemic JIA RF+ JIA Early onset ANA+ JIA Other JIA Unclassified JIA
related JIA
5
Systemic JIA
Fever of unknown origin for > 3 days and recurring for at
least 2 weeks
Major criteria: erythematous rash and/or arthritis
Minor criteria: generalized LAD/hepatomegaly/splenomegaly, serositis; arthralgia
without arthritis; leukocytosis with neutrophila
Need fever + 2 major or 1 major and 2 minor
Systemic JIA
• Leukocytosis, hypochromic microcytic
anemia, thrombocytosis, elevated acute
phase reactants4,13
• ANA and RF negative4,13
6
Systemic JIA
• Salmon colored rash on
trunk and proximal
extremities
• Can be polyarticular in
both small or large joints
Poll Question #1
Which of the following is not required for the
diagnosis of systemic juvenile idiopathic arthritis?
A. +ANA
B. Fever of unknown origin
C. Arthralgia
D. A and C
E. A and B
7
+Rheumatoid Factor JIA
• Arthritis > 6 weeks and 2 +RF
tests or +CCP13
+Rheumatoid Factor JIA
• Worst prognosis
• Female predominance
• Late onset
• Symmetric and progressive
• Predominantly affects wrists and small
joints hands and feet13
8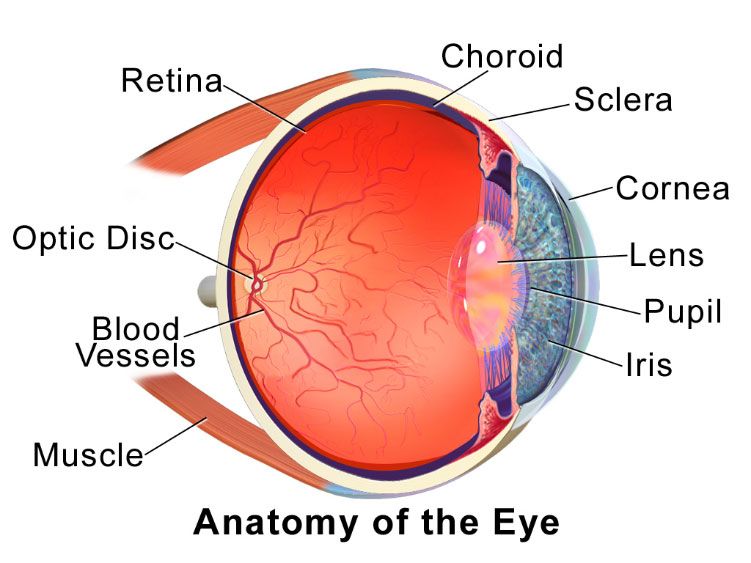
Enthesitis/spondylitis-related JIA
Arthritis or enthesitis + >/=3
Peripheral arthritis and Athritis or enthesitis + two of
months of inflammatory back
enthesitis the following
pain and sacroiliitis on xrays
• SIJ TTP
• Inflammatory back pain
• +HLA‐B27 antigen
• Acute symptomatic anterior
uveitis
• H/o SpA in 1st degree
relative
Early onset ANA+ JIA
Two +ANA at least 3
Early onset (< 6
Arthritis >/= 6 weeks months apart (titer >
years)
1/160)
9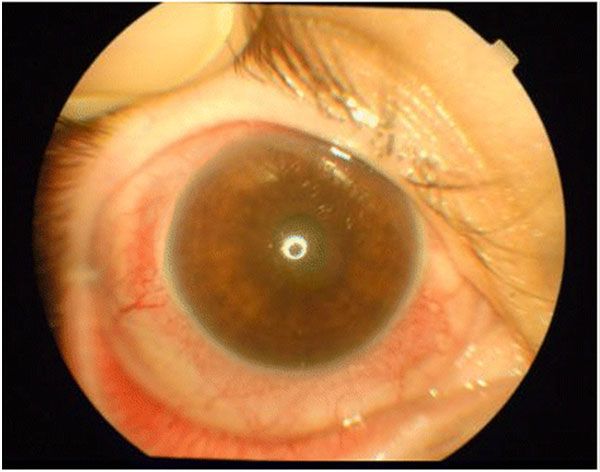
Other JIA
• Arthritis > 6 weeks
• Does not fit criteria for previous categories
Unclassified JIA
• Arthritis > 6 weeks
• Fits > 1 previous disorder
10Poll Question #2
A 13 year female with a 8 week history of joint pain
and swelling in bilateral wrist and toes would most
likely have the following lab values?
A. -ANA
B. -RF and -ANA
C. +RF and +CCP
D. +HLA-B27
E. Type O blood
Work Up
• No antibody panels unless positive ANA
and evidence of rheum disease!2
• Initial lab testing: ANA, CBC, RF, ESR and
CRP1
• Initial imaging: MRI or ultrasound
preferred8
11Complications
• Uveitis
Complications
• Increased risk of developing
CVD4,11
• Increased systolic and diastolic
pressures11
• Increased aortic stiffness11
12Complications
• Sleep and psychosocial factors
Complications
• Growth retardation
• Macrophage activation syndrome
• Multi-organ insufficiency
• Osteoporosis
13Treatment
• Involves multidisciplinary team4, 9
– PCP
– Pediatric rheumatologic
– Ophthalmologist
– Pediatric psychiatrist
– Physical therapist
– Sports med/ortho
Treatment
• NSAIDs
• DMARDs
• Corticosteroids
• Biologics
14Treatment
• Monitor pain, sleep and psychosocial
indicators for both parents and patients6
Prognosis
• FHx disease, early ankle or hip joint
involvement, erosions on xray and higher
number of joints affected are poor
prognostic indicators4, 8
• Remission rate increased and rate of joint
damage decreases with early initiation of
treatment4
15Follow Up
• Psychosocial monitoring
• Cardiac screening
• Eye screening
Poll Question 4
You are evaluating a 3 year old female with fever of
unknown origin daily for 2 weeks and joint swelling. You
suspect JIA, although are still waiting on lab results and
imaging. Which is the most appropriate next step?
A. Refer to sports medicine/ortho
B. Discuss patient’s sleep habits with patient
C. Refer to ophthalmology
D. Order EKG
E. Order bone marrow biopsy
16Practice Recommendations
• JIA is a broad diagnosis of exclusion and does not necessarily
require arthritis/arthralgia
• Practitioners need to be aware of presentations in order to start work
ups quickly – better outcomes are associated with early treatment
• Initial lab work should include ANA, RF, CBC, ESR, CRP, HLA-B27
and imaging of affected joints
• Inclusion of multidisciplinary team is key early in diagnosis and
treatment
• Uveitis is the primary extra-articular complication of JIA and needs to
be screened frequently
• NSAIDs and DMARDs are first line therapies
Questions
17Resources
1. Ali Y. Rheumatologic Tests: A Primer for Family Physicians. American family physician. 2018;98(3):164-170.
2. American College of Rheumatolgy. Choosing Wisely: Don’t order antibody panels unless positive antinuclear antibodies (ANA) and evidence of rheumatic disease.
Choosing Wisely https://www.aafp.org/afp/recommendations/viewRecommendation.htm?recommendationId=151. Accessed June 2019.
3. Arthritis Foundation. Pediatric Rheumatic Diseases: What are Pediatric Rheumatic Diseases? 2018; https://www.arthritis.org/about-arthritis/types/pediatric-rheumatic-
diseases. Accessed June, 2019.
4. Barut, et al. Juvenile Idiopathic Arthritis. Balkan Med J. 2017 Mar, 34(2): 90-101.
5. Beukelman T, Patkar NM, Saag KG, et al. 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and
safety monitoring of therapeutic agents for the treatment of arthritis and systemic features. Arthritis care & research. 2011;63(4):465-482.
6. Bromberg MH, Gil KM, Schanberg LE. Daily sleep quality and mood as predictors of pain in children with juvenile polyarticular arthritis. Health psychology : official
journal of the Division of Health Psychology, American Psychological Association. 2012;31(2):202-209.
7. Cassidy J, Kivlin J, Lindsley C, Nocton J. Ophthalmologic Examinations in Children With Juvenile Rheumatoid Arthritis. Pediatrics. 2006;117(5):1843-1845.
8. Cellucci T, Guzman J, Petty RE, et al. Management of Juvenile Idiopathic Arthritis 2015: A Position Statement from the Pediatric Committee of the Canadian
Rheumatology Association. The Journal of rheumatology. 2016;43(10):1773-1776.
9. Chausset A, Gominon AL, Montmaneix N, et al. Why we need a process on breaking news of Juvenile Idiopathic Arthritis: a mixed methods study. Pediatric
rheumatology online journal. 2016;14(1):31.
10. Clark, Sarah, et al. Juvenile idiopathic arthritis-associated uveitis. Pediatri Rheumatol Online J. 2016; 14:27.
11. Coulson, Elizabeth, et al. Cardiovascular risk in juvenile idiopathic arthritis. Rheumatology, Vol 52: 7. 07/2013: 1163-1171.
12. Hersh AO, Salimian PK, Weitzman ER. Using Patient-Reported Outcome Measures to Capture the Patient's Voice in Research and Care of Juvenile Idiopathic
Arthritis. Rheumatic diseases clinics of North America. 2016;42(2):333-346.
13. Martini, et al. Toward new classification criteria for juvenile idiopathic arthritis: first steps, pediatric rheumatology international trials organization international
consensus. Journal of Rheumatology 2019, 46:2.
14. Ringold S, Weiss PF, Beukelman T, et al. 2013 update of the 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic
arthritis: recommendations for the medical therapy of children with systemic juvenile idiopathic arthritis and tuberculosis screening among children receiving biologic
medications. Arthritis and rheumatism. 2013;65(10):2499-2512.
15. Seid M, Huang B, Niehaus S, Brunner HI, Lovell DJ. Determinants of health-related quality of life in children newly diagnosed with Juvenile Idiopathic Arthritis. Arthritis
care & research. 2014;66(2):263-269.
16. CME Training Session Needs Survey. In. Leawood KS: AAFP, 2016.
17. Rodriguez-Garcia A. The importance of an ophthalmologic evaluation in patients with juvenile idiopathic arthritis. Reumatologia clinica. 2015; 11(3):133-138.
18. Junnila JL, Cartwright VW. Chronic musculoskeletal pain in children: part II. Rheumatic causes. American family physicians. 2006; 74 (2): 293-300.
19. Garcia-Carrasco M et al. Efficacy of thalomide in systemic onset juvenile rheumatoid arthritis. Joint Bone Spine 2017; 75(2): 500-503. Available
https://doi.org/10.1016/j.jbspin.2006.12.004
Contact Information
Sarah Merrill, MD
UC San Diego Health Systems
semerrill@ucsd.edu
18You can also read