ALZHEIMER'S AND DIET: NEW RESEARCH FRONTIERS - AYESHA SHERZAI, MD DEAN SHERZAI MD, PHD(C)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Alzheimer’s and Diet:
New Research Frontiers
Ayesha Sherzai, MD
Dean Sherzai MD, PhD(c)
Co-Directors of Brain Health Center
Department of Neurology
Loma Linda University Health
Our Aging Society

growth provided by the U.S. Census suggest that
dementia, as shown in Figure 4. A12,31
this number may be as high as 16 million. A14,207
FIGURE 4
Projected Number of People Age 65 and Older (Total and by Age Group)
in the U.S. Population with Alzheimer’s Dementia, 2010 to 2050
Millions of people
Ages 65-74 Ages 75-84 Ages 85+
with Alzheimer’s
13.8
14
11.6
12
10
8.4
8
5.8
6
4.7
4
2
0
Year 2010 2020 2030 2040 2050
Created from data from Hebert et al. A12, 31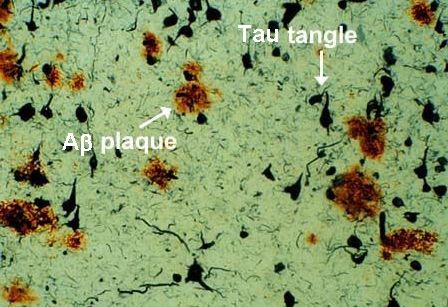
New Diseases • Alzheimer’s disease • Vascular dementia • Stroke • Parkinson’s disease

Alzheimer’s

1 in 10 people age 65 and older has Alzheimer’s disease.
89% increase in deaths due to Alzheimer’s between 2000 and 2014.
FIGURE 5
Percentage Changes in Selected Causes of Death (All Ages) Between 2000 and 2014
Percentage
89%
90
80
70
60
50
40
30
20
10
0
-1%
-10
-9%
-14%
-20
-21%
-30
-40
-50
-54%
-60
Cause Breast Prostate Heart Stroke HIV Alzheimer’s
of Death cancer cancer disease disease
Created from data from the National Center for Health Statistics. 208, 219
Between 2000 and 2014, deaths from Alzheimer’s State-by-State Deaths from$259 billion total annual payments for caring for individuals living with Alzheimer’s or other dementias in 2017.
More than 15 million Americans provide 18 billion unpaid care hours for people with Alzheimer’s or other dementias, valued at $230 billion.
The Big Myth
Source: Alzheimer’s Drug Discovery FoundationNormal Aging
Alzheimer’s
Mild Cognitive
Impairment No change
Other dementiasSperling, et al. (2011). Alzheimer's & dementia, 7(3), 280-292.
In more than 400 clinical trial between 2000 to 2012 99.6% Alzheimer’s drug failure rate.
Treatment & Research • Only 4 drugs for symptomatic management • Inadequate models: Mice are Not Men/Women • Clearance vs. Restoration
Genetics • Polygenetic disease: more than 90% in origin • Apolipoprotein E4 • Presenilin 1 • Presenilin 2 • Amyloid Precursor Protein (APP)
Opportunity Lost Wrong target Wrong models Wrong timing
18 THE ALZHEIMER’S SOLUTION
Hypothesis of Cognitive Diseases
Poor Diet
RISK High Sugar
s Ob
FACTORS te igh Saturated Fats es
e H ity
iab
D
Alc buse
A
rol
oh
n
Ox
Chol igh
io
este
ol
id
at
at
m
H
io
m
n
fla
In
Smoking
Stress
Dy G
ha ary
sre luc
n
io
gu ose
gu id
r
Be dent
lat
vio
sre Lip
lat
Hig
io
Blo ssur
Pre
Se
n
h
Dy
o d
ad a
e
Po e
H m
Sle or u
ep Small Tra
Vessel
DiseaseSle or
ep Small Tra
Vessel
Disease
Hypothesis of Cognitive Diseases
Regular Exercise1
PROTECTIVE +S
Moving tanding
FACTORS Str
ht e es
Exercise
r
M Ma
po g
ed na
Ex ayli
su
s
ita gem
D
tio
n ent
2
ind
ga-3 Fatty Acids
nw
Plant-Ba d Diet 3
U
Nutrition
se
1. Aerobic exercise,
ual
ng
resistance training,
Contin
Learni
and balance
e
strengthening.
m
Learn more in
O
Re
Chapter 4. st
ize
or
e
tim
2. Walking
s en
Op
meditation, mindful
7– Sl
riv
breathing, yoga, -D e
8H
o
of
and others. Learn ee urs o
e
s iti
p p v
more in Chapter 5. Pur Acti
3. Learn more about Social
Engage nt
beneficial and me
Volunteering
harmful foods on
page 126.Dietary Confusion
Loma Linda
• The only Blue
Zone in the US
• Focus on Lifestyle
and preventive
medicineDecade of Evidence
Adventist Health Study:
A 1993 study titled “The Incidence of Dementia and
Intake of Animal Products,” found that in a group of
over 3,000 individuals, those who ate meat—
including those who ate only poultry and fish—had
twice the risk of developing dementia compared to
vegetarians.Decade of Evidence The Chicago Health and Aging Project: Longitudinal study, 2500 older adults, those who consumed higher amounts of saturated and trans fatty acids over a six-year period had a higher risk of developing Alzheimer’s, while those eating fats derived from plants had a lower risk.
Decade of Evidence Kaiser Permanente Northern California Group: 9,900 patients, individuals with high cholesterol during midlife had a 57% higher risk of developing Alzheimer’s disease later on. Even borderline high cholesterol increased the risk of Alzheimer’s by 23%.
Decade of Evidence
Women’s Health Study
• Nearly 6,000 women followed over a 4-years
• Higher saturated fat intake was associated with a
poor trajectory of cognition—specifically a faster
decline in memory by 70%
• Women with the lowest saturated fat intake had
the brain function of women six years youngerMediterranean Diet Score Construct
High Score Low Score
• Vegetables • Meat, poultry, and
• Fruits
dairy
• Whole grains • Sugar
• Nuts and seeds
• Legumes
• Mono- and Polyunsaturated
fats
• Fish - as a source of omega
fatsMIND Diet
• Emphasizes whole food,
plant-based diet
• Limits meat, poultry, dairy
and sugar
• Specifies consumption of
berries, green leafy
vegetables and beansAlzheimer’s & Dementia 11 (2015) 1007-1014
Featured Articles
MIND diet associated with reduced incidence of Alzheimer’s disease
Martha Clare Morrisa,*, Christy C. Tangneyb, Yamin Wanga, Frank M. Sacksc,
David A. Bennettd,e, Neelum T. Aggarwald,e
a
Department of Internal Medicine and the Rush Alzheimer’s Disease Center at Rush University Medical Center, Chicago, IL, USA
b
Department of Clinical Nutrition and the Rush Alzheimer’s Disease Center at Rush University Medical Center, Chicago, IL, USA
c
Department of Nutrition, Harvard School of Public Health, Boston, MA, USA
d
Department of Behavioral Sciences and the Rush Alzheimer’s Disease Center at Rush University Medical Center, Chicago, IL, USA
e
Department of Neurology and the Rush Alzheimer’s Disease Center at Rush University Medical Center, Chicago, IL, USA
Abstract Introduction: In a previous study, higher concordance to the MIND diet, a hybrid Mediterranean-
Dietary Approaches to Stop Hypertension diet, was associated with slower cognitive decline. In
this study we related these three dietary patterns to incident Alzheimer’s disease (AD).
Methods: We investigated the diet-AD relations in a prospective study of 923 participants, ages 58 to
98 years, followed on average 4.5 years. Diet was assessed by a semiquantitative food frequency
questionnaire.
Results: In adjusted proportional hazards models, the second (hazards ratio or HR 5 0.65, 95%
confidence interval or CI 0.44, 0.98) and highest tertiles (HR 5 0.47, 95% CI 0.26, 0.76) of
MIND diet scores had lower rates of AD versus tertile 1, whereas only the third tertiles of the
DASH (HR 5 0.61, 95% CI 0.38, 0.97) and Mediterranean (HR 5 0.46, 95% CI 0.26, 0.79) diets
were associated with lower AD rates.
Discussion: High adherence to all three diets may reduce AD risk. Moderate adherence to the MIND
diet may also decrease AD risk.
! 2015 The Alzheimer’s Association. Published by Elsevier Inc. All rights reserved.
Keywords: Cognition; Alzheimer’s disease; Nutrition; diet; Epidemiological study; Aging
1. Introduction the Mini-Mental State Examination (MMSE) and Clock
Drawing Test compared with the control diet participants.Alzheimer’s & Dementia 11 (2015) 1015-1022
MIND diet slows cognitive decline with aging
Martha Clare Morrisa,*, Christy C. Tangneyb, Yamin Wanga, Frank M. Sacksc, Lisa L. Barnesd,e,f,
David A. Bennette,f, Neelum T. Aggarwale,f
a
Department of Internal Medicine at Rush University Medical Center, Chicago, IL, USA
b
Department of Clinical Nutrition at Rush University Medical Center, Chicago, IL, USA
c
Department of Nutrition, Harvard School of Public Health, Harvard University, Boston, MA, USA
d
Department of Behavioral Sciences at Rush University Medical Center, Chicago, IL, USA
e
Department of Neurological Sciences at Rush University Medical Center, Chicago, IL, USA
f
Rush Alzheimer’s Disease Center at Rush University Medical Center, Chicago, IL, USA
Abstract Introduction: The Mediterranean and dash diets have been shown to slow cognitive decline; how-
ever, neither diet is specific to the nutrition literature on dementia prevention.
Methods: We devised the Mediterranean-Dietary Approach to Systolic Hypertension (DASH) diet
intervention for neurodegenerative delay (MIND) diet score that specifically captures dietary compo-
nents shown to be neuroprotective and related it to change in cognition over an average 4.7 years
among 960 participants of the Memory and Aging Project.
Results: In adjusted mixed models, the MIND score was positively associated with slower decline in
global cognitive score (b 5 0.0092; P , .0001) and with each of five cognitive domains. The differ-
ence in decline rates for being in the top tertile of MIND diet scores versus the lowest was equivalent
to being 7.5 years younger in age.
Discussion: The study findings suggest that the MIND diet substantially slows cognitive decline with
age. Replication of these findings in a dietary intervention trial would be required to verify its rele-
vance to brain health.
! 2015 The Alzheimer’s Association. Published by Elsevier Inc. All rights reserved.
Keywords: Cognition; Cognitive decline; Nutrition; Diet; Epidemiologic study; Agingsumption i
ids58 appea
following a
used to der
study, mil
higher vege
risk for AD
of the indiv
dictor when
results stre
that compo
of nutrition
nents, and
have a grea
The Me
mechanism
tion, which
AD.59 Com
Fig 2. Survival curves based on Cox analysis comparing cu- with impor
mulative Alzheimer’s disease (AD) incidenceScarmeas et al. Ann Neurol. 2006
in subjects be- C, vitamin
longing to each Mediterranean diet (MeDi) tertile (p for“Each additional unit of the MeDi score was associated with 9
to 10% less risk for development of AD, and progression of the
disease.”
Scarmeas et al. Ann Neurol. 20064
memory
Hypothetical cardiovascular disease cascade in cognitve decline recognit
able to m
Cardiovascular disease risk factors fraction
progres
Disturbed hemodynamics
clusion
Cerebral hypoperfusion less, it
CATCH
detects
Energy substrate delivery iac outp
diovascu
Proteinopathy and Abeta misfolding linked,
cardiac
Clearance of Abeta and various toxins
in preve
Executive function Psychomotor speed
dement
Verbal fluency Mental flexibility and sequencing
Abnormal MMSE Memory
5. Atri
Figure 2: Hypothetical model based on the collective evidence
available showing how cardiovascular risk factors give rise to Atrial fi
disturbed hemodynamic flow patterns inducing cerebral hypoper- usuallyR.S. Marshall / Hemodynamics and Cognitive Impairment 635
Fig. 1. Levels of hemodynamic impairment associated with cognitive dysfunction. Hemispheral flow impairment due to carotid artery stenosis
Marshall, R. Journal of Alzheimer’s Disease,2012
illustrated by angiogram of internal carotid artery stenosis; global flow impairment illustrated by heart failure; microvascular blood flow
impairment illustrated by arteriolar anatomy.Articles
A 2 year multidomain intervention of diet, exercise, cognitive
training, and vascular risk monitoring versus control to
prevent cognitive decline in at-risk elderly people (FINGER):
a randomised controlled trial
Tiia Ngandu, Jenni Lehtisalo, Alina Solomon, Esko Levälahti, Satu Ahtiluoto, Riitta Antikainen, Lars Bäckman, Tuomo Hänninen, Antti Jula,
Tiina Laatikainen, Jaana Lindström, Francesca Mangialasche, Teemu Paajanen, Satu Pajala, Markku Peltonen, Rainer Rauramaa,
Anna Stigsdotter-Neely, Timo Strandberg, Jaakko Tuomilehto, Hilkka Soininen, Miia Kivipelto
Summary
Background Modifiable vascular and lifestyle-related risk factors have been associated with dementia risk in Lancet 2015; 385: 2255–63
observational studies. In the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability Published Online
(FINGER), a proof-of-concept randomised controlled trial, we aimed to assess a multidomain approach to prevent March 12, 2015
http://dx.doi.org/10.1016/
cognitive decline in at-risk elderly people from the general population.
S0140-6736(15)60461-5
Chronic Disease Prevention
Methods In a double-blind randomised controlled trial we enrolled individuals aged 60–77 years recruited from Unit (T Ngandu PhD,
previous national surveys. Inclusion criteria were CAIDE (Cardiovascular Risk Factors, Aging and Dementia) J Lehtisalo MSc, E Levälahti MSc,
Dementia Risk Score of at least 6 points and cognition at mean level or slightly lower than expected for age. We S Ahtiluoto MD, Prof A Jula PhD,
Prof T Laatikainen PhD,
randomly assigned participants in a 1:1 ratio to a 2 year multidomain intervention (diet, exercise, cognitive training,
J Lindström PhD,
vascular risk monitoring), or a control group (general health advice). Computer-generated allocation was done in Prof M Peltonen PhD,
blocks of four (two individuals randomly allocated to each group) at each site. Group allocation was not actively Prof J Tuomilehto PhD,
disclosed to participants and outcome assessors were masked to group allocation. The primary outcome was change Prof M Kivipelto PhD) and
Welfare and Health Promotion
in cognition as measured through comprehensive neuropsychological test battery (NTB) Z score. Analysis was by
Unit (S Pajala PhD), National
modified intention to treat (all participants with at least one post-baseline observation). This trial is registered at Institute for Health and
ClinicalTrials.gov, number NCT01041989. Welfare, Helsinki, Finland;
Karolinska Institutet Center for
Alzheimer Research,
Findings Between Sept 7, 2009, and Nov 24, 2011, we screened 2654 individuals and randomly assigned 1260 to the
Stockholm, Sweden (T Ngandu,
intervention group (n=631) or control group (n=629). 591 (94%) participants in the intervention group and 599 (95%) A Solomon PhD,
in the control group had at least one post-baseline assessment and were included in the modified intention-to-treat Prof M Kivipelto); Institute of
analysis. Estimated mean change in NTB total Z score at 2 years was 0·20 (SE 0·02, SD 0·51) in the intervention Clinical Medicine/Neurology
(A Solomon,M. Kivipelto et al. / Alzheimer’s & Dementia - (2013) 1–9
Screening (Nurse: CERAD; Physician) INTENSIVE INTERVENTION
NUTRITIONAL COUNCELING:
7 group & 3 individual sessions
Recruitment (Dementia risk score)
PHYSICAL ACTIVITY: PHYSICAL ACTIVITY:
INTERVENTION KICK-OFF 1-2x/wk muscle strength & 2-3x/wk muscle strength &
1-4x/wk aerobic training 5-6x/wk aerobic training
Baseline visit (NTB)
COGNITIVE TRAINING: COGNITIVE TRAINING:
RANDOMIZATION
9 group sessions, 2 group sessions,
Independent training 3x/wk 6mo Independent training 3x/wk 6mo
MANAGEMENT OF METABOLIC AND VASCULAR RISK FACTORS
6 nurse visits, 4 physician visits
Follow-up visit Follow-up visit Follow-up visit
Month 3 6 9 12 15 18 21 24
MINI- Follow-up visit Follow-up visit Follow-up visit
INTERVENTION
REGULAR HEALTH ADVICE
Fig. 2. FINGER protocol.
Kivipelto et al. Alzheimer’s & Dementia, 2013intensive intervention group (n=631) or control group (p=0·07). The main
(n=629; figure 1). 1168 (93%) participants completed related (56 [37%]
See Online for appendix the 12 month assessments, and 1105 (88%) participants motivation (22 [14%
participation (18 [1
NTB total score Executive functioning the study.
0·25 Control 0·14 Baseline character
Intervention
0·12 in detail.15 The inte
0·20 similar at baseline
p=0·03 p=0·04
0·10
for intention-to-trea
0·15 0·08 appendix). The m
Z score
69·3 years (SD 4·7),
0·10 0·06
mini mental state
0·04 (SD 2·0). Mean co
0·05 0·5 SD below the ave
0·02
Finnish population.
0·00 0·00 factors were present
Processing speed Memory
We noted a sig
0·14 0·40 intervention for the p
Estimated mean cha
0·12 0·35
p=0·03 p=0·36 was 0·20 (SE 0·01, SD
0·30
0·10 0·16 (0·01, 0·51)
0·25 difference between
0·08
change of NTB tota
Z score
0·20
0·06 0·002–0·042, p=0·03
0·15
0·04
after 24 months was
0·10
than in the contr
0·02 0·05 unchanged in sensit
0·00 0·00 treat analyses (appen
Baseline 12 months 24 months Baseline 12 months 24 months We also noted a s
Figure 2: Change in cognitive performance during the 2 year intervention secondary cognitive
Figure shows estimated mean change in cognitive performance from baseline until 12 and 24 months (higher (p=0·039) and proc
scores suggest better performance) in the modified intention-to-treat population. Error bars are SEs. Mixed-model appendix). Improvem
repeated-measures analyses were used to assess between-group differences (group × time interaction) in changes 83% higher, and in pOur Research
10 SHERZAI/c/p_04 LORD_c 18/04/12 13:26 Page319
The Journal of Nutrition, Health & Aging©
Volume 16, Number 4, 2012
JNHA: CLINICAL NEUROSCIENCES
NUTRITION AND VASCULAR DEMENTIA
D SHERZAI
L. PEREZ, L. HEIM, A. SHERZAI, K. JACELDO-SIEGL, A.
Loma Linda University. Correspondance author: A. Dean Sherzai MD, MAS, PhD(c), Director of Memory and Aging Center, Director of Research, Neurology, 11370 Anderson Street,
Suite 2400, (909) 558-2880 (office), (909) 558-2237 (fax), adsherzai@llu.edu
Abstract: Objective: The objective of this review was to elucidate the relationship between VaD and various
nutritional factors based on epidemiological studies. Background: Vascular dementia (VaD) is the second most
common type of dementia. The prevalence of VaD continues to increase as the US population continues to grow
and age. Currently, control of potential risk factors is believed to be the most effective means of preventing VaD.
Thus, identification of modifiable risk factors for VaD is crucial for development of effective treatment
modalities. Nutrition is one of the main modifiable variables that may influence the development of VaD.
Methods: A systematic review of literature was conducted using the PubMed, Web of Science, and CINAHL
Plus databases with search parameters inclusive of vascular dementia, nutrition, and vascular cognitive
impairment (VCI). Results: Fourteen articles were found that proposed a potential role of specific nutritional
components in VaD. These components included antioxidants, lipids, homocysteine, folate, vitamin B12, and fish
consumption. Antioxidants, specifically Vitamin E and C, and fatty fish intake were found to be protective
against VaD risk. Fried fish, elevated homocysteine, and lower levels of folate and vitamin B12 were associated
with increased VaD. Evidence for dietary lipids was inconsistent, although elevated midlife serum cholesterol
may increase risk, while late-life elevated serum cholesterol may be associated with decreased risk of VaD.
Conclusion: Currently, the most convincing evidence as to the relationship between VaD and nutrition exists for
micronutrients, particularly Vitamin E and C. Exploration of nutrition at the macronutrient level and additional
long term prospective cohort studies are warranted to better understand the role of nutrition in VaD disease
development and progression. At present, challenges in this research include limitations in sample size, which
was commonly cited. Also, a variety of diagnostic criteria for VaD were employed in the studies reviewed,
indicating the need for constructing a correct nosological definition of VaD for consistency and conformity in
future studies and accurate clinical diagnosis of VaD.
Key words: Vascular dementia, nutrition, diet.
Introduction care than AD, other dementias, or cerebrovascular disease
without dementia (10).
In the United States, the proportion of people over the age of Currently,
The Journalcontrol of VaDHealth
of Nutrition, risk factors is believed
& Aging, to be the
2012, 16(4), 319-324.
65 is projected to increase from 35 million in the year 2000 to most effective way to prevent onset or delay progression of theArticle
Journal of Geriatric Psychiatry
and Neurology
The Association Between Diabetes and 2016, Vol. 29(3) 120-125
ª The Author(s) 2016
Dementia Among Elderly Individuals: Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0891988715627016
A Nationwide Inpatient Sample Analysis jgpn.sagepub.com
Dean Sherzai, MD, MAS, PhD(c)1, Ayesha Sherzai, MD2, Keith Lui, MD2,
Deyu Pan, MS3, Daniel Chiou, MD2, Mohsen Bazargan, PhD3,
and Magda Shaheen, PhD, MPH4
Abstract
Background/Aim: To date, few studies have cross-examined the relationship between diabetes mellitus (DM) and dementia
nationally. There is also a lack of evidence regarding dementia subtypes and how this relationship changes among older individuals.
The objective was to better delineate this relationship and influence of multiple comorbidities using a nationwide sample.
Methods: Data were obtained from the Nationwide Inpatient Sample 1998 to 2011 using appropriate International Classification of
Diseases, Ninth Version codes. Descriptive and bivariate analysis was performed. Multivariate nominal logistic regression models
adjusted for age, sex, race, and comorbidities explored the independent relationship between Alzheimer dementia (AD), non-
Alzheimer dementia (VaD), and diabetes. Results: 21% of the participants were diabetic patients, 3.7% had AD, and 2.2% had
VaD. Diabetes prevalence in AD, VaD, and no dementia groups were 20.6%, 24.3%, and 26.2%, respectively. In the unadjusted
model, those with DM had lower odds of AD (odds ratio [OR] 0.73; 95% confidence interval [CI] 0.72-0.74) and VaD (OR 0.91,
95% CI 0.89-0.92). Adjusting for age, sex, race, and comorbidities, diabetic patients had significantly higher odds of VaD
(OR ¼ 1.10, 95% CI 1.08-1.11) and lower odds of AD (OR 0.87, 95% CI 0.86-0.88). Inclusion of interaction terms (age, race/
ethnicity, depression, stroke, and hypertension) made the relationship between diabetes and VaD not significant (OR 1.002,
95% CI 0.97-1.03), but the relationship of DM with AD remained significant (OR 0.57, 95% CI 0.56-0.58; P < .05).
Conclusion: Patients with a diagnosis of diabetes mellitus had lower odds of having AD. Age, race/ethnicity, depression,
stroke, and hypertension modified the relationship between DM and both VaD and AD. Further exploration of the relationship
between DM and AD is warranted.
Keywords
dementia, vascular dementia, Alzheimer disease
Introduction who used participants aged 65 years and older and 80 years and
older,Journal of Geriatric
respectively, Psychiatry
both found andrisk
no increased Neurology,
of AD and 2016,
a Vol. 29(3) 120-125
Currently, there are more than 24 million people worldwide with
greater than 2-fold increase in risk of non-Alzheimer dementiabs_bs_banner
Lead Article
Stroke, food groups, and dietary patterns: a systematic review
Ayesha Sherzai, Lauren T Heim, Cassaundra Boothby, and A Dean Sherzai
Stroke is the fourth leading cause of mortality in the United States, yet it is 80%
preventable by addressing lifestyle factors including nutrition. Evaluating the
impact of nutrition at the food group and dietary pattern level will provide greater
insight into the role of nutrition in stroke. For this purpose, a review of the literature
was conducted using the PubMed, Web of Science, and CINAHL Plus online
databases. While fruits, vegetables, and soy demonstrated a protective effect,
variable findings were observed for fish, animal products, and whole grains.
Adherence to DASH, Mediterranean, and prudent dietary patterns reduced the risk of
stroke, whereas the Western dietary pattern was associated with increased stroke
risk. Low-fat diet was not found to have a protective effect. Additional
epidemiological evidence is needed to elucidate the impact of specific dietary
patterns and food groups on stroke. Future research should consider developing
dietary recommendations for stroke prevention, which are based on clinical trials
and have an emphasis on food groups and dietary patterns that are palatable to the
general public.
© 2012 International Life Sciences Institute
INTRODUCTION while lifestyle risk factors such as diet, exercise, and use of
tobacco and alcohol are considered modifiable risk fac-
Stroke places a tremendous burden on the healthcare tors.5 By addressing the modifiable risk factors, it is esti-
system worldwide. In the United States, it is the 4th leading mated that stroke prevalence can be reduced by as much
cause of mortality, with an estimated 795,000 incident as 80%.6 Thus, primary prevention of stroke takes central
strokes each year.1,2 As age is one of the main risk factors importance.
for stroke, and with the elderly population expected to Substantial research has been done over the past
double to more than 70 million by the year 2030, reducing decades in order to advanceNutrition
understanding
Reviews, of 2012,
stroke1;70(8):423-35
the incidence of stroke has become a central healthcare mechanisms and therapies. Despite a large body of dataCALIFORNIA TEACHERS STUDY • In 1995, 133,479 female public school teachers and administrators were enrolled in the study • Geographically and socioeconomically diverse • Mail paper questionnaires every 4-5 years • Linked with California Cancer Registry
MEDITERRANEAN DIET AND ALL
STROKE INCIDENCE
1 1
0.89 0.89
0.86
0.83
0.5
0-2 3 4 5 6-9
Adjusted* Hazard Ratio Mediterranean Diet Score groups
(p trend 0.009)
*Age, race, SES, moderate plus strenuous physical activity, kilocalories, BMI, smoking,
hypertension, diabetes, atrial fibrillation, hypercholesterolemia, history of cardiac disease
and menopausal status and hormone therapy.
Submitted for publication to Stroke.Cognitive Function and Diet
• Our formal study of the California Verbal Learning
Test (CVLT), revealed that among 500 individuals
who ate a vegetarian had on average a 28 percent
lower risk of cognitive impairment.
In the process of publication.Circulation, 2016 (Vol. 133).
Sugar Consumption
• Reductions in brain glucose metabolism have long
been associated with Alzheimer’s disease
• Brain insulin resistance initiates a cascade of
inflammatory stress and oxidative damage,
disruption of synaptic function, resulting in amyloid
proteins becoming insoluble
• Deregulation of endothelial glucose transporter
GLUT1, vital for maintaining brain energy
metabolism and vascular clearance of amyloid-βAlzheimer’s & Dementia - (2017) 1-10
Featured Article
Sugary beverage intake and preclinical Alzheimer’s disease in the
community
Matthew P. Pasea,b,c,*, Jayandra J. Himalia,b,d, Paul F. Jacquesb,e, Charles DeCarlib,f,
Claudia L. Satizabala,b, Hugo Aparicioa,b, Ramachandran S. Vasanb,g,h, Alexa S. Beisera,b,d,
Sudha Seshadria,b
a
Department of Neurology, Boston University School of Medicine, Boston, MA, USA
b
Framingham Heart Study, Framingham, MA, USA
c
Centre for Human Psychopharmacology, Swinburne University of Technology, Hawthorn, Australia
d
Department of Biostatistics, Boston University School of Public Health, Boston, MA, USA
e
Jean Mayer-U.S. Department of Agriculture Human Nutrition Research Center on Aging, Tufts University, Boston, MA, USA
f
Department of Neurology, School of Medicine & Imaging of Dementia and Aging Laboratory, Center for Neuroscience, University of California Davis,
Sacramento, CA, USA
g
Sections of Preventive Medicine and Epidemiology, Department of Medicine, Boston University School of Medicine, Boston, MA, USA
h
Department of Epidemiology, Boston University School of Public Health, Boston, MA, USA
Abstract Introduction: Excess sugar consumption has been linked with Alzheimer’s disease (AD) pathology
in animal models.
Methods: We examined the cross-sectional association of sugary beverage consumption with
neuropsychological (N 5 4276) and magnetic resonance imaging (N 5 3846) markers of preclinical
Alzheimer’s disease and vascular brain injury (VBI) in the community-based Framingham Heart
Study. Intake of sugary beverages was estimated using a food frequency questionnaire.
Results: Relative to consuming less than one sugary beverage per day, higher intake of sugary bev-
erages was associated with lower total brain volume (1–2/day, b 6 standard error
[SE] 5 20.55 6 0.14 mean percent difference, P 5 .0002; .2/day, b 6 SE 5 20.68 6 0.18,
P ,.0001), and poorer performance on tests of episodic memory (all P ,.01). Daily fruit juice intake
was associated with lower total brain volume, hippocampal volume, and poorer episodic memory (all
P ,.05). Sugary beverage intake was not associated with VBI in a consistent manner across outcomes.
Discussion: Higher intake of sugary beverages was associated cross-sectionally with markers of pre-Alzheimer’s & Dementia - (2017) 1-10
Featured Article
Sugary beverage intake and preclinical Alzheimer’s disease in the
community
Matthew P. Pasea,b,c,*, Jayandra J. Himalia,b,d, Paul F. Jacquesb,e, Charles DeCarlib,f,
High sugar consumption was associated with low
Claudia L. Satizabala,b, Hugo Aparicioa,b, Ramachandran S. Vasanb,g,h, Alexa S. Beisera,b,d,
Sudha Seshadria,b
hippocampal and total brain volumes. Individuals who
a
Department of Neurology, Boston University School of Medicine, Boston, MA, USA
b
Framingham Heart Study, Framingham, MA, USA
consumed more sugar also experienced a greater loss of
e
c
Centre for Human Psychopharmacology, Swinburne University of Technology, Hawthorn, Australia
d
Department of Biostatistics, Boston University School of Public Health, Boston, MA, USA
Jean Mayer-U.S. Department of Agriculture Human Nutrition Research Center on Aging, Tufts University, Boston, MA, USA
f
brain volume over the course of two years
Department of Neurology, School of Medicine & Imaging of Dementia and Aging Laboratory, Center for Neuroscience, University of California Davis,
g
Sacramento, CA, USA
Sections of Preventive Medicine and Epidemiology, Department of Medicine, Boston University School of Medicine, Boston, MA, USA
h
Department of Epidemiology, Boston University School of Public Health, Boston, MA, USA
Abstract Introduction: Excess sugar consumption has been linked with Alzheimer’s disease (AD) pathology
in animal models.
Methods: We examined the cross-sectional association of sugary beverage consumption with
neuropsychological (N 5 4276) and magnetic resonance imaging (N 5 3846) markers of preclinical
Alzheimer’s disease and vascular brain injury (VBI) in the community-based Framingham Heart
Study. Intake of sugary beverages was estimated using a food frequency questionnaire.
Results: Relative to consuming less than one sugary beverage per day, higher intake of sugary bev-
erages was associated with lower total brain volume (1–2/day, b 6 standard error
[SE] 5 20.55 6 0.14 mean percent difference, P 5 .0002; .2/day, b 6 SE 5 20.68 6 0.18,
P ,.0001), and poorer performance on tests of episodic memory (all P ,.01). Daily fruit juice intakeThe Danger of Ketogenic
Diet
• Background: Alternative source of energy needed
for the brain
• Proven to be beneficial in certain cases of
childhood epilepsy
• No strong data for benefit in neurodegenerative
conditions
• High saturated fat in ketogenic diets cause
vascular damageClinic Experience
• 2500 patients evaluated in brain health clinic
• Less than 1% (n=19) patients were vegetarians
and led a healthy lifestyle (NEURO Plan)n
ssu
d
re
Po ead a
H m
Our Lifestyle Intervention Program Sle or
ep Small
Vessel
Tra
u
Disease
at Loma Linda Health
Regular Exercise1
PROTECTIVE +S
Moving tanding
FACTORS Str
ht e es
Exercise
r
M Ma
po g
ed na
Ex ayli
su
s
ita gem
D
tio
n ent
2
ind
ga-3 Fatty Acids
w
Un
Plant-Ba d Diet 3
Nutrition
se
1. Aerobic exercise,
ual
ng
resistance training,
Contin
Learni
and balance
e
strengthening.
m
Learn more in
O
Re
Chapter 4. st
ize
or
e
tim
2. Walking
s en
Op
meditation, mindful
7– f Sl
riv
breathing, yoga, -D e
8H
o
o
and others. Learn ee urs e
os viti
p r p
more in Chapter 5. Pu Acti
3. Learn more about Social
Engage nt
beneficial and me
Volunteering
harmful foods on
page 126.NEURO Plan
• Nutrition (whole-food, plant-based diet, low in
sugar)
• Exercise
• Unwind
• Restorative sleep
• Optimize medical and cognitive activitiesCurrent Research
• Effect of comprehensive lifestyle intervention on
cognitive health compared to standard-of-care
• Comparison of dietary patterns and Alzheimer’s
disease (whole-food, plant-based diet vs. high fat,
low carbohydrate diet)
• Aggressive management of vascular risk factors
among patients with Mild Cognitive ImpairmentThank you!
Join us:
TeamSherzai.com
Twitter: @TeamSherzai
Facebook: Team Sherzai
Instagram: @TeamSherzaiYou can also read

















































