Addressing Myths and Vaccine Hesitancy: A Randomized Trial
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Addressing Myths and Vaccine
Hesitancy: A Randomized Trial
Maryke S. Steffens, PhD,a Adam G. Dunn, PhD,b Mathew D. Marques, PhD,c Margie Danchin, PhD,d,e
Holly O. Witteman, PhD,f Julie Leask, PhDg
OBJECTIVES:Evidence on repeating vaccination misinformation or "myths" in debunking text is abstract
inconclusive; repeating myths may unintentionally increase agreement with myths or help
discredit myths. In this study we aimed to compare the effect of repeating vaccination myths
and other text-based debunking strategies on parents’ agreement with myths and their
intention to vaccinate their children.
METHODS: For this online experiment we recruited 788 parents of children aged 0 to 5 years;
454 (58%) completed the study. We compared 3 text-based debunking strategies (repeating
myths, posing questions, or making factual statements) and a control. We measured changes
in agreement with myths and intention to vaccinate immediately after the intervention and at
least 1 week later. The primary analysis compared the change in agreement with vaccination
myths from baseline, between groups, at each time point after the intervention.
RESULTS:There was no evidence that repeating myths increased agreement with myths
compared with the other debunking strategies or the control. Posing questions significantly
decreased agreement with myths immediately after the intervention compared with the
control (difference: 0.30 points, 99.17% confidence interval: 0.58 to 0.02, P 5 .004,
d 5 0.39). There was no evidence of a difference between other debunking strategies or the
control at either time point, or on intention to vaccinate.
CONCLUSIONS:Debunking strategies that repeat vaccination myths do not appear to be inferior to
strategies that do not repeat myths.
Full article can be found online at www.pediatrics.org/cgi/doi/10.1542/peds.2020-049304
a
Centre for Health Informatics, Australian Institute of Health Innovation, Macquarie University, Sydney,
Australia; bBiomedical Informatics and Digital Health, School of Medical Sciences, Faculty of Medicine and Health, WHAT’S KNOWN ON THIS SUBJECT: Vaccination
The University of Sydney, Sydney, Australia; cSchool of Psychology and Public Health, Department of Psychology and misinformation may fuel hesitancy and refusal and factor
Counselling, La Trobe University, Melbourne, Australia; dVaccine Uptake Research Group, Murdoch Children’s
in vaccine-preventable disease outbreaks. Evidence on
Research Institute, Melbourne, Australia; eDepartment of Paediatrics, The University of Melbourne, Melbourne,
Australia; fDepartment of Family and Emergency Medicine, Faculty of Medicine, Laval University, Quebec, Canada;
repeating vaccination misinformation or “myths” in
and gSusan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, The University of Sydney, debunking text is inconclusive; repeating myths may
Sydney, Australia unintentionally increase agreement with myths or help
discredit myths.
Dr Steffens performed the literature search, developed the study design and protocol,
conducted the statistical analysis and interpretation of the data, developed the figures and WHAT THIS STUDY ADDS: This online experiment was
tables, drafted the initial manuscript, and reviewed and revised the manuscript; Drs Dunn, conducted in parents of children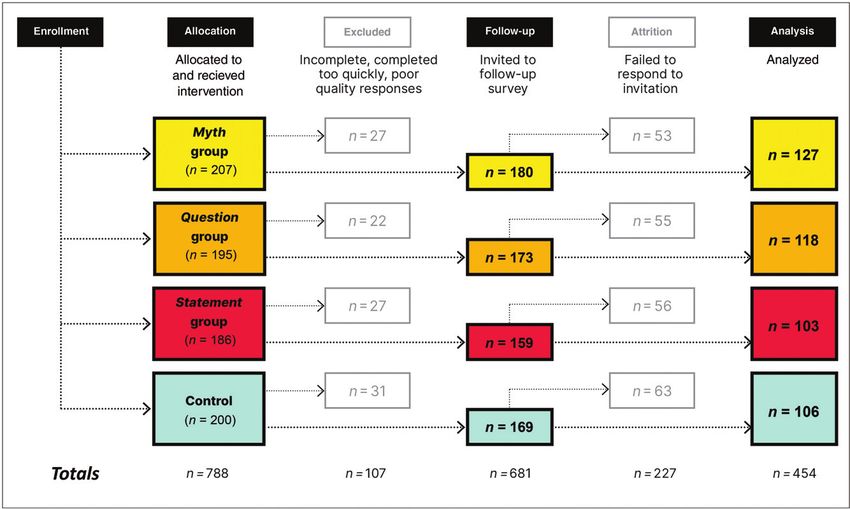
Childhood vaccination raises examples of misinformation or Participants were parents of
questions and concerns for 40% of “myths” before debunking them. children aged 0 to 5 years. Eligible
parents in Australia.1 In addition to With this strategy, myths are often participants were 18 years or older,
practical barriers to vaccination, presented as headings, followed by residing in Australia, and competent
vaccine concerns among parents can corrective, evidence-based text.14,15 at reading and responding in
lower childhood vaccination rates Reviews of evidence and some English. Participants gave written
and are associated with outbreaks of recent studies, however, suggest this informed consent. The Macquarie
measles and pertussis.2,3 Vaccine approach may be flawed: repeating University Human Research Ethics
misinformation (information not a myth may backfire by rendering it Committee granted ethics approval
supported by evidence) can memorable and thus likely to be (ref. 5201954658790).
exacerbate parental concerns: recalled as true on the basis of
shared in social networks or spread recall and familiarity, a phenomenon Procedure
by those seeking to oppose known as familiarity bias.16–19 Research company Quality Online
vaccination,4,5 misinformation may Hence, recommendations for Research recruited participants from
reduce confidence in vaccination by debunking misinformation have its accredited online panel, the
increasing perceptions of risk.6,7 emphasized providing factual representativeness of which is
Misinformation provides an information over repeating myths to obtained by using quota controls
underpinning for misperceptions avoid triggering familiarity backfire according to Australian Bureau of
such as vaccines overwhelming effects.20 Authors of a recent review, Statistics Census data. The company
children’s immune systems and the however, have questioned whether recruited participants between
dangers of giving too many vaccines backfire effects reliably occur,21 September 16 and October 30, 2019,
too early, the preference for natural while other research has failed to inviting them via e-mail or survey
rather than vaccine-induced reveal evidence that repeating technology and offering between
immunity, and the association of myths is counterproductive.22–25 A$1.00 and A$3.00 as incentive for
vaccines with autism.1,8 The literature on debunking participation. The company stopped
vaccination misinformation is recruitment when predetermined
Countering misinformation is key to
limited. This gap in evidence is targets were achieved.
avoiding negative effects on
important to address, especially in
vaccination attitudes.9 Parents of
view of the deployment of At baseline, participants responded
young children are at high risk of
coronavirus disease of 2019 (COVID- to myth agreement, intention to
misinformation exposure10 and are
19) vaccines, which are subject to a vaccinate, and vaccine confidence
important targets for interventions
range of claims made by opponents items (see Materials for definitions).
to counter misinformation.
of vaccination. Participants were randomly
Encouragingly, parents indicate
assigned to receive 1 of 3 debunking
receptiveness to trusted sources
With this study, we sought to assist interventions or a control text.
that address their concerns and
health communicators addressing Immediately after the intervention,
provide accurate, evidenced-based
misinformation about childhood participants responded to myth
information.11 Global health
vaccination with evidence on the agreement and intention to
agencies, like the World Health
effectiveness of various debunking vaccinate items again. Participants
Organization and United Nations
strategies. The aim of this study was were also asked to provide
Children’s Fund (UNICEF), health
to compare how different text-based demographic information. For
care providers, other advocates of
vaccination, and the media all play a debunking strategies affect parents’ quality control, participants were
key role in addressing agreement with vaccination myths asked to summarize the intervention
misinformation, especially in online and their intention to vaccinate their text in a free-response text box.
settings, where it is most easily children. After 1 week, participants were
spread.12 invited to complete a follow-up
METHODS survey responding to myth
Commonly used strategies to agreement and intention to
address misinformation, however,
Participants vaccinate items. They had up to 3
have been shown to have adverse This was a prospective online weeks to respond. At the close of
rather than positive effects in parent experiment testing a communication study, participants were given a
populations.13 One frequently used intervention aimed at reducing debriefing statement with credible
strategy to counter misinformation agreement with vaccination myths information correcting vaccination
is to prominently repeat specific in parents of young children. myths used in the intervention.
Downloaded from www.aappublications.org/news by guest on October 23, 2021
2 STEFFENS et al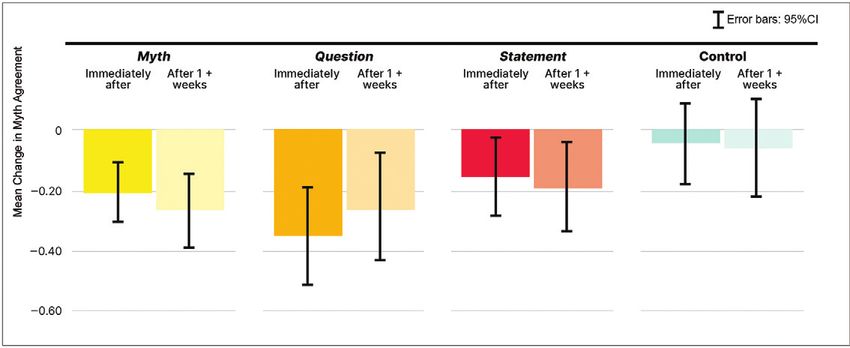
The study aimed to recruit 452 were included in the analysis (Fig 1). vaccinate at baseline. Participants
participants to ensure a sample size Of the 454 participants included, 63% who did not complete the follow-up
of 376 participants (with an were female (284 of 454), 56% (255 survey were more likely to be
expected 17% loss to follow-up), of 454) were aged between 30 and female (x2 5 9.91, P 5 .007) and
calculated to allow detection of an 39 years, 60% (272 of 454) had a have a lower vaccine confidence
effect size of d 5 0.5 when household income of $80 0001 per score at baseline (P 5 .046, Cohen’s
comparing change in myth year, and 61% (275 of 454) had d 5 0.15). There was no evidence of
agreement (primary outcome) university qualifications. a difference in myth agreement or
between groups (see Supplemental intention to vaccinate at baseline
Information for sample size Mean response time between baseline between participants who did and
calculations). This study was and follow-up survey was 16 (SD 5 did not complete the follow-up
powered at 80% to be confirmatory 5.55) days. Of the 788 randomly survey. There was no significant
for the primary outcome. assigned participants, 14% (107 of difference in attrition across
Participants with incomplete 788) were excluded because of their intervention groups (x2[N 5 681,
surveys or poor-quality free poor-quality responses, while 29% df 53] 5 2.85, P 5 .42).
responses (off-topic, unclear, (227 of 788) failed to respond to the
unanswered) or who responded too invitation to complete a follow-up Materials
quickly (determined a priori by the survey; this attrition was higher than
Intervention
research company as per their the expected 17%. There was no
quality control measures) were significant difference in exclusion Participants were asked to read a
excluded by the research company. across intervention groups (x2[N 5 short piece of text (350 words)
788, df 53] 5 1.70, P 5 .64). debunking 3 vaccination myths. The
Of the 788 parents of children aged 0 3 myths were “It’s better for
to 5 years who consented and were Attrition analysis compared sex and children to develop immunity from
randomly assigned, 454 (58%) measures of vaccine confidence, diseases”; “It’s safer to vaccinate
completed the follow-up survey and myth agreement, and intention to babies and young children when
FIGURE 1
Flow diagram revealing progress of participants through the online experiment.
PEDIATRICS Volume 148, number 5, Downloaded
November 2021
from www.aappublications.org/news by guest on October 23, 2021 3they are older”; and “Vaccines text with a similar length and 1 5 strongly disagree, 5 5 strongly
overwhelm a baby's immune structure about parenting strategies. agree; a 5 .85) and were averaged
system.” The text was modified from Survey software required to create a vaccine confidence score.
a resource addressing common participants to view this page for a
vaccine misperceptions developed to minimum of 30 seconds (see Data Analysis
support health care providers’ Supplemental Information for full
The primary outcome measure was
consultations with parents.26 intervention texts).
the change in myth agreement,
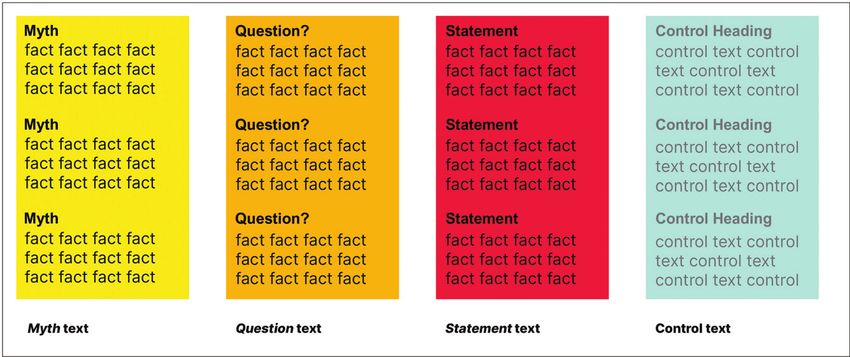
Each intervention (myth, question, Survey Items calculated as the difference from
or statement) used a different baseline at each time point after the
Myth agreement was assessed with
debunking strategy to counter the intervention. The primary analysis
3 items, by using a 5-point scale
compared mean change in myth
myths. The myth intervention (1 5 strongly disagree, 5 5 strongly
repeated the vaccination myths agreement between groups, at each
agree). The responses to each of the
(“Myth: Vaccines overwhelm a time point after the intervention.
3 individual vaccination myths
baby’s immune system”) in the For this analysis, independent
described above were averaged to
headings before providing corrective samples t tests were used, adjusted
create a myth agreement score,
text. The question intervention which revealed high internal for multiple comparisons between
posed questions (“Can vaccines consistency at baseline (a 5 .84), groups with Bonferroni correction
overwhelm a baby’s immune immediately after the intervention (P < .0083; confidence intervals
system?”) in the headings before (a 5 .85), and 11 weeks after the [CIs] of 99.17%). Cohen’s d was
providing corrective text. The intervention (a 5 .84). Intention to calculated to describe the magnitude
statement intervention made factual vaccinate was assessed with a single of intervention effects.30
statements (“A baby’s immune item, by using a 0 to 100 scale Observational within-group changes
system to able to respond to a (0 5 definitely not, 100 5 defini- in myth agreement from baseline
vaccine and fight germs at the same tely). Myth agreement and intention were also analyzed by using
time”) in the headings before to vaccinate items were consistent repeated measures analysis of
providing corrective text. The with survey questions used in stu- variance (ANOVA). The findings of
corrective text was the same for dies with similar parent popula- the difference-in-difference analyses
each intervention (Fig 2); only the tions.8,27 Vaccine confidence was were confirmed with a repeated
headings differed between measured by using the 4-item short measures analysis of covariance
interventions. Participants in the form of the Vaccine Confidence Scale (ANCOVA ) (see Supplemental
control group were given unrelated (benefits factor)28,29 (5-point scale, Information).
FIGURE 2
Intervention texts, comprising 3 vaccination myths, followed by corrective text.
Downloaded from www.aappublications.org/news by guest on October 23, 2021
4 STEFFENS et alA secondary outcome measure was Preregistration 99.17% CI: 0.58 to 0.02, P 5 .004,
the change in intention to vaccinate, The study aims and hypotheses, Cohen’s d 5 0.39). We found no clear
calculated as the difference from methods, and data analysis plan evidence of a difference between
baseline at each time point after the were preregistered with the Open change in myth agreement between
intervention. Changes between Science Framework (https://osf.io/ the control and other groups or
groups were compared by using jthn2). A minor variation to the pre- between the groups themselves: there
independent samples t tests. registration was to analyze myth was no evidence of differences
Observational within-group changes agreement as a composite score, between any other groups at this time
from baseline were analyzed by point or at 11 weeks after the
with the aim of presenting simple
using repeated measures ANOVAs. intervention. This includes the myth
and straightforward results in the
All analyses were conducted by group, which did not increase myth
article. An analysis of change in
using SPSS (version 25; IBM SPSS agreement compared with the other
myth agreement for each individual
Statistics, IBM Corporation). groups or the control at any time
myth is retained in the Supplemen-
point (see Table 3). There was no
Subgroup Analysis tal Information.
evidence of a difference between
A prespecified subgroup analysis groups in intention to vaccinate at any
included data from 217 moderate- RESULTS
time point. The results of the repeated
low vaccine confidence participants At baseline, mean myth agreement measures ANCOVA aligned with those
only (48%; 217 of 454). Participants scores were between neutral (3) and of the difference-in-difference analyses
were categorized as moderate-low slightly disagree (2) (see Table 1). (see Supplemental Information).
vaccine confidence if their vaccine Within-group observational changes
confidence score measured at in myth agreement, both imme- Comparing changes in myth
baseline (5 point scale, 1 5 strongly diately after the intervention and agreement between groups for each
disagree, 5 5 strongly agree) was 11 weeks after the intervention, are myth individually indicated differences
#4.38. High vaccine confidence shown in Table 2 and Fig 3. between myths. For the “Vaccines
participants (score >4.38) (52%; overwhelm immune systems” myth,
237 of 454) were excluded. These The primary analysis compared the the question and myth groups showed
categories are based on results of a change in myth agreement from a significant decrease in myth
previous study in parents of young baseline, between groups, at each time agreement of a medium size
children, in which a score of #4.38 point after the intervention. The compared with the control (difference
(converted from a score by using an results of this analysis are shown in between question and control: 0.45
11 point scale) was associated with Table 3. The null hypothesis for points, 99.17% CI: 0.81 to 0.09,
delay of any vaccine.29 Mean comparing change in myth agreement P 5 .001, Cohen’s d 5 0.45; difference
changes in myth agreement and between posing questions and control between myth and control: 0.31
intention to vaccinate were immediately after the intervention points, 99.17% CI: 0.59 to 0.03, P
compared between groups, at each was rejected: compared with the 5 .004, Cohen’s d 5 0.38). There
time point after the intervention. control group, the question group were no significant differences
Independent samples t tests were showed a significant decrease in between groups for the “Disease-
used for this analysis, adjusting for agreement with vaccination myths of acquired immunity is better” myth or
multiple comparisons between a medium effect size immediately the “Delaying vaccines is safer” myth
groups with Bonferroni correction after the intervention (difference (see Supplemental Table 6 for full
(P < .0083). between groups: 0.30 points, results of analysis per myth).
TABLE 1 Vaccination-Specific Characteristics of Participants by Intervention Group at Baseline, Immediately After the Intervention and 11 Week After
the Intervention
Myth Agreement,a Mean Score (SD) Intention to Vaccinate,b Mean Score (SD)
Vaccine Confidence,c Mean
Baseline Immediately After 11 wk After Baseline Immediately After 11 wk After Score (SD), Baseline
All (n 5 454) 2.39 (1.06) 2.20 (1.04) 2.19 (1.02) 92.00 (15.26) 92.29 (15.94) 91.90 (16.06) 4.33 (0.65)
Myth (n 5 127) 2.41 (1.00) 2.20 (1.03) 2.14 (1.00) 92.61 (12.58) 92.81 (14.82) 91.76 (15.80) 4.32 (0.63)
Question (n 5 118) 2.37 (1.18) 2.03 (1.08) 2.12 (0.96) 93.23 (14.28) 93.57 (13.17) 91.88 (16.76) 4.37 (0.69)
Statement (n 5 103) 2.36 (1.07) 2.20 (1.03) 2.17 (1.00) 88.91 (19.67) 90.74 (17.66) 90.99 (16.50) 4.34 (0.70)
Control (n 5 106) 2.42 (0.97) 2.38 (1.02) 2.36 (1.12) 92.89 (14.12) 91.75 (18.19) 92.99 (15.28) 4.30 (0.60)
a
Five-point scale, 1 5 strongly disagree, 5 5 strongly agree; higher scores indicate more agreement with vaccination myths.
b
Scale of 0–100, 0 5 definitely not, 100 5 definitely; higher scores indicate stronger intention to vaccinate.
c
Five-point scale, 1 5 strongly disagree, 5 5 strongly agree; higher scores indicate more positive beliefs about vaccination.
PEDIATRICS Volume 148, number 5, Downloaded
November 2021
from www.aappublications.org/news by guest on October 23, 2021 5TABLE 2 Within-Group Observational Mean Change in Myth Agreement and Intention to Vaccinate From Baseline, Immediately After the Intervention
and 11 Week After the Intervention
Immediately After the Intervention 11 wk After the Intervention
M Diff (SD) df, Error F P np2 M Diff (SD) df, Error F P np2
a
Change in myth agreement from baseline
Myth 0.20 (0.87) 1, 126 17.18TABLE 3 Comparing Mean Change in Myth Agreement and Intention to Vaccinate Between Groups
Immediately After the Intervention 11 wk After the Intervention
99.17% CI 99.17% CI
M Diff t (df) P Lower Upper M Diff t (df) P Lower Upper
Comparing change in myth agreement from baseline
Myth versus question 0.15 1.579 (243) .116 0.10 0.39 0.01 0.101 (243) .920 0.30 0.28
Myth versus statement 0.05 0.593 (228) .554 0.26 0.16 0.08 0.812 (228) .418 0.33 0.18
Myth versus control 0.16 1.954 (231) .052 0.37 0.06 0.21 2.058 (231) .041 0.47 0.06
Question versus statement 0.19 1.846 (219) .066 0.47 0.09 0.07 0.565 (219) .572 0.38 0.25
Question versus control 0.30* 2.884 (222) .004 0.58 0.02 0.19 1.606 (222) .110 0.52 0.13
Statement versus control 0.11 1.207 (207) .229 0.36 0.13 0.13 1.181 (207) .239 0.42 0.16
Comparing change in intention to vaccinate from baseline
Myth versus question 0.14 0.127 (243) .899 3.12 2.84 0.49 0.270 (243) .787 4.33 5.31
Myth versus statement 1.63 1.139 (228) .256 5.44 2.18 2.94 1.371 (228) .172 8.64 2.76
Myth versus control 1.34 0.934 (231) .351 2.48 5.15 0.96 0.629 (231) .530 5.03 3.11
Question versus statement 1.49 1.168 (219) .244 4.88 1.90 3.43 1.522 (219) .129 9.42 2.57
Question versus control 1.48 1.154 (222) .250 1.94 4.90 1.45 0.892 (222) .373 5.78 2.88
Statement versus control 2.97 1.836 (207) .068 1.34 7.27 1.97 0.985 (207) .326 3.37 7.31
df, degree of freedom; M Diff, mean difference.
*Mean difference significant at the 0.0083 level; 99.17% CI is Bonferroni adjusted.
reduce misinformation effects.31 values related to bodily purity misconceptions.35 Experiments
Research comparing message versus degradation.32 Equally, the with vaccination misinformation
formats for debunking influenza novelty of a myth to an individual specifically would be worthwhile
vaccination misinformation has also may render corrections conducting, as would further
found that accurate knowledge ineffective.33 investigations of the relationship
increases after debunking, between novel vaccine
regardless of the message format, This study has implications for how misinformation and social media
and that repeating misinformation health professionals, global health amplification.
does not inadvertently increase authorities, and other advocates of
inaccurate knowledge.22 Repeating vaccination debunk vaccine This research was conducted in
misinformation with corrective text misinformation in written text. In parents of childrenparticipants’ willingness to accept may improve intentions. Finally, in Further research should elucidate
the debunking information. Although this study, myth agreement was why some myths are more
the sample was intended to be analyzed as a continuous variable. persistent than others and evaluate
representative of the population, Informal analysis of the data as debunking strategies for novel
respondents analyzed were not, categories of agreeing and vaccination myths and those that
which may impact on the external disagreeing parents (not included change behavior.
validity of the findings. Parents’ here) suggests exposing parents to
vaccination intention, rather than vaccination myths without ACKNOWLEDGMENTS
uptake, was measured as an corrective text may increase myth We acknowledge the contributions
outcome. Although in keeping with agreement. This effect is worth of Noel Brewer and Ullrich Ecker in
similar studies, uptake would investigating further in future critiquing and improving this article.
provide a more accurate measure of
research.
vaccination behavior. Furthermore,
no significant findings for parents’
CONCLUSIONS ABBREVIATIONS
vaccination intentions were
observed. Further investigation of In this study, repeating myths as a ANCOVA: analysis of covariance
how parents’ agreement with debunking strategy did not appear CI: confidence interval
vaccination myths is associated with to be inferior to strategies that do COVID-19: coronavirus disease of
intentions and behavior is not. Posing myths as questions may 2019
warranted, as is research into what be an effective debunking strategy
types of debunking interventions when paired with corrective text.
DOI: https://doi.org/10.1542/peds.2020-049304
Accepted for publication Aug 3, 2021
Address correspondence to Maryke S. Steffens, PhD, Australian Institute of Health Innovation, Macquarie University, North Ryde 2113 NSW Australia. E-mail:
maryke.steffens@health.nsw.gov.au
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2021 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by Macquarie University Research Training Program Scholarship 2017438 and National Health and Medical Research Council project
grant APP1128968. The funder/sponsor did not participate in the work.
POTENTIAL CONFLICT OF INTEREST: During the conduct of the study, Dr Steffens reports funding from Macquarie University; Dr Dunn reports grants from the
National Health and Medical Research Council; Dr Leask reports grants from the National Health and Medical Research Council and funding from the World Health
Organization; Dr Witteman reports funding from the Canada Research Chairs program and grants from the Canadian Institutes of Health Research; and Drs Marques
and Dr Danchin have indicated they have no potential conflicts of interest to disclose.
REFERENCES mandatory immunization, and the risks 7. Betsch C, Renkewitz F, Betsch T, Ulsh€ofer
1. Costa-Pinto JC, Willaby HW, Leask J, et al. of vaccine-preventable diseases. N Engl C. The influence of vaccine-critical web-
Parental Immunisation Needs and J Med. 2009;360(19):1981–1988 sites on perceiving vaccination risks. J
Attitudes Survey in paediatric hospital 4. Smith N, Graham T. Mapping the anti- Health Psychol. 2010;15(3):446–455
clinics and community maternal and vaccination movement on Facebook. 8. Chow M, Danchin M, Willaby HW, Pem-
child health centres in Melbourne, Aus- Inf Commun Soc. 2017;22(9): berton S, Leask J. Parental attitudes,
tralia. J Paediatr Child Health. 2018; 1310–1327 beliefs, behaviours and concerns
54(5):522–529 towards childhood vaccinations in Aus-
5. Wang Y, McKee M, Torbica A, Stuckler D.
2. Zimet GD, Rosberger Z, Fisher WA, Perez Systematic literature review on the tralia: a national online survey. Aust
S, Stupiansky NW. Beliefs, behaviors and spread of health-related misinformation Fam Physician. 2017;46(3):145–151
HPV vaccine: Correcting the myths and on social media. Soc Sci Med. 2019;
9. Schmid P, Betsch C. Effective
the misinformation. Prev Med. 2013; 240:112552
strategies for rebutting science
57(5):414–418 6. Larson HJ. The biggest pandemic risk? denialism in public discussions.
3. Omer SB, Salmon DA, Orenstein WA, Viral misinformation. Nature. 2018; Nat Hum Behav. 2019;3(9):
deHart MP, Halsey N. Vaccine refusal, 562(7727):309 931–939
Downloaded from www.aappublications.org/news by guest on October 23, 2021
8 STEFFENS et al10. Royal Society for Public Health. Moving successful debiasing. Psychol Sci Public support intervention. Vaccine.
the needle: promoting vaccination Interest. 2012;13(3):106–131 2018;36(44):6480–6490
uptake across the life course. 2018. 18. Pluviano S, Watt C, Della Sala S. Misin- 27. Wroe AL, Turner N, Owens RG. Evalua-
Available at: https://www.rsph.org.uk/ tion of a decision-making aid for
formation lingers in memory: failure of
uploads/assets/uploaded/f8cf580a-57b5- parents regarding childhood immuniza-
three pro-vaccination strategies. PLoS
41f4-8e21de333af20f32.pdf. Accessed April tions. Health Psychol. 2005;24(6):
One. 2017;12(7):e0181640
20, 2020 539–547
19. Pluviano S, Watt C, Ragazzini G, Della
11. Ames HMR, Glenton C, Lewin S. Parents’ 28. Gilkey MB, Reiter PL, Magnus BE,
Sala S. Parents’ beliefs in misinforma-
and informal caregivers’ views and
tion about vaccines are strengthened McRee AL, Dempsey AF, Brewer NT.
experiences of communication about
by pro-vaccine campaigns. Cogn Pro- Validation of the vaccination confi-
routine childhood vaccination: a synthe-
cess. 2019;20(3):325–331 dence scale: A brief measure to
sis of qualitative evidence. Cochrane
identify parents at risk for refusing
Database Syst Rev. 2017;(2):CD011787 20. Cook J, Lewandowsky S. The debunking
adolescent vaccines. Acad Pediatr.
12. Capurro D, Cole K, Echavarrıa MI, Joe J, handbook. 2011. Available at: http://sks. 2016;16(1):42–49
Neogi T, Turner AM. The use of social to/debunk. Accessed April 20, 2020
29. Gilkey MB, McRee AL, Magnus BE, Reiter
networking sites for public health prac- 21. Swire-Thompson B, DeGutis J, Lazer D. PL, Dempsey AF, Brewer NT. Vaccination
tice and research: a systematic review. Searching for the backfire effect: mea- confidence and parental refusal/delay
J Med Internet Res. 2014;16(3):e79 surement and design considerations. J of early childhood vaccines. PLoS One.
13. Nyhan B, Reifler J, Richey S, Freed GL. Appl Res Mem Cogn. 2020;9(3):286–299 2016;11(7):e0159087
Effective messages in vaccine promo- 22. Cameron KA, Roloff ME, Friesema EM, et 30. Cohen J. A power primer. Psychol Bull.
tion: a randomized trial. Pediatrics. al. Patient knowledge and recall of 1992;112(1):155–159
2014;133(4). Available at: www. health information following exposure
pediatrics.org/cgi/content/full/133/4/ 31. Walter N, Murphy ST. How to unring the
to “facts and myths” message format
e835 bell: a meta-analytic approach to cor-
variations. Patient Educ Couns. 2013;
rection of misinformation. Commun
14. UNICEF. 10 outrageous things you may 92(3):381–387
Monogr. 2018;85(3):423–441
have heard about vaccines. BuzzFeed.
23. Ecker UKH, Hogan JL, Lewandowsky S.
2014. Available at: https://www.buzzfeed. 32. Amin AB, Bednarczyk RA, Ray CE, et al.
Reminders and repetition of misinfor-
com/unicef/10-outrageous-things- Association of moral values with
mation: Helping or hindering its retrac- vaccine hesitancy. Nat Hum Behav.
you-may-have-heard-about-vacc-1ebx.
tion? J Appl Res Mem Cogn. 2017;6(2): 2017;1(12):873–880
Accessed April 20, 2020
185–192
15. Wessel L. Four vaccine myths and 33. Carey JM, Chi V, Flynn DJ, Nyhan B, Zeitzoff
24. Swire B, Ecker UKH, Lewandowsky S. T. The effects of corrective information
where they came from. Science. 2017.
Available at: https://www.sciencemag. The role of familiarity in correcting about disease epidemics and outbreaks:
org/news/2017/04/four-vaccine-myths- inaccurate information. J Exp Psychol evidence from Zika and yellow fever in
and-where-they-came#. Accessed Learn Mem Cogn. 2017;43(12): Brazil. Sci Adv. 2020;6(5):eaaw7449
April 20, 2020 1948–1961
34. Schwarz N, Newman E, Leach W. Making
16. Schwarz N, Sanna LJ, Skurnik I, Yoon C. 25. Ecker UKH, O’Reilly Z, Reid JS, Chang EP. the truth stick and the myths fade: les-
Metacognitive experiences and the intri- The effectiveness of short-format refu- sons from cognitive psychology. Behav
cacies of setting people straight: Impli- tational fact-checks. Br J Psychol. Sci Policy. 2016;2:85–95
cations for debiasing and public 2020;111(1):36–54
35. Ecker UKH, Lewandowsky S, Chadwick
information campaigns . Adv Exp Soc 26. Berry NJ, Danchin M, Trevena L, et al. M. Can corrections spread misinfor-
Psychol. 2007;39:127–161 Sharing knowledge about immunisation mation to new audiences? Testing
17. Lewandowsky S, Ecker UKH, Seifert CM, (SKAI): An exploration of parents’ com- for the elusive familiarity backfire
Schwarz N, Cook J. Misinformation and munication needs to inform develop- effect. Cogn Res Princ Implic. 2020;
its correction: Continued influence and ment of a clinical communication 5(1):41
PEDIATRICS Volume 148, number 5, Downloaded
November 2021
from www.aappublications.org/news by guest on October 23, 2021 9Addressing Myths and Vaccine Hesitancy: A Randomized Trial
Maryke S. Steffens, Adam G. Dunn, Mathew D. Marques, Margie Danchin, Holly O.
Witteman and Julie Leask
Pediatrics originally published online October 11, 2021;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2021/10/08/peds.2
020-049304
References This article cites 29 articles, 1 of which you can access for free at:
http://pediatrics.aappublications.org/content/early/2021/10/08/peds.2
020-049304#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Interpersonal & Communication Skills
http://www.aappublications.org/cgi/collection/interpersonal_-_comm
unication_skills_sub
Vaccine/Immunization
http://www.aappublications.org/cgi/collection/vaccine:immunization
_sub
Public Health
http://www.aappublications.org/cgi/collection/public_health_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on October 23, 2021Addressing Myths and Vaccine Hesitancy: A Randomized Trial
Maryke S. Steffens, Adam G. Dunn, Mathew D. Marques, Margie Danchin, Holly O.
Witteman and Julie Leask
Pediatrics originally published online October 11, 2021;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2021/10/08/peds.2020-049304
Data Supplement at:
http://pediatrics.aappublications.org/content/suppl/2021/10/08/peds.2020-049304.DCSupplemental
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2021
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on October 23, 2021You can also read

















































