Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations - 04 June 2014
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Adrenaline Auto-injectors:
A Review of Clinical and Quality
Considerations
04 June 2014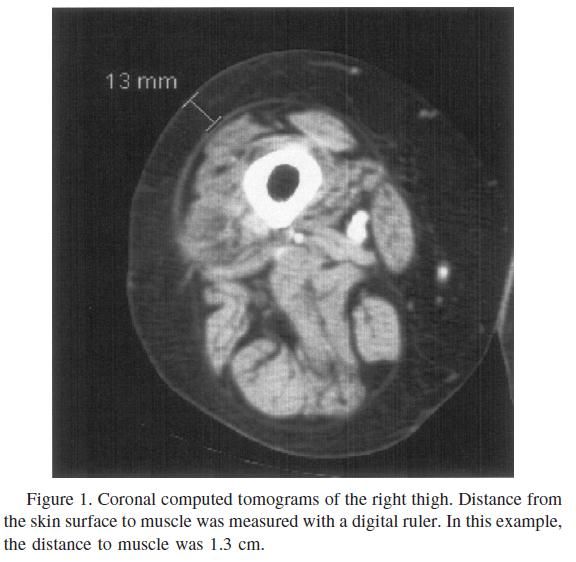
Contents
Abbreviations ....................................................................................................... 3
1 Lay Summary.................................................................................................. 4
2 Introduction .................................................................................................... 6
2.1 Background .............................................................................................. 6
2.1.1 The issues.......................................................................................... 6
2.1.2 History of auto-injectors ...................................................................... 6
2.2 Anaphylaxis.............................................................................................. 8
2.2.1 Incidence and treatment ...................................................................... 8
2.2.2 Pharmacokinetics of adrenaline ............................................................. 9
2.2.3 Doses needed to treat anaphylaxis ...................................................... 10
3 Quality Aspects ............................................................................................. 10
3.1 Drug Substance:- adrenaline .................................................................... 10
3.2 Design and Operating Principle of auto-injectors ......................................... 10
3.3 Finished product specification ................................................................... 12
4 Non-Clinical Evidence ..................................................................................... 14
4.1 Gelatine models ...................................................................................... 14
4.2 Pig models ............................................................................................. 16
4.3 Non-Clinical Conclusion ............................................................................ 16
5 Clinical Evidence ............................................................................................ 17
5.1 Intramuscular vs subcutaneous injection .................................................... 17
5.1.1 Intramuscular versus subcutaneous injection conclusions ...................... 19
5.2 Site of injection ...................................................................................... 19
5.2.1 Conclusion ....................................................................................... 21
5.3 Appropriate needle length ........................................................................ 22
5.3.1 Clinical Comment .............................................................................. 25
5.4 Post-marketing data ................................................................................ 26
5.4.1 Exposure data .................................................................................. 26
5.4.2 Clinical Comment:............................................................................. 28
6 Discussion and recommendations .................................................................... 28
7 Independent Advice Received .......................................................................... 30
References ......................................................................................................... 32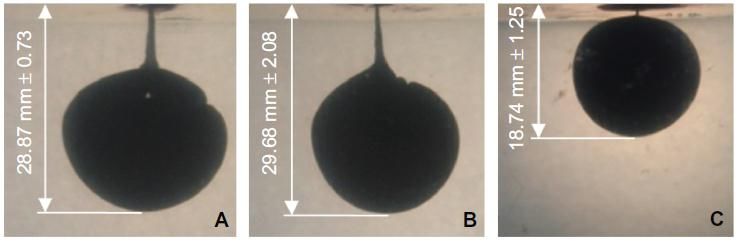
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
Abbreviations
AAI Adrenaline Auto-injector
ADR Adverse Drug Reaction
BP British Pharmacopoeia
BMI Body mass index
Cmax Maximum plasma concentration
CT Computed tomography
DoH Department of Health
EVDAS EudraVigilance Data Analysis System
IM Intramuscular
ISO International Organization for Standardization
MAH Marketing Authorisation Holder
NHS National Health Service
Ph Eur European Pharmacopoeia
PIL Patient Information Leaflet
PK Pharmacokinetic
RMS Reference Member State
SC Subcutaneous
STMD Skin To Muscle Depth
Tmax Time to maximum plasma concentration
3
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
1 Lay Summary
Adrenaline auto-injectors (AAIs) are intended for self-administration of adrenaline
solution as an emergency, on-the-spot treatment during the early onset of symptoms of
an anaphylactic reaction. As the progression of anaphylactic shock can be rapid,
individuals with known allergy profiles are prescribed AAIs to carry with them at all times
and they should be familiar with the operation of their specific auto-injector.
The Medicines and Healthcare products Regulatory Agency (MHRA) has undertaken a
review of all AAIs licensed in the UK on the recommendation of a coroner’s report into a
death of a patient who had used such a device to self-treat anaphylaxis.
This paper mainly discusses two of the issues raised by the coroner:
1. The most effective site for injection and the clarity of instructions
2. The most appropriate auto-injector needle length for injections into the muscle
(intramuscular or IM) rather than injections into the fatty layer under the skin
(subcutaneous or SC) administration
The review has also considered information supplied with these products and whether
clearer instructions and advice to prescribers, patients and carers could be provided in
order to improve outcome.
Anaphylaxis is a severe type of allergic response and is a life-threatening condition that
can escalate into something very serious extremely rapidly. It can be associated with
marked swelling of the face and neck causing constriction of the throat and upper
airway, tightness of the chest and difficulty in breathing, a raised skin rash and
sometimes a marked decline in blood pressure causing collapse of the patient. Known
factors affecting severity of an anaphylactic episode include the degree of exposure to
the substance responsible for the allergic reaction (the “allergen”) and other factors such
as associated poorly controlled asthma, recent illness or strenuous exercise after
exposure to the allergen. Fortunately, fatalities occurring as a result of anaphylaxis are
rare and even less common when AAIs have been used. It is vital however that these
devices are used correctly and an important part of the MHRA review has been to clarify
information provided with these products to ensure as far as possible their correct use.
Anaphylaxis can be fatal and in these unfortunate cases, death usually occurs very soon
after contact with the allergen. Some allergens act faster than others. Food allergens can
cause breathing to stop (respiratory arrest) after approximately 30–35 minutes; insect
stings can cause collapse from shock after 10–15 minutes; and allergic reactions to
medicines given by injection can cause death within 5 minutes. Therefore the speed of
treatment of an anaphylactic reaction is of great importance and can have a significant
impact on the patient’s recovery.
It is widely accepted that an injection into the muscle is the best way for treatment with
adrenaline to be administered. Even if the injection does not reach into the muscle, it will
still have some effect, but it may take longer to relieve the symptoms of anaphylaxis.
The best place for the injection is considered to be the side of the thigh in the middle
between the hip and the knee, as recommended in the Resuscitation Council Guidelines.
This review considered the data regarding all possible injection sites and concluded that
patients should continue to use the middle of the thigh, as this represented the best
location and minimised the risk of the needle going too deep and hitting bone or
accidentally injecting adrenaline into a blood vessel or tendon which could cause
additional problems.
As everyone has different body shapes, concerns were raised about the length of the
needle within the actual auto-injector devices and whether or not these were long
enough to inject adrenaline into the muscle of all patients needing treatment for
anaphylaxis. It is difficult to study how deep the needle goes into the thighs of patients
using these devices. Models using blocks of gelatine and pork tissue have been used to
represent the thigh and measure how far the adrenaline travels after being propelled
from an auto-injector device following injection. The pork tissue model is considered
more like the human thigh than the gelatine model but both models provide some data
4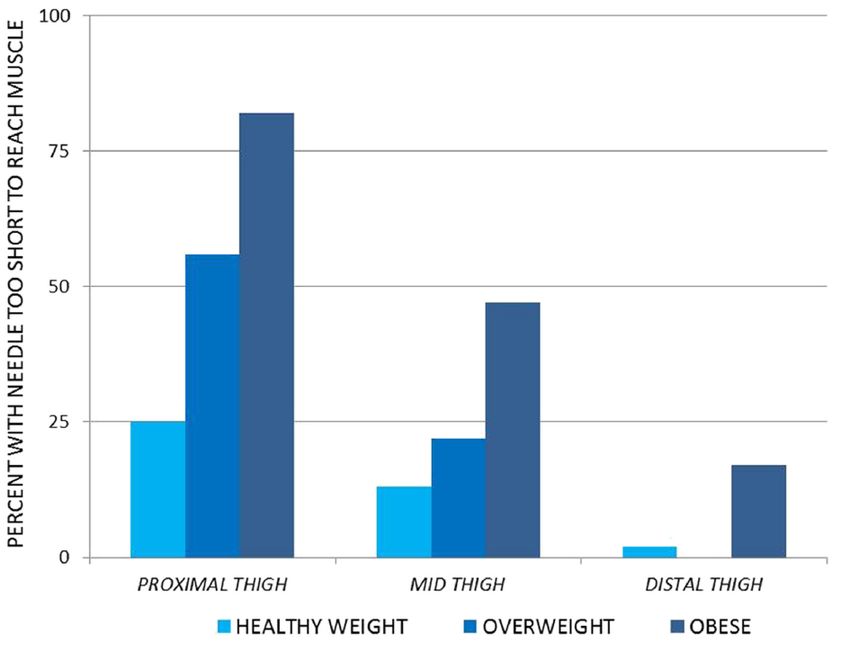
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
that shows that the spring-loaded auto-injectors can project the adrenaline beyond the
end of the needle to as much as twice the depth that the needle penetrates. However,
not all of the pork tissue studies confirm this. Furthermore, the models cannot fully
mirror the real-life situation where other factors exist including local tissue blood flow
and barriers such as fibrous tissue layers surrounding muscle, all of which may have an
impact on how efficiently the adrenaline can penetrate into the muscle tissue.
Two studies19,20 measured the skin to muscle distance in adults and in children and
showed that the skin to muscle depth is greater than the length of the needle (15mm) in
many people, particularly women due to a different distribution of fat from men. These
studies also showed that Body Mass Index (BMI) and skin to muscle depth are not
directly linked and people with low BMI may have still have thighs with a high skin to
muscle depth.
The AAI devices are spring loaded and the manufacturers claim that the adrenaline is
injected forcibly into the muscle tissue. This is supported by non-human studies which
provide some reassurance that the adrenaline does penetrate beyond the exposed
needle length. However, as outlined above, there are additional factors that may
influence how well the adrenaline penetrates.
The MHRA’s report was presented to and evaluated by independent panels of experts
(Commission on Human Medicines (CHM) and the Chemistry, Pharmacy and Standards
Expert Advisory Group) in January 2014 and a number of recommendations were made.
The experts advised on improvements to the information for healthcare professionals
and patients on the management of an anaphylaxis episode, they proposed that
manufacturers should conduct studies to evaluate injection delivery and should improve
the quality standards for AAIs. The full list of recommendations made is provided in this
report. The recommendations are currently being taken forward by the MHRA for
consideration at a European level. This will enable the different AAIs authorised across
Europe to benefit from this review.
5
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
2 Introduction
2.1 Background
2.1.1 The issues
Adrenaline auto-injectors (AAIs) are intended for self-administration of adrenaline
solution as an emergency, on-the-spot treatment during the early onset symptoms of
anaphylaxis. As the progression of anaphylactic shock can be rapid, individuals with
severe allergies are prescribed AAIs to carry with them at all times and they should be
familiar with the operation of their specific brand of auto-injector.
A coroner’s report raised four areas for consideration and investigation in relation to the
death of a patient following use of an AAI for emergency treatment of an anaphylactic
episode.
The four areas were:
1. The need to contact emergency services after first use of auto-injector even if
symptoms are abating
2. The most effective site for injection and clarity of instructions
3. The most appropriate auto-injector needle length for IM injection
rather than SC administration
4. The best position for transporting a patient following an anaphylactic event
The MHRA was asked to address the first three items. Item 1 was addressed by the
MHRA during 2012. All marketing authorisation holders (MAHs) were required to clearly
state in the Patient Information Leaflet (PIL) and/or labelling of all AAIs licensed in the
UK that the patient should call 999 even if symptoms appeared to be abating.
Although the review did not specifically address Item 4, it did consider whether
improvements could be made to the information supplied by the manufacturers of these
products, relating to instructions to be followed by the patient/carer and healthcare
professionals at the scene of the emergency, as well as advice for follow-up.
Therefore the scope of this paper is primarily to address items 2 and 3.
In order to help with this review the MAHs for EpiPen (Meda Pharmaceuticals Ltd), Jext
(Alk-Abello A/S) and Emerade (Namtall AB) were asked to provide:
(a) Evidence that a complete dose of adrenaline solution is delivered intra-
muscularly throughout the proposed shelf life of the product
(b) Evidence that the above can be delivered through clothing
(c) Any post-marketing clinical evidence that the product (adrenaline plus device)
is effective in the treatment of acute anaphylaxis
(d) A summary of out of specification (OOS) results from stability studies
conducted on all product strengths over the past three years
(e) Product complaints history (reported by either patients or healthcare
professionals).
2.1.2 History of auto-injectors
Auto-injectors were developed in the 1960s for military use following research between
the American military and NASA. The original objective was to develop a self-injecting
device that would inject atropine, the antidote for nerve agents in biological weapons.
From this original design platform the AAI was developed and was introduced into the
medical field approximately 25 years ago in the United States of America.
The first marketing authorisation in Europe was for EpiPen® which was granted a
Marketing Authorisation in Germany in 1989 and in the UK in March 1996.
Subsequently other brands of AAIs were licensed: Anapen®, Jext® and most recently
6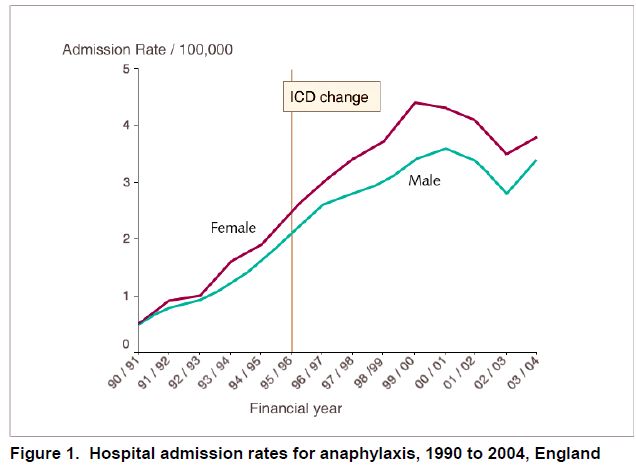
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
Emerade®. Anapen® is no longer marketed in the UK but is still available in other EU
countries.
Scope of review
Currently the following AAIs are licensed in the UK for use in adults and children and
were included in the review:
Table 1: Licensed AAIs
Product name Container Product licence Marketing
closure number/Type Authorisation Holder’s
detail of licence name and address
EpiPen® Pre-filled PL 15142/0245
Adrenaline cartridge
(Epinephrine) encased in
Auto-Injector an auto-
0.3mg injector MEDA Pharmaceuticals
Limited, Skyway House
Parsonage Road
Takeley, Bishop’s
Stortford, CM22 6PU
EpiPen® Jr. PL 15142/0246
United Kingdom
Adrenaline
(Epinephrine)
Auto-Injector
0.15mg
Jext 150 Pre-filled PL 10085/0052
micrograms cartridge
solution for enclosed in
ALK-Abelló A/S
injection in pre- an auto-
filled pen injector Bøge Allé 6-8
Jext 300 PL 10085/0053 DK-2970 Hørsholm
micrograms Sweden
solution for
injection in pre-
filled pen
Emerade 150 Pre-filled PL 42457/0001
micrograms, syringe
solution for encased in
injection in pre- an auto-
filled pen injector
Emerade 300 PL 42457/0002
micrograms, European NAMTALL AB
solution for Rapsgatan 7, SE-754 50
injection in pre- Uppsala, Sweden
filled pen
Emerade 500 PL 42457/0003
micrograms, European
solution for
injection in pre-
filled pen
No new clinical studies were required to be submitted in support of the original
applications.
7Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
2.2 Anaphylaxis
2.2.1 Incidence and treatment
Anaphylaxis is a severe, life-threatening systemic reaction that can affect all ages. The
clinical syndrome may involve multiple target organs, including skin, respiratory,
gastrointestinal and cardiovascular systems. The essential underlying mechanism is the
presence of biologically active chemical mediators such as histamine and tryptase
released from mast cells or basophils. The complex signalling cascades that regulate
mast cell activation have been extensively investigated and described in the literature 1.
The true incidence of anaphylaxis is unknown. Epidemiological studies have shown
differing results owing to differences in both definitions of anaphylaxis and the
population groups studied; however the incidence is increasing in recent years.
Prescribing of adrenaline increased by 97% between the years 2001 and 2005. It has
been estimated that by the end of 2005 there were 37,800 people in England that had
experienced anaphylaxis at some point in their lives2.
There are very limited data on trends in anaphylaxis internationally, but data indicate a
dramatic increase in the rate of hospital admissions for anaphylaxis in England,
increasing from 0.5 to 3.6 admissions per 100,000 between 1990 and 2004: an increase
of 700% (Figure 1)5.
Most of the data for the incidence of anaphylaxis have been derived from hospital
databases, and it is widely believed that anaphylaxis is under-recognised and under-
reported3.
Anaphylaxis can be triggered by any of a very broad range of allergens, but those most
commonly identified include food, drugs and venom (including wasp and bee stings). The
relative importance of these varies very considerably with age; with food being
8Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
particularly important in children and medicinal products being much more common
triggers in older people.
Anaphylaxis remains a significant cause of mortality. Of 164 fatal reactions identified
between 1992 and 1998 in the United Kingdom, around half were caused by drugs. Of
those not caused by drugs, half were related to venom and most of the remainder to
food3. With the increase in food allergies, the Office of National Statistics (ONS) started
recording deaths from anaphylaxis due to food allergies separately from anaphylaxis due
to other causes in 2002.
When anaphylaxis is fatal, death usually occurs very soon after contact with the trigger.
From a case-series, fatal food reactions cause respiratory arrest typically after 30–35
minutes; insect stings cause collapse from shock after 10–15 minutes; and deaths
caused by intravenous medication occur most commonly within five minutes. Death
never occurred more than six hours after contact with the trigger
Studies of fatal and near-fatal anaphylaxis in humans delineate risk factors for
anaphylaxis such as pre-existing asthma, a current asthma attack, food allergies
(particularly peanuts, tree nuts and shellfish), reaction to trace amounts of foods and
use of non-selective β-blockers4. Other factors include recent infection, intense exercise
after the exposure and concurrent exposure to other allergens such as pollen in pollen
allergic individuals.
Treatment
Early intramuscular adrenaline is the optimal treatment for patients suffering
anaphylaxis5. Most studies of fatal anaphylaxis show that a lack of, or delay in,
administration of adrenaline is a frequent factor in death, whereas early administration
of adrenaline even in severe attacks is associated with survival. The median time to
respiratory or cardiac arrest is reported to be 30 minutes for food- and 15 minutes for
venom-induced anaphylaxis, so adrenaline usually needs to be administered before
medical help is available. However, self-injectable adrenaline is underused even when it
is available4.
The recommended dose for auto-injectors is 300-500 µg for adults and 150-300µg for
children depending on body weight (10 µg/kg).
One injection from an auto-injector should be given immediately when symptoms are
recognised and a second injection can be given 5-15 minutes later if symptoms are not
improving. Therefore patients known to be at risk of anaphylaxis should have access to
at least two AAIs.
The Resuscitation Council guidelines advise that patients should always be observed
after treatment for anaphylaxis, for at least 6 hours and up to 24 hours in adults and for
12 to 24 hours in children, as symptoms can recur up to 24 hours after the initial
reaction (this is called a biphasic reaction). The incidence of biphasic reactions is
reported as 1-20% and unfortunately it is not possible to predict which patients will
experience a biphasic reaction.
2.2.2 Pharmacokinetics of adrenaline
Adrenaline is a naturally occurring substance produced by the adrenal gland in the body
and secreted in response to exertion or stress. Endogenous plasma concentrations of
adrenaline in normal subjects are in the range 30–160 ng/L.
Adrenaline is rapidly destroyed in the gut if swallowed and therefore needs to be given
by injection. The effects of adrenaline after subcutaneous (SC) injection (injection into
the fatty tissue beneath the skin) are produced within 5 minutes but increase more
slowly, taking 30 minutes to reach optimal levels compared with a more rapid peak after
intramuscular (IM) injection (injection into the muscle)6.
9Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
The amount of adrenaline in the blood is halved in about 2.5 minutes. However, by
subcutaneous or intramuscular routes, local constriction of the blood supply slows the
absorption, so that the effects build up and last much longer than the half-life of
2.5 minutes would predict7.
Adrenaline does have side effects, mainly on the heart (fast or irregular heartbeat, or
angina).
2.2.3 Doses needed to treat anaphylaxis
Even though adrenaline is considered to be the optimal drug for use in connection with
anaphylactic or threatening anaphylactic reactions, very little is known about what doses
or plasma concentrations are required in this context.
The recommended dose of adrenaline is usually within the range 5-10 µg/kg bodyweight
but higher doses may be necessary in some cases. When adrenaline is delivered by an
auto-injector device the following are recommended doses: in children between 15 kg
and 30 kg in weight the usual dose is 150 µg and in adolescents and adults the
recommended dose is 300 to 500 µg.
There is a risk of overdosing small children with a body weight of under 15kg with an
auto-injector so these are not generally recommended for such small children.
The following intramuscular doses are recommended in the Resuscitation Council
Guidelines which are specified as being in the context of administration by a healthcare
professional:
> 12 years: 500 µg IM i.e. same as adult dose 300 µg if child is small or
prepubertal
> 6 – 12 years: 300 µg IM
> 6 months – 6 years: 150 µg IM
< 6 months: 150 µg IM
Most patients only require one dose but the dose can be repeated after 5-15 minutes if
symptoms do not improve or recur.
The scientific basis for the recommended doses is weak. The recommended doses are
based on what is considered to be safe and practical to draw up and inject in an
emergency.
3 Quality Aspects
3.1 Drug Substance: adrenaline
The European Pharmacopeia (Ph Eur) is a publication detailing the official European
quality standards for ingredients of medicinal products. The quality of the drug
substance adrenaline is controlled according to the Ph Eur. specification in all of the
licenced AAIs.
3.2 Design and Operating Principle of auto-injectors
All AAIs comprise a sterile adrenaline solution filled into a container consisting of either a
glass cartridge (also known as a carpoule) or pre-filled glass syringe with a fixed needle.
In all cases they are made from glass suitable for injections. There are two fundamental
designs for AAIs licensed in the UK:
10Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
- the cartridge type injector for example EpiPen® and Jext®
- the syringe type injector for example Emerade®
Each auto-injector brand has a different delivery/administration system. Likewise the
firing mechanism which provides the force behind the actual injection process which
pierces the skin and enters the outer (antero-lateral) thigh is unique to each brand. The
assembled auto-injectors are enclosed in a “carry case” to protect them from mechanical
shock and damage.
In the cartridge type injectors the volume of adrenaline solution that the auto-injector
contains (the fill volume) is significantly larger than the actual volume of adrenaline
solution intended to be injected (the delivered volume) so unused solution remains in
the activated auto-injector after use. In the case of EpiPen the volume of adrenaline
delivered is the same in both the adult and the paediatric injectors: the concentration of
adrenaline in the solution is adjusted to give the different doses (150 µg for paediatric
use and 300 µg for adult). Conversely the paediatric and adult versions of JEXT and
Emerade auto-injectors contain the same concentration of adrenaline solution but the
delivered volume is adjusted to achieve the correct paediatric dose.
As delivered volume relates to the quantity of adrenaline actually injected it is a critical
test for all AAIs to ensure delivery of the intended dose throughout the shelf life of the
product.
During a conventional manual injection i.e. one given by a healthcare professional to an
individual in a medical setting, the force to move the solution in a pre-filled syringe is
provided by the thumb pushing the plunger. An auto-injector is generally intended for
self-administration by an individual or by a family member or friend. Prior to use the
plunger and needle are concealed within a plastic shell. The injector is activated by
pulling off a cap or pressing a button and either swinging the AAI towards the thigh or
placing it against the thigh. A coiled spring is then released inside the auto-injector
which pushes the plunger to inject the solution into the patient. The adrenaline solution
is pressurised to varying degrees depending on the design of the AAI. When the auto-
injector is used the needle is propelled forward to pierce the skin and deliver the
solution.
Discussion on the design of AAIs
There has been considerable discussion in the medical community and in patient groups
regarding the suitability of the needle length used with AAIs with respect to the ability of
the injectors to deliver the adrenaline solution to the optimal body compartment i.e. into
the thigh muscle tissue. All UK licensed products claim to deliver an intra-muscular
injection of adrenaline. The way the AAI is used (its method of operation), the force
behind the adrenaline solution and how these factors contribute to the dose delivery
have also been debated. Evidence of how these factors influence the site of deposition in
the tissue is based on limited studies using non-clinical models. These three issues (a)
needle length (b) method of operation and (c) applied mechanical force are discussed in
greater detail below.
(a) Needle length
As there are differences in AAI design and method of operation, the total needle length
cannot be considered on its own, as a portion of the needle remains within the device
once fired - unlike a manual injection. The extended needle length measurement
11Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
provides an indication of the effective needle length available to deliver the adrenaline
solution into the body and should be controlled.
Schwirtz and Seeger11 reported “the mean exposed needle length was 15.36 mm
(standard deviation [SD] 0.22) for Jext and 15.02 mm (SD 0.25) for EpiPen”. Non-
clinical evidence exists -using both ballistic gelatine and porcine models - to support that
adrenaline solution from both EpiPen and JEXT auto-injectors penetrate some distance
into body tissues beyond the needle tip (Refer to section 4. Non-Clinical Evidence, for
study detail and discussion). This suggests that there are additional factors to take into
consideration when determining where the adrenaline solution is actually deposited in
the body:-
1. the method of operation of the respective auto-injectors, and
2. the force applied to the plunger by the firing mechanism.
(b) Method of operation
In all AAIs a safety cap is removed immediately prior to the actual injection sequence.
The safety cap is at the opposite end of the device from the needle and once removed
the device is considered to be “armed” for use. There are two principal methods used for
the self-injection of adrenaline using auto-injectors. These are the “swing and jab”
method or “place and press” method. EpiPen® utilises the swing and jab method of
administration while JEXT® and Emerade® utilise the place and press method. The
method employed is related to the activation force required for each delivery system.
It is possible that there is some degree of tissue compression during both the “swing and
jab” technique and the “place and press method”. This may result in a net decrease in
the skin to muscle distance (STMD), enabling the solution to penetrate deeper into the
tissues.
(c) Force applied to the plunger by firing mechanism/power pack
As liquids cannot be compressed, the adrenaline solution is pressurised to varying
degrees depending on the individual device design and construction. This phenomenon
theoretically causes the solution to be expelled beyond the needle tip to varying degrees
and is device dependent. This is confirmed by studies where ballistic gelatine has been
used as a substitute for human tissue (Refer to section 4. Non-Clinical Evidence).
However, it is not known how this correlates to administration into live human tissue.
3.3 Finished product specification
AAIs comprise a drug product i.e. the adrenaline solution, which is sealed in a glass
container, with a device component (the injector) for delivering the solution. These
elements form the finished product. The finished product specification is a set of
characteristics and acceptance limits that each batch of finished product must comply
with before it can be released for sale.
As a part of this review the finished product specifications were examined for all licensed
AAIs. The tests applied to auto-injectors can be sub divided into the following:
a. Tests to meet the Ph Eur general requirements for injections
b. Tests to monitor adrenaline content, degradation substances and other
impurities and levels of important ingredients such as sodium
metabisulphite (an antioxidant used to stabilise the adrenaline solution)
12Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
c. Functional tests to monitor the performance of the delivery mechanism
d. The British Pharmacopeia (BP) monograph controls the quality of the
adrenaline solution to a minimum standard in respect of the content of the
active pharmaceutical ingredient, pH and degradation products.
The above quality standards are reviewed for each individual product in an application
for a marketing authorisation in the European Union.
Functional tests related to the delivery mechanism
Although these quality characteristics are controlled in the design of the products, they
should be brought together in the finished product specification:
1. Delivered volume
The delivered volume (the volume of adrenaline solution released when the auto-
injector is deployed) requires tight control.
2. Delivery time
The time taken to eject the adrenaline solution from the needle (the delivery time) is
critical. As anaphylaxis progresses very rapidly, delivery time should be measured for all
AAIs and should reflect a rapid delivery time in the order of seconds.
3. Exposed needle length
The design of an auto-injector should ensure that consistent extended needle length
occurs when the device is activated by a patient.
4. Activation Force
All auto-injectors need to be activated by the patient before use. This is achieved by
removing the safety cap and either swinging or pressing the needle end of the device to
the thigh. These operations should be possible for both adults and children; however the
safety cap should not come away too readily either, to prevent accidental removal.
The force required to initiate the injection cycle should be consistent during storage to
ensure that AAIs are usable throughout the shelf-life period.
Discussion on functional testing
The approach to functional testing varies between manufacturers. Our recommendation
is that the acceptance criteria for functional tests should be based on a critical evaluation
of historical long-term stability data with consideration of the impact on the delivered
dose. Critical quality attributes which ensure the correct dose is delivered within defined
time limits should be included in the release and shelf-life specification requirements.
AAI product defect reporting and product recalls
In the past two years quality defects have been reported regarding Anapen® and JEXT.
A recall was issued by the MHRA Defective Medicines Report Centre (DMRC) for all
strengths of Anapen in 2012, based on finished product testing failures to deliver the
correct volume and/or delivery time failure. The JEXT quality defect was announced by
the Reference Member State (RMS) Sweden and a Class II recall notification was issued
by the DMRC in early December 2013. In January 2014 Sweden (RMS) issued a Class II
recall notification for Emerade due to suspected technical defects, at this point the
13Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
product had not been launched within the UK. In addition there was a recall in October
2013 concerning another auto-injector product (which does not contain adrenaline) as a
small number of syringes potentially had needles protruding through the needle shield.
Assembly of “ready to use” injectable drug products is complex and these incidents
suggest that additional controls might be necessary.
AAIs are intended for single use and are classified as medicinal products with an integral
delivery system (device). The device aspects of AAIs should be designed and qualified by
the manufacturers to be fit for purpose with relevant supporting data on the
development and manufacture of the device submitted in the marketing authorisation
application reviewed by the Licensing Authority.
Although the AAIs do not require a CE mark, they should be compliant with the relevant
sections of standards published by the International Organization for Standardization
(ISO), for example BS EN ISO 11608 Needle-based injection systems for medical use.
They should meet the essential requirements of Annex 1 of the Medical Device Directive.
The marketing authorisations for AAIs should be reviewed with respect to ensuring the
finished product specifications and in-process controls (IPCs) for the device assembly
process are adequately described and that a summary of the following is provided.
1. The design and qualification of the delivery system i.e. the device development
history.
2. A summary of identified critical failure modes for the delivery system.
3. Updated finished product specifications including appropriate functional tests with
sample size tested per batch and the acceptable quality level (AQL) for each test.
4. An overview of how the essential requirements of Annex 1 of the Medical Device
Directive are met.
Product Stability Update
At the request of the MHRA, the manufacturers of the licensed AAIs provided updated
stability data for their products to the MHRA for review.
4 Non-Clinical Evidence
Two main non-clinical models have been cited in the MAH’s response to the MHRA’s
request to provide further information on their products; gelatine and porcine tissue.
Both have been used in the study of ballistics and weapons research. A brief discussion
is presented below of both models in the context of their usefulness for assessing the
performance of injector pens in delivering adrenaline to the muscle layer.
4.1 Gelatine models
Ballistic gelatine is reported as being designed to simulate living soft tissue (Nicholas and
Welsch, 2004)8. It is regarded by the US military as the standard for evaluating the
effectiveness of firearms against humans because of its convenience and acceptability
over animal or cadaver testing. Use by the military would appear to have resulted in the
acceptance of the use of gelatine in ballistic and other research and it has been referred
to in some publications (including those cited by the MAH) as a ‘validated tissue
simulant’. However, its use appears to be based more on custom and practice than
inherent suitability. It was first used in 1960 and various techniques were used to
measure the kinetic energy of a projectile travelling through a block of gelatine. Early
models were not compared to living tissue in a quantitative or reproducible way.
14Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
In the first of many papers in the mid to late 1980s, researchers at the Letterman Army
Institute of Research (LAIR) used both live swine (50-70 kg) and gelatine blocks to test
bullets and subsequently compared the results9. Although the paper did not include
specific comparisons between gelatine and animal tissue, the LAIR team and many other
researchers afterward cited this published paper as the foundation for using Fackler’s
gelatine model as an approximate or equivalent substitute for animal tissue. A paper by
Fackler and Malinowski (1985)10 states that the depth of penetration measured in living
swine leg muscle was reproduced in the gelatine within 3%. These findings and the
convenience of using non-animal or non-cadaveric tissue appear to have led to the use
of gelatine on its own.
While the conditions and preparation of the gelatine have been standardised to some
extent, and can be used to compare the behaviour of projectiles within that limited
context, the model cannot be regarded as fully representative of living tissue, primarily
because it is homogeneous rather than heterogeneous. The different types and textures
of animal tissue, particularly bones, cannot be regarded as being adequately simulated
in a gelatine alone system. Also, differences in the gelatine such as method of
preparation, concentration and temperature mean that consistency between laboratories
cannot be guaranteed.
The acceptance of the model for ballistics has led to its use in investigating the track of
injections from auto-injectors. In this context, it could be suitable for investigating the
depth to which a drug might be injected, as the only tissues to be penetrated are skin
and fat, unlike in ballistics research, where the full range of tissues could be
encountered. It might be acceptable, for example, to use gelatine models to rank
devices against one another for depth of penetration, but it would not simulate clinical
conditions as closely as live animal or human tissue.
A study comparing three injector pens was reported by Schwirtz and Seeger (2012)11.
Three AAIs (Jext, EpiPen® and Anapen) were tested for, amongst other features, the
injection depth and estimated volume of black ink delivered into ballistic gelatine. The
mean maximum injection depths in gelatine within 10 seconds were 28.87 mm (SD
0.73) for Jext, 29.68 mm (SD 2.08) for EpiPen® and 18.74 mm (SD 1.25) for Anapen
(Figure 2). The length of the EpiPen® and Jext needles is 14.3 mm and the Anapen
needle is 8.9 mm to 9.9 mm.
Figure 2: Photographs showing the total injection depth into gelatine 10
seconds after activation of Jext (A), EpiPen (B), and Anapen (C), measured as
the vertical distance from the surface of the gelatine to the lowest part of the
ink area using digital image processing.
(Photographs copyright of Schwirtz and Seeger, 201212)
A previous pilot study reported by the same authors (Schwirtz and Seeger, 2010) 12
included a simulation of firing two AAIs through clothes, EpiPen® Junior and Anapen®
Junior. Each auto-injector was fired into ballistic gelatine in the presence or absence of a
15Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations piece of denim (a double seam of Levi’s blue jeans). The activation force was recorded, and the effective (exposed) needle length was measured by a calliper after the device was removed from the ballistic gelatine. The presence of denim did not alter the activation force or effective needle length of either of the AAIs. 4.2 Pig models Based on current knowledge, the pig as an animal model for human skin is generally accepted as being the most representative of human skin13 and it is commonly used in pharmaceutical development for local tolerance and skin penetration studies. Given the difficulty in generating clinical data on injector pens, the use of the pig for this purpose is considered appropriate and the most valid model currently available. The MAH for Epipen® has cited a study conducted by the US military on the depth of penetration into porcine thighs achieved by the EpiPen® to address the question of its performance in obese patients14. Adrenaline from 21 EpiPen® devices was mixed with methylene blue as a colour tracer and triggered into the lateral aspect of 21 cadaver pig- thighs. The results show that with an exposed needle length of 14.3 mm, the mean ± SD delivery depth from the skin to the muscle was 26.9 ± 5.4 mm (p
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
The data from ballistic gelatine are consistent with those obtained using porcine tissue.
Consistent results were obtained in the study reported by Schwirtz and for the purposes
of comparison of the three devices, the model is considered acceptable. While the results
in a gelatine system show that the degree of penetration was not affected by the
presence of denim, the results are not considered as robust as if porcine tissues covered
with denim had been used. Nonetheless, the data are considered to be reasonably
reliable and the conclusion that the performance of the AAI is not affected by the
presence of clothing, including denim, is considered acceptable.
5 Clinical Evidence
The following section contains evidence from published literature and evidence provided
by the Marketing Authorisation Holders (MAH) at the request of the MHRA.
5.1 Intramuscular vs subcutaneous injection
There is some debate over the most appropriate route of administration of adrenaline in
the treatment of acute anaphylaxis. Many different authoritative recommendations have
been made but these are largely based on descriptive studies, clinical experience and
tradition rather than on prospective clinical studies, tailored for these products.
Adrenaline is most effective when given immediately after the onset of anaphylaxis
symptoms. The initial recommended adult dose is 300 - 500 µg, injected intramuscularly
in the anterolateral aspect of the mid-thigh. When injected by other routes, adrenaline
appears to have a less satisfactory therapeutic window; for example, onset of action is
potentially delayed when it is injected subcutaneously, and the risk of adverse effects
potentially increases when it is injected intravenously. An intravenous injection should
only be given under medical supervision when continuous monitoring is available.
Pharmacokinetics
Simons et al15 conducted a prospective, randomized, blinded, placebo-controlled, 6-way
crossover study of intramuscular versus subcutaneous injection of adrenaline in healthy
allergic men aged 18-35 years. The objective of the study was to provide information
regarding the optimal route and site of adrenaline injection in adults.
During the course of the study, each participant received 4 injections of adrenaline 0.3
mg (0.3 mL) and 2 injections of saline solution (0.9% NaCl, 0.3 mL) through use of a
variety of injection routes and sites. Adrenaline USP I: 1000, 0.3 mg (0.3 mL) was
injected either IM into the thigh (vastus lateralis) muscle or the upper arm (deltoid)
muscle or SC in the upper arm.
To ensure blinding, all injections were given by a nurse not otherwise involved in the
study, and at each visit both the thigh and upper arm sites were covered after the
injection.
17Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
Figure 3: Mean plasma adrenaline concentrations versus time are shown after administration of
an identical 0.3 mg (0.3mL) dose of adrenaline by IM or SC injection in 2 different sites. T; Thigh;
A upper arm. Mean endogenous plasma adrenaline concentrations are shown after IM or SC
injection of 0.9% saline solution (0.3 mL) in the upper arm. The plasma adrenaline concentrations
shown were calculated by averaging (mean ±SEM) the adrenaline concentrations at each sampling
time for each route and each site of injection.
The results showed a swift increase in plasma levels of adrenaline following IM injection
into the thigh, which was greater than levels achieved from an IM or SC injection into
the arm. Unfortunately the study did not investigate SC injection into the thigh. The time
to maximum concentration in the blood (Tmax) for the IM injection was around 10
minutes
Using the EpiPen a second peak in plasma concentration was seen at 40 minutes which
the authors suggest may be due to further absorption of exogenous adrenaline at the
injection site after a period of initial vasoconstriction at the site, or due to rebound
endogenous adrenaline release. The latter seems unlikely as it is not seen with the other
routes of administration. Another explanation could be that part of the dose from the
EpiPen was delivered subcutaneously and was therefore absorbed more slowly giving a
delayed onset of action.
A further study by Simons et al16 in children measured the pharmacokinetics (PK) of
adrenaline following subcutaneous injection (9 children) and intramuscular injection (8
children). The study was a prospective, randomised, blinded parallel group study in
children with a history of anaphylaxis. The subcutaneous injection was administered via
needle and syringe while the intramuscular injection was administered using an EpiPen
Auto-injector.
Results
In the nine children who received a SC injection the mean maximum plasma
concentration of adrenaline was 1802 ±214 pg/mL, achieved at a mean time of 34 ±14
minutes (range 5 to 120 minutes). Only two of the children achieved a maximum
concentration of adrenaline by 5 minutes. In the eight children who received
18Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
intramuscular injection via EpiPen the mean maximum concentration of adrenaline was
2136 ±351 pg/mL achieved at a mean time of 8 ±2 minutes, which was significantly
faster than the mean time at which maximum plasma concentrations of adrenaline were
achieved using the SC route.
Figure 4: Mean plasma adrenaline concentration versus time after injection of
adrenaline subcutaneously or intramuscularly
The results of this study, despite its limitations, support the intramuscular route as the
optimal route of injection of adrenaline in the treatment of anaphylaxis.
5.1.1 Intramuscular versus subcutaneous injection conclusions
The data regarding subcutaneous versus intramuscular injections are sparse and the
recommendation for intramuscular injection of adrenaline in the treatment of
anaphylaxis appears to be mainly based on theoretical grounds. It is imperative that the
adrenaline is absorbed quickly in order to minimise the risk of a fatal outcome in
anaphylaxis and therefore the intramuscular route is the logical choice. The study by
Simons et al in children with a history of anaphylaxis supports the assumption that the
intramuscular route gives a faster time to maximum plasma concentration of adrenaline,
although the data are limited by the small number of children included in the study. It
also lends some support to the supposition that EpiPen delivers its dose intramuscularly
at least in the children studied; but it should be borne in mind that children, in general,
have less subcutaneous fat than adults. Owing to the nature of anaphylaxis no clinical
studies to compare the relative effectiveness of the two routes during an actual
anaphylactic reaction have been conducted, nor would they be ethical. It may be that
the auto-injectors actually deliver some of the dose intramuscularly and some
subcutaneously. As the subcutaneous portion would be absorbed more slowly this may
be beneficial in some cases where the anaphylactic reaction is prolonged, but it is
imperative that the adrenaline is delivered quickly to halt the allergic cascade and
therefore the major part of the dose should be delivered intramuscularly.
5.2 Site of injection
The Resuscitation Council Guidelines state that the best site for IM injection is the
anterolateral aspect of the middle third of the thigh and that the subcutaneous or inhaled
routes for adrenaline are not recommended for the treatment of an anaphylactic reaction
because they are less effective. Injection in the anterolateral aspect of the middle third
19Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
of the thigh is emphasised in the auto-injector Patient Information Leaflet (PIL) for
EpiPen and in the DVD given to patients.
A prospective study by Bewick et al17 recruited 93 children (age range, 1-16 years) with
food allergies who attended the authors’ regional paediatric allergy outpatient clinics
over a 6-month period in mid-2012. Using a MicroMaxx portable ultrasound machine
with a linear HFL38/13.6 MHz probe the authors measured the distance from the skin
surface to the vastus lateralis muscle interface at 3 distances along the outer thigh (one-
fourth [proximal thigh], one-half [mid-thigh], and three-fourths [distal thigh] the
distance from the greater trochanter to the lateral epicondyle of the femur) as
determined with a tape measure. Weight, height and waist circumference were also
measured, and BMI as well as age- and sex-appropriate BMI centiles were calculated
(Table 2).
Table 2: Anthropometric measures of 93 children referred to the local paediatric
allergy service
Parameter* Children 30 All children
kg weight kg weight
No. (%) 62 (67) 31 (33) 93 (100)
Age (y), median (IQR) 4 (2-6) 12 (8-14) 6 (3-10)
Boys, no. (%) 35 (57) 19 (61) 54 (58)
Weight (kg), median (IQR) 16.6 (12.2 – 43.8 (38.4-53.3) 20.8 (14.5-38.6)
20.8)
Height (cm), median (IQR) 102 (88-114)
150 (140-159) 114 (96-141)
BMI (kg/m2), median (IQR) 16.1 (15.5-17.1)
19.9 (18.2-22.4) 16.8 (15.7-19.1)
Waist circumference (cm), 52 (49-56) 75 (68-80) 56 (51-68)
median (IQR)
Skin surface to muscle depth
(mm), median (IQR)
Proximal thigh 10.0 (8.3-13.2) 19.2 (12.8-25.7) 12.0 (8.6-16.9)
Mid-thigh 8.4 (7.0-10.2) 12.2 (7.8-16.5) 8.8 (7.0-12.9)
Distal thigh 6.8 (5.8-8.5) 9.7 (7.2-12.2) 7.9 (5.9-9.6)
Mid-calf 7.0 (6.2-7.2) 9.5 (8.6-10.5) 8.5 (7.0-9.8)
Skin surface to muscle depth >12.7 >15.9
greater than needle length
(mm)
Proximal thigh, no. (%) 17 (27) 19 (61) 36 (39)
Mid-thigh, no. (%) 10 (16) 9 (29) 19 (0)
Distal thigh, no. (%) 1 (2) 4 (13) 5 (5)
Mid-calf, no. (%) 0 (0) 0 (0) 0 (0)
IQR, Interquartile range
*The median (IQR) is based on triplicate measurements
20Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations Figure 5 Percentage of children whose skin surface-to-muscle depth was greater than the Epipen (children > 30kg) or Epipen Junior (children
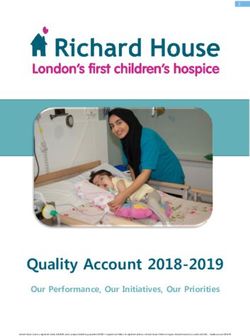
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations 5.3 Appropriate needle length There are concerns that, owing to the increasing obesity (BMI ≥30) of the population in the UK, the needle lengths in the currently licensed AAIs are not adequate to deliver the dose of adrenaline to the muscle tissue of the thigh. A survey published in 2012 found that just over a quarter of all adults (26%) in England are obese. The report compiled by the Health and Social Care Information Centre, relates to information gathered during 2011. There has been a marked increase in obesity rates over the past eighteen years – in 1993 13% of men and 16% of women were obese; in 2011 this rose to 24% for men and 26% for women. For children attending reception class (aged 4-5 years) during 2011-12, 9.5% were obese18. A study by Song et al19 investigated whether EpiPen auto-injector, with a needle length of 14.3 mm, is sufficient for intramuscular delivery of adrenaline in men and women. The distance from skin to muscle in the anterolateral aspect of the thigh was measured in 50 men and 50 women who had undergone computed tomography (CT) of the thighs for other medical reasons. For each individual, body mass index (BMI; a measure of weight in kilograms divided by the square of height in meters) was also calculated, and the individuals were classified as underweight (BMI, 18.5), normal (BMI, 18.5–24.9), overweight (BMI, 25.0 –29.9), and obese (BMI, 30.0) using standard definition. The CTs were analysed for measurement of the distance from the skin surface to the muscle. This is the path the needle traverses before reaching the fascia of the vastus lateralis muscle. Results The 50 men included 39 white individuals (78%), 4 African American individuals (8%), 1 Asian individual (2%), and 6 individuals of other races (12%). The 50 women included 35 white individuals (70%), 12 African American individuals (24%), 2 Asian individuals (4%), and 1 individual of another race (2%). In the study participants the mean ±SD distance from skin to muscle was 6.6 ±4.7 mm for men and 14.8 ±7.2 mm for women (P
Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
21 women (11 obese with a mean BMI of 35.2, 6 overweight with a mean BMI of 30.1,
and 4 normal with a mean BMI of 24.5) had a greater distance from skin to muscle than
the EpiPen extended needle length of 14.3 mm.
As a certain pressure is required to activate the EpiPen device, in order to investigate the
role of any subsequent compression, the distance to muscle was measured with an
ultrasound machine in 1 representative man and 1 representative woman with and
without 8 lb. of weight applied. The 8 lb. of weight decreased the distance to muscle by
25% in the woman and 19% in the man. Assuming a liberal estimate of 25%
compression of distance to muscle in both sexes, the authors recalculated the distance
to muscle for all study participants. The single man with a distance to muscle of 34.7
mm would not be affected, whereas the number of women with a distance to muscle
greater than 14.3 mm was calculated to still be 14 (28%).
These results demonstrate that the EpiPen needle length is adequate to reach the muscle
and therefore deliver adrenaline intramuscularly in most men but not in a number of
women. Even when allowance was made for BMI the gender difference remained as seen
in the figure above. Applying the pressure needed to trigger an EpiPen device decreased
the skin to muscle distance in a representative man and woman but not sufficiently to
ensure that an intramuscular injection of the dose would be delivered in all women or in
very obese men. From this study it would seem that even the longer needle length of the
Emerade auto-injector would not be adequate for all subjects.
Another study conducted by Stecher et al20 in children demonstrated that the needle on
AAIs is not long enough to ensure delivery of the medication intramuscularly in a
significant number of children.
Patients between the ages of 1 and 12 years who presented to a children’s hospital were
enrolled in the study. Ultrasound was used to determine the depth from the skin to the
vastus lateralis muscle. The patient’s body mass index was also recorded. The data were
analysed using simple descriptive statistics, and logistic regression was used to identify
variables that might predict whether or not the needle length was exceeded.
In addition, the data were analysed using an estimate of 25% for displacement of tissue
with applied pressure from the adult study cited above.
23Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations
Results
A total of 256 children were enrolled. Of these, 158 children weighed less than 30 kg and
would be prescribed the 0.15 mg AAI (extended needle length of 10.16 to 15.24 mm).
Nineteen of these children (12%) had a skin to muscle surface distance of >12.5 mm
and would not receive adrenaline intramuscularly from current auto-injectors. There
were 98 children weighing ≥30 kg who would receive the 0.3 mg AAI. Of these 98
children, a total of 29 (30%) had a skin to muscle surface distance of >16 mm and
would not receive adrenaline intramuscularly.
Figure 6: Scatter plot of depth to muscle from skin surface vs BMI (30 kg
group). The vertical line represents the length of the needle (15.8 mm).
24Adrenaline Auto-injectors: A Review of Clinical and Quality Considerations From these data there is no clear correlation between the muscle depth and the BMI in this population of children. Also, not surprisingly, unlike the adult population, there is no marked difference between the genders. A further study was conducted by Bhalla et al21 in order to measure muscle depth and evaluate predictors of auto-injector needle length inadequacy. This was a prospective cross-sectional study of a sample of low acuity emergency department patients aged 18 to 55 years. Demographic data and thigh circumference were recorded and body mass index (BMI) was calculated. Depth-to-muscle measurements of the vastus lateralus in a standing position, with and without gentle pressure to simulate muscle compression that occurs with correct auto-injector use were made using ultrasound. Results One hundred and twenty (120) subjects were enrolled with a mean BMI of 29.2 kg/m2. Thirty-one percent (31%) of the sample were found to be failure risks (36/116; confidence interval, 22.6%-39.5%) because these ED patients had compressed muscle depths exceeding 15.9 mm. Women were 6.4 times more likely than men to be a failure risk (54.4% vs 5% for men failure rate; P
You can also read